

Upper-Arm SBP Decline Associated with Repeated Cuff-Oscillometric Inflation Significantly Correlated with the Arterial Stiffness Index


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. AVI and API
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
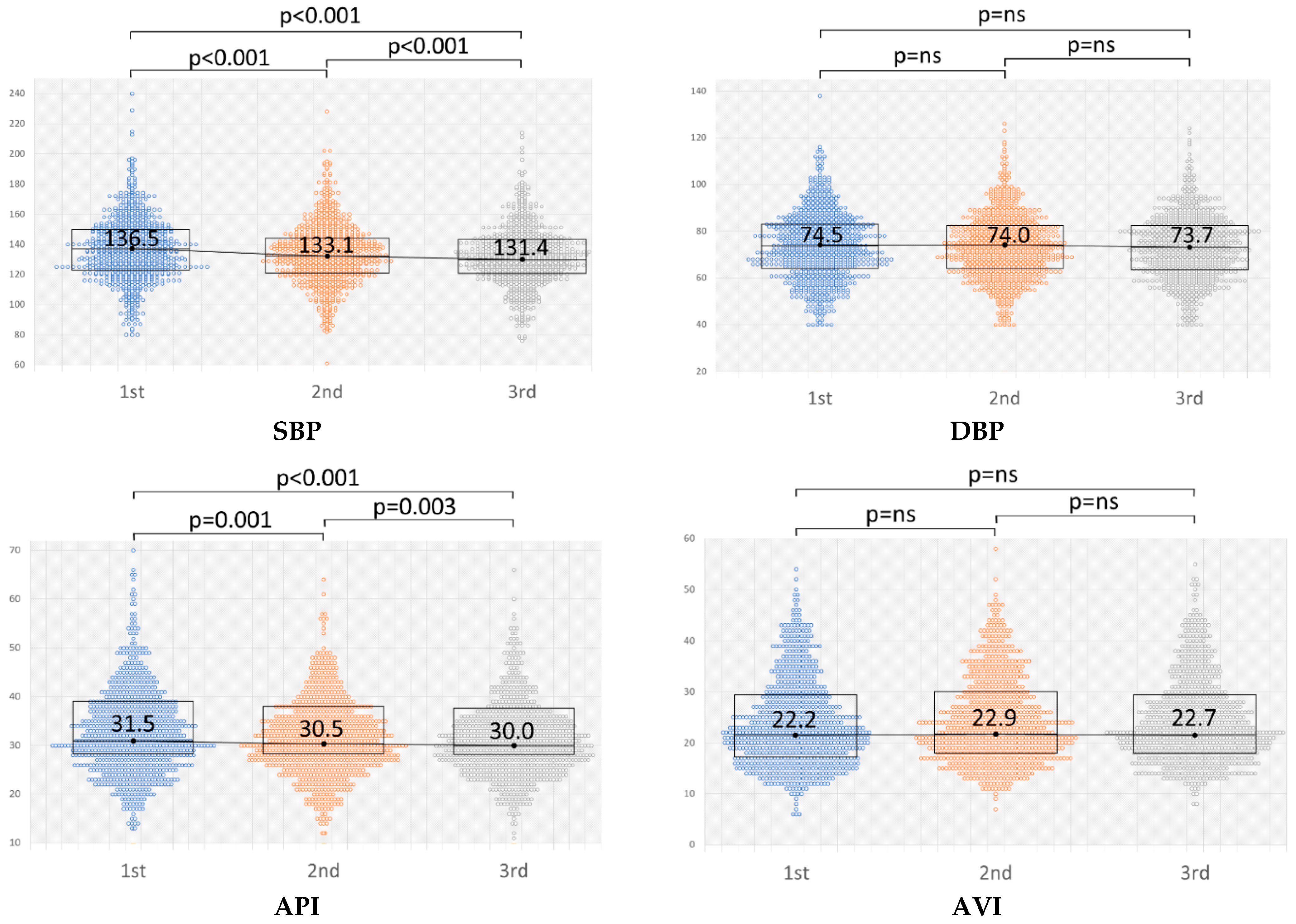
3.2. Changes in BP, API, and AVI with Repeated Measurements
3.3. Regression Analysis of the Relationship between Novel Vascular Indices and Clinical Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, H.Y.; Oh, B.H. Aging and arterial stiffness. Circ. J. 2010, 74, 2257–2262. [Google Scholar] [CrossRef] [PubMed]
- Singhal, A. Endothelial dysfunction: Role in obesity-related disorders and the early origins of CVD. Proc. Nutr. Soc. 2005, 64, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Nabel, E.G.; Braunwald, E. A tale of coronary artery disease and myocardial infarction. N. Engl. J. Med. 2012, 366, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Rajaram, V.; Pandhya, P.; Patel, S.; Peter, M.M.; Goldin, M. Role of surrogate markers in assessing patients with diabetes mellitus and the metabolic syndrome and in evaluating lipid-lowering therapy. Am. J. Cardiol. 2004, 93, 32–48. [Google Scholar] [CrossRef] [PubMed]
- Birmpili, P.; Johal, A.; Li, Q.; Waton, S.; Chetter, I.; Boyle, J.R.; Cromwell, D. Factors associated with delays in revascularization in patients with chronic limb-threatening ischaemia: Population-based cohort study. Br. J. Surg. 2021, 108, 951–959. [Google Scholar] [CrossRef]
- Falk, E. Pathogenesis of Atherosclerosis Viewpoint. J. Am. Coll. Cardiol. 2006, 47 (Suppl. 8), C7–C12. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Kanayama, N.; Nakayama, Y. Current status, issues and future prospects of personalized medicine for each disease. J. Pers. Med. 2022, 12, 444. [Google Scholar] [CrossRef]
- Liang, F.; Takagi, S.; Himeno, R.; Liu, H. A computational model of the cardiovascular system coupled with an upper-arm oscillometric cuff and its application to studying the suprasystolic cuff oscillation wave, concerning its value in assessing arterial stiffness. Comput. Methods Biomech. Biomed. Eng. 2013, 16, 141–145. [Google Scholar] [CrossRef]
- Komine, H.; Asai, Y.; Yokoi, T.; Yoshizawa, M. Non-invasive assessment of arterial stiffness using oscillometric blood pressure measurement. Biomed. Eng. Online 2012, 11, 6. [Google Scholar] [CrossRef]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redón, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A. 2013 ESH/ESC guidelines for the management of arterial hypertension: The task force for the management of arterial hypertension of the European society of hypertension (ESH) and of the European society of cardiology (ESC). Eur. Heart J. 2013, 34, 2159–2219. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W. ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American college of cardiology/American heart association task force on clinical practice guidelines. Hypertension 2017, 71, e13. [Google Scholar] [PubMed]
- Umemura, S.; Arima, H.; Arima, S.; Asayama, K.; Dohi, Y.; Hirooka, Y.; Horio, T.; Hoshide, S.; Ikeda, S.; Ishimitsu, T.; et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019). Hypertens. Res. 2019, 42, 1235–1481. [Google Scholar] [CrossRef] [PubMed]
- Sueta, D.; Yamamoto, E.; Tanaka, T.; Hirata, Y.; Sakamoto, K.; Tsujita, K. The accuracy of central blood pressure waveform by novel mathematical transformation of non-invasive measurement. Int. J. Cardiol. 2015, 189, 244–246. [Google Scholar] [CrossRef] [PubMed]
- Sasaki-Nakashima, R.; Kino, T.; Chen, L.; Doi, H.; Ishigami, T. Successful prediction of cardiovascular risk by new non-invasive vascular indexes using suprasystolic cuff oscillometric waveform analysis. J. Cardiol. 2017, 69, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Doi, H.; Ishigami, T.; Nakashima-Sasaki, R.; Kino, T.; Chen, L. New non-invasive indexes of arterial stiffness are significantly correlated with severity and complexity of coronary atherosclerosis. Clin. Exp. Hypertens. 2018, 41, 187–193. [Google Scholar] [CrossRef]
- Kawabe, H.; Saito, I.; Saruta, T. Influence of repeated measurement on one occasion, on successive days, and on workdays on home blood pressure values. Clin. Exp. Hypertens. 2005, 27, 215–222. [Google Scholar] [CrossRef]
- Eguchi, K.; Kuruvilla, S.; Ogedegbe, G.; Gerin, W.; Schwartz, J.E.; Pickering, T.G. What is the optimal interval between successive home blood pressure readings using an automated oscillometric device? J. Hypertens. 2009, 27, 1172. [Google Scholar] [CrossRef]
- Imamura, M.; Asayama, K.; Sawanoi, Y.; Shiga, T.; Saito, K.; Ohkubo, T. Effects of measurement intervals on the values of repeated auscultatory blood pressure measurements. Clin. Exp. Hypertens. 2020, 42, 105–109. [Google Scholar] [CrossRef]
- van Loo, J.M.; Peer, P.G.; Thien, T.A. Twenty-five minutes between blood pressure readings: The influence on prevalence rates of isolated systolic hypertension. J. Hypertens. 1986, 4, 631–635. [Google Scholar] [CrossRef]
- Reeves, R.A. The rational clinical examination: Does this patient have hypertension? How to measure blood pressure. JAMA 1995, 273, 1211–1218. [Google Scholar] [CrossRef]
- Okamoto, M.; Nakamura, F.; Musha, T.; Kobayashi, Y. Association between novel arterial stiffness indices and risk factors of cardiovascular disease. BMC Cardiovasc. Disord. 2016, 16, 211. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yin, P.; Xu, Z.; Xie, Y. Non-Invasive Assessment of Early Atherosclerosis Based on New Arterial Stiffness Indices Measured with an Upper-Arm Oscillometric Device. Tohoku J. Exp. Med. 2017, 241, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, S.; Tomiyama, H.; Kimura, K.; Matsumoto, C.; Shiina, K.; Yamashina, A. Comparison of the clinical significance of single cuff-based arterial stiffness parameters with that of the commonly used parameters. J. Cardiol. 2017, 69, 678–683. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kobayashi, R.; Iwanuma, S.; Ohashi, N.; Hashiguchi, T. New indices of arterial stiffness measured with an upper-arm oscillometric device in active versus inactive women. Physiol. Rep. 2018, 6, e13574. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Male (n = 148) | Female (n = 88) | Total (n = 236) | |
|---|---|---|---|
| Age (years) | 68.0 ± 12.1 | 68.2 ± 12.1 | 68.1 ± 12.1 |
| Hypertension (%) | 99 (66.9) | 59 (67.1) | 158 (67.0) |
| Diabetes (%) | 38 (25.7) | 10 (11.4) | 48 (20.3) |
| Dyslipidemia (%) | 70 (47.3) | 39 (44.3) | 109 (46.2) |
| IHD (%) | 28 (18.9) | 6 (6.8) | 34 (14.4) |
| ASO (%) | 11 (7.4) | 4 (4.6) | 15 (6.4) |
| VHD (%) | 11 (7.4) | 10 (11.4) | 21 (8.9) |
| OMI (%) | 12 (8.1) | 4 (4.6) | 16 (6.8) |
| CHF (%) | 20 (13.5) | 10 (11.4) | 30 (12.7) |
| Cardiomyopathy (%) | 5 (3.4) | 4 (4.6) | 9 (3.8) |
| PH (%) | 1 (0.7) | 3 (3.4) | 4 (1.7) |
| AF (%) | 29 (19.6) | 7 (8.0) | 36 (15.3) |
| PM/ICD (%) | 2 (1.4) | 0 (0) | 2 (0.85) |
| COPD (%) | 5 (3.4) | 0 (0) | 5 (2.1) |
| Smoking | |||
| Current (%) | 24 (16.2) | 7 (8.0) | 31 (13.2) |
| Past (%) | 61 (41.2) | 6 (6.8) | 67 (28.4) |
| Never (%) | 63 (42.6) | 75 (85.2) | 138 (58.4) |
| Laboratory data | |||
| Creatinine (mg/dL) | 1.12 ± 1.20 | 0.73 ±0.46 | 0.98 ± 1.01 |
| eGFR (mL/min/1.73 m2) | 67.45 ± 21.96 | 72.43 ± 26.34 | 69.26 ± 23.72 |
| Uric acid (mg/dL) | 5.90 ± 1.46 | 5.01 ± 1.35 | 5.58 ± 1.49 |
| Plasma glucose (mg/dL) | 130.29 ± 34.35 | 116.92 ± 32.07 | 125.84 ± 34.07 |
| HbA1c (%) | 6.10 ± 0.84 | 6.15 ± 1.00 | 6.11 ± 0.89 |
| CRP (mg/dL) | 0.32 ± 0.75 | 0.49 ± 1.25 | 0.38 ± 0.96 |
| TG (mg/dL) | 143.63 ± 80.09 | 152.28 ± 95.43 | 146.49 ± 85.35 |
| HDL-C (mg/dL) | 59.10 ± 16.30 | 66.58 ± 22.38 | 61.54 ± 18.79 |
| LDL-C (mg/dL) | 105.27 ± 34.80 | 115.47 ± 35.78 | 108.85 ± 35.38 |
| T-Cho (mg/dL) | 181.37 ± 37.64 | 204.55 ± 44.24 | 189.29 ± 41.36 |
| BNP (pg/mL) | 121.06 ± 230.01 | 62.6 ± 106.4 | 99.93 ± 196.27 |
| Male (n = 148) | Female (n = 88) | Total (n = 236) | |
|---|---|---|---|
| RAS inhibitors (%) | 79 (53.4) | 42 (47.7) | 121 (51.3) |
| Ca antagonists (%) | 72 (48.7) | 47 (53.4) | 119 (50.4) |
| β-blockers (%) | 48 (32.4) | 23 (26.1) | 71 (30.1) |
| Diuretics (%) | 32 (21.6) | 22 (25.0) | 54 (22.9) |
| α-blockers (%) | 1 (0.7) | 1 (1.1) | 2 (0.9) |
| Nitrites (%) | 16 (10.8) | 8 (9.1) | 24 (10.2) |
| Biguanides (%) | 7 (4.7) | 3 (3.4) | 10 (4.2) |
| Statins (%) | 60 (40.5) | 39 (44.3) | 99 (42.0) |
| Bezafibrates (%) | 7 (4.7) | 2 (2.3) | 9 (3.8) |
| EPA (%) | 6 (4.1) | 1 (1.1) | 7 (3.0) |
| Ezetimibe (%) | 6 (4.1) | 3 (3.4) | 9 (3.8) |
| Sulfonylureas (%) | 11 (7.4) | 1 (1.1) | 12 (5.1) |
| α-glucosidase inhibitors (%) | 13 (8.8) | 0 (0) | 13 (4.3) |
| Thiazolidine (%) | 6 (4.1) | 1 (1.1) | 7 (3.0) |
| DPP-4 inhibitors (%) | 17 (11.5) | 6 (6.8) | 23 (9.8) |
| GLP-1 analogs (%) | 2 (1.4) | 0 (0) | 2 (0.9) |
| Insulin (%) | 8 (5.4) | 2 (2.3) | 10 (4.2) |
| Aspirin (%) | 46 (31.1) | 18 (20.5) | 64 (27.1) |
| Thienopyridine (%) | 15 (10.1) | 3 (3.4) | 18 (7.6) |
| Cilostazol (%) | 6 (4.1) | 4 (4.6) | 10 (4.2) |
| Sarpogrelate (%) | 1 (0.7) | 0 (0) | 1 (0.4) |
| Dipyridamole (%) | 0 (0) | 0 (0) | 0 (0) |
| Prostaglandin (%) | 3 (2.0) | 1 (1.1) | 4 (1.7) |
| Male (n = 148) | Female (n = 88) | Total (n = 236) | |
|---|---|---|---|
| SBP (mmHg) | 131.9 ± 19.8 | 135.2 ± 23.4 | 133.1 ± 21.2 |
| DBP (mmHg) | 75.3 ± 34.4 | 71.7 ± 14.4 | 73.9 ± 13.6 |
| AVI | 22.9 ± 8.4 | 25.4 ± 7.9 | 23.8 ± 8.3 |
| API | 29.3 ± 6.9 | 34.2 ± 8.5 | 31.1 ± 7.9 |
| Pulse rate (/min) | 73.5 ± 12.4 | 75.2 ± 14.4 | 74.1 ± 13.2 |
| Measurements of AVI and API | |||
| Total number | 1545 | 907 | 2452 |
| Total visits | 300 | 496 | 796 |
| Per visit per person | 3.02 | 3.12 | 3.04 |
| First Measurement | Second Measurement | Third Measurement | |
|---|---|---|---|
| SBP | 136.6± 20.4 | 133.6 ± 19.8 | 131.9 ± 18.2 |
| DBP | 74.5 ± 13.8 | 74.0 ± 12.7 | 73.7 ± 13.0 |
| AVI | 23.8 ± 8.2 | 24.1 ± 7.8 | 24.2 ± 7.7 |
| API | 32.5 ± 8.8 | 31.1 ± 6.5 | 30.5 ± 6.4 |
| Independent Variables | Standardized Regression Estimate | 95%CI | p | |
|---|---|---|---|---|
| Sex | 0.0261 | 0.0081 | 0.0440 | 0.005 * |
| Creatinine | −0.0058 | −0.0134 | 0.0019 | 0.14 |
| Independent Variables | Standardized Regression Estimate | 95%CI | p | |
|---|---|---|---|---|
| Age | −0.0020 | −0.0038 | −0.0003 | 0.020 * |
| Diabetes | −0.0578 | −0.1105 | −0.0050 | 0.032 * |
| Sex | 0.0248 | −0.0200 | 0.0695 | 0.276 |
| Creatinine | −0.0189 | −0.0378 | −0.00001 | 0.050 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawaura, N.; Nakashima-Sasaki, R.; Doi, H.; Uchida, K.; Sugawara, T.; Saigo, S.; Abe, K.; Arakawa, K.; Tamura, K.; Hibi, K.; et al. Upper-Arm SBP Decline Associated with Repeated Cuff-Oscillometric Inflation Significantly Correlated with the Arterial Stiffness Index. J. Clin. Med. 2022, 11, 6455. https://doi.org/10.3390/jcm11216455
Kawaura N, Nakashima-Sasaki R, Doi H, Uchida K, Sugawara T, Saigo S, Abe K, Arakawa K, Tamura K, Hibi K, et al. Upper-Arm SBP Decline Associated with Repeated Cuff-Oscillometric Inflation Significantly Correlated with the Arterial Stiffness Index. Journal of Clinical Medicine. 2022; 11(21):6455. https://doi.org/10.3390/jcm11216455
Chicago/Turabian StyleKawaura, Noriyuki, Rie Nakashima-Sasaki, Hiroshi Doi, Kotaro Uchida, Takuya Sugawara, Sae Saigo, Kaito Abe, Kentaro Arakawa, Koichi Tamura, Kiyoshi Hibi, and et al. 2022. "Upper-Arm SBP Decline Associated with Repeated Cuff-Oscillometric Inflation Significantly Correlated with the Arterial Stiffness Index" Journal of Clinical Medicine 11, no. 21: 6455. https://doi.org/10.3390/jcm11216455
APA StyleKawaura, N., Nakashima-Sasaki, R., Doi, H., Uchida, K., Sugawara, T., Saigo, S., Abe, K., Arakawa, K., Tamura, K., Hibi, K., & Ishigami, T. (2022). Upper-Arm SBP Decline Associated with Repeated Cuff-Oscillometric Inflation Significantly Correlated with the Arterial Stiffness Index. Journal of Clinical Medicine, 11(21), 6455. https://doi.org/10.3390/jcm11216455