
Impact of COVID-19 Related Maternal Stress on Fetal Brain Development: A Multimodal MRI Study
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Subject Demographics
2.2. Stress and Coping Behavioral Assessments
2.3. Child Opportunity Index (COI)
2.4. Image Acquisition
2.5. Image Processing
2.5.1. Brain Structure
2.5.2. Brain Function
2.6. Statistical Analysis
2.6.1. Brain Structure
2.6.2. Brain Function
2.6.3. Comparison of Coping Behaviors
3. Results
3.1. Subject Demographics
3.2. Brain Structure
3.3. Brain Function
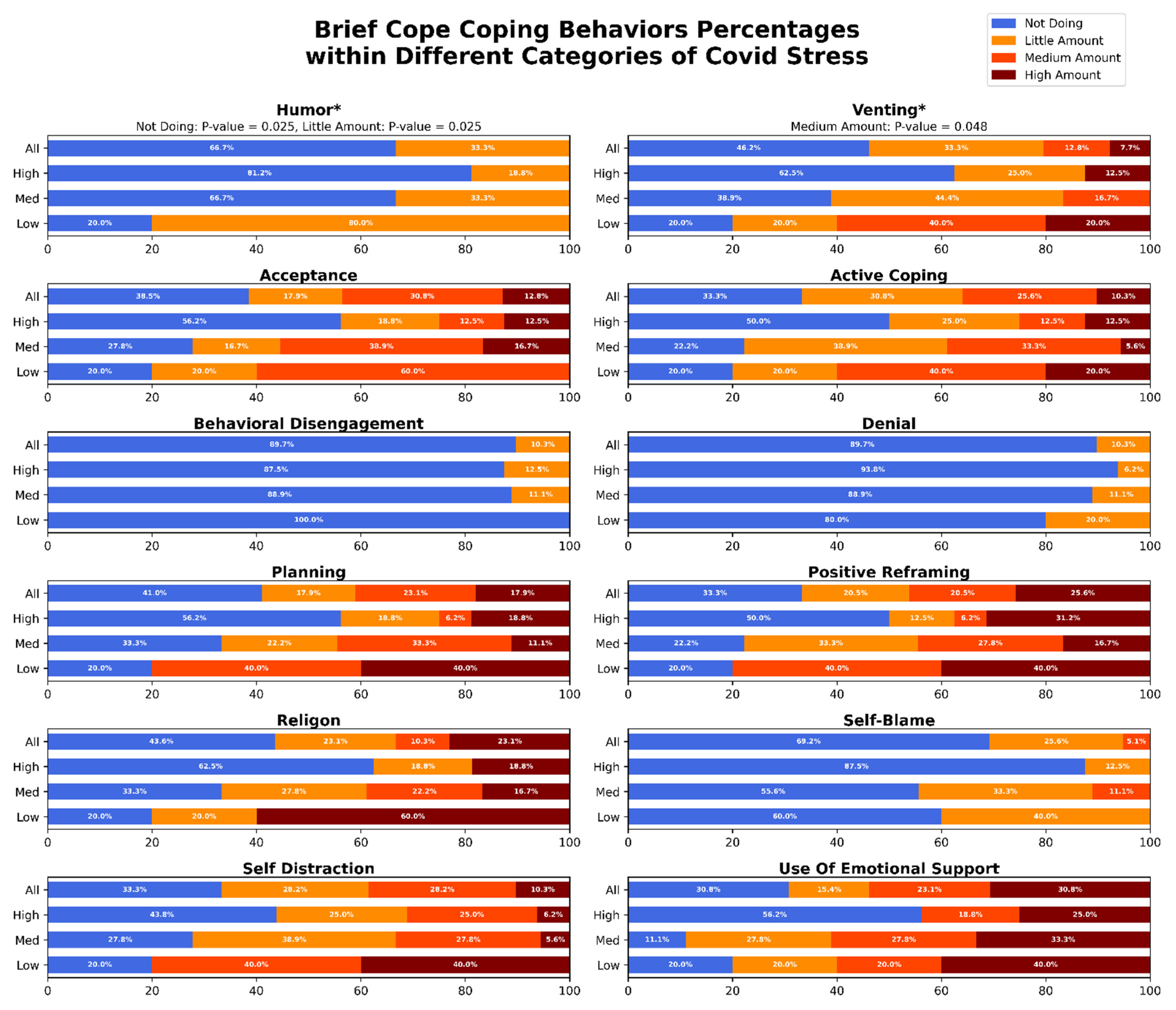
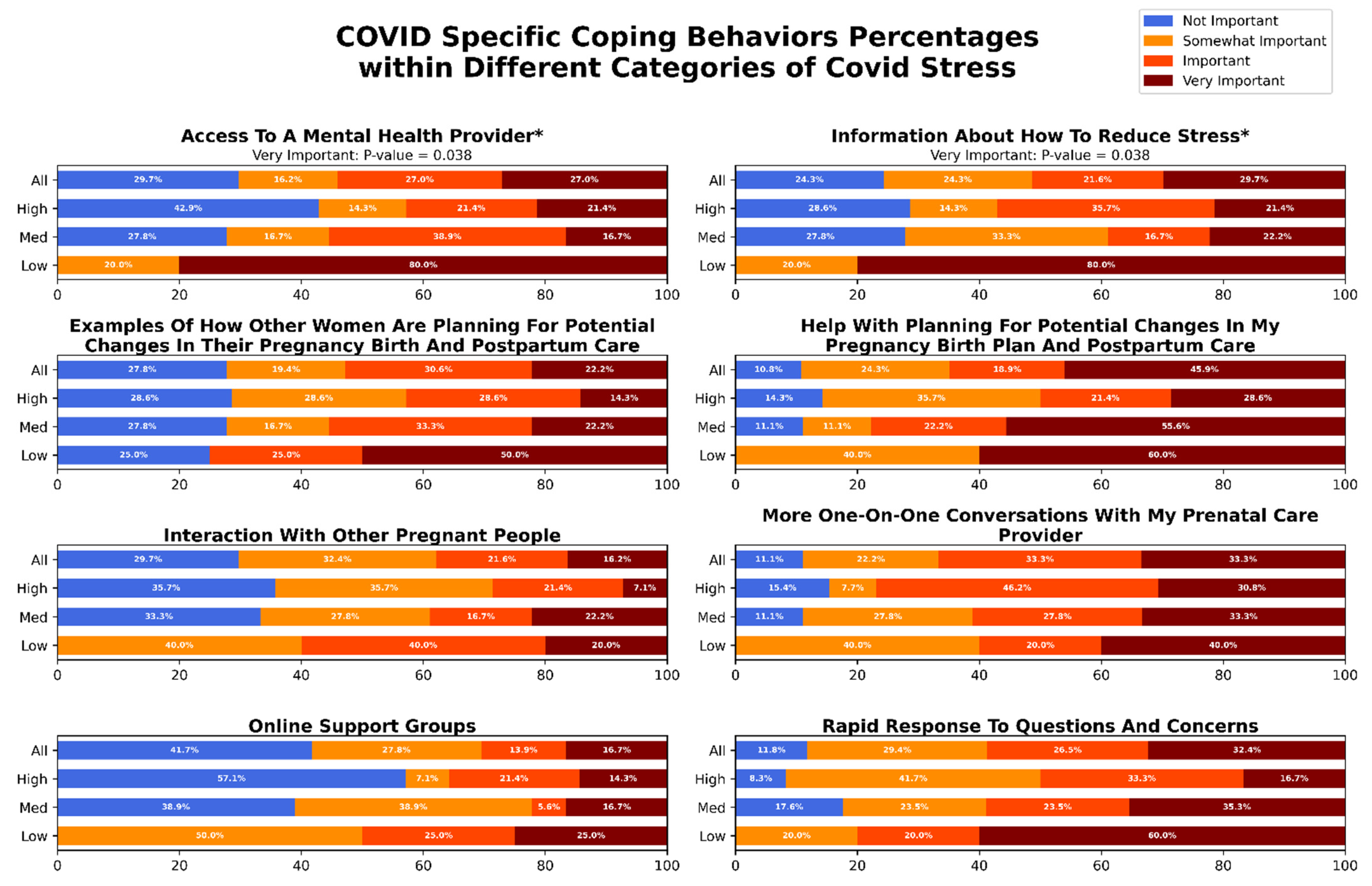
3.4. Comparison of Coping Behaviors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, J.; Havens, K.L.; Starnes, C.P.; Pickering, T.A.; Brito, N.H.; Hendrix, C.L.; Thomason, M.E.; Vatalaro, T.C.; Smith, B.A. Changes in Social Support of Pregnant and Postnatal Mothers during the COVID-19 Pandemic. Midwifery 2021, 103, 103162. [Google Scholar] [CrossRef] [PubMed]
- Barbosa-Leiker, C.; Smith, C.L.; Crespi, E.J.; Brooks, O.; Burduli, E.; Ranjo, S.; Carty, C.L.; Hebert, L.E.; Waters, S.F.; Gartstein, M.A. Stressors, Coping, and Resources Needed during the COVID-19 Pandemic in a Sample of Perinatal Women. BMC Pregnancy Childbirth 2021, 21, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Shorey, S.; Chee, C.Y.I.; Ng, E.D.; Chan, Y.H.; Tam, W.W.S.; Chong, Y.S. Prevalence and Incidence of Postpartum Depression among Healthy Mothers: A Systematic Review and Meta-Analysis. J. Psychiatr. Res. 2018, 104, 235–248. [Google Scholar] [CrossRef] [PubMed]
- King, S.; Dancause, K.; Turcotte-Tremblay, A.M.; Veru, F.; Laplante, D.P. Using Natural Disasters to Study the Effects of Prenatal Maternal Stress on Child Health and Development. Birth Defects Res. C Embryo Today 2012, 96, 273–288. [Google Scholar] [CrossRef] [PubMed]
- Salm Ward, T.; Kanu, F.A.; Robb, S.W. Prevalence of Stressful Life Events during Pregnancy and Its Association with Postpartum Depressive Symptoms. Arch. Womens Ment. Health 2017, 20, 161–171. [Google Scholar] [CrossRef]
- Motrico, E.; Domínguez-Salas, S.; Rodríguez-Domínguez, C.; Gómez-Gómez, I.; Rodríguez-Muñoz, M.F.; Gómez-Baya, D. The Impact of the COVID-19 Pandemic on Perinatal Depression and Anxiety: A Large Cross-Sectional Study in Spain. Psicothema 2022, 34, 200–208. [Google Scholar] [CrossRef]
- Bianco, C.; Sania, A.; Kyle, M.H.; Beebe, B.; Barbosa, J.; Bence, M.; Coskun, L.; Fields, A.; Firestein, M.R.; Goldman, S.; et al. Pandemic beyond the Virus: Maternal COVID-Related Postnatal Stress Is Associated with Infant Temperament. Pediatric Res. 2022, 2022, 1–7. [Google Scholar] [CrossRef]
- Shuffrey, L.C.; Firestein, M.R.; Kyle, M.H.; Fields, A.; Alcántara, C.; Amso, D.; Austin, J.; Bain, J.M.; Barbosa, J.; Bence, M.; et al. Association of Birth During the COVID-19 Pandemic With Neurodevelopmental Status at 6 Months in Infants with and without In Utero Exposure to Maternal SARS-CoV-2 Infection. JAMA Pediatr. 2022, 176, e215563. [Google Scholar] [CrossRef]
- Schuurmans, C.; Kurrasch, D.M. Neurodevelopmental Consequences of Maternal Distress: What Do We Really Know? Clin. Genet. 2013, 83, 108–117. [Google Scholar] [CrossRef]
- Talge, N.M.; Neal, C.; Glover, V. Antenatal Maternal Stress and Long-Term Effects on Child Neurodevelopment: How and Why? J. Child Psychol. Psychiatry 2007, 48, 245–261. [Google Scholar] [CrossRef]
- Wu, Y.; Lu, Y.C.; Jacobs, M.; Pradhan, S.; Kapse, K.; Zhao, L.; Niforatos-Andescavage, N.; Vezina, G.; du Plessis, A.J.; Limperopoulos, C. Association of Prenatal Maternal Psychological Distress with Fetal Brain Growth, Metabolism, and Cortical Maturation. JAMA Netw. Open 2020, 3, e1919940. [Google Scholar] [CrossRef] [PubMed]
- van den Heuvel, M.I.; Hect, J.L.; Smarr, B.L.; Qawasmeh, T.; Kriegsfeld, L.J.; Barcelona, J.; Hijazi, K.E.; Thomason, M.E. Maternal Stress during Pregnancy Alters Fetal Cortico-Cerebellar Connectivity in Utero and Increases Child Sleep Problems after Birth. Sci. Rep. 2021, 11, 2228. [Google Scholar] [CrossRef] [PubMed]
- Griffin, M.; Ghassabian, A.; Majbri, A.; Brubaker, S.G.; Thomason, M. Evaluating the Association between Maternal Peripartum Care Interruptions and Infant Affect: A Longitudinal Study. Am. J. Obstet. Gynecol. 2022, 226, S310. [Google Scholar] [CrossRef]
- Provenzi, L.; Grumi, S.; Altieri, L.; Bensi, G.; Bertazzoli, E.; Biasucci, G.; Cavallini, A.; Decembrino, L.; Falcone, R.; Freddi, A.; et al. Prenatal Maternal Stress during the COVID-19 Pandemic and Infant Regulatory Capacity at 3 Months: A Longitudinal Study. Dev. Psychopathol. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Manning, K.Y.; Long, X.; Watts, D.; Tomfohr-Madsen, L.; Giesbrecht, G.F.; Lebel, C. Prenatal Maternal Distress During the COVID-19 Pandemic and Associations with Infant Brain Connectivity. Biol. Psychiatry 2022, 92, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.-C.; Andescavage, N.; Wu, Y.; Kapse, K.; Andersen, N.R.; Quistorff, J.; Saeed, H.; Lopez, C.; Henderson, D.; Barnett, S.D.; et al. Maternal Psychological Distress during the COVID-19 Pandemic and Structural Changes of the Human Fetal Brain. Commun. Med. 2022, 2, 47. [Google Scholar] [CrossRef]
- Varescon, I.; Leignel, S.; Poulain, X.; Gerard, C. Coping Strategies and Perceived Stress in Pregnant Smokers Seeking Help for Cessation. J. Smok. Cessat. 2011, 6, 126–132. [Google Scholar] [CrossRef]
- Razurel, C.; Kaiser, B.; Sellenet, C.; Epiney, M. Relation between Perceived Stress, Social Support, and Coping Strategies and Maternal Well-Being: A Review of the Literature. Women Health 2013, 53, 74–99. [Google Scholar] [CrossRef]
- Rimal, S.P.; Thapa, K.; Shrestha, R. Psychological Distress and Coping among Pregnant Women during the COVID 19 Pandemic. J. Nepal Health Res. Counc. 2022, 20, 234–240. [Google Scholar] [CrossRef]
- Kinser, P.A.; Jallo, N.; Amstadter, A.B.; Thacker, L.R.; Jones, E.; Moyer, S.; Rider, A.; Karjane, N.; Salisbury, A.L. Depression, Anxiety, Resilience, and Coping: The Experience of Pregnant and New Mothers during the First Few Months of the COVID-19 Pandemic. J. Womens Health 2021, 30, 654–664. [Google Scholar] [CrossRef]
- Werchan, D.M.; Hendrix, C.L.; Ablow, J.C.; Amstadter, A.B.; Austin, A.C.; Babineau, V.; Anne Bogat, G.; Cioffredi, L.A.; Conradt, E.; Crowell, S.E.; et al. Behavioral Coping Phenotypes and Associated Psychosocial Outcomes of Pregnant and Postpartum Women during the COVID-19 Pandemic. Sci. Rep. 2022, 12, 1209. [Google Scholar] [CrossRef] [PubMed]
- Thomason, M.; Graham, A.; Sullivan, E.; van den Heuvel, M.I. COVID-19 and Perinatal Experiences Study. Available online: https://osf.io/uqhcv/ (accessed on 28 August 2022).
- Brief Symptom Inventory—PsycNET. Available online: https://psycnet.apa.org/doiLanding?doi=10.1037%2Ft00789-000 (accessed on 16 September 2022).
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Carver, C.S. You Want to Measure Coping but Your Protocol’s Too Long: Consider the Brief COPE. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing Coping Strategies: A Theoretically Based Approach. J. Pers. Soc. Psychol. 1989, 56, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Connor-Smith, J.K.; Flachsbart, C. Relations between Personality and Coping: A Meta-Analysis. J. Pers. Soc. Psychol. 2007, 93, 1080–1107. [Google Scholar] [CrossRef]
- García, F.E.; Barraza-Peña, C.G.; Wlodarczyk, A.; Alvear-Carrasco, M.; Reyes-Reyes, A. Psychometric Properties of the Brief-COPE for the Evaluation of Coping Strategies in the Chilean Population. Psicol. Reflex. Crit. 2018, 31, 1–11. [Google Scholar] [CrossRef]
- Lefmann, T.; Combs-Orme, T. Prenatal Stress, Poverty, and Child Outcomes. Child Adolesc. Soc. Work J. 2014, 31, 577–590. [Google Scholar] [CrossRef]
- Silverman, M.E.; Medeiros, C.; Burgos, L. Early Pregnancy Mood before and during COVID-19 Community Restrictions among Women of Low Socioeconomic Status in New York City: A Preliminary Study. Arch. Womens Ment. Health 2020, 23, 779. [Google Scholar] [CrossRef]
- Sandel, M.; Faugno, E.; Mingo, A.; Cannon, J.; Byrd, K.; Garcia, D.A.; Collier, S.; McClure, E.; Jarrett, R.B. Neighborhood-Level Interventions to Improve Childhood Opportunity and Lift Children out of Poverty. Acad. Pediatr. 2016, 16, S128–S135. [Google Scholar] [CrossRef]
- Acevedo-Garcia, D.; McArdle, N.; Hardy, E.F.; Crisan, U.I.; Romano, B.; Norris, D.; Baek, M.; Reece, J. The Child Opportunity Index: Improving Collaboration between Community Development and Public Health. Health Aff. 2014, 33, 1948–1957. [Google Scholar] [CrossRef]
- Ebner, M.; Wang, G.; Li, W.; Aertsen, M.; Patel, P.A.; Aughwane, R.; Melbourne, A.; Doel, T.; Dymarkowski, S.; de Coppi, P.; et al. An Automated Framework for Localization, Segmentation and Super-Resolution Reconstruction of Fetal Brain MRI. Neuroimage 2020, 206, 116324. [Google Scholar] [CrossRef] [PubMed]
- Gholipour, A.; Rollins, C.K.; Velasco-Annis, C.; Ouaalam, A.; Akhondi-Asl, A.; Afacan, O.; Ortinau, C.M.; Clancy, S.; Limperopoulos, C.; Yang, E.; et al. A Normative Spatiotemporal MRI Atlas of the Fetal Brain for Automatic Segmentation and Analysis of Early Brain Growth. Sci. Rep. 2017, 7, 476. [Google Scholar] [CrossRef] [PubMed]
- Avants, B.B.; Tustison, N.J.; Song, G.; Cook, P.A.; Klein, A.; Gee, J.C. A Reproducible Evaluation of ANTs Similarity Metric Performance in Brain Image Registration. Neuroimage 2011, 54, 2033–2044. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.M. Fast Robust Automated Brain Extraction. Hum. Brain Mapp. 2002, 17, 143–155. [Google Scholar] [CrossRef]
- Cox, R.W. AFNI: Software for Analysis and Visualization of Functional Magnetic Resonance Neuroimages. Comput. Biomed. Res. 1996, 29, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Amin, S.B.; Orlando, M.S.; Dalzell, L.E.; Merle, K.S.; Guillet, R. Morphological Changes in Serial Auditory Brain Stem Responses in 24 to 32 Weeks’ Gestational Age Infants during the First Week of Life. Ear Hear. 1999, 20, 410–418. [Google Scholar] [CrossRef]
- Jiang, Z.D.; Xiu, X.; Brosi, D.M.; Shao, X.M.; Wilkinson, A.R. Sub-Optimal Function of the Auditory Brainstem in Term Infants with Transient Low Apgar Scores. Clin. Neurophysiol. 2007, 118, 1088–1096. [Google Scholar] [CrossRef]
- DiPietro, J.A.; Kivlighan, K.T.; Costigan, K.A.; Rubin, S.E.; Shiffler, D.E.; Henderson, J.L.; Pillion, J.P. Prenatal Antecedents of Newborn Neurological Maturation. Child Dev. 2010, 81, 115. [Google Scholar] [CrossRef]
- de Asis-Cruz, J.; Krishnamurthy, D.; Zhao, L.; Kapse, K.; Vezina, G.; Andescavage, N.; Quistorff, J.; Lopez, C.; Limperopoulos, C. Association of Prenatal Maternal Anxiety with Fetal Regional Brain Connectivity. JAMA Netw. Open 2020, 3, e2022349. [Google Scholar] [CrossRef]
- Garrett, D.D.; Kovacevic, N.; McIntosh, A.R.; Grady, C.L. The Importance of Being Variable. J. Neurosci. 2011, 31, 4496–4503. [Google Scholar] [CrossRef]
- Rogers, C.E.; Lean, R.E.; Wheelock, M.D.; Smyser, C.D. Aberrant Structural and Functional Connectivity and Neurodevelopmental Impairment in Preterm Children. J. Neurodev. Disord. 2018, 10, 38. [Google Scholar] [CrossRef] [PubMed]
- Evans, T.M.; Kochalka, J.; Ngoon, T.J.; Wu, S.S.; Qin, S.; Battista, C.; Menon, V. Brain Structural Integrity and Intrinsic Functional Connectivity Forecast 6 Year Longitudinal Growth in Children’s Numerical Abilities. J. Neurosci. 2015, 35, 11743–11750. [Google Scholar] [CrossRef] [PubMed]
- Barch, D.M.; Belden, A.C.; Tillman, R.; Whalen, D.; Luby, J.L. Early Childhood Adverse Experiences, Inferior Frontal Gyrus Connectivity, and the Trajectory of Externalizing Psychopathology. J. Am. Acad. Child Adolesc. Psychiatry 2018, 57, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Zhao, Z.; Cui, H.; Zhang, T.; Zhao, L.; He, Z.; Liu, H.; Guo, L.; Liu, T.; Becker, B.; et al. Temporal Variability of Cortical Gyral-Sulcal Resting State Functional Activity Correlates with Fluid Intelligence. Front. Neural Circuits 2019, 13, 36. [Google Scholar] [CrossRef] [PubMed]
- Stevens, W.D.; Spreng, R.N. Resting-State Functional Connectivity MRI Reveals Active Processes Central to Cognition. Wiley Interdiscip. Rev. Cogn. Sci. 2014, 5, 233–245. [Google Scholar] [CrossRef]
- Vidaurre, D.; Llera, A.; Smith, S.M.; Woolrich, M.W. Behavioural Relevance of Spontaneous, Transient Brain Network Interactions in FMRI. Neuroimage 2021, 229, 117713. [Google Scholar] [CrossRef]
- Thomason, M.E.; Hect, J.L.; Waller, R.; Curtin, P. Interactive Relations between Maternal Prenatal Stress, Fetal Brain Connectivity, and Gestational Age at Delivery. Neuropsychopharmacology 2021, 46, 1839–1847. [Google Scholar] [CrossRef]
- Han, L.; Bai, H.; Lun, B.; Li, Y.; Wang, Y.; Ni, Q. The Prevalence of Fear of Childbirth and Its Association with Intolerance of Uncertainty and Coping Styles among Pregnant Chinese Women during the COVID-19 Pandemic. Front. Psychiatry 2022, 13, 935760. [Google Scholar] [CrossRef]
- Anderson, M.R.; Salisbury, A.L.; Uebelacker, L.A.; Abrantes, A.M.; Battle, C.L. Stress, Coping and Silver Linings: How Depressed Perinatal Women Experienced the COVID-19 Pandemic. J. Affect. Disord. 2022, 298, 329–336. [Google Scholar] [CrossRef]
- Giurgescu, C.; Penckofer, S.; Maurer, M.C.; Bryant, F.B. Impact of Uncertainty, Social Support, and Prenatal Coping on the Psychological Well-Being of High-Risk Pregnant Women. Nurs. Res. 2006, 55, 356–365. [Google Scholar] [CrossRef]
- Yadav, A.K.; Jena, P.K. Explaining Changing Patterns and Inequalities in Maternal Healthcare Services Utilization in India. J. Public Aff. 2022, 22, e2570. [Google Scholar] [CrossRef]
- Yadav, A.K.; Jena, P.K. Maternal Health Outcomes of Socially Marginalized Groups in India. Int. J. Health Care Qual. Assur. 2020, 33, 172–188. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Total | Range/Percentage of Total |
|---|---|---|
| Total Participants | 45 | |
| Sex of fetus | 18 | |
| Female | 18 | 40% |
| Male | 20 | 44.5% |
| Unknown | 7 | 15.5% |
| 45 | ||
| Total MRI’s | ||
| GA, median (range), wk. | ||
| At MRI | 31.57 | (22.57 to 38.42) |
| At Birth | 39.14 | (33 to 41.86) |
| Maternal age at MRI, median, yr. | 32 | (18 to 43) |
| Maternal parity | ||
| Primiparous | 18 | 40% |
| Multiparous | 22 | 49% |
| Unknown | 5 | 11% |
| Infant Weight, median, kg | 3.54 | |
| Caucasian | 8 | 18% |
| Hispanic or Latino | 28 | 62% |
| Asian/Pacific Islander | 7 | 16% |
| African American | 1 | 2% |
| Middle Eastern | 0 | |
| Other or unknown | 1 | 2% |
| Volume (cm3) | COVID Stress Score | COI Nationally Normed Value | COI Stress Interaction | |||
|---|---|---|---|---|---|---|
| β (CI) | p-Value | β (CI) | p-Value | β (CI) | p-Value | |
| Brainstem | 3.89 × 100, (−7.62 × 101, 8.40 × 101) | 0.97 | −2.81 × 10−1, (−1.41 × 101, 1.35 × 101) | 0.99 | 4.06 × 10−1, (−1.18 × 100, 1.99 × 100) | 0.86 |
| Cerebellum | 1.54 × 102, (−4.84 × 101, 3.56 × 102) | 0.61 | 3.28 × 101, (4.13 × 10−1, 6.52 × 101) | 0.49 | −1.95 × 100, (−5.79 × 100, 1.89 × 100) | 0.73 |
| Cortical Plate | −7.33 × 102, (−1.35 × 103, −1.18 × 102) | 0.42 | −3.78 × 100, (−1.59 × 102, 1.52 × 102) | 0.99 | 1.23 × 101, (−1.43 × 100, 2.60 × 101) | 0.55 |
| Deep Grey | 1.93 × 101, (−1.83 × 102, 2.22 × 102) | 0.95 | 2.76 × 100, (−3.17 × 101, 3.73 × 101) | 0.96 | 1.65 × 100, (−2.28 × 100, 5.58 × 100) | 0.78 |
| Extra Axial CSF | −7.29 × 102, (−1.74 × 103, 2.81 × 102) | 0.63 | −9.28 × 101, (−3.06 × 102, 1.21 × 102) | 0.77 | 1.76 × 101, (−5.28 × 100, 4.04 × 101) | 0.60 |
| Hippocampus amygdala complex | −1.31 × 100, (−2.72 × 101, 2.46 × 101) | 0.97 | −7.62 × 10−1, (−6.21 × 100, 4.69 × 100) | 0.92 | 2.17 × 10−1, (−3.33 × 10−1, 7.68 × 10−1) | 0.79 |
| Intra ventricular CSF | 2.59 × 101, (−7.98 × 101, 1.32 × 102) | 0.87 | 1.23 × 101, (−1.15 × 101, 3.60 × 101) | 0.73 | −5.07 × 10−1, (−2.81 × 100, 1.79 × 100) | 0.88 |
| White Matter | −5.17 × 102, (−1.69 × 103, 6.58 × 102) | 0.77 | −8.47 × 101, (−2.99 × 102, 1.30 × 102) | 0.79 | 1.19 × 101, (−1.25 × 101, 3.63 × 101) | 0.74 |
| Total Brain Volume | −2.51 × 103, (−6.81 × 103, 1.80 × 103) | 0.69 | −2.27 × 102, (−1.05 × 103, 5.96 × 102) | 0.85 | 5.92 × 101, (−3.03 × 101, 1.49 × 102) | 0.66 |
| Volume Normalized by Total Brain Volume | COVID Stress | Overall COI by Zip Code | COVID Stress and COI Interaction | |||
|---|---|---|---|---|---|---|
| β (CI) | p-Value | β (CI) | p-Value | β (CI) | p-Value | |
| Brainstem | 1.30 × 10−4, (9.00 × 10−5, 1.70 × 10−4) | 0.03 * | 1.00 × 10−5, (0.00 × 100, 2.00 × 10−5) | 0.65 | 0.00 × 100, (0.00 × 100, 0.00 × 100) | 0.31 |
| Cerebellum | 3.40 × 10−4, (1.50 × 10−4, 5.40 × 10−4) | 0.24 | 7.00 × 10−5, (4.00 × 10−5, 1.10 × 10−4) | 0.12 | −1.00 × 10−5, (−1.00 × 10−5, 0.00 × 100) | 0.26 |
| Cortical Plate | −1.42 × 10−3, (−2.10 × 10−3, −7.40 × 10−4) | 0.16 | −1.00 × 10−5, (−2.20 × 10−4, 2.00 × 10−4) | 0.97 | 1.00 × 10−5, (−1.00 × 10−5, 3.00 × 10−5) | 0.64 |
| Deep Grey | 1.90 × 10−4, (3.00 × 10−5, 3.60 × 10−4) | 0.42 | 2.00 × 10−5, (−3.00 × 10−5, 6.00 × 10−5) | 0.82 | 0.00 × 100, (0.00 × 100, 1.00 × 10−5) | 0.90 |
| Extra Axial CSF | 1.10 × 10−4, (−7.00 × 10−5, 2.80 × 10−4) | 0.68 | −5.00 × 10−5, (−1.20 × 10−4, 2.00 × 10−5) | 0.61 | 0.00 × 100, (0.00 × 100, 1.00 × 10−5) | 0.60 |
| Hippocampus amygdala complex | 4.00 × 10−5, (2.00 × 10−5, 6.00 × 10−5) | 0.22 | 0.00 × 100, (−1.00 × 10−5, 1.00 × 10−5) | 0.94 | 0.00 × 100, (0.00 × 100, 0.00 × 100) | 0.99 |
| Intra ventricular CSF | 1.20 × 10−4, (−4.00 × 10−5, 2.80 × 10−4) | 0.61 | 5.00 × 10−5, (−1.00 × 10−5, 1.00 × 10−4) | 0.55 | 0.00 × 100, (−1.00 × 10−5, 0.00 × 100) | 0.64 |
| White Matter | 3.80 × 10−4, (−1.60 × 10−4, 9.20 × 10−4) | 0.63 | −3.00 × 10−5, (−1.80 × 10−4, 1.20 × 10−4) | 0.89 | −1.00 × 10−5, (−3.00 × 10−5, 0.00 × 100) | 0.62 |
| COVID Stress | Overall COI by Zip Code | |||
|---|---|---|---|---|
| β (CI) | p-Value | β (CI) | p-Value | |
| Temporal mean of BOLD Signal | 135.369, (−509.52, 38.1) | 0.09 | 316.9634, (−604.97, 1238.9) | 0.49 |
| Temporal variability of BOLD Signal | −113.94, (−215.18, −12. 71) | 0.03 * | −19.5173, (−360.388, 321.354) | 0.91 |
| Variance of framewise mean BOLD signal | −5336.81, (−2.87 × 104, 1.81 × 104) | 0.65 | −5191.57, (−8.4 × 104, 7.36 × 104) | 0.9 |
| Kurtosis of framewise mean BOLD signal | 0.329, (−0.144, 0.802) | 0.17 | 0.457, (−1.135, 2.049) | 0.57 |
| Autocorrelation of framewise mean BOLD | −6.828 × 106, (−1.41 × 107, 4.89 × 105) | 0.07 | 1.005 × 107, (−1.46 × 107, 3.47 × 107) | 0.41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajagopalan, V.; Reynolds, W.T.; Zepeda, J.; Lopez, J.; Ponrartana, S.; Wood, J.; Ceschin, R.; Panigrahy, A. Impact of COVID-19 Related Maternal Stress on Fetal Brain Development: A Multimodal MRI Study. J. Clin. Med. 2022, 11, 6635. https://doi.org/10.3390/jcm11226635
Rajagopalan V, Reynolds WT, Zepeda J, Lopez J, Ponrartana S, Wood J, Ceschin R, Panigrahy A. Impact of COVID-19 Related Maternal Stress on Fetal Brain Development: A Multimodal MRI Study. Journal of Clinical Medicine. 2022; 11(22):6635. https://doi.org/10.3390/jcm11226635
Chicago/Turabian StyleRajagopalan, Vidya, William T. Reynolds, Jeremy Zepeda, Jeraldine Lopez, Skorn Ponrartana, John Wood, Rafael Ceschin, and Ashok Panigrahy. 2022. "Impact of COVID-19 Related Maternal Stress on Fetal Brain Development: A Multimodal MRI Study" Journal of Clinical Medicine 11, no. 22: 6635. https://doi.org/10.3390/jcm11226635
APA StyleRajagopalan, V., Reynolds, W. T., Zepeda, J., Lopez, J., Ponrartana, S., Wood, J., Ceschin, R., & Panigrahy, A. (2022). Impact of COVID-19 Related Maternal Stress on Fetal Brain Development: A Multimodal MRI Study. Journal of Clinical Medicine, 11(22), 6635. https://doi.org/10.3390/jcm11226635