
Effect of Bariatric Surgery on Intima Media Thickness: A Systematic Review and Meta-Analysis

 , ,
, ,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Methods
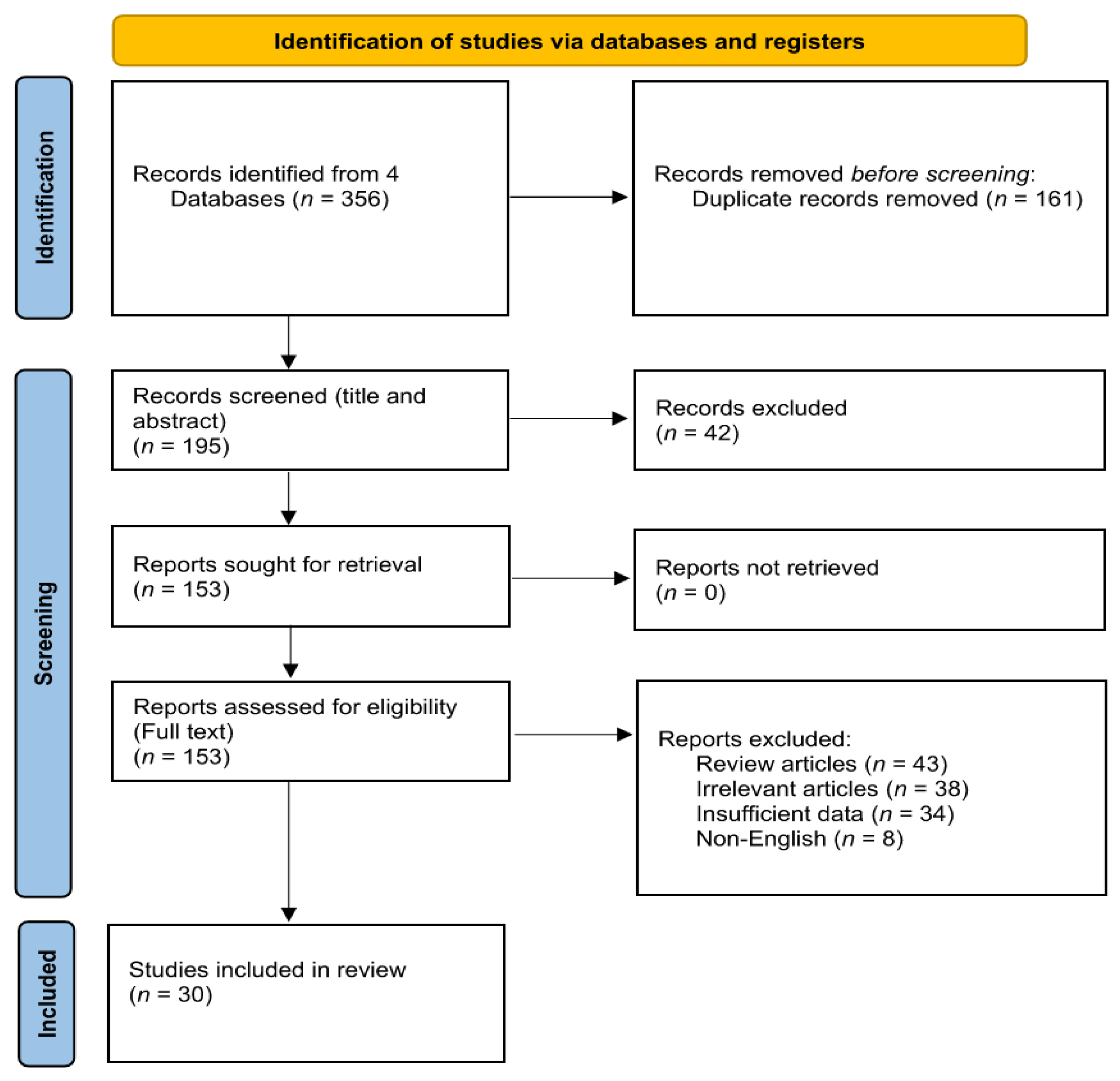
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Quantitative Data Synthesis
2.6. Meta-Regression
2.7. Subgroup Analysis
2.8. Publication Bias
3. Results
3.1. Quality Assessment of the Included Studies
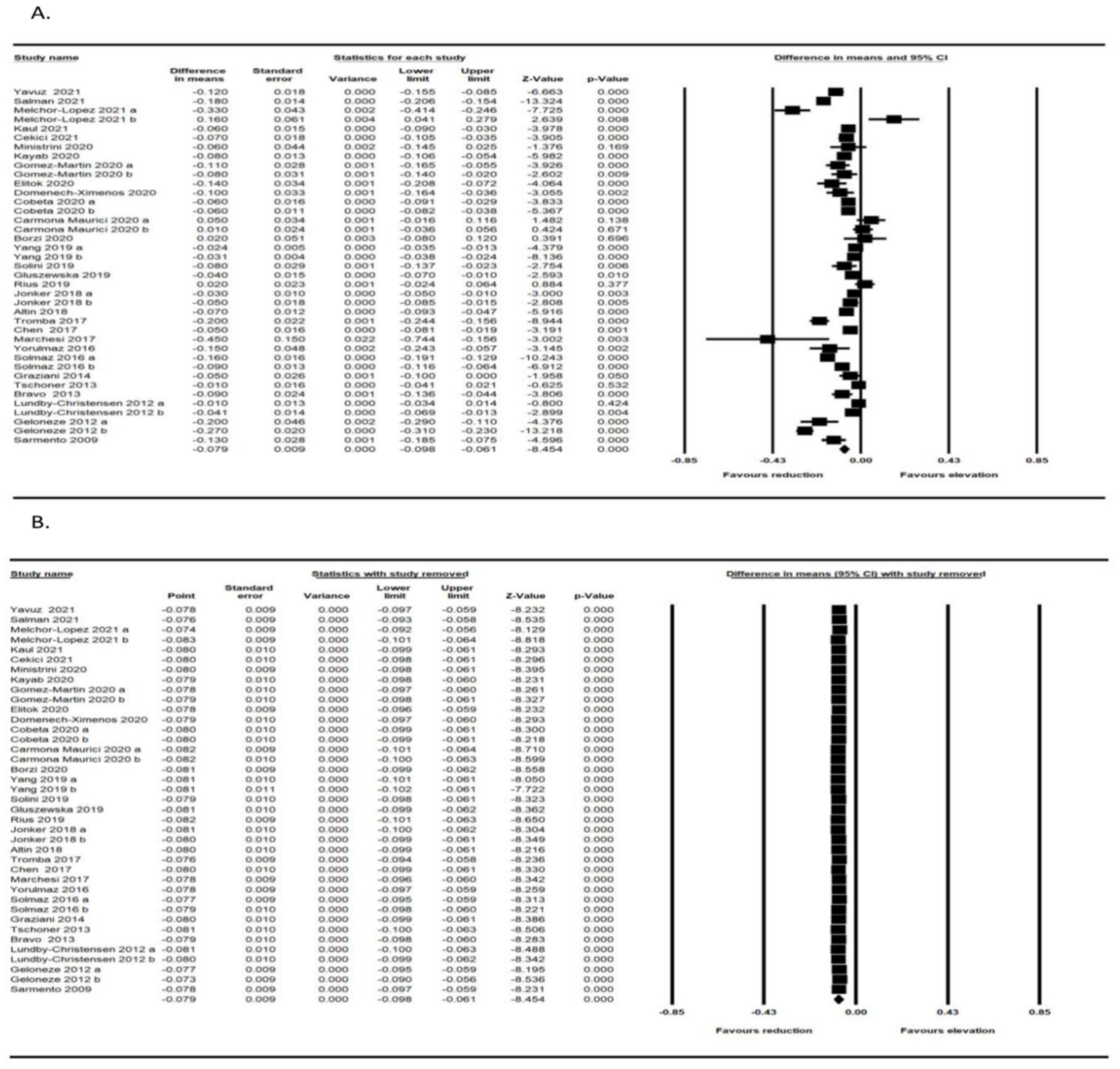
3.2. Effect of Bariatric Surgery on IMT
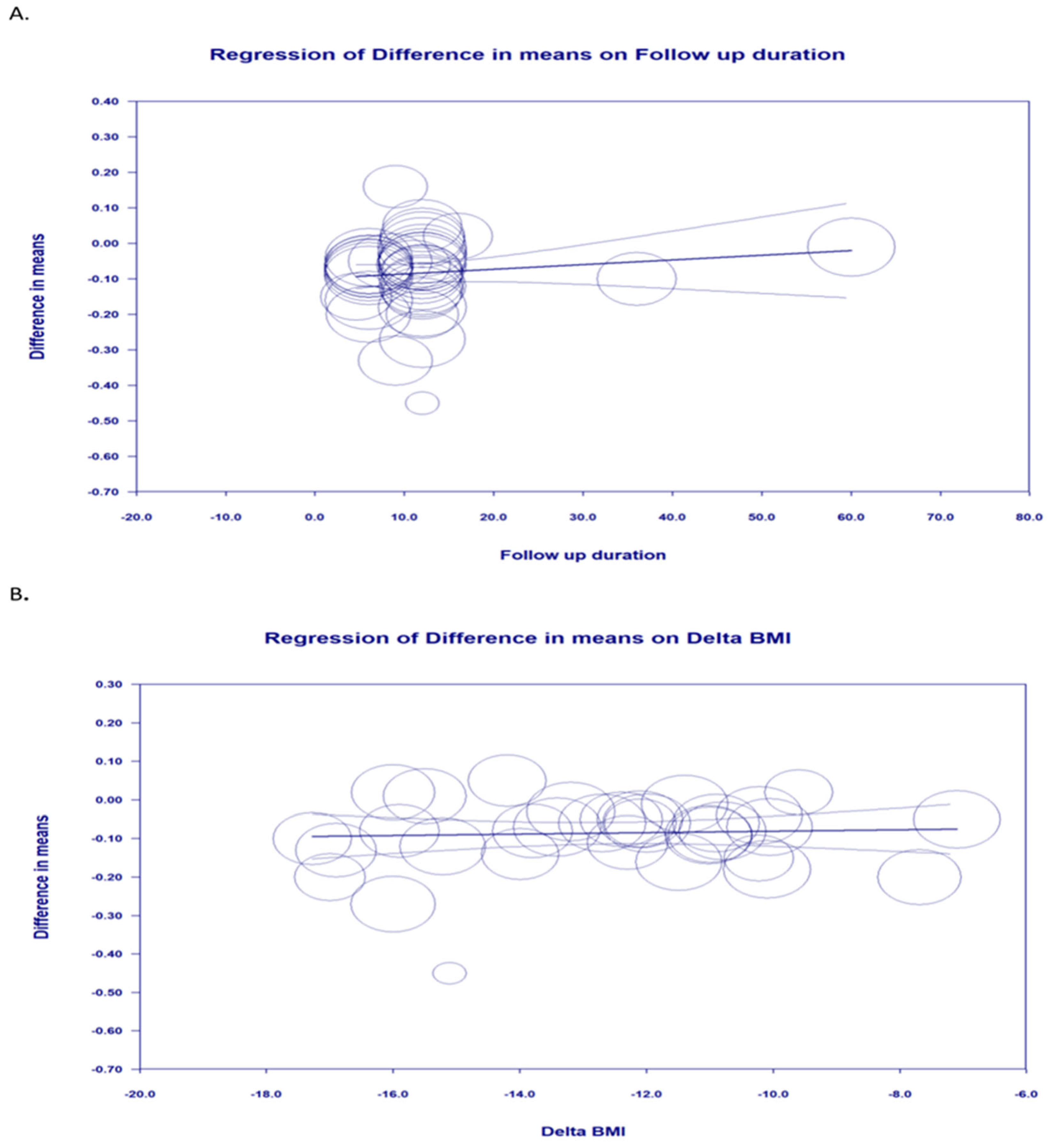
3.3. Meta-Regression
3.4. Subgroup Analysis
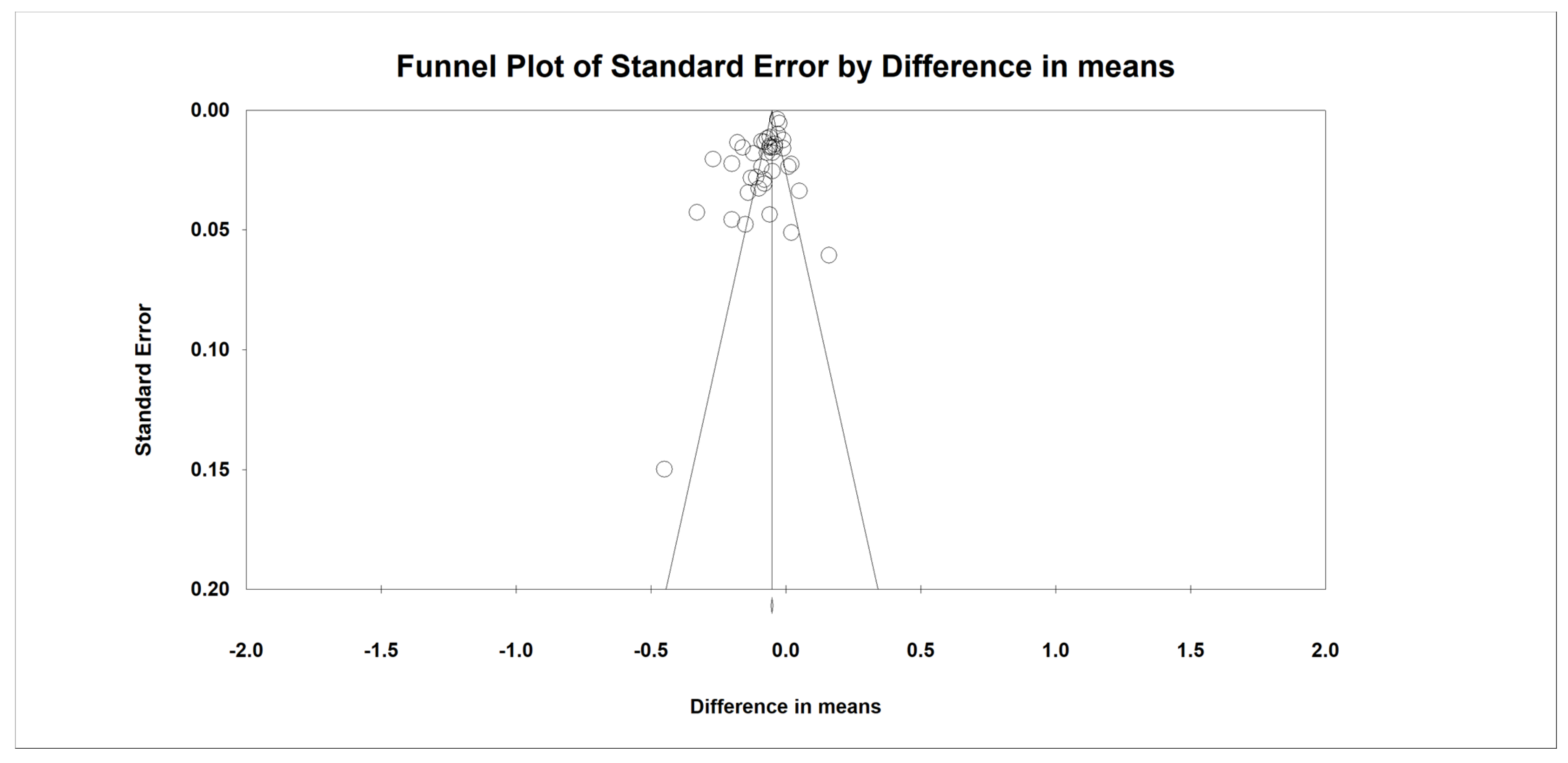
3.5. Publication Bias
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO (World Health Organisation). Obesity and Overweight; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Centers for Disease Control and Prevention. Adult Obesity Facts; CDC: Atlanta, GA, USA, 2021.
- Kim, M.S.; Kim, W.J.; Khera, A.V.; Kim, J.Y.; Yon, D.K.; Lee, S.W.; Shin, J.I.; Won, H.-H. Association between adiposity and cardiovascular outcomes: An umbrella review and meta-analysis of observational and Mendelian randomization studies. Eur. Heart J. 2021, 42, 3388–3403. [Google Scholar] [CrossRef] [PubMed]
- Theel, W.; Boxma-de Klerk, B.M.; Dirksmeier-Harinck, F.; van Rossum, E.F.; Kanhai, D.A.; Apers, J.; van Dalen, B.M.; de Knegt, R.J.; Holleboom, A.G.; Tushuizen, M.E. Evaluation of nonalcoholic fatty liver disease (NAFLD) in severe obesity using noninvasive tests and imaging techniques. Obes. Rev. 2022, 23, e13481. [Google Scholar] [CrossRef] [PubMed]
- Stasi, A.; Cosola, C.; Caggiano, G.; Cimmarusti, M.T.; Palieri, R.; Acquaviva, P.M.; Rana, G.; Gesualdo, L. Obesity-Related Chronic Kidney Disease: Principal Mechanisms and New Approaches in Nutritional Management. Front. Nutr. 2022, 9, 925619. [Google Scholar] [CrossRef]
- Cottam, D.R.; Mattar, S.G.; Barinas-Mitchell, E.; Eid, G.; Kuller, L.; Kelley, D.E.; Schauer, P.R. The chronic inflammatory hypothesis for the morbidity associated with morbid obesity: Implications and effects of weight loss. Obes. Surg. 2004, 14, 589–600. [Google Scholar] [CrossRef]
- Guo, Z.; Yang, Y.; Liao, Y.; Shi, Y.; Zhang, L.-J. Emerging Roles of Adipose Tissue in the Pathogenesis of Psoriasis and Atopic Dermatitis in Obesity. JID Innov. 2022, 2, 100064. [Google Scholar] [CrossRef] [PubMed]
- Van Raemdonck, K.; Umar, S.; Szekanecz, Z.; Zomorrodi, R.K.; Shahrara, S. Impact of obesity on autoimmune arthritis and its cardiovascular complications. Autoimmun. Rev. 2018, 17, 821–835. [Google Scholar] [CrossRef]
- Coelho, C.; Crane, J.; Agius, R.; McGowan, B. The bariatric-metabolic physician’s role in managing clinically severe obesity. Curr. Obes. Rep. 2021, 10, 263–273. [Google Scholar] [CrossRef]
- Jamialahmadi, T.; Reiner, Ž.; Alidadi, M.; Kroh, M.; Cardenia, V.; Xu, S.; Al-Rasadi, K.; Santos, R.D.; Sahebkar, A. The Effect of Bariatric Surgery on Circulating Levels of Oxidized Low-Density Lipoproteins Is Apparently Independent of Changes in Body Mass Index: A Systematic Review and Meta-Analysis. Oxidative Med. Cell. Longev. 2021, 2021, 4136071. [Google Scholar] [CrossRef]
- Jamialahmadi, T.; Reiner, Ž.; Alidadi, M.; Kroh, M.; Simental-Mendia, L.E.; Pirro, M.; Sahebkar, A. Impact of Bariatric Surgery on Pulse Wave Velocity as a Measure of Arterial Stiffness: A Systematic Review and Meta-analysis. Obes. Surg. 2021, 31, 4461–4469. [Google Scholar] [CrossRef]
- Jamialahmadi, T.; Alidadi, M.; Atkin, S.L.; Kroh, M.; Almahmeed, W.; Moallem, S.A.; Al-Rasadi, K.; Rodriguez, J.H.; Santos, R.D.; Ruscica, M.; et al. Effect of Bariatric Surgery on Flow-Mediated Vasodilation as a Measure of Endothelial Function: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 4054. [Google Scholar] [CrossRef]
- Jamialahmadi, T.; Jangjoo, A.; Rezvani, R.; Goshayeshi, L.; Tasbandi, A.; Nooghabi, M.J.; Rajabzadeh, F.; Ghaffarzadegan, K.; Mishamandani, Z.J.; Nematy, M. Hepatic Function and Fibrosis Assessment Via 2D-Shear Wave Elastography and Related Biochemical Markers Pre- and Post-Gastric Bypass Surgery. Obes. Surg. 2020, 30, 2251–2258. [Google Scholar] [CrossRef]
- Nabavi, N.; Ghodsi, A.; Rostami, R.; Torshizian, A.; Jamialahmadi, T.; Jangjoo, A.; Nematy, M.; Bahari, A.; Ebrahimzadeh, F.; Mahmoudabadi, E.; et al. Impact of Bariatric Surgery on Carotid Intima-Media Thickness in Patients with Morbid Obesity: A Prospective Study and Review of the Literature. Obes. Surg. 2022, 32, 1563–1569. [Google Scholar] [CrossRef]
- van Veldhuisen, S.L.; Gorter, T.M.; van Woerden, G.; de Boer, R.A.; Rienstra, M.; Hazebroek, E.J.; van Veldhuisen, D.J. Bariatric surgery and cardiovascular disease: A systematic review and meta-analysis. Eur. Heart J. 2022, 43, 1955–1969. [Google Scholar] [CrossRef] [PubMed]
- Carmona-Maurici, J.; Cuello, E.; Sánchez, E.; Miñarro, A.; Rius, F.; Bueno, M.; de la Fuente, M.C.; Olsina Kissler, J.J.; Vidal, T.; Maria, V.; et al. Impact of bariatric surgery on subclinical atherosclerosis in patients with morbid obesity. Surg. Obes. Relat. Dis. 2020, 16, 1419–1428. [Google Scholar] [CrossRef] [PubMed]
- Roumeliotis, A.; Roumeliotis, S.; Panagoutsos, S.; Theodoridis, M.; Argyriou, C.; Tavridou, A.; Georgiadis, G.S. Carotid intima-media thickness is an independent predictor of all-cause mortality and cardiovascular morbidity in patients with diabetes mellitus type 2 and chronic kidney disease. Ren. Fail. 2019, 41, 131–138. [Google Scholar] [CrossRef]
- Zhang, Y.; Fang, X.; Hua, Y.; Tang, Z.; Guan, S.; Wu, X.; Liu, H.; Liu, B.; Wang, C.; Zhang, Z. Carotid artery plaques, carotid intima–media thickness, and risk of cardiovascular events and all-cause death in older adults: A 5-year prospective, community-based study. Angiology 2018, 69, 120–129. [Google Scholar] [CrossRef]
- Saba, L.; Antignani, P.L.; Gupta, A.; Cau, R.; Paraskevas, K.I.; Poredos, P.; Wasserman, B.; Kamel, H.; Avgerinos, E.D.; Salgado, R. International Union of Angiology (IUA) consensus paper on imaging strategies in atherosclerotic carotid artery imaging: From basic strategies to advanced approaches. Atherosclerosis 2022, 354, 23–40. [Google Scholar] [CrossRef]
- Abeysuriya, V.; Perera, B.; Wickremasinghe, A. Regional and demographic variations of Carotid artery Intima and Media Thickness (CIMT): A Systematic review and meta-analysis. PLoS ONE 2022, 17, e0268716. [Google Scholar] [CrossRef]
- Gloy, V.L.; Briel, M.; Bhatt, D.L.; Kashyap, S.R.; Schauer, P.R.; Mingrone, G.; Bucher, H.C.; Nordmann, A.J. Bariatric surgery versus non-surgical treatment for obesity: A systematic review and meta-analysis of randomised controlled trials. BMJ 2013, 347, f5934. [Google Scholar] [CrossRef]
- Vest, A.R.; Heneghan, H.M.; Agarwal, S.; Schauer, P.R.; Young, J.B. Bariatric surgery and cardiovascular outcomes: A systematic review. Heart 2012, 98, 1763–1777. [Google Scholar] [CrossRef]
- Zagorski, S.M.; Papa, N.N.; Chung, M.H. The effect of weight loss after gastric bypass on Creactive protein levels. Surg. Obes. Relat. Dis. 2005, 1, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Yudkin, J.S.; Stehouwer, C.D.A.; Emeis, J.J.; Coppack, S.W. C-reactive protein in healthy subjects: Associations with obesity, insulin resistance, and endothelial dysfunction: A potential role for cytokines originating from adipose tissue? Arterioscler. Thromb. Vasc. Biol. 1999, 19, 972–978. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.R. Inflammatory markers and bariatric surgery: A meta-analysis. Inflamm. Res. 2012, 61, 789–807. [Google Scholar] [CrossRef]
- Sutton, A.J.; Abrams, K.R.; Jones, D.R.; Jones, D.R.; Sheldon, T.A.; Song, F. Methods for Meta-Analysis in Medical Research; Wiley Chichester: Chichester, UK, 2000; Volume 348. [Google Scholar]
- Higgins, J.P. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.0.1; The Cochrane Collaboration: London, UK, 2008; Available online: http://www.cochrane-handbook.org (accessed on 25 April 2022).
- Wells, G.A.; Shea, B.; O’Connell, D.A.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Oxford: Oxford, UK, 2000. [Google Scholar]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive Meta-Analysis; Version 2 Biostat; Meta-Analysis: Englewood, NJ, USA, 2005. [Google Scholar]
- Banach, M.; Serban, C.; Ursoniu, S.; Rysz, J.; Muntner, P.; Toth, P.P.; Jones, S.R.; Rizzo, M.; Glasser, S.P.; Watts, G.F. Statin therapy and plasma coenzyme Q10 concentrations—A systematic review and meta-analysis of placebo-controlled trials. Pharmacol. Res. 2015, 99, 329–336. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Yavuz, D.G.; Apaydin, T.; Imre, E.; Uygur, M.M.; Yazici, D. Skin Autofluorescence and Carotid Intima-Media Thickness Evaluation Following Bariatric Surgery in Patients with Severe Obesity. Obes. Surg. 2021, 31, 1055–1061. [Google Scholar] [CrossRef] [PubMed]
- Salman, M.A.; Salman, A.A.; El Sherbiny, M.; Elkholy, S.; Youssef, A.; Labib, S.; El-Din, M.T.; Monazea, K.A.; Tourky, M.S.; Mikhail, H.M.S.; et al. Changes of Carotid Intima-Media Thickness After Sleeve Gastrectomy in High Cardiovascular Risk Patients: A Prospective Study. Obes. Surg. 2021, 31, 3541–3547. [Google Scholar] [CrossRef]
- Melchor-López, A.; Suárez-Cuenca, J.A.; Banderas-Lares, D.Z.; Peña-Sosa, G.D.L.; Salamanca-García, M.; Vera-Gómez, E.; Hernández-Patricio, A.; Gutiérrez-Buendía, J.A.; Zamora-Alemán, C.R.; Alcaráz-Estrada, S.L.; et al. Identification of adipose tissue-related predictors of the reduction in cardiovascular risk induced by metabolic surgery. J. Int. Med. Res. 2021, 49, 03000605211012569. [Google Scholar] [CrossRef]
- Kaul, A.; Kumar, A.; Baksi, A.; Singla, V.; Aggarwal, S.; Gulati, G.; Narang, R.; Kashyap, L. Impact of bariatric surgery on carotid intima-medial thickness and cardiovascular risk: Results of a prospective study. Surg. Endosc. Other Interv. Tech. 2021, 35, 6006–6012. [Google Scholar] [CrossRef]
- Cekici, Y.; Kaya, B.C.; Elkan, H. The Effect of Laparoscopic Sleeve Gastrectomy on Subclinical Atherosclerosis in Patients with Severe Obesity. Obes. Surg. 2021, 31, 738–745. [Google Scholar] [CrossRef]
- Ministrini, S.; Ricci, M.A.; Nulli Migliola, E.; De Vuono, S.; D’Abbondanza, M.; Paganelli, M.T.; Vaudo, G.; Siepi, D.; Lupattelli, G. Chemerin predicts carotid intima-media thickening in severe obesity. Eur. J. Clin. Investig. 2020, 50, e13256. [Google Scholar] [CrossRef] [PubMed]
- Kaya, B.C.; Elkan, H. The impact of weight loss after laparoscopic sleeve gastrectomy on early markers of atherosclerotic vascular disease: A prospective study. Kardiol. Pol. 2020, 78, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Martin, J.M.; Aracil, E.; Insenser, M.; de la Peña, G.; Lasunción, M.A.; Galindo, J.; Escobar-Morreale, H.F.; Balsa, J.A.; Botella-Carretero, J.I. Changes in Soluble TWEAK Concentrations, but Not Those in Amyloid-β(1–40), Are Associated with a Decrease in Carotid Intima-Media Thickness after Bariatric Surgery in Obese Women. Obes. Facts 2020, 13, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Elitok, A.; Emet, S.; Bayramov, F.; Karaayvaz, E.; Türker, F.; Barbaros, U.; Özcan, M. Effect of bariatric surgery on flow-mediated dilation and carotid intima-media thickness in patients with morbid obesity: 1-year follow-up study. Anatol. J. Cardiol. 2020, 23, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Domenech-Ximenos, B.; Cuba, V.; Daunis-i-Estadella, P.; Thio-Henestrosa, S.; Jaldo, F.; Biarnes, C.; Molina, X.; Xifra, G.; Ricart, W.; Bardera, A.; et al. Bariatric Surgery-Induced Changes in Intima-Media Thickness and Cardiovascular Risk Factors in Class 3 Obesity: A 3-Year Follow-Up Study. Obesity 2020, 28, 1663–1670. [Google Scholar] [CrossRef]
- Cobeta, P.; Osorio, A.; Cuadrado-Ayuso, M.; Garcia-Moreno, F.; Pestana, D.; Galindo, J.; Botella-Carretero, J.I. Sleeve Gastrectomy and Gastric Bypass Decrease the Carotid Intima-Media Thickness in Obese Men: Association with Weight Loss, Cardiovascular Risk Factors, and Circulating Testosterone. Obes. Surg. 2020, 30, 851–859. [Google Scholar] [CrossRef]
- Borzi, A.M.; Buscemi, C.; Corleo, D.; Randazzo, C.; Rosafio, G.; Pantuso, G.; Buscemi, S. Endothelial Function in Obese Patients Treated with Bariatric Surgery. Diabetes Metab. Syndr. Obes.-Targets Ther. 2020, 13, 247–256. [Google Scholar] [CrossRef]
- Yang, W.; Jiang, S.; Cheung, P.N.; Wang, C. Effects and predictive factors of bariatric surgery on carotid intima-media thickness in patients with obesity Cardiovascular risk and bariatric surgery. Obes. Surg. 2019, 29, 140. [Google Scholar]
- Solini, A.; Seghieri, M.; Santini, E.; Giannini, L.; Biancalana, E.; Taddei, S.; Volterrani, D.; Bruno, R.M. Renal Resistive Index Predicts Post-Bariatric Surgery Renal Outcome in Nondiabetic Individuals with Severe Obesity. Obesity 2019, 27, 68–74. [Google Scholar] [CrossRef]
- Gluszewska, A.; Gryglewska, B.; Rewiuk, K.; Zarzycki, B.; Dzieza-Grudnik, A.; Kwater, A.; Major, P.; Budzynski, A.; Gasowski, J.; Grodzicki, T. Arterial structure and function and its short- and long-term changes after bariatric surgery. J. Physiol. Pharmacol. 2019, 70, 909–916. [Google Scholar] [CrossRef]
- Rius, F.; Sanchez, E.; Betriu, A.; Baena-Fustegueras, J.A.; Yeramian, A.; Vidal, T.; Hernandez, M.; Lopez-Cano, C.; Bueno, M.; Gutierrez-Carrasquilla, L.; et al. Influence of Morbid Obesity and Bariatric Surgery Impact on the Carotid Adventitial Vasa Vasorum Signal. Obes. Surg. 2018, 28, 3935–3942. [Google Scholar] [CrossRef] [PubMed]
- Jonker, F.H.W.; van Houten, V.A.A.; Wijngaarden, L.H.; Klaassen, R.A.; de Smet, A.A.E.A.; Niezen, A.; Schelfhout, L.J.D.M.; Bruning, T.A.; van der Harst, E. Age-Related Effects of Bariatric Surgery on Early Atherosclerosis and Cardiovascular Risk Reduction. Obes. Surg. 2018, 28, 1040–1046. [Google Scholar] [CrossRef] [PubMed]
- Altin, C.; Erol, V.; Aydin, E.; Yilmaz, M.; Tekindal, M.A.; Sade, L.E.; Gulay, H.; Muderrisoglu, H. Impact of weight loss on epicardial fat and carotid intima media thickness after laparoscopic sleeve gastrectomy: A prospective study. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Tromba, L.; Tartaglia, F.; Carbotta, S.; Sforza, N.; Pelle, F.; Colagiovanni, V.; Carbotta, G.; Cavaiola, S.; Casella, G. The Role of Sleeve Gastrectomy in Reducing Cardiovascular Risk. Obes. Surg. 2017, 27, 1145–1151. [Google Scholar] [CrossRef]
- Chen, J.; Yu, H.Y.; Chen, L.; Wu, L.; Hu, B.; Bao, Y.Q.; Jiang, L.X. Effect of Roux-en-Y gastric bypass on carotid intima-media thickness in Chinese obese patients with type 2 diabetes. Surg. Obes. Relat. Dis. 2017, 13, 1530–1535. [Google Scholar] [CrossRef]
- Marchesi, F.; Giacosa, R.; Reggiani, V.; De Sario, G.; Tartamella, F.; Melani, E.; Mita, M.T.; Cinieri, F.G.; Cecchini, S.; Ricco, M.; et al. Morphological Changes in the Carotid Artery Intima after Gastric Bypass for Morbid Obesity. Obes. Surg. 2017, 27, 357–363. [Google Scholar] [CrossRef]
- Yorulmaz, G.; Cilekar, M.; Bilge, U.; Akcan, E.; Akalin, A. Carotid intima-media thickness and insulin resistance changes in patients who underwent sleeve gastrectomy: A prospective study. Niger. J. Clin. Pract. 2016, 19, 344–348. [Google Scholar] [CrossRef]
- Solmaz, A.; Arlcl, S.; Gülçiçek, O.B.; Yavuz, E.; Yiǧitbaş, H.; Erçetin, C.; Öncü, M.; Çelebi, F.; Çelik, A.; Kutaniş, R. Influence of Bariatric Surgery on Carotid Intima-Media Thickness. Bariatr. Surg. Pract. Patient Care 2016, 11, 56–60. [Google Scholar] [CrossRef]
- Graziani, F.; Leone, A.M.; Basile, E.; Cialdella, P.; Tritarelli, A.; Della Bona, R.; Liuzzo, G.; Nanni, G.; Iaconelli, A.; Iaconelli, A.; et al. Endothelial Progenitor Cells in Morbid Obesity-Pathogenetic Implications. Circ. J. 2014, 78, 977–985. [Google Scholar] [CrossRef]
- Tschoner, A.; Sturm, W.; Gelsinger, C.; Ress, C.; Laimer, M.; Engl, J.; Laimer, E.; Muhlmann, G.; Mittermair, R.; Kaser, S.; et al. Long-term Effects of Weight Loss after Bariatric Surgery on Functional and Structural Markers of Atherosclerosis. Obesity 2013, 21, 1960–1965. [Google Scholar] [CrossRef]
- Bravo, G.G.; Bunout, D.; Mella, J.; Quiroga, E.; de la Maza, M.P.; Cavada, G.; Hirsch, S. Bariatric surgery decreases carotid intima-media thickness in obese subjects. Nutr. Hosp. 2013, 28, 1102–1108. [Google Scholar] [CrossRef]
- Lundby-Christensen, L.; Tarnow, L.; Vaag, A.; Wiinberg, N.; Hansen, D.; Worm, D.; Hvolris, L.; Naver, L.; Almdal, T. Carotid intima-media thickness is reduced 12 months after gastric bypass surgery in patients with type 2 diabetes. Diabetologia 2012, 55, S505. [Google Scholar]
- Geloneze, S.R.; Geloneze, B.; Morari, J.; Matos-Souza, J.R.; Lima, M.M.; Chaim, E.A.; Pareja, J.C.; Velloso, L.A. PGC1α gene Gly482Ser polymorphism predicts improved metabolic, inflammatory and vascular outcomes following bariatric surgery. Int. J. Obes. 2012, 36, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Sarmento, P.L.F.A.; Plavnik, F.L.; Zanella, M.T.; Pinto, P.E.; Miranda, R.B.; Ajzen, S.A. Association of carotid intima-media thickness and cardiovascular risk factors in women pre- and post-bariatric surgery. Obes. Surg. 2009, 19, 339–344. [Google Scholar] [CrossRef] [PubMed]
- van Mil, S.R.; Biter, L.U.; van de Geijn, G.J.M.; Birnie, E.; Dunkelgrun, M.; Ijzermans, J.N.; van der Meulen, N.; Mannaerts, G.H.; Castro Cabezas, M. The effect of sex and menopause on carotid intima-media thickness and pulse wave velocity in morbid obesity. Eur. J. Clin. Investig. 2019, 49, e13118. [Google Scholar]
- Dalmas, E.; Kahn, J.-F.; Giral, P.; Abdennour, M.; Bouillot, J.-L.; Fellahi, S.; Oppert, J.-M.; Clément, K.; Guerre-Millo, M.; Poitou, C. Intima-media thickness in severe obesity: Links with BMI and metabolic status but not with systemic or adipose tissue inflammation. Diabetes Care 2013, 36, 3793–3802. [Google Scholar] [CrossRef]
- Sandgren, T.; Sonesson, B.; Ahlgren, Å.R.; Länne, T. The diameter of the common femoral artery in healthy human: Influence of sex, age, and body size. J. Vasc. Surg. 1999, 29, 503–510. [Google Scholar] [CrossRef]
- Boras, J.; Ljubic, S.; Car, N.; Metelko, Z.; Petrovecki, M.; Lovrencic, M.V.; Reiner, Z. Lipoprotein (a) predicts progression of carotid artery intima-media thickening in patients with type 2 diabetes: A four-year follow-up. Wien. Klin. Wochenschr. 2010, 122, 159–164. [Google Scholar] [CrossRef]
- Reiner, Ž.; Simental-Mendía, L.; Ruscica, M.; Katsiki, N.; Banach, M.; Rasadi, K.; Jamialahmadi, T.; Sahebkar, A. Pulse wave velocity as a measure of arterial stiffness in patients with familial hypercholesterolemia: A systematic review and meta-analysis. Arch. Med. Sci. 2019, 15, 1365–1374. [Google Scholar] [CrossRef]
- Reiner, Ž. Impact of Early Evidence of Atherosclerotic Changes on Early Treatment in Children with Familial Hypercholesterolemia; American Heart Association: Dallas, TX, USA, 2014; Volume 114, pp. 233–235. [Google Scholar]
- Gómez-Martin, J.M.; Balsa, J.; Aracil, E.; Cuadrado-Ayuso, M.; Rosillo, M.; De la Peña, G.; Lasunción, M.; Escobar-Morreale, H.F.; Botella-Carretero, J.I. Beneficial changes on plasma apolipoproteins A and B, high density lipoproteins and oxidized low density lipoproteins in obese women after bariatric surgery: Comparison between gastric bypass and sleeve gastrectomy. Lipids Health Dis. 2018, 17, 145. [Google Scholar] [CrossRef]
- Lupoli, R.; Di Minno, M.; Guidone, C.; Cefalo, C.; Capaldo, B.; Riccardi, G.; Mingrone, G. Effects of bariatric surgery on markers of subclinical atherosclerosis and endothelial function: A meta-analysis of literature studies. Int. J. Obes. 2016, 40, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Borui, T.; Zhang, Y.; Wang, Y.; Wang, X.; An, Z.; Yu, X. Effect of Bariatric Surgery on Long-Term Cardiovascular Outcomes: A Systematic Review and Meta-analysis of Population-Based Cohort Studies. Surg. Obes. Relat. Dis. 2022, 18, 1074–1086. [Google Scholar]
- Poredoš, P.; Cífková, R.; Maier, J.A.M.; Nemcsik, J.; Šabovič, M.; Jug, B.; Ježovnik, M.K.; Schernthaner, G.H.; Antignani, P.L.; Catalano, M. Preclinical atherosclerosis and cardiovascular events: Do we have a consensus about the role of preclinical atherosclerosis in the prediction of cardiovascular events? Atherosclerosis 2022, 348, 25–35. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Year | Study Design | Follow-up | Treatment | Control | Clinical Outcome | Patients | No. of Patients |
|---|---|---|---|---|---|---|---|
| C-IMT | |||||||
| Yavuz et al., 2021 [32] | Observational study | 6 months 12 months | LSG or RYGB | - | Significant reduction was observed after 6 months | Patients with Class 3 obesity mean age of 42.3 ± 10.1 years. | 41 |
| Salman et al., 2021 [33] | Prospective study | 6 months 12 months | LSG | - | Significant reduction was observed after 12 months | Patients with obesity and high cardiovascular risk M/F (63/57) mean age of 43.7 ± 8.5 years. | 120 |
| Melchor-López et al., 2021 [34] | Case–control study | 9 months | LSG or RYGB | - | Significant reduction was observed No change | Patients with morbid obesity ≥ 10% reduction in CIMT Patients with morbid obesity <10% reduction in CIMT 75% F mean age 44.5 years. | 28 12 |
| Kaul et al., 2021 [35] | Prospective study | 6 months 12 months | LSG or RYGB or OAGB | - | Significant reduction was observed after 6 months | Patients with obesity 70% F mean age of 40.8 ± 10.7 years. | 40 |
| Cekici et al., 2021 [36] | Prospective study | 6 months | LSG | - | Significant reduction was observed | Patients with severe obesity 35F/12M mean age of 38 ± 10.48 years. | 47 |
| Ministrini et al., 2020 [37] | Single arm, open labeled, prospective pilot study | 10–12 months | LSG | - | Significant reduction was observed | Patients with severe obesity 77.2% F, average age of 44.0 ± 10.1 years. | 54 |
| Kaya and Elkan, 2020 [38] | Prospective cohort study | 6 months | LSG | - | Significant reduction was observed | Patients with morbid obesity 67.6% M mean age of 37.6 ± 11.2 years. | 71 |
| Gómez-Martin et al., 2020 [39] | Prospective study | 12 months | LSG RYGB | diet and lifestyle modification | Significant reduction was observed in both groups compared with baseline and control group | Women with severe obesity mean age of 48 ± 9 years. | 20 20 |
| Elitok et al., 2020 [40] | Observational study | 3 months 6 months 9 months 12 months | RYGB | - | Significant reduction was observed after 9 months | Patients with morbid obesity 13 F Mean age of 40.4 ± 5.6 years. | 23 |
| Domenech-Ximenos et al., 2020 [41] | Prospective observational study | 3 years | RYGB | 1. nonsurgical approaches 2. without any intervention (healthy controls) | Significant reduction was observed compared with nonsurgical approaches | Patients with class 3 obesity 17 F 46 (38–54) age | 21 |
| Cobeta et al., 2020 [42] | Observational study | 6 months | LSG RYGB | diet and lifestyle modification | Significant reduction was observed in both groups compared with baseline and control group | Men with severe obesity and high cardiovascular risk 48 ± 8 age | 20 20 |
| Carmona-Maurici et al., 2020 [16] | Observational study | 6 months 12 months | RYGB or LSG | - | No change | Patients with obesity and plaque Patients with obesity without plaque F (56%) mean age of 51.8 ± 1.8 years. | 32 34 |
| Borzi et al., 2020 [43] | Observational study | 6–24 months (mean:16 ± 8) | Adjustable GB or GBP or BPD | Medical nutrition treatment | No change | Patients with obesity F/M 13/4 Mean age of 39.8 ± 10.4 years. | 17 |
| Yang et al., 2019 [44] | Retrospective study | 12 months | RYGB or LSG | - | Significant reduction was observed | Patients with obesity and T2D Patients with obesity without T2D | 28 62 |
| Solini et al., 2019 [45] | Prospective observational study | 12 months | RYGB | - | Significant reduction was observed | Nondiabetic subjects with severe obesity F/M 19/6 Mean age of 46.7 ± 12.9 years. | 25 |
| Gluszewska et al., 2019 [46] | Prospective cohort study | 10 days 6 months | RYGB or LSG | - | Significant reduction was observed after 6 months | Patients with extreme obesity 45% M Mean age of 45.6 (±10.9) years. | 71 |
| Rius et al., 2019 [47] | Case-control study | 12 months | RYGB or LSG | - | No change | Patients with morbid obesity 77.5% F Mean age of 45.0 ± 11.7 years. | 33 |
| Jonker et al., 2018 [48] | Prospective study | 6 months 12 months | LSG or RYGB | - | Significant reduction was observed after 12 months | Women with obesity Men with obesity F 83.1% Mean age of 42.5 (19.4–62.1) years. | 111 35 |
| Altin et al., 2018 [49] | Prospective study | 6 months | LSG | - | Significant reduction was observed | Patients with severe obesity (79F/26M) Mean age of 43.61 12.42 years. | 105 |
| Tromba et al., 2017 [50] | Observational study | 3 months 6 months | LSG | - | Significant reduction was observed after 6 months | Patients with obesity 27 F Mean age of 38.7 ± 9 years | 45 |
| Chen et al., 2017 [51] | Retrospective study | 12 months | RYGB | - | Significant reduction was observed | Patients with obesity and T2D F/M 17/16 Mean age of 47.7 ± 11.6 years | 33 |
| Marchesi et al., 2017 [52] | Prospective study | 1 month 12 months | RYGB | - | Significant reduction was observed after 12 months | Women with morbid obesity Mean age of 42.68 | 22 |
| Yorulmaz et al., 2016 [53] | Prospective study | 4–5 months (average: 4.6 months) | LSG | - | Significant reduction was observed | Patients with minimum BMI of 40, who did not have any known chronic diseases 14F/2M, Average age of 39.12 ± 10.63 years. | 16 |
| Solmaz et al., 2016 [54] | Prospective study | 3 months 6 months | LSG LGP | - | Significant reduction was observed after 3 months | Patients with obesity F/M 31/17 42.96 ± 7.87 (LSG) 38.3 ± 9.88 (LGP) | 25 23 |
| Graziani et al., 2014 [55] | Observational study | 252 ± 108 days | bariatric surgery | - | No change | Patients with obesity Mean age of 39.8 ± 8.0 | 48 |
| Tschoner et al., 2013 [56] | Prospective study | 5 years | SAGB or GBP | - | Significant reduction was observed | Patients with morbid obesity 40F/12M Mean age of 35.3 years. | 52 |
| Bravo et al., 2013 [57] | Prospective study | 354 ± 92.1 days | LSG or RYGB | - | Significant reduction was observed | Patients with obesity Mean age of 43.6 ± 8.1 years. | 27 |
| Lundby-Christensen et al., 2012 [58] | Observational prospective study | 6 months 12 months | RYGB | - | Significant reduction was observed 12 months after RYGB in patients with T2D/IGT | Patients with obesity and normal glucose tolerance 31.3% M Mean age of 44.8 ± 10.4 Patients with obesity and type 2 diabetes or impaired glucose tolerance (T2D/IGT) 33.3% M Mean age of 47.4 ± 6.7 | 16 18 |
| Geloneze et al., 2012 [59] | Observational study | 1 month 6 months 12 months | RYGB | - | Significant reduction was observed | Patients with obesity without Gly482Ser polymorphism 24F/2M Mean age of 37.2 ± 10.7 Patients with obesity and Gly482Ser polymorphism of the ppargc1a gene 23F/6M Mean age of 37.2 ± 9.4 | 26 29 |
| Sarmento et al., 2009 [60] | Observational study | 3 months 6 months 12 months | RYGB | - | Significant reduction was observed after 6 months | Women with morbid obesity Mean age of 44.1 ± 9.8 years. | 18 |
| Study | Selection | Comparability | Outcome | |||||
|---|---|---|---|---|---|---|---|---|
| Representativeness of the Exposed Cohort | Selection of the Nonexposed Cohort | Ascertainment of Exposure | Demonstration that Outcome of Interest Was not Present at the Beginning of the Study | Comparability of Cohorts on the Basis of the Design or Analysis | Assessment of Outcome | Follow-up Was Not Long Enough for Outcomes to Occur | Adequacy of Follow-up of Cohorts | |
| Yavuz et al., 2021 [32] | * | - | * | * | - | * | * | - |
| Salman et al., 2021 [33] | * | - | * | * | - | * | * | * |
| Kaul et al., 2021 [35] | * | - | * | * | - | * | * | * |
| Cekici et al., 2021 [36] | * | - | * | * | - | * | * | * |
| Ministrini et al., 2020 [37] | * | - | * | * | - | * | * | * |
| Kaya et al., 2020 [38] | * | - | * | * | - | * | * | * |
| Gómez-Martin et al., 2020 [39] | * | * | * | * | * | * | * | * |
| Elitok et al., 2020 [40] | * | - | * | * | - | * | * | * |
| Domenech-Ximenos et al., 2020 [41] | * | * | * | * | * | * | * | * |
| Cobeta et al., 2020 [42] | * | * | * | * | * | * | * | * |
| Carmona-Maurici et al., 2020 [16] | * | - | * | * | - | * | * | - |
| Borzi et al. 2020 [43] | * | - | * | * | - | * | * | * |
| Yang et al., 2019 [44] | * | - | - | - | - | * | * | - |
| Solini et al., 2019 [45] | * | - | * | * | - | * | * | * |
| Gluszewska et al., 2019 [46] | * | - | * | * | - | * | * | * |
| Jonker et al., 2018 [48] | * | - | * | * | - | * | * | - |
| Altin et al., 2018 [49] | * | - | * | * | - | * | * | * |
| Tromba et al., 2017 [50] | * | - | * | * | - | * | * | * |
| Chen et al., 2017 [51] | - | * | * | - | * | * | * | * |
| Marchesi et al., 2017 [52] | * | - | * | * | - | * | * | * |
| Yorulmaz et al., 2016 [53] | * | - | * | * | - | * | * | * |
| Solmaz et al., 2016 [54] | * | - | * | * | - | * | * | * |
| Graziani et al., 2014 [55] | * | - | * | * | - | * | * | * |
| Tschoner et al., 2013 [56] | * | - | * | * | - | * | * | * |
| Bravo et al., 2013 [57] | * | - | * | * | - | * | * | * |
| Lundby-Christensen et al., 2012 [58] | * | * | * | * | - | * | * | * |
| Geloneze et al., 2012 [59] | * | - | * | * | - | * | * | * |
| Sarmento et al., 2009 [60] | * | - | * | * | - | * | * | * |
| Study | Selection | Comparability | Exposure | |||||
|---|---|---|---|---|---|---|---|---|
| The Definition Was Adequate | Representativeness of the Cases | Selection of Controls | Definition of Controls | Comparability of Cases and Controls on the Basis of the Design or Analysis | Ascertainment of Exposure | The Same Method of Ascertainment for Cases and Controls | Non-Response Rate | |
| Melchor-López et al., 2021 [34] | * | * | * | * | - | * | * | * |
| Rius et al., 2019 [47] | * | * | * | * | * | * | * | * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jamialahmadi, T.; Reiner, Ž.; Alidadi, M.; Almahmeed, W.; Kesharwani, P.; Al-Rasadi, K.; Eid, A.H.; Rizzo, M.; Sahebkar, A. Effect of Bariatric Surgery on Intima Media Thickness: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 6056. https://doi.org/10.3390/jcm11206056
Jamialahmadi T, Reiner Ž, Alidadi M, Almahmeed W, Kesharwani P, Al-Rasadi K, Eid AH, Rizzo M, Sahebkar A. Effect of Bariatric Surgery on Intima Media Thickness: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(20):6056. https://doi.org/10.3390/jcm11206056
Chicago/Turabian StyleJamialahmadi, Tannaz, Željko Reiner, Mona Alidadi, Wael Almahmeed, Prashant Kesharwani, Khalid Al-Rasadi, Ali H. Eid, Manfredi Rizzo, and Amirhossein Sahebkar. 2022. "Effect of Bariatric Surgery on Intima Media Thickness: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 20: 6056. https://doi.org/10.3390/jcm11206056
APA StyleJamialahmadi, T., Reiner, Ž., Alidadi, M., Almahmeed, W., Kesharwani, P., Al-Rasadi, K., Eid, A. H., Rizzo, M., & Sahebkar, A. (2022). Effect of Bariatric Surgery on Intima Media Thickness: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(20), 6056. https://doi.org/10.3390/jcm11206056