
Clinical Characteristics and Predictors of In-Hospital Mortality among Older Patients with Acute Heart Failure


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.1.1. Case Identification and Categorization
2.1.2. Data Source
2.1.3. Patients’ Characteristics
2.1.4. Established Comorbid Medical Diagnoses
2.1.5. Pharmacological Treatment
2.1.6. Acute Medical Conditions
2.2. Outcome Measures
2.3. Statistics
3. Results
3.1. Study Sample
3.1.1. Sociodemographic Characteristics
3.1.2. Clinical Variables
3.1.3. Comorbid Medical Diagnoses
3.1.4. Pharmacological Treatment
3.1.5. Acute Medical Conditions
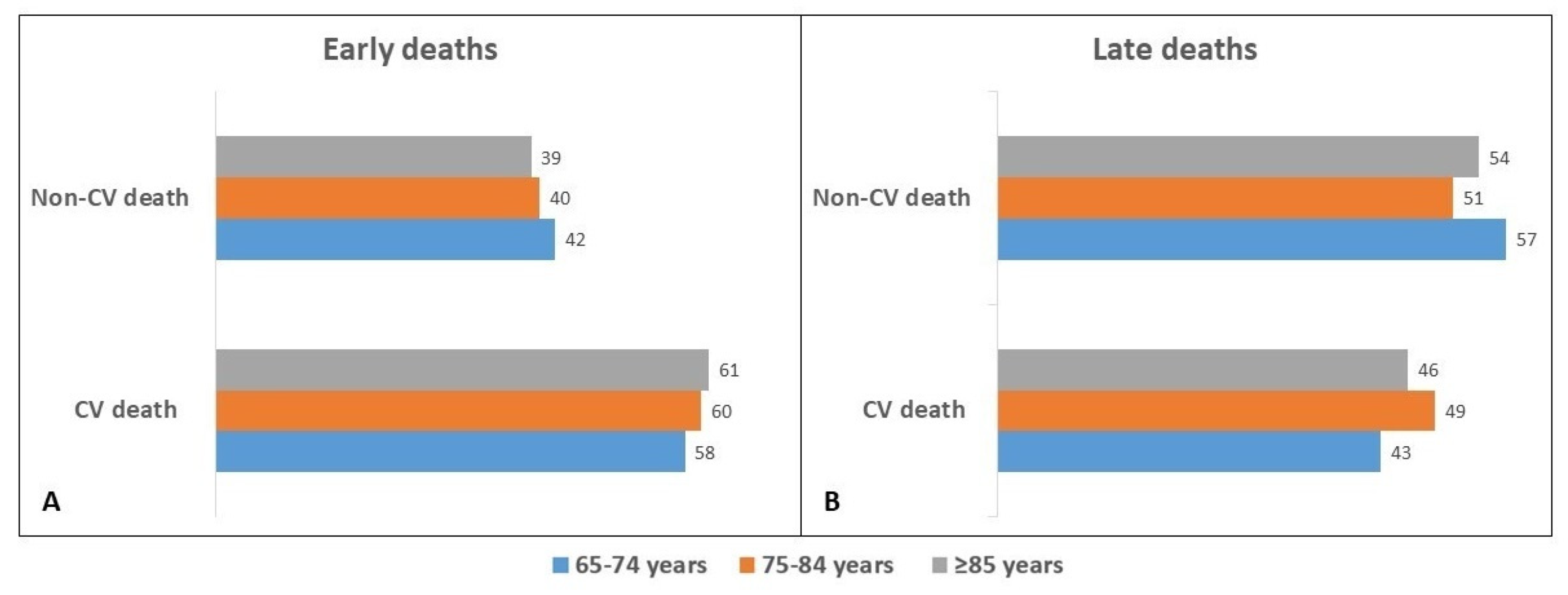
3.1.6. In-Hospital Death
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mizuno, M.; Kajimoto, K.; Sato, N.; Yumino, D.; Minami, Y.; Murai, K.; Munakata, R.; Asai, K.; Keida, T.; Sakata, Y.; et al. Clinical profile, management, and mortality in very elderly patients hospitalized with acute decompensated heart failure. An analysis from the ATTEND registry. Eur. J. Intern. Med. 2016, 27, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Adams, K.F., Jr.; Fonarow, G.C.; Emerman, C.L.; LeJemtel, T.H.; Costanzo, M.R.; Abraham, W.T.; Berkowitz, R.L.; Galvao, M.; Horton, D.P. Characteristics and outcomes of patients hospitalized for heart failure in the United States: Rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am. Heart J. 2005, 149, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.G.; Swedberg, K.; Follath, F.; Komajda, M.; Cohen-Solal, A.; Aguilar, J.C.; Dietz, R.; Gavazzi, A.; Hobbs, R.; Korewicki, J.; et al. The EuroHeart Failure survey programme-a survey on the quality of care among patients with heart failure in Europe. Part 1: Patient characteristics and diagnosis. Eur. Heart J. 2003, 24, 442–463. [Google Scholar] [CrossRef] [Green Version]
- Nieminen, M.S.; Brutsaert, D.; Dickstein, K.; Drexler, H.; Follath, F.; Harjola, V.P.; Hochadel, M.; Komajda, M.; Lassus, J.; Lopez-Sendon, J.L.; et al. EuroHeart Failure Survey II (EHFS II): A survey on hospitalized acute heart failure patients: Description of population. Eur. Heart J. 2006, 27, 2725–2736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliva, F.; Mortara, A.; Cacciatore, G.; Chinaglia, A.; Di Lenarda, A.; Gorini, M.; Metra, M.; Senni, M.; Maggioni, A.; Tavazzi, L.; et al. Acute heart failure patient profiles, management and in-hospital outcome: Results of the Italian Registry on Heart Failure Outcome. Eur. J. Heart Fail. 2012, 14, 1208–1217. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar]
- Conrad, N.; Judge, A.; Canoy, D.; Tran, J.; Pinho-Gomes, A.C.; Millett, E.R.C.; Salimi-Khorshidi, G.; Cleland, J.G.; McMurray, J.J.V.; Rahimi, K. Temporal trends and patterns in mortality after incident heart failure: A longitudinal analysis of 86,000 individuals. JAMA Cardiol. 2019, 4, 1102–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Deursen, V.M.; Urso, R.; Laroche, C.; Damman, K.; Dahlström, U.; Tavazzi, L.; Maggioni, A.P.; Voors, A.A. Co-morbidities in patients with heart failure: An analysis of the European Heart Failure Pilot Survey. Eur. J. Heart Fail. 2014, 16, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Zhao, X.; Hammill, B.G.; Hernandez, A.F.; Fonarow, G.C.; Felker, G.M.; Yancy, C.W.; Heidenreich, P.A.; Ezekowitz, J.A.; DeVore, A.D. Trends in noncardiovascular comorbidities among patients hospitalized for heart failure: Insights from the get with the guidelines-Heart Failure Registry. Circ. Heart Fail. 2018, 11, e004646. [Google Scholar] [CrossRef] [PubMed]
- Ueda, T.; Kawakami, R.; Horii, M.; Sugawara, Y.; Matsumoto, T.; Okada, S.; Nishida, T.; Soeda, T.; Okayama, S.; Somekawa, S.; et al. Noncardiovascular death, especially infection, is a significant cause of death in elderly patients with acutely decompensated heart failure. J. Card. Fail. 2014, 20, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Rossello, X.; Gil, V.; Escoda, R.; Jacob, J.; Aguirre, A.; Martín-Sánchez, F.J.; Llorens, P.; Herrero Puente, P.; Rizzi, M.; Raposeiras-Roubín, S.; et al. Impact of identifying precipitating factors on 30-day mortality in acute heart failure patients. Eur. Heart J. Acute Cardiovasc. Care 2019, 8, 667–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orr, N.M.; Forman, D.E.; De Matteis, G.; Gambassi, G. Heart failure among older adults in skilled nursing facilities: More of a dilemma than many now realize. Curr. Geriatr. Rep. 2015, 4, 318–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maggioni, A.; Irso, F.; Calabria, S.; Rossi, E.; Cinconze, E.; Baldasseroni, S.; Marini, N. The real-world evidence of heart failure: Findings from 41,413 patients of the ARNO database. Eur. J. Heart Fail. 2016, 18, 402–410. [Google Scholar] [CrossRef]
- Abraham, W.T.; Fonarow, G.C.; Albert, N.M.; Stough, W.G.; Gheorghiade, M.; Greenberg, B.H.; O’Connor, C.M.; Sun, J.L.; Yancy, C.W.; Young, J.B.; et al. Predictors of in-hospital mortality in patients hospitalized for heart failure: Insights from the organized program to initiate lifesaving treatment in hospitalized patients with heart failure (OPTIMIZE-HF). J. Am. Coll. Cardiol. 2008, 52, 347–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logeart, D.; Isnard, R.; Resche-Rigon, M.; Seronde, M.F.; de Groote, P.; Jondeau, G.; Galinier, M.; Mulak, G.; Donal, E.; Delahaye, F.; et al. Current aspects of the spectrum of acute heart failure syndromes in a real-life setting: The OFICA study. Eur. J. Heart Fail. 2013, 15, 465–476. [Google Scholar] [CrossRef] [Green Version]
- Mogensen, U.M.; Ersbøll, M.; Andersen, M.; Andersson, C.; Hassager, C.; Torp-Pedersen, C.; Gustafsson, F.; Køber, L. Clinical characteristics and major comorbidities in heart failure patients more than 85 years of age compared with younger age groups. Eur. J. Heart Fail. 2011, 13, 1216–1223. [Google Scholar] [CrossRef] [PubMed]
- Fernández Gassó, M.L.; Hernando-Arizaleta, L.; Palomar-Rodríguez, J.A.; Soria-Arcos, F.; Pascual-Figal, D.A. Trends and characteristics of hospitalization for heart failure in a population setting from 2003 to 2013. Rev. Esp. Cardiol. 2017, 70, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Conrad, N.; Judge, A.; Tran, J.; Mohseni, H.; Hedgecott, D.; Crespillo, A.P.; Allison, M.; Hemingway, H.; Cleland, J.G.; McMurray, J.J.V.; et al. Temporal trends and patterns in heart failure incidence: A population-based study of 4 million individuals. Lancet 2018, 391, 572–580. [Google Scholar] [CrossRef] [Green Version]
- Komajda, M.; Hanon, O.; Hochadel, M.; Follath, F.; Swedberg, K.; Gitt, A.; Cleland, J.G. Management of octogenarians hospitalized for heart failure in Euro Heart Failure Survey I. Eur. Heart J. 2007, 28, 1310–1318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricciardi, E.; La Malfa, G.; Guglielmi, G.; Cenni, E.; Micali, M.; Corsello, L.M.; Lopena, P.; Manco, L.; Pontremoli, R.; Moscatelli, P.; et al. Characteristics of current heart failure patients admitted to internal medicine vs cardiology hospital units: The VASCO study. Intern. Emerg. Med. 2020, 15, 1219–1229. [Google Scholar] [CrossRef]
- Maymon, S.L.; Moravsky, G.; Marcus, G.; Shuvy, M.; Pereg, D.; Epstein, D.; Litovchik, I.; Fuchs, S.; Minha, S. Disparities in the characteristics and outcomes of patients hospitalized with acute decompensated heart failure admitted to internal medicine and cardiology departments: A single-centre, retrospective cohort study. ESC Heart Fail. 2021, 8, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.; Klabunde, C.N.; Yabroff, K.R.; Wang, Z.; Meekins, A.; Lansdorp-Vogelaar, I.; Mariotto, A.B. Comorbidity-adjusted life expectancy: A new tool to inform recommendations for optimal screening strategies. Ann. Intern. Med. 2013, 159, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Holmström, A.; Sigurjonsdottir, R.; Edner, M.; Jonsson, A.; Dahlström, U.; Fu, M.L. Increased comorbidities in heart failure patients ≥85 years but declined from >90 years: Data from the Swedish Heart Failure Registry. Int. J. Cardiol. 2013, 167, 2747–2752. [Google Scholar] [CrossRef]
- Shah, R.U.; Tsai, V.; Klein, L.; Heidenreich, P.A. Characteristics and outcomes of very elderly patients after first hospitalization for heart failure. Circ. Heart Fail. 2011, 4, 301–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mebazaa, A.; Yilmaz, M.B.; Levy, P.; Ponikowski, P.; Peacock, W.F.; Laribi, S.; Ristic, A.D.; Lambrinou, E.; Masip, J.; Riley, J.P.; et al. Recommendations on pre-hospital and early hospital management of acute heart failure. Eur. J. Heart Fail. 2015, 17, 544–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arrigo, M.; Gayat, E.; Parenica, J.; Ishihara, S.; Zhang, J.; Choi, D.J.; Park, J.J.; Alhabib, K.F.; Sato, N.; Miro, O.; et al. Precipitating factors and 90-day outcome of acute heart failure: A report from the intercontinental GREAT registry. Eur. J. Heart Fail. 2017, 19, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Arrigo, M.; Tolppanen, H.; Sadoune, M.; Feliot, E.; Teixeira, A.; Laribi, S.; Plaisance, P.; Nouira, S.; Yilmaz, M.B.; Gayat, E.; et al. Effect of precipitating factors of acute heart failure on readmission and long-term mortality. ESC Heart Fail. 2016, 3, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, A.; Arrigo, M.; Tolppanen, H.; Gayat, E.; Laribi, S.; Metra, M.; Seronde, M.F.; Cohen-Solal, A.; Mebazaa, A. Management of acute heart failure in elderly patients. Arch. Cardiovasc. Dis. 2016, 109, 422–430. [Google Scholar] [CrossRef]
- Pandey, A.; Vaduganathan, M.; Arora, S.; Qamar, A.; Mentz, R.J.; Shah, S.J.; Chang, P.P.; Russell, S.D.; Rosamond, W.D.; Caughey, M.C. Temporal trends in prevalence and prognostic implications of comorbidities among patients with acute decompensated heart failure: The ARIC study community surveillance. Circulation 2020, 142, 230–243. [Google Scholar] [CrossRef]
- Vergaro, G.; Ghionzoli, N.; Innocenti, L.; Taddei, C.; Giannoni, A.; Valleggi, A.; Borrelli, C.; Senni, M.; Passino, C.; Emdin, M. Noncardiac versus cardiac mortality in heart failure with preserved, midrange, and reduced ejection fraction. J. Am. Heart Assoc. 2019, 8, e013441. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.M.N.; Drozd, M.; Hall, M.; Patel, P.A.; Paton, M.; Lowry, J.; Gierula, J.; Byrom, R.; Kearney, L.; Sapsford, R.J.; et al. Prevalence and predictors of sepsis death in patients with chronic heart failure and reduced left ventricular ejection fraction. J. Am. Heart Assoc. 2018, 7, e009684. [Google Scholar] [CrossRef] [Green Version]
- De Groote, P.; Lamblin, N.; Mouquet, F.; Plichon, D.; McFadden, E.; Van Belle, E.; Bauters, C. Impact of diabetes mellitus on long-term survival in patients with congestive heart failure. Eur. Heart J. 2004, 25, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Passantino, A.; Monitillo, F.; Iacoviello, M.; Scrutinio, D. Predicting mortality in patients with acute heart failure: Role of risk scores. World J. Cardiol. 2015, 7, 902–911. [Google Scholar] [CrossRef] [PubMed]
- Harjola, V.P.; Parissis, J.; Bauersachs, J.; Brunner-La Rocca, H.P.; Bueno, H.; Čelutkienė, J.; Chioncel, O.; Coats, A.J.S.; Collins, S.P.; de Boer, R.A.; et al. Acute coronary syndromes and acute heart failure: A diagnostic dilemma and high-risk combination. A statement from the Acute Heart Failure Committee of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 1298–1314. [Google Scholar] [CrossRef] [PubMed]
- Damman, K.; Valente, M.A.; Voors, A.A.; O’Connor, C.M.; van Veldhuisen, D.J.; Hillege, H.L. Renal impairment, worsening renal function, and outcome in patients with heart failure: An updated meta-analysis. Eur. Heart J. 2014, 35, 455–469. [Google Scholar] [CrossRef] [Green Version]
- Hayıroğlu, M.İ.; Bozbeyoglu, E.; Yıldırımtürk, Ö.; Tekkeşin, A.İ.; Pehlivanoğlu, S. Effect of acute kidney injury on long-term mortality in patients with ST-segment elevation myocardial infarction complicated by cardiogenic shock who underwent primary percutaneous coronary intervention in a high-volume tertiary center. Türk Kardiyoloji Derneği Arşivi 2020, 48, 1–9. [Google Scholar] [CrossRef]
- Hayıroğlu, M.İ.; Çanga, Y.; Yıldırımtürk, Ö.; Bozbeyoğlu, E.; Gümüşdağ, A.; Uzun, A.O.; Kalenderoğlu, K.; Keskin, M.; Çinier, G.; Acarel, M.; et al. Clinical characteristics and outcomes of acute coronary syndrome patients with intra-aortic balloon pump inserted in intensive cardiac care unit of a tertiary clinic. Türk Kardiyoloji Derneği Arşivi 2018, 46, 10–17. [Google Scholar]
- Alon, D.; Stein, G.Y.; Korenfeld, R.; Fuchs, S. Predictors and outcomes of infection-related hospital admissions of heart failure patients. PLoS ONE 2013, 8, e72476. [Google Scholar] [CrossRef]
- Drozd, M.; Garland, E.; Walker, A.M.N.; Slater, T.A.; Koshy, A.; Straw, S.; Gierula, J.; Paton, M.; Lowry, J.; Sapsford, R.; et al. Infection-related hospitalization in heart failure with reduced ejection fraction. A prospective observational cohort study. Circ. Heart Fail. 2020, 13, e006746. [Google Scholar] [CrossRef]
- Seko, Y.; Kato, T.; Morimoto, T.; Yaku, H.; Inuzuka, Y.; Tamaki, Y.; Ozasa, N.; Shiba, M.; Yamamoto, E.; Yoshikawa, Y.; et al. Newly diagnosed infection after admission for acute heart failure: From the KCHF registry. J. Am. Heart Assoc. 2021, 10, e023256. [Google Scholar] [CrossRef]


{kind=link}
| 65–74 Years (n = 1464) | 75–84 Years (n = 2975) | ≥85 Years (n = 2491) | All (n = 6930) | p Value | |
|---|---|---|---|---|---|
| Age (years) | 70.2 ± 2.8 | 79.8 ± 2.8 | 89.0 ± 3.4 | 81.1 ± 7.5 | <0.001 |
| Female | 38.6 | 49.3 | 59.1 | 50.6 | <0.001 |
| Clinical symptoms/signs | |||||
| Dyspnea | 66.4 | 64.9 | 64.7 | 65.1 | 0.521 |
| Peripheral edema | 25.8 | 25.5 | 23.8 | 24.9 | 0.277 |
| Chest pain | 15.8 | 12.8 | 9.4 | 12.2 | <0.001 |
| NYHA class | |||||
| II | 20.2 | 20.9 | 18.4 | 19.9 | |
| III | 70.4 | 68.6 | 69.5 | 69.3 | 0.023 |
| IV | 9.4 | 10.5 | 12.1 | 10.8 | |
| Vital parameters | |||||
| Systolic blood pressure (mmHg) | 138 ± 30 | 137 ± 29 | 137 ± 29 | 137 ± 29 | 0.538 |
| Diastolic blood pressure (mmHg) | 77 ± 17 | 76 ± 18 | 75 ± 17 | 76 ± 17 | 0.006 |
| Heart Rate (beats/min) | 88 ± 23 | 86 ± 23 | 86 ± 22 | 86 ± 23 | <0.001 |
| O2 saturation | 93 ± 5 | 93 ± 6 | 92 ± 6 | 93 ± 6 | <0.001 |
| Number of comorbidities | |||||
| 0–1 | 24.2 | 2.3 | 2.2 | 6.9 | |
| 2–3 | 36.0 | 61.6 | 55.8 | 54.1 | <0.001 |
| 4+ | 39.8 | 36.1 | 42.0 | 39.0 | |
| CV comorbidities | |||||
| Coronary artery disease | 51.9 | 51.1 | 42.0 | 48.0 | <0.001 |
| Prior coronary revascularization | 20.7 | 17.6 | 10.6 | 15.7 | <0.001 |
| Hypertension | 50.1 | 54.8 | 53.7 | 53.4 | 0.016 |
| Valve disease | 25.6 | 21.6 | 18.9 | 21.5 | <0.001 |
| Chronic atrial fibrillation | 40.6 | 45.2 | 47.3 | 44.9 | <0.001 |
| Pacemaker/ICD | 20.2 | 21.2 | 19.2 | 20.3 | 0.190 |
| Cerebrovascular disease | 6.1 | 8.9 | 8.1 | 8.1 | 0.004 |
| Non-CV comorbidities | |||||
| Diabetes | 37.1 | 32.9 | 23.5 | 30.4 | <0.001 |
| Chronic obstructive pulmonary disease | 25.3 | 32.2 | 31.4 | 30.4 | <0.001 |
| Chronic kidney disease | 42.8 | 44.3 | 41.5 | 43.0 | 0.208 |
| Chronic Liver disease | 3.8 | 2.1 | 0.8 | 2.0 | <0.001 |
| Cancer | 11.7 | 9.1 | 7.7 | 9.2 | 0.021 |
| Dementia | 0.6 | 4.0 | 8.4 | 4.8 | <0.001 |
| Medications | |||||
| Loop Diuretics | 75.3 | 77.7 | 76.5 | 76.8 | 0.097 |
| ACE-I/ARBs | 47.9 | 49.3 | 45.8 | 47.7 | 0.145 |
| β-Blockers | 64.4 | 61.5 | 53.1 | 59.0 | <0.001 |
| Mineralocorticoid antagonists | 28.2 | 22.8 | 21.5 | 23.4 | 0.001 |
| Digoxin | 12.5 | 12.7 | 14.1 | 13.2 | 0.214 |
| Calcium Channel Blockers | 14.6 | 17.2 | 16.0 | 16.2 | 0.286 |
| Antiarrhythmic drugs | 14.0 | 13.4 | 10.8 | 12.6 | 0.018 |
| Oral anticoagulants | 41.4 | 40.1 | 31.9 | 37.4 | <0.001 |
| Statins | 30.6 | 29.3 | 17.2 | 25.2 | <0.001 |
| 65–74 Years (n = 1464) | 75–84 Years (n = 2975) | ≥85 Years (n = 2491) | All (n = 6930) | p Value | |
|---|---|---|---|---|---|
| Precipitating factors | |||||
| At least one | 63.5 | 65.8 | 72.7 | 67.8 | <0.001 |
| Not identified | 36.5 | 34.2 | 27.3 | 32.2 | |
| Acute medical conditions | |||||
| Uncontrolled blood pressure | 20.4 | 20.0 | 21.4 | 20.6 | 0.438 |
| Acute coronary syndrome | 3.2 | 3.2 | 4.0 | 3.5 | 0.227 |
| Acute pulmonary embolism | 0.8 | 0.8 | 1.2 | 0.9 | 0.245 |
| New-onset atrial fibrillation | 14.5 | 13.4 | 13.6 | 13.7 | 0.115 |
| Stroke | 1.6 | 2.8 | 3.7 | 2.9 | 0.001 |
| Fever/febrile episodes | 5.5 | 5 | 5.3 | 5.3 | 0.766 |
| Infections | 20.2 | 25.4 | 29.9 | 25.9 | <0.001 |
| Pneumonia | 9.7 | 11.1 | 17.3 | 13.1 | <0.001 |
| COPD acute exacerbation | 4.6 | 7.0 | 6.3 | 6.2 | 0.011 |
| Urinary tract infection | 2.7 | 3.9 | 7.0 | 4.8 | <0.001 |
| Sepsis/bloodstream infection | 3.3 | 4.2 | 3.5 | 3.8 | 0.264 |
| Worsening renal function | 4.1 | 4.5 | 6.1 | 5.0 | 0.005 |
| Metabolic/Electrolyte derangement | 2.3 | 2.4 | 4.1 | 3.0 | <0.001 |
| Anemia | 5.4 | 5.3 | 5.1 | 5.3 | 0.905 |
| 65–74 Years (n = 1464) | 75–84 Years (n = 2975) | ≥85 Years (n = 2491) | All (n = 6930) | p | |
|---|---|---|---|---|---|
| Length of stay (days) | 11 (7–18) | 10 (7–17) | 9 (6–16) | 10 (6–16) | <0.001 |
| All-cause In-hospital mortality | 8 | 11 | 19 | 13 | <0.001 |
| Causes of death | |||||
| CV-related | 49.3 | 53.9 | 54.7 | 53.4 | 0.541 |
| Non-CV related | 50.7 | 46.1 | 45.3 | 46.6 | |
| CV/Non-CV ratio | 0.97 | 1.16 | 1.20 | 1.14 | |
| Time of death | |||||
| Early deaths | 41.4 | 44.2 | 59.1 | 51.2 | <0.001 |
| Non-CV related | 41.6 | 39.7 | 39.1 | 39.6 | |
| Late deaths | 58.6 | 55.8 | 40.9 | 48.8 | |
| Non-CV related | 57.3 | 51.3 | 53.8 | 53.3 |
| 65–74 Years | 75–84 Years | ≥85 Years | All | |||||
|---|---|---|---|---|---|---|---|---|
| Dead/Alive (116/1348) | p | Dead/Alive (342/2633) | p | Dead/Alive (450/2041) | p | Dead/Alive (908/6022) | p | |
| Age (deceased) | 71 (68–73) | 0.369 | 80 (78–83) | 0.012 | 88 (87–92) | 0.079 | 84 (79–88) | <0.001 |
| Female | 37.9 | 0.879 | 45.9 | 0.181 | 59.1 | 0.992 | 51.4 | 0.581 |
| NYHA class | ||||||||
| II | 14.7 | 14.6 | 8.9 | 11.8 | ||||
| III | 69.0 | 0.015 | 67.3 | <0.001 | 71.8 | <0.001 | 69.7 | <0.001 |
| IV | 16.4 | 18.1 | 19.3 | 18.5 | ||||
| Number of comorbidities | ||||||||
| 0–1 2–3 4+ | 19.8 44.0 36.2 | 0.162 | 11.7 51.8 36.5 | <0.001 | 11.1 50.4 38.4 | <0.001 | 12.4 50.1 37.4 | <0.001 |
| CV comorbidities | ||||||||
| Coronary artery disease | 66.4 | 0.001 | 57.9 | 0.007 | 44.2 | 0.281 | 52.2 | 0.006 |
| Hypertension | 58.6 | 0.063 | 57.3 | 0.339 | 57.8 | 0.059 | 57.7 | 0.007 |
| Valve disease | 28.4 | 0.547 | 27.2 | 0.036 | 22.7 | 0.142 | 25.1 | 0.044 |
| Chronic atrial fibrillation | 47.4 | 0.118 | 49.1 | 0.119 | 52.7 | 0.011 | 50.7 | <0.001 |
| Pacemaker/ICD | 24.1 | 0.273 | 19.6 | 0.445 | 16.0 | 0.058 | 18.4 | 0.133 |
| Cerebrovascular disease | 5.2 | 0.670 | 12.3 | 0.020 | 11.6 | 0.007 | 11.0 | 0.001 |
| Non-CV comorbidities | ||||||||
| Diabetes | 48.3 | 0.009 | 38.0 | 0.032 | 35.8 | <0.001 | 38.2 | <0.001 |
| COPD | 23.3 | 0.594 | 29.5 | 0.261 | 28.9 | 0.213 | 28.4 | 0.153 |
| Chronic kidney disease | 47.4 | 0.369 | 46.2 | 0.686 | 42.0 | 0.679 | 44.3 | 0.850 |
| Chronic Liver Disease | 1.7 | 0.230 | 3.2 | 0.134 | 2.7 | <0.001 | 2.8 | 0.078 |
| Cancer | 22.4 | 0.001 | 14.0 | 0.020 | 9.8 | 0.816 | 13.0 | 0.022 |
| Dementia | 1.7 | 0.111 | 6.4 | 0.015 | 12.7 | <0.001 | 8.9 | <0.001 |
| Acute medical conditions | ||||||||
| Uncontrolled blood pressure | 10.3 | 0.005 | 9.6 | <0.001 | 13.8 | <0.001 | 11.8 | <0.001 |
| Acute coronary syndromes | 4.3 | 0.484 | 3.8 | 0.523 | 3.6 | 0.584 | 3.7 | 0.676 |
| Acute pulmonary embolism | 0.9 | 0.598 | 0.9 | 0.742 | 1.6 | 0.463 | 1.2 | 0.303 |
| New onset atrial fibrillation | 6.9 | <0.001 | 11.4 | <0.001 | 16.0 | <0.001 | 13.1 | <0.001 |
| Syncope | 5.2 | 0.749 | 3.8 | 0.742 | 3.3 | 0.217 | 3.7 | 0.353 |
| Stroke | 1.7 | 0.703 | 2.0 | 0.485 | 4.0 | 0.703 | 3.0 | 0.821 |
| Fever/febrile episodes | 7.8 | 0.274 | 5.8 | 0.469 | 5.6 | 0.822 | 5.9 | 0.314 |
| Infections | 31.9 | 0.001 | 34.5 | <0.001 | 36.4 | 0.001 | 35.1 | <0.001 |
| Worsening of renal function | 19.0 | <0.001 | 13.2 | <0.001 | 12.0 | <0.001 | 13.3 | <0.001 |
| Metabolic/Electrolyte disturbances | 1.7 | 1.000 | 0.9 | 0.057 | 5.1 | 0.209 | 3.1 | 0.811 |
| Anemia | 3.4 | 0.517 | 2.6 | 0.019 | 3.1 | 0.034 | 3.0 | 0.001 |
| 65–74 Years | 75–84 Years | ≥85 Years | All | |||||
|---|---|---|---|---|---|---|---|---|
| Variable | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p |
| Age | 1.08 (1.07–1.09) | <0.001 | ||||||
| NYHA class II | Ref. | Ref. | Ref. | Ref. | ||||
| NYHA class III | 1.64 (1.20–2.24) | 0.002 | 1.64 (1.20–2.24) | 0.002 | 2.11 (1.51–2.93) | <0.001 | 1.80 (1.46–2.21) | <0.001 |
| NYHA class IV | 2.44 (1.67–3.56) | <0.001 | 2.43 (1.67–3.56) | <0.001 | 3.09 (2.12–4.50) | <0.001 | 2.73 (2.14–3.49) | <0.001 |
| Coronary artery disease | 1.42 (1.13–1.78) | 0.002 | 1.42 (1.14–1.77) | 0.002 | 1.38 (1.19–1.58) | <0.001 | ||
| Hypertension | 1.38 (1.20–1.59) | <0.001 | ||||||
| Valve disease | 1.18 (0.93–1.51) | 0.173 | 1.28 (1.09–1.49) | 0.002 | ||||
| Cerebrovascular disease | 1.30 (0.94–1.80) | 0.120 | 1.53 (1.14–2.04] | 0.004 | 1.42 (1.15–1.75) | 0.001 | ||
| Diabetes | 1.13 (0.91–1.42) | 0.274 | 1.13 (0.91–1.42) | 0.274 | 1.44 (0.82–1.94) | 0.453 | 1.55 (1.34–1.79) | <0.001 |
| Cancer | 1.48 (1.09–2.03) | 0.013 | 1.48 (1.09–2.03) | 0.013 | … | … | … | … |
| Dementia | ... | ... | 1.74 (1.12–2.71) | 0.014 | 1.74 (1.43–2.12) | <0.001 | 1.59 (1.25–2.02) | <0.001 |
| Infections | 1.74 (1.10–2.71) | 0.014 | 1.83 (1.34–2.49) | 0.001 | 1.74 (1.24–2.19) | 0.001 | 1.97 (1.61–2.41) | 0.001 |
| New onset atrial fibrillation | 0.61 (0.44–0.86) | 0.005 | 0.61 (0.43–0.86) | 0.005 | 0.68 (0.53–0.88) | 0.003 | 0.76 (0.59–0.86) | 0.002 |
| Uncontrolled blood pressure | 0.49 (0.26–0.88) | 0.018 | 0.44 (0.31–0.64) | <0.001 | 0.58 (0.43–0.74) | <0.001 | 0.50 (0.41–0.62) | <0.001 |
| Worsening renal function | 2.11 (1.53–2.92) | <0.001 | 2.11 (1.53–2.92) | <0.001 | 1.92 (1.44–2.56) | <0.001 | 2.21 (1.82–2.69) | <0.001 |
| Anemia | 0.46 (0.24–0.90) | 0.023 | 0.59 (0.34–1.02) | 0.051 | 0.63 (0.43–0.93) | 0.019 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Matteis, G.; Covino, M.; Burzo, M.L.; Della Polla, D.A.; Franceschi, F.; Mebazaa, A.; Gambassi, G. Clinical Characteristics and Predictors of In-Hospital Mortality among Older Patients with Acute Heart Failure. J. Clin. Med. 2022, 11, 439. https://doi.org/10.3390/jcm11020439
De Matteis G, Covino M, Burzo ML, Della Polla DA, Franceschi F, Mebazaa A, Gambassi G. Clinical Characteristics and Predictors of In-Hospital Mortality among Older Patients with Acute Heart Failure. Journal of Clinical Medicine. 2022; 11(2):439. https://doi.org/10.3390/jcm11020439
Chicago/Turabian StyleDe Matteis, Giuseppe, Marcello Covino, Maria Livia Burzo, Davide Antonio Della Polla, Francesco Franceschi, Alexandre Mebazaa, and Giovanni Gambassi. 2022. "Clinical Characteristics and Predictors of In-Hospital Mortality among Older Patients with Acute Heart Failure" Journal of Clinical Medicine 11, no. 2: 439. https://doi.org/10.3390/jcm11020439
APA StyleDe Matteis, G., Covino, M., Burzo, M. L., Della Polla, D. A., Franceschi, F., Mebazaa, A., & Gambassi, G. (2022). Clinical Characteristics and Predictors of In-Hospital Mortality among Older Patients with Acute Heart Failure. Journal of Clinical Medicine, 11(2), 439. https://doi.org/10.3390/jcm11020439