
Endometriosis, an Ongoing Pain—Step-by-Step Treatment

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
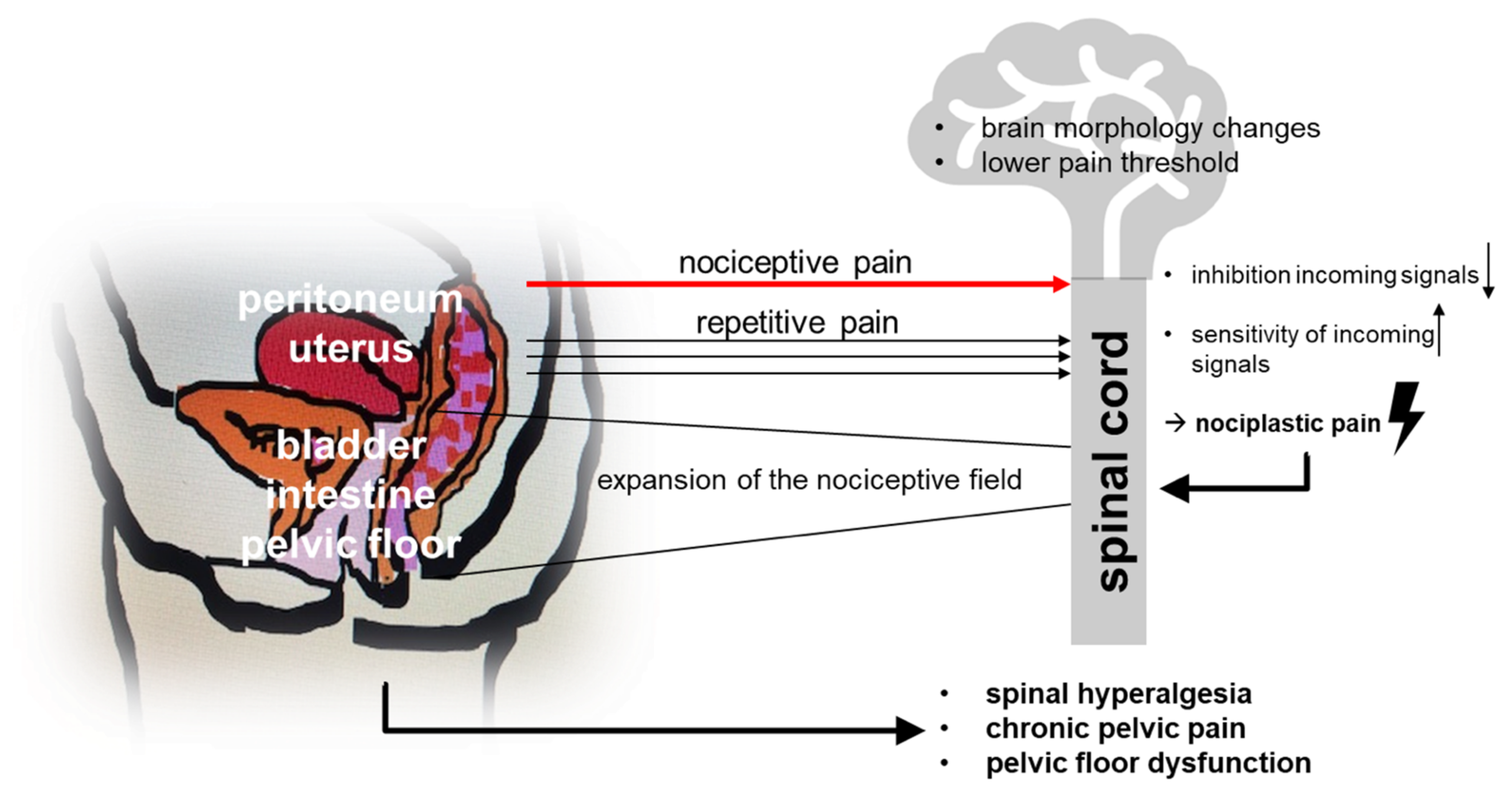
2. What to Do with Pain-Ridden Endometriosis Patients
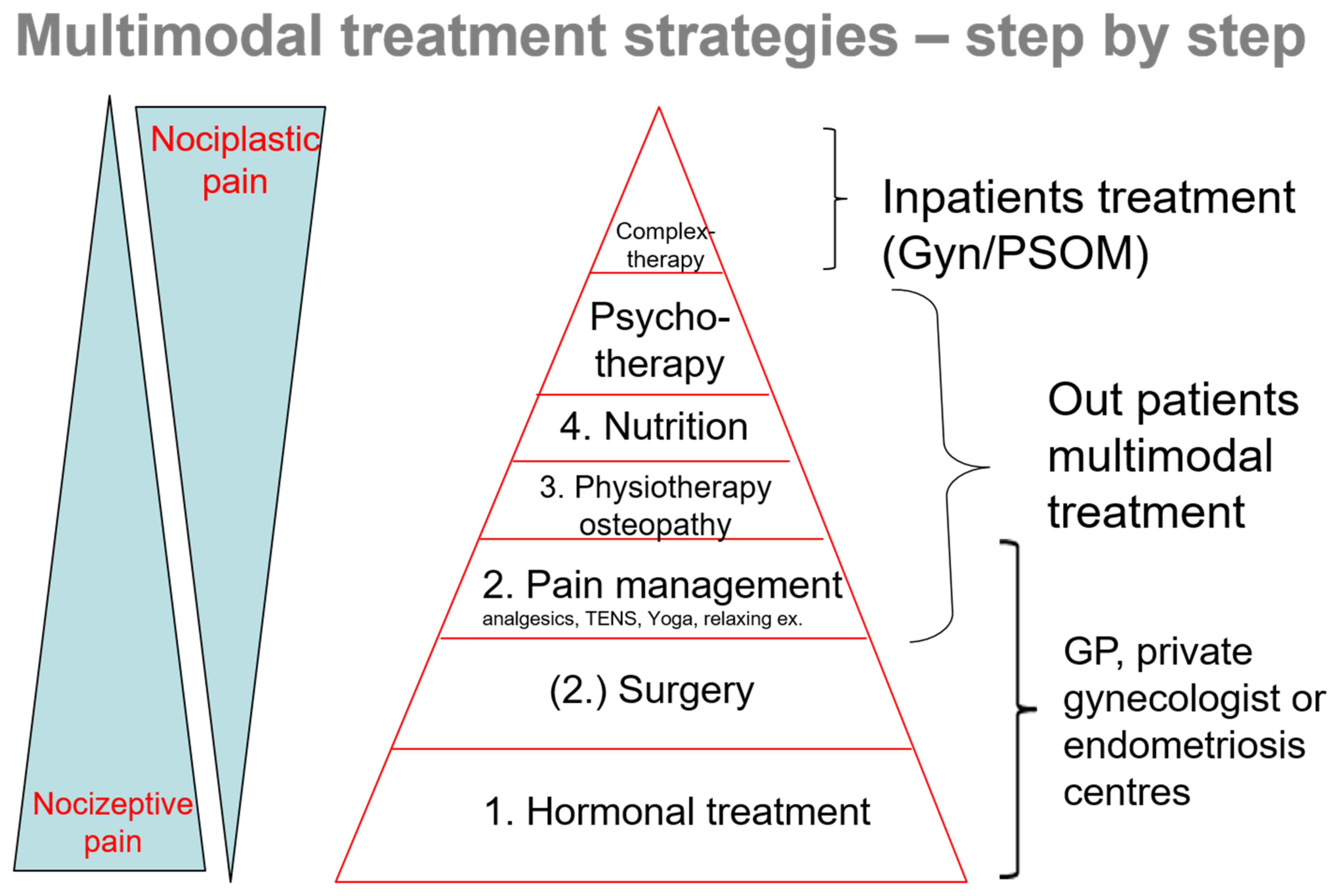
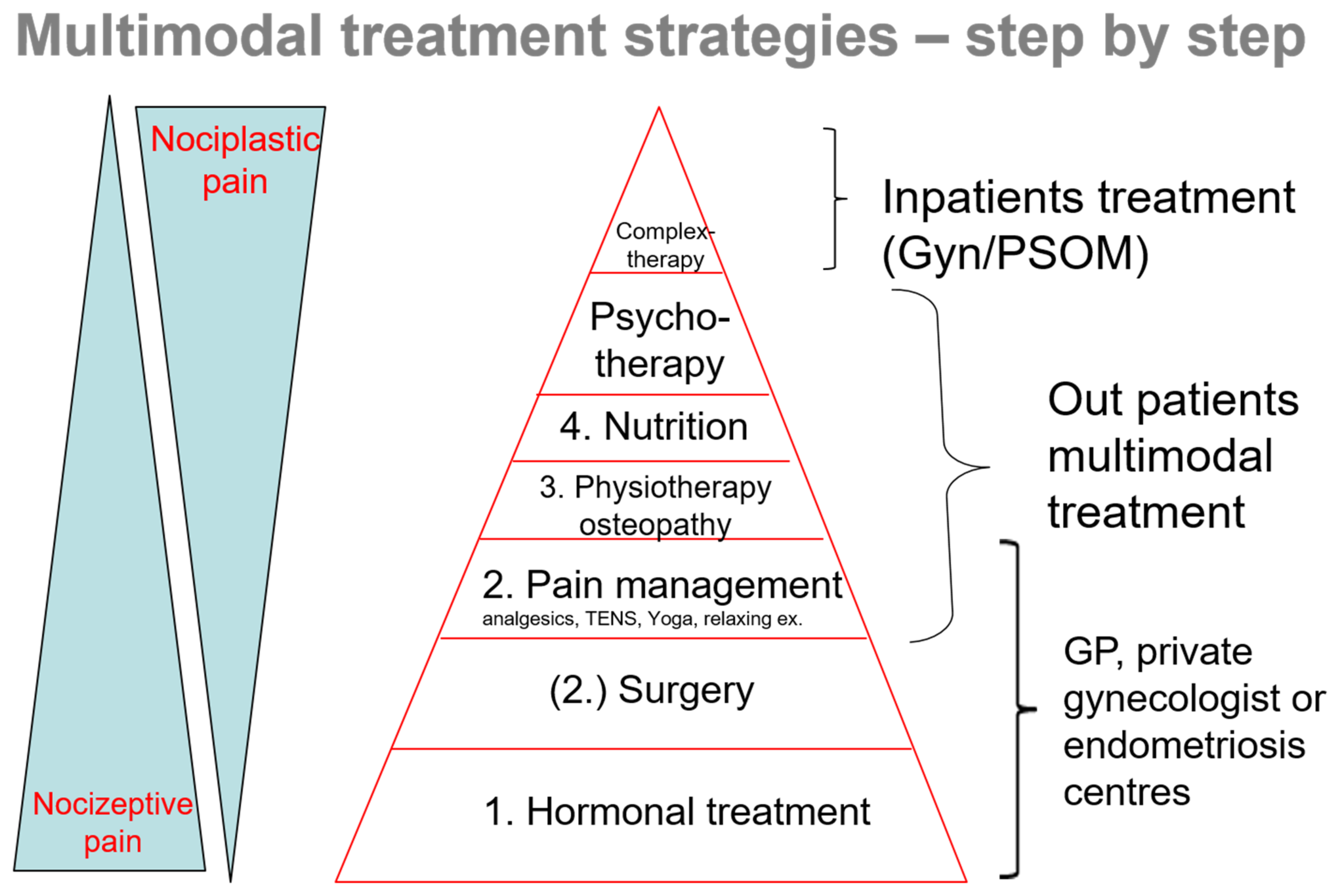
3. Practical Course of Action—Examining the Individual Steps
3.1. Hormonal Therapy
3.2. Repeated Surgery
3.3. Analgesics
3.4. Musculoskeletal System/Pelvic Floor
3.5. Diet
3.6. Psyche
3.7. Pain Complex Therapy
4. Conclusions
Funding
Conflicts of Interest
References
- Ballweg, M.L. Impact of endometriosis on women’s health: Comparative historical data show that the earlier the onset, the more severe the disease. Best Pract. Res. Clin. Obstet. Gynaecol. 2004, 18, 201–218. [Google Scholar] [CrossRef] [PubMed]
- Shakiba, K.; Bena, J.F.; McGill, K.M.; Minger, J.; Falcone, T. Surgical treatment of endometriosis: A 7-year follow-up on the requirement for further surgery. Obstet. Gynecol. 2008, 111, 1285–1292. [Google Scholar] [CrossRef] [Green Version]
- Seo, J.W.; Lee, D.Y.; Yoon, B.K.; Choi, D. Effects of long-term postoperative dienogest use for treatment of endometriosis on bone mineral density. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 212, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Kerner, W.; Brückel, J. Definition, classification and diagnosis of diabetes mellitus. Exp. Clin. Endocrinol. Diabetes 2014, 122, 384–386. [Google Scholar] [CrossRef] [Green Version]
- Greene, R.; Stratton, P.; Cleary, S.D.; Ballweg, M.L.; Sinaii, N. Diagnostic experience among 4334 women reporting surgically diagnosed endometriosis. Fertil. Steril. 2009, 91, 32–39. [Google Scholar] [CrossRef]
- Ng, N.; Wahl, K.; Orr, N.L.; Noga, H.; Williams, C.; Allaire, C.; Bedaiwy, M.A.; Yong, P.J. Endometriosis and Negative Perception of the Medical Profession. J. Obstet. Gynaecol. Can. 2020, 42, 248–255. [Google Scholar] [CrossRef] [Green Version]
- Klatt, F. Ist die Betreuung von Endometriosepatientinnen in der Praxis gesundheitsökonomisch sinnvoll? 2020. Available online: http://dx.doi.org/10.17169/refubium-28196 (accessed on 14 January 2021).
- Becker, C.M.; Gattrell, W.T.; Gude, K.; Singh, S.S. Reevaluating response and failure of medical treatment of endometriosis: A systematic review. Fertil. Steril. 2017, 108, 125–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vercellini, P.; Somigliana, E.; Viganò, P.; Abbiati, A.; Barbara, G.; Crosignani, P.G. Surgery for endometriosis-associated infertility: A pragmatic approach. Hum. Reprod. 2009, 24, 254–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mechsner, S. Endometriosis: An often unrecognized pain disorder. Schmerz 2016, 30, 477–490. [Google Scholar] [CrossRef]
- Gruber, T.M.; Mechsner, S. Pathogenesis of Endometriosis: The Origin of Pain and Subfertility. Cells 2021, 10, 1381. [Google Scholar] [CrossRef] [PubMed]
- Chapron, C.; Marcellin, L.; Borghese, B.; Santulli, P. Rethinking mechanisms, diagnosis and management of endometriosis. Nat. Rev. Endocrinol. 2019, 15, 666–682. [Google Scholar] [CrossRef]
- Casper, R.F. Progestin-only pills may be a better first-line treatment for endometriosis than combined estrogen-progestin contraceptive pills. Fertil. Steril. 2017, 107, 533–536. [Google Scholar] [CrossRef] [Green Version]
- Dunselman, G.A.; Vermeulen, N.; Becker, C.; Calhaz-Jorge, C.; D’Hooghe, T.; De Bie, B.; Heikinheimo, O.; Horne, A.W.; Kiesel, L.; Nap, A.; et al. ESHRE guideline: Management of women with endometriosis. Hum. Reprod. 2014, 29, 400–412. [Google Scholar] [CrossRef]
- Brandes, I.; Neuser, M.; Kopf, A.; Chiantera, V.; Sehouli, J.; Mechsner, S. Endometriosis-associated Pain in Patients with and without Hormone Therapy. J. Endometr. Pelvic Pain Disord. 2017, 9, 200–205. [Google Scholar] [CrossRef]
- Mechsner, S. Endometrioseschmerz Beherrschen. Der Schmerz 2021, 35, 159–171. [Google Scholar] [CrossRef]
- Strowitzki, T.; Marr, J.; Gerlinger, C.; Faustmann, T.; Seitz, C. Dienogest is as effective as leuprolide acetate in treating the painful symptoms of endometriosis: A 24-week, randomized, multicentre, open-label trial. Hum. Reprod. 2010, 25, 633–641. [Google Scholar] [CrossRef] [Green Version]
- Ferrero, S.; Evangelisti, G.; Barra, F. Current and emerging treatment options for endometriosis. Expert Opin. Pharmacother. 2018, 19, 1109–1125. [Google Scholar] [CrossRef]
- Abesadze, E.; Chiantera, V.; Sehouli, J.; Mechsner, S. Post-operative management and follow-up of surgical treatment in the case of rectovaginal and retrocervical endometriosis. Arch. Gynecol. Obstet. 2020, 302, 957–967. [Google Scholar] [CrossRef]
- He, W.; Liu, X.; Zhang, Y.; Guo, S.W. Generalized hyperalgesia in women with endometriosis and its resolution following a successful surgery. Reprod. Sci. 2010, 17, 1099–1111. [Google Scholar] [PubMed]
- Köhler, G.; Faustmann, T.A.; Gerlinger, C.; Seitz, C.; Mueck, A.O. A dose-ranging study to determine the efficacy and safety of 1, 2, and 4mg of dienogest daily for endometriosis. Int. J. Gynaecol. Obstet. 2010, 108, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Henzl, M.R.; Buttram, V.; Segre, E.J.; Bessler, S. The treatment of dysmenorrhea with naproxen sodium: A report on two independent double-blind trials. Am. J. Obstet. Gynecol. 1977, 127, 818–823. [Google Scholar] [CrossRef]
- Hoffman, D. Central and peripheral pain generators in women with chronic pelvic pain: Patient centered assessment and treatment. Curr. Rheumatol. Rev. 2015, 11, 146–166. [Google Scholar] [CrossRef] [PubMed]
- Bouaziz, J.; Bar On, A.; Seidman, D.S.; Soriano, D. The Clinical Significance of Endocannabinoids in Endometriosis Pain Management. Cannabis. Cannabinoid. Res. 2017, 2, 72–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, C.; Clark, J.D.; Oh, U.; Vasko, M.R.; Wilcox, G.L.; Overland, A.C.; Vanderah, T.W.; Spencer, R.H. Peripheral mechanisms of pain and analgesia. Brain Res. Rev. 2009, 60, 90–113. [Google Scholar] [CrossRef] [Green Version]
- Borrelli, G.M.; Carvalho, K.I.; Kallas, E.G.; Mechsner, S.; Baracat, E.C.; Abrão, M.S. Chemokines in the pathogenesis of endometriosis and infertility. J. Reprod. Immunol. 2013, 98, 1–9. [Google Scholar] [CrossRef]
- Finas, D.; Hüppe, M.; Diedrich, K.; Kowalcek, I. Chronischer Unterbauchschmerz Am. Beispiel der Endometriose-Problempatientin in der Gynäkologie? Geburtshilfe Frauenheilkd. 2005, 65, 156–163. [Google Scholar] [CrossRef]
- Gonçalves, A.V.; Barros, N.F.; Bahamondes, L. The Practice of Hatha Yoga for the Treatment of Pain Associated with Endometriosis. J. Altern. Complement. Med. 2017, 23, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Wienhard, J.; Tinneberg, H.R. Alternative treatment possibilities of complaints due to endometriosis. Zentralbl. Gynakol. 2003, 125, 286–289. [Google Scholar] [CrossRef]
- Krabbenborg, I.; de Roos, N.; van der Grinten, P.; Nap, A. Diet quality and perceived effects of dietary changes in Dutch endometriosis patients: An observational study. Reprod. Biomed. Online 2021, 43, 952–961. [Google Scholar] [CrossRef]
- Ata, B.; Yildiz, S.; Turkgeldi, E.; Brocal, V.P.; Dinleyici, E.C.; Moya, A.; Urman, B. The Endobiota Study: Comparison of Vaginal, Cervical and Gut Microbiota Between Women with Stage 3/4 Endometriosis and Healthy Controls. Sci. Rep. 2019, 9, 2204. [Google Scholar] [CrossRef] [Green Version]
- Nodler, J.L.; DiVasta, A.D.; Vitonis, A.F.; Karevicius, S.; Malsch, M.; Sarda, V.; Fadayomi, A.; Harris, H.R.; Missmer, S.A. Supplementation with vitamin D or ω-3 fatty acids in adolescent girls and young women with endometriosis (SAGE): A double-blind, randomized, placebo-controlled trial. Am. J. Clin. Nutr. 2020, 112, 229–236. [Google Scholar] [CrossRef]
- Lasco, A.; Catalano, A.; Benvenga, S. Improvement of primary dysmenorrhea caused by a single oral dose of vitamin D: Results of a randomized, double-blind, placebo-controlled study. Arch. Intern. Med. 2012, 172, 366–367. [Google Scholar] [CrossRef] [Green Version]
- Mariani, M.; Viganò, P.; Gentilini, D.; Camisa, B.; Caporizzo, E.; Di Lucia, P.; Monno, A.; Candiani, M.; Somigliana, E.; Panina-Bordignon, P. The selective vitamin D receptor agonist, elocalcitol, reduces endometriosis development in a mouse model by inhibiting peritoneal inflammation. Hum. Reprod. 2012, 27, 2010–2019. [Google Scholar] [CrossRef] [Green Version]
- Miyashita, M.; Koga, K.; Izumi, G.; Sue, F.; Makabe, T.; Taguchi, A.; Nagai, M.; Urata, Y.; Takamura, M.; Harada, M.; et al. Effects of 1,25-Dihydroxy Vitamin D3 on Endometriosis. J. Clin. Endocrinol. Metab. 2016, 101, 2371–2379. [Google Scholar] [CrossRef] [Green Version]
- Barcena de Arellano, M.L.; Mechsner, S. The peritoneum—An important factor for pathogenesis and pain generation in endometriosis. J. Mol. Med. 2014, 92, 595–602. [Google Scholar] [CrossRef]
- Campo, S.; Campo, V.; Benagiano, G. Adenomyosis and infertility. Reprod. Biomed. Online 2012, 24, 35–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapron, C.; Pietin-Vialle, C.; Borghese, B.; Davy, C.; Foulot, H.; Chopin, N. Associated ovarian endometrioma is a marker for greater severity of deeply infiltrating endometriosis. Fertil. Steril. 2009, 92, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Cousins, F.L.; Gargett, C.E. Endometrial stem/progenitor cells and their role in the pathogenesis of endometriosis. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 50, 27–38. [Google Scholar] [CrossRef]
- De Graaff, A.A.; D’Hooghe, T.M.; Dunselman, G.A.; Dirksen, C.D.; Hummelshoj, L.; Simoens, S. The significant effect of endometriosis on physical, mental and social wellbeing: Results from an international cross-sectional survey. Hum. Reprod. 2013, 28, 2677–2685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Ziegler, D.; Borghese, B.; Chapron, C. Endometriosis and infertility: Pathophysiology and management. Lancet 2010, 376, 730–738. [Google Scholar] [CrossRef]
- Berman, B.M.; Langevin, H.M.; Witt, C.M.; Dubner, R. Acupuncture for chronic low back pain. N. Engl. J. Med. 2010, 363, 454–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lund, I.; Lundeberg, T. Is acupuncture effective in the treatment of pain in endometriosis? J. Pain Res. 2016, 9, 157–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, R. Botulinum Toxin to Treat Endometriosis Pain. JAMA 2019, 322, 716. [Google Scholar] [CrossRef] [PubMed]
- Weinschenk, S. Neuraltherapie in der Frauenheilkunde—Update 2016. Geburtshilfe Frauenheilkd. 2016, 76, 507–512. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mechsner, S. Endometriosis, an Ongoing Pain—Step-by-Step Treatment. J. Clin. Med. 2022, 11, 467. https://doi.org/10.3390/jcm11020467
Mechsner S. Endometriosis, an Ongoing Pain—Step-by-Step Treatment. Journal of Clinical Medicine. 2022; 11(2):467. https://doi.org/10.3390/jcm11020467
Chicago/Turabian StyleMechsner, Sylvia. 2022. "Endometriosis, an Ongoing Pain—Step-by-Step Treatment" Journal of Clinical Medicine 11, no. 2: 467. https://doi.org/10.3390/jcm11020467
APA StyleMechsner, S. (2022). Endometriosis, an Ongoing Pain—Step-by-Step Treatment. Journal of Clinical Medicine, 11(2), 467. https://doi.org/10.3390/jcm11020467