The Management of Dry Eye Disease: Proceedings of Italian Dry Eye Consensus Group Using the Delphi Method

 ,
,  , , ,
, , ,  , , , , , , ,
, , , , , , ,  , , , and add
Show full author list
, , , and add
Show full author list
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Methods
3. Results
3.1. Managing Dry Eye Disease and Inflammation over Time
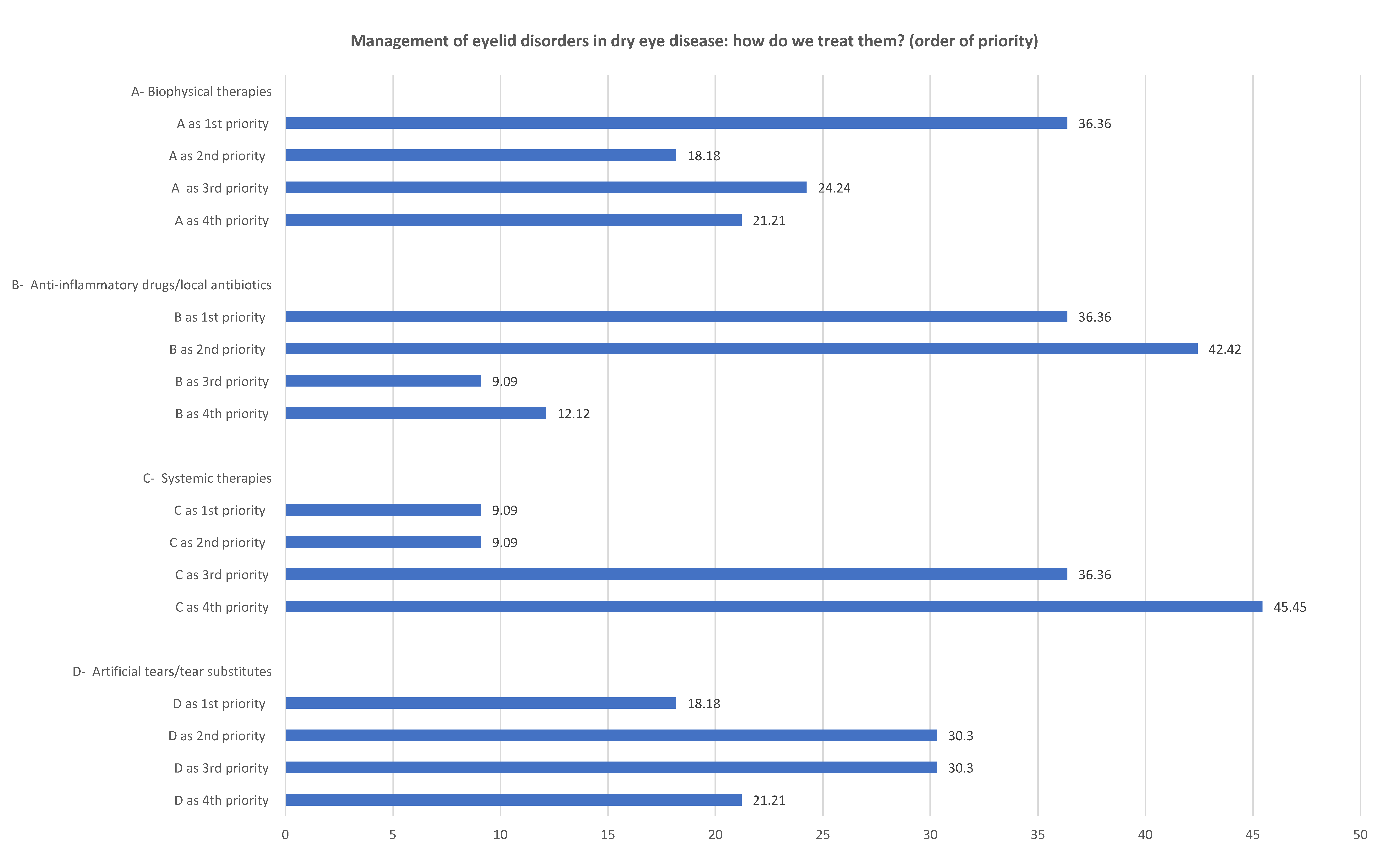
3.2. Managing Eyelid Disorders in Dry Eye Disease
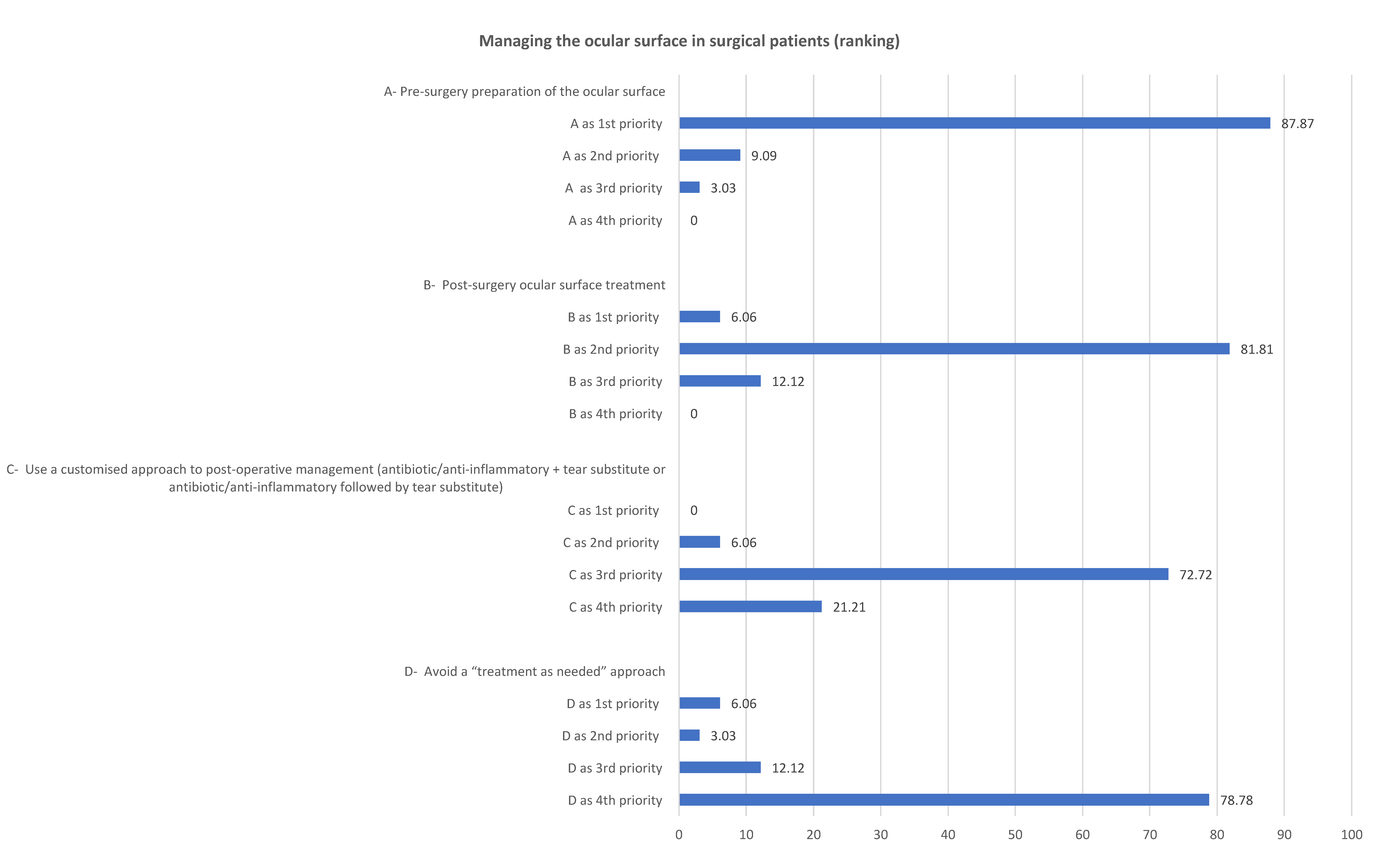
3.3. Managing the Ocular Surface in Surgical Patients
3.4. Improving Patient Satisfaction, Collaboration and Treatment Adherence
4. Discussion
Funding
Conflicts of Interest
References
- Anonymous. Research in dry eye: Report of the research subcommittee of the International Dry Eye WorkShop (2007). Ocul. Surf. 2007, 5, 179–193. [Google Scholar] [CrossRef]
- Lemp, M.A. Report of the National Eye Institute/Industry workshop on clinical trials in dry eyes. CLAO J. 1995, 21, 221–232. [Google Scholar]
- Anonymous. 2007 Report of the International Dry Eye WorkShop (DEWS). Ocul. Surf. 2007, 5, 1–204. [Google Scholar]
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II definition and classification report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef]
- Nichols, K.K. Patient-reported symptoms in dry dye disease. Ocul. Surf. 2006, 4, 137–145. [Google Scholar] [CrossRef]
- Friedman, N.J. Impact of dry eye disease and treatment on quality of life. Curr. Opin. Ophthalmol. 2010, 21, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Grubbs, J.R., Jr.; Tolleson-Rinehart, S.; Huynh, K.; Davis, R.M. A review of quality of life measures in dry eye questionnaires. Cornea 2014, 33, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Miljanović, B.; Dana, R.; Sullivan, D.A.; Schaumberg, D.A. Impact of dry eye syndrome on vision-related quality of life. Am. J. Ophthalmol. 2007, 143, 409–415. [Google Scholar] [CrossRef]
- Li, M.; Gong, L.; Sun, X.; Chapin, W.J. Anxiety and depression in patients with dry eye syndrome. Curr. Eye Res. 2011, 36, 1–7. [Google Scholar] [CrossRef]
- Barabino, S.; Labetoulle, M.; Rolando, M.; Messmer, E.M. Understanding symptoms and quality of life in patients with dry eye syndrome. Ocul. Surf. 2016, 14, 365–376. [Google Scholar] [CrossRef]
- Aragona, P.; Giannaccare, G.; Mencucci, R.; Rubino, P.; Cantera, E.; Rolando, M. Modern approach to the treatment of dry eye disease: A P.I.C.A.S.S.O. board review. Br. J. Ophthalmol. 2021, 105, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Aragona, P.; Rolando, M. Towards a dynamic customised therapy for ocular surface dysfunctions. Br. J. Ophthalmol. 2013, 97, 955–960. [Google Scholar] [CrossRef] [PubMed]
- Rolando, M.; Cantera, E.; Mencucci, R.; Rubino, P.; Aragona, P. The correct diagnosis and therapeutic management of tear dysfunction: Recommendations of the P.I.C.A.S.S.O. board. Int. Ophthalmol. 2018, 38, 875–895. [Google Scholar] [CrossRef] [PubMed]
- Aragona, P.; Giannaccare, G.; Rolando, M. Special issue “Managing dry eye disease over time: An Italian consensus conference”. J. Clin. Med. 2022, 11, 2507. [Google Scholar] [CrossRef] [PubMed]
- Pill, J. The Delphi method: Substance, context, a critique and an annotated bibliography. Socio-Econ. Plan. Sci. 1971, 5, 57–71. [Google Scholar] [CrossRef]
- Rowe, G.; Wright, G.; Bolger, F. Delphi: A re-evaluation of research and theory. Technol. Forecast. Soc. Change 1991, 39, 235–251. [Google Scholar] [CrossRef]
- Jones, J.; Hunter, D. Qualitative research: Consensus methods for medical and health services research. BMJ 1995, 311, 376–380. [Google Scholar] [CrossRef]
- van Setten, G.; Labetoulle, M.; Baudouin, C.; Rolando, M. Evidence of seasonality and effects of psychrometry in dry eye disease. Acta Ophthalmol. 2016, 94, 499–506. [Google Scholar] [CrossRef]
- Horwath-Winter, J.; Berghold, A.; Schmut, O.; Floegel, I.; Solhdju, V.; Bodner, E.; Schwantzer, G.; Haller-Schober, E.M. Evaluation of the clinical course of dry eye syndrome. Arch. Ophthalmol. 2003, 121, 1364–1368. [Google Scholar] [CrossRef]
- Lienert, J.P.; Tarko, L.; Uchino, M.; Christen, W.G.; Schaumberg, D.A. Long-term natural history of dry eye disease from the patient’s perspective. Ophthalmology 2016, 123, 425–433. [Google Scholar] [CrossRef]
- Ezuddin, N.S.; Alawa, K.A.; Galor, A. Therapeutic strategies to treat dry eye in an aging population. Drugs Aging 2015, 32, 505–513. [Google Scholar] [CrossRef]
- Kawashima, M.; Uchino, M.; Yokoi, N.; Uchino, Y.; Dogru, M.; Komuro, A.; Sonomura, Y.; Kato, H.; Kinoshita, S.; Tsubota, K. The association of sleep quality with dry eye disease: The Osaka study. Clin. Ophthalmol. 2016, 10, 1015–1021. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Liu, X.; Han, J.; Shao, T.; Wang, Y. Association between sleep quality, mood status, and ocular surface characteristics in patients with dry eye disease. Cornea 2019, 38, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Ning, K.; Zhou, J.; Guo, Y.; Zhang, H.; Zhu, Y.; Zhang, L.; Jia, C.; Chen, Y.; Sol Reinach, P.; et al. Sleep deprivation disrupts the lacrimal system and induces dry eye disease. Exp. Mol. Med. 2018, 50, e451. [Google Scholar] [CrossRef]
- Kasetsuwan, N.; Satitpitakul, V.; Changul, T.; Jariyakosol, S. Incidence and pattern of dry eye after cataract surgery. PLoS ONE 2013, 8, e78657. [Google Scholar] [CrossRef]
- Rosenthal, P.; Borsook, D. Ocular neuropathic pain. Br. J. Ophthalmol. 2016, 100, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Kohlhaas, M. Corneal sensation after cataract and refractive surgery. J. Cataract. Refract. Surg. 1998, 24, 1399–1409. [Google Scholar] [CrossRef]
- Khanal, S.; Tomlinson, A.; Esakowitz, L.; Bhatt, P.; Jones, D.; Nabili, S.; Mukerji, S. Changes in corneal sensitivity and tear physiology after phacoemulsification. Ophthalmic. Physiol. Opt. 2008, 28, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Epitropoulos, A.T.; Matossian, C.; Berdy, G.J.; Malhotra, R.P.; Potvin, R. Effect of tear osmolarity on repeatability of keratometry for cataract surgery planning. J. Cataract. Refract. Surg. 2015, 41, 1672–1677. [Google Scholar] [CrossRef]
- Baudouin, C.; Aragona, P.; Messmer, E.M.; Tomlinson, A.; Calonge, M.; Boboridis, K.G.; Akova, Y.A.; Geerling, G.; Labetoulle, M.; Rolando, M. Role of hyperosmolarity in the pathogenesis and management of dry eye disease: Proceedings of the OCEAN group meeting. Ocul. Surf. 2013, 11, 246–258. [Google Scholar] [CrossRef]
- Cejková, J.; Ardan, T.; Cejka, C.; Luyckx, J. Favorable effects of trehalose on the development of UVB-mediated antioxidant/pro-oxidant imbalance in the corneal epithelium, proinflammatory cytokine and matrix metalloproteinase induction, and heat shock protein 70 expression. Graefes Arch. Clin. Exp. Ophthalmol. 2011, 249, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- Luyckx, J.; Baudouin, C. Trehalose: An intriguing disaccharide with potential for medical application in ophthalmology. Clin. Ophthalmol. 2011, 5, 577–581. [Google Scholar]
- Emanuele, E. Can trehalose prevent neurodegeneration? Insights from experimental studies. Curr. Drug Targets 2014, 15, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zhang, X.; Liu, M.; Zhang, J.; Ye, Y.; Lin, Y.; Luyckx, J.; Qu, J. Trehalose protects against ocular surface disorders in experimental murine dry eye through suppression of apoptosis. Exp. Eye Res. 2009, 89, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Aragona, P.; Colosi, P.; Rania, L.; Colosi, F.; Pisani, A.; Puzzolo, D.; Micali, A. Protective effects of trehalose on the corneal epithelial cells. Sci. World J. 2014, 2014, 717835. [Google Scholar] [CrossRef] [PubMed]
- Iturriaga, G.; Suárez, R.; Nova-Franco, B. Trehalose metabolism: From osmoprotection to signaling. Int. J. Mol. Sci. 2009, 10, 3793–3810. [Google Scholar] [CrossRef]
- Sutu, C.; Fukuoka, H.; Afshari, N.A. Mechanisms and management of dry eye in cataract surgery patients. Curr. Opin. Ophthalmol. 2016, 27, 24–30. [Google Scholar] [CrossRef]
- Tuft, S.; Lakhani, S. Medical management of dry eye disease. Dev. Ophthalmol. 2008, 41, 54–74. [Google Scholar]
- Giannaccare, G.; Scorcia, V. False myths versus medical facts: Ten common misconceptions related to dry eye disease. Biomedicines 2020, 8, 172. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aragona, P.; Giannaccare, G.; Mencucci, R.; Rubino, P.; Cantera, E.; Finocchiaro, C.Y.; Vaccaro, S.; Aiello, F.; Antoniazzi, E.; Barabino, S.; et al. The Management of Dry Eye Disease: Proceedings of Italian Dry Eye Consensus Group Using the Delphi Method. J. Clin. Med. 2022, 11, 6437. https://doi.org/10.3390/jcm11216437
Aragona P, Giannaccare G, Mencucci R, Rubino P, Cantera E, Finocchiaro CY, Vaccaro S, Aiello F, Antoniazzi E, Barabino S, et al. The Management of Dry Eye Disease: Proceedings of Italian Dry Eye Consensus Group Using the Delphi Method. Journal of Clinical Medicine. 2022; 11(21):6437. https://doi.org/10.3390/jcm11216437
Chicago/Turabian StyleAragona, Pasquale, Giuseppe Giannaccare, Rita Mencucci, Pierangela Rubino, Emilia Cantera, Claudia Yvonne Finocchiaro, Sabrina Vaccaro, Francesco Aiello, Elena Antoniazzi, Stefano Barabino, and et al. 2022. "The Management of Dry Eye Disease: Proceedings of Italian Dry Eye Consensus Group Using the Delphi Method" Journal of Clinical Medicine 11, no. 21: 6437. https://doi.org/10.3390/jcm11216437
APA StyleAragona, P., Giannaccare, G., Mencucci, R., Rubino, P., Cantera, E., Finocchiaro, C. Y., Vaccaro, S., Aiello, F., Antoniazzi, E., Barabino, S., Bonini, S., Carlini, G., Chierego, C., Gisoldi, R. A. M. C., Di Zazzo, A., Fasciani, R., Franch, A., Gabbriellini, G., Gagliano, C., ... Rolando, M. (2022). The Management of Dry Eye Disease: Proceedings of Italian Dry Eye Consensus Group Using the Delphi Method. Journal of Clinical Medicine, 11(21), 6437. https://doi.org/10.3390/jcm11216437