
Early Spirometry Following Bronchoscopic Lung Volume Reduction with Endobronchial Valves

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
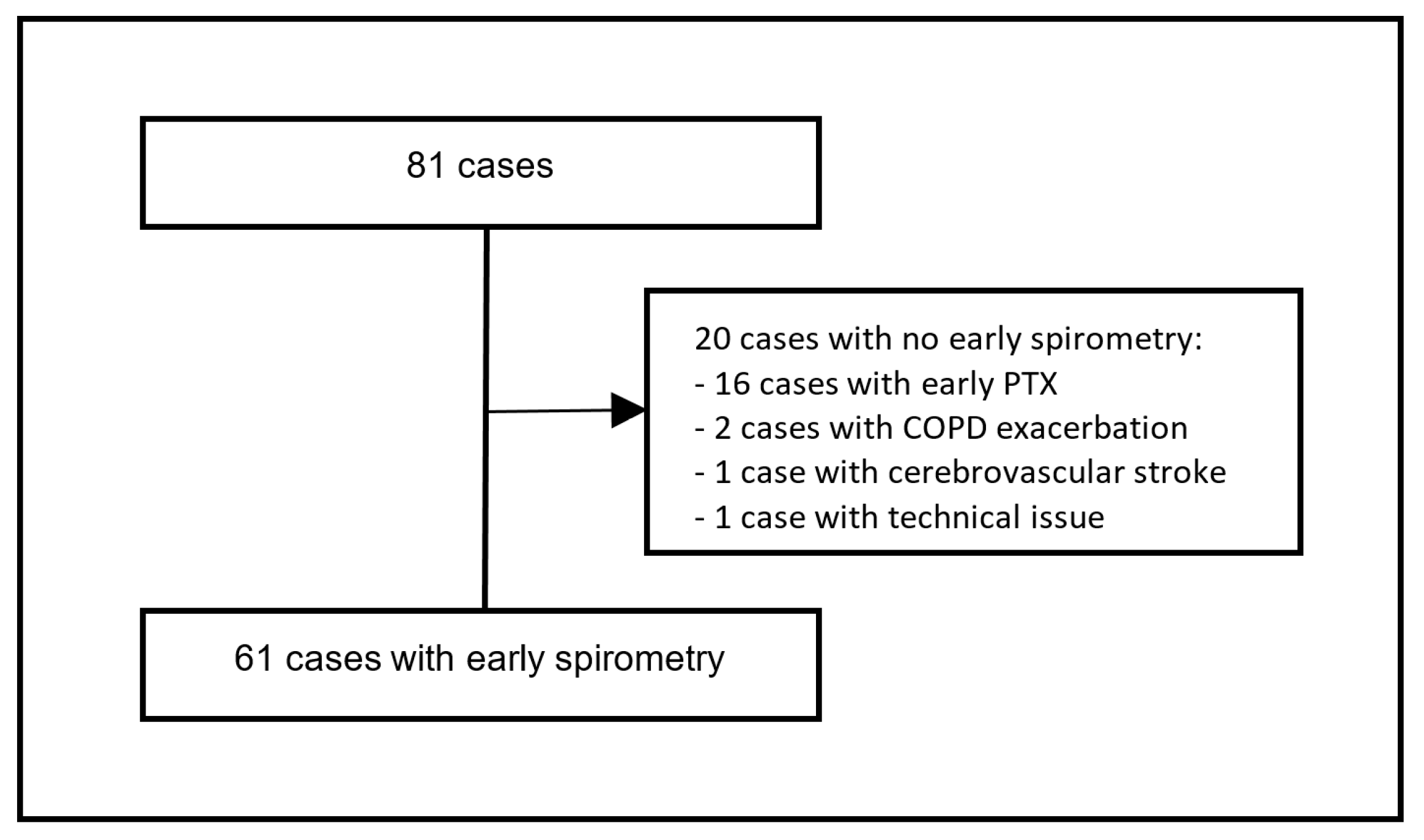
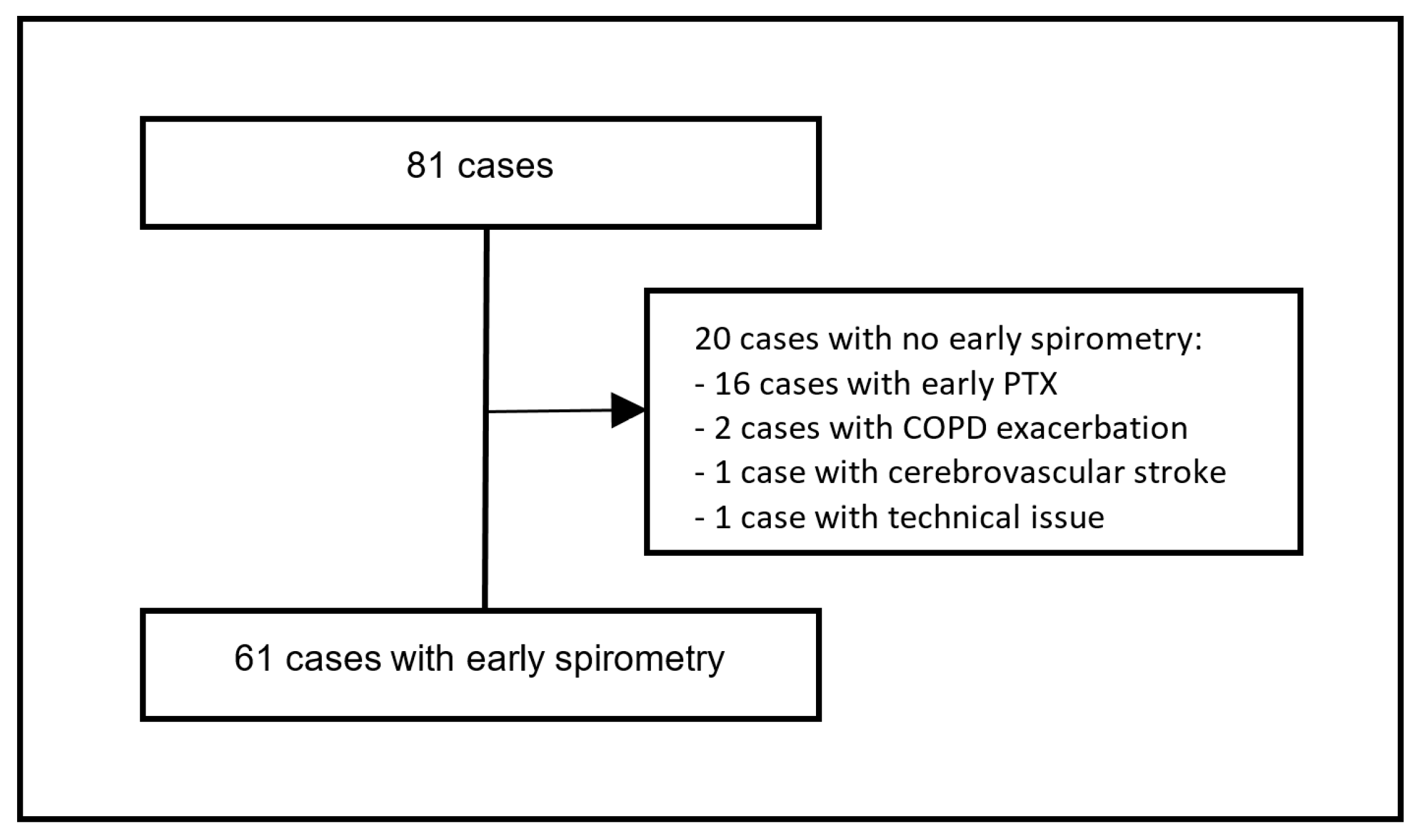
2.2. Patient Selection
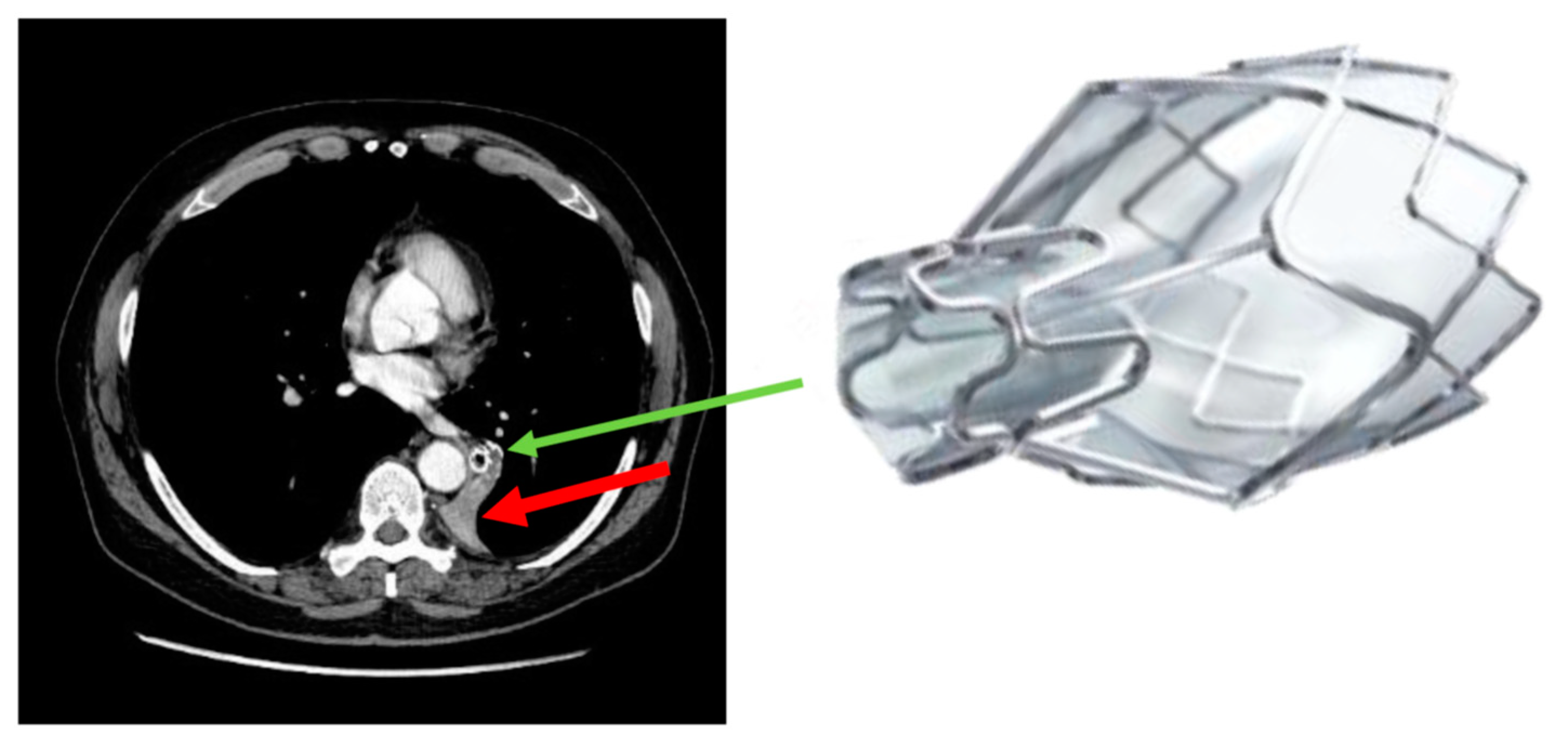
2.3. Bronchoscopy and Post-Interventional Care
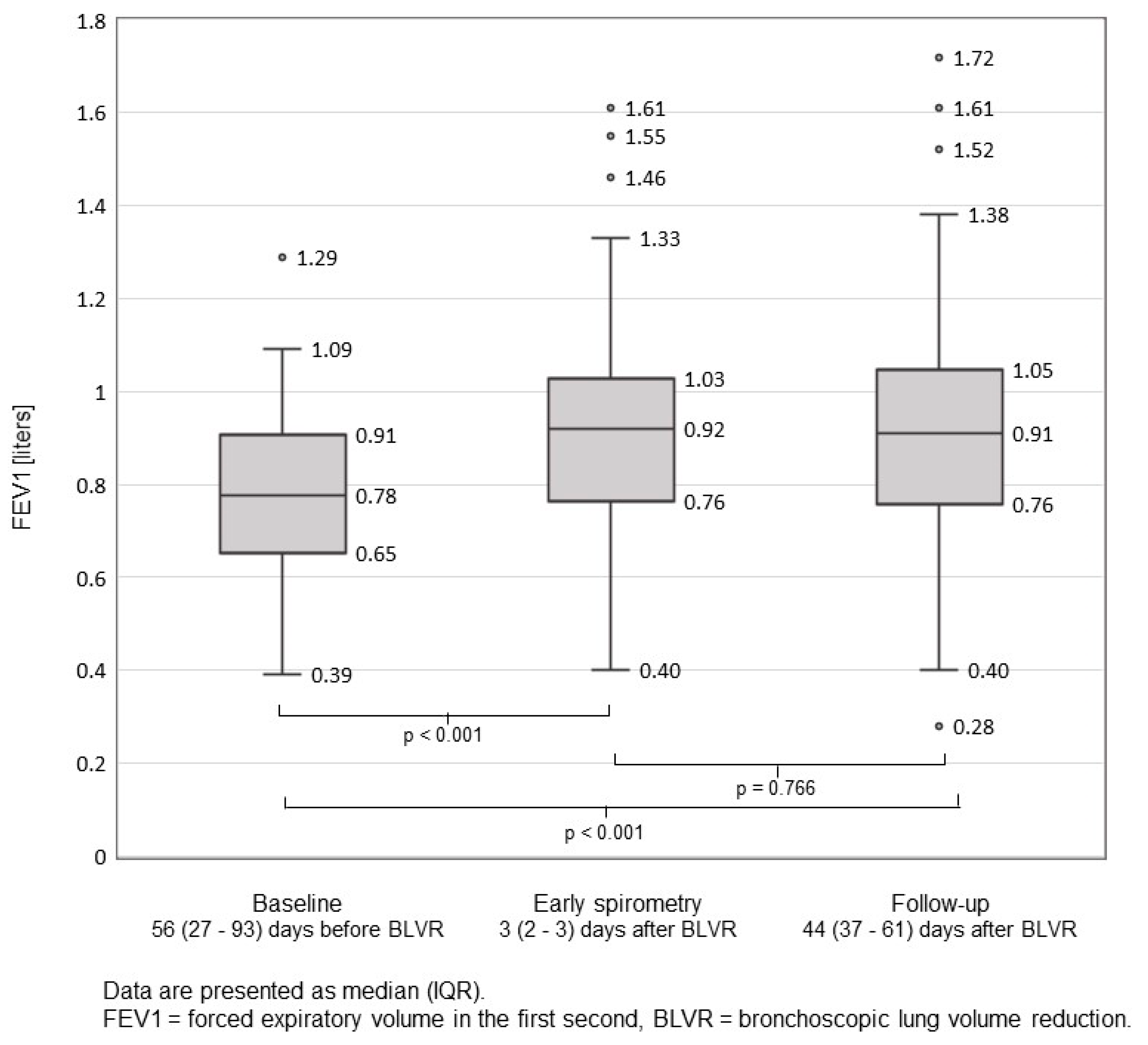
2.4. Spirometry
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
Pneumothorax
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shah, P.L.; Herth, F.J.; van Geffen, W.H.; Deslee, G.; Slebos, D.-J. Lung volume reduction for emphysema. Lancet Respir. Med. 2017, 5, 147–156. [Google Scholar] [CrossRef]
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2021 Report). 2021. Available online: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf. (accessed on 8 November 2021).
- Klooster, K.; Hacken NHT ten Hartman, J.E.; Kerstjens, H.A.M.; van Rikxoort, E.M.; Slebos, D.-J. Endobronchial valves for emphysema without interlobar collateral ventilation. N. Engl. J. Med. 2015, 373, 2325–2335. [Google Scholar] [CrossRef] [PubMed]
- Valipour, A.; Slebos, D.J.; Herth, F.; Darwiche, K.; Wagner, M.; Ficker, J.H.; Petermann, C.; Hubner, R.H.; Stanzel, F.; Eberhardt, R. Endobronchial valve therapy in patients with homogeneous emphysema. results from the IMPACT study. Am. J. Respir. Crit. Care Med. 2016, 194, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Kemp, S.V.; Slebos, D.J.; Kirk, A.; Kornaszewska, M.; Carron, K.; Ek, L.; Broman, G.; Hillerdal, G.; Mal, H.; Pison, C.; et al. A multicenter randomized controlled trial of zephyr endobronchial valve treatment in heterogeneous emphysema (TRANSFORM). Am. J. Respir. Crit. Care Med. 2017, 196, 1535–1543. [Google Scholar] [CrossRef] [PubMed]
- Davey, C.; Zoumot, Z.; Jordan, S.; McNulty, W.H.; Carr, D.H.; Hind, M.D.; Hansell, D.M.; Rubens, M.B.; Banya, W.; Polkey, M.I.; et al. Bronchoscopic lung volume reduction with endobronchial valves for patients with heterogeneous emphysema and intact interlobar fissures (the BeLieVeR-HIFi study): A randomised controlled trial. Lancet 2015, 386, 1066–1073. [Google Scholar] [CrossRef] [Green Version]
- Criner, G.J.; Sue, R.; Wright, S.; Dransfield, M.; Rivas-Perez, H.; Wiese, T.; Sciurba, F.C.; Shah, P.L.; Wahidi, M.M.; de Oliveira, H.G.; et al. A Multicenter RCT of Zephyr® endobronchial valve treatment in heterogeneous emphysema (LIBERATE). Am. J. Respir. Crit. Care Med. 2018, 198, 1151–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herth, F.J.; Noppen, M.; Valipour, A.; Leroy, S.; Vergnon, J.M.; Ficker, J.H.; Egan, J.J.; Gasparini, S.; Agusti, C.; Holmes-Higgin, D.; et al. Efficacy predictors of lung volume reduction with Zephyr valves in a European cohort. Eur. Respir. J. 2012, 39, 1334–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franzen, D.; Straub, G.; Freitag, L. Complications after bronchoscopic lung volume reduction. J. Thorac. Dis. 2018, 10 (Suppl. 23), S2811–S2815. [Google Scholar] [CrossRef] [PubMed]
- Valipour, A.; Slebos, D.J.; De Oliveira, H.G.; Eberhardt, R.; Freitag, L.; Criner, G.J.; Herth, F.J. Expert statement: Pneumothorax associated with endoscopic valve therapy for emphysema--potential mechanisms, treatment algorithm, and case examples. Respiration 2014, 87, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Gompelmann, D.; Lim, H.J.; Eberhardt, R.; Gerovasili, V.; Herth, F.J.; Heussel, C.P.; Eichinger, M. Predictors of pneumothorax following endoscopic valve therapy in patients with severe emphysema. Int. J. Chron. Obstruct. Pulmon. Dis. 2016, 11, 1767–1773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herzog, D.; Poellinger, A.; Doellinger, F.; Schuermann, D.; Temmesfeld-Wollbrueck, B.; Froeling, V.; Schreiter, N.F.; Neumann, K.; Hippenstiel, S.; Suttorp, N.; et al. Modifying Post-operative medical care after ebv implant may reduce pneumothorax incidence. PLoS ONE 2015, 10, e0128097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slebos, D.-J.; Shah, P.L.; Herth, F.J.F.; Valipour, A. Endobronchial valves for endoscopic lung volume reduction: Best practice recommendations from expert panel on endoscopic lung volume reduction. Respiration 2017, 93, 138–150. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.A.T.S.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; Van Der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dejene, S.; Ahmed, F.; Jack, K.; Anthony, A. Pneumothorax, music and balloons: A case series. Ann. Thorac. Med. 2013, 8, 176–178. [Google Scholar] [CrossRef] [PubMed]
- Casha, A.R.; Manché, A.; Gatt, R.; Wolak, W.; Dudek, K.; Gauci, M.; Schembri-Wismayer, P.; Camilleri-Podesta, M.T.; Grima, J.N. Is there a biomechanical cause for spontaneous pneumothorax? Eur. J. Cardio-Thorac. Surg. 2014, 45, 1011–1016. [Google Scholar] [CrossRef] [PubMed]
- Cran, I.R.; Rumball, C.A. Survey of spontaneous pneumothoraces in the royal air force. Thorax 1967, 22, 462–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bense, L.; Wiman, L.G.; Hedenstierna, G. Onset of symptoms in spontaneous pneumothorax: Correlations to physical activity. Eur. J. Respir. Dis. 1987, 71, 181–186. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Demographic Data | ||
| Age, years | 69.0 | (62.9–74.4) |
| Male gender | 30 | (45) |
| Height | 166 | (162–171.8) |
| Weight | 59 | (52–71.8) |
| BMI | 22.4 | (19.3–24.6) |
| EBV Implantation | ||
| Number of EBVs implanted per patient | 5 | (4–6) |
| Volume of target lobe *, mL | 1510 | (1277.5–1817) |
| Target lobe | ||
| Left lower lobe | 29 | (43.9) |
| Left upper lobe | 29 | (43.9) |
| Right lower lobe | 2 | (3.0) |
| Middle lobe | 1 | (1.5) |
| Right upper lobe | 6 | (9.1) |
| Baseline PFT and 6-MWD | ||
| FEV1, L | 0.75 | (0.56–0.91) |
| FEV1, % predicted | 29 | (23–34) |
| RV, L | 5.09 | (4.36–5.66) |
| RV, % predicted | 230 | (199–258) |
| RV/TLC, % | 69 | (63–74) |
| DLCO, mmol/kPa/min | 2.4 | (1.9–2.9) |
| DLCO, % | 30 | (25–38) |
| 6-MWD, m | 300 | (225–368) |
| Post Procedural PTX before Early Spirometry | ||
| Same day | 7 | (43.8) |
| 1st day | 6 | (37.5) |
| 2nd day | 2 | (12.5) |
| 3rd day | 1 | (6.3) |
| Clinically Relevant PTX during or after Early Spirometry | ||
| PTX during Spirometry | 0 | (0) |
| PTX after Spirometry | 0 | (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bezel, P.; Wani, J.; Wiederkehr, G.; Bodmer, C.; Steinack, C.; Franzen, D.P. Early Spirometry Following Bronchoscopic Lung Volume Reduction with Endobronchial Valves. J. Clin. Med. 2022, 11, 440. https://doi.org/10.3390/jcm11020440
Bezel P, Wani J, Wiederkehr G, Bodmer C, Steinack C, Franzen DP. Early Spirometry Following Bronchoscopic Lung Volume Reduction with Endobronchial Valves. Journal of Clinical Medicine. 2022; 11(2):440. https://doi.org/10.3390/jcm11020440
Chicago/Turabian StyleBezel, Pascal, Jasmin Wani, Gilles Wiederkehr, Christa Bodmer, Carolin Steinack, and Daniel P. Franzen. 2022. "Early Spirometry Following Bronchoscopic Lung Volume Reduction with Endobronchial Valves" Journal of Clinical Medicine 11, no. 2: 440. https://doi.org/10.3390/jcm11020440
APA StyleBezel, P., Wani, J., Wiederkehr, G., Bodmer, C., Steinack, C., & Franzen, D. P. (2022). Early Spirometry Following Bronchoscopic Lung Volume Reduction with Endobronchial Valves. Journal of Clinical Medicine, 11(2), 440. https://doi.org/10.3390/jcm11020440