
Factors Influencing the Improvement of Activities of Daily Living during Inpatient Rehabilitation in Newly Diagnosed Patients with Glioblastoma Multiforme

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
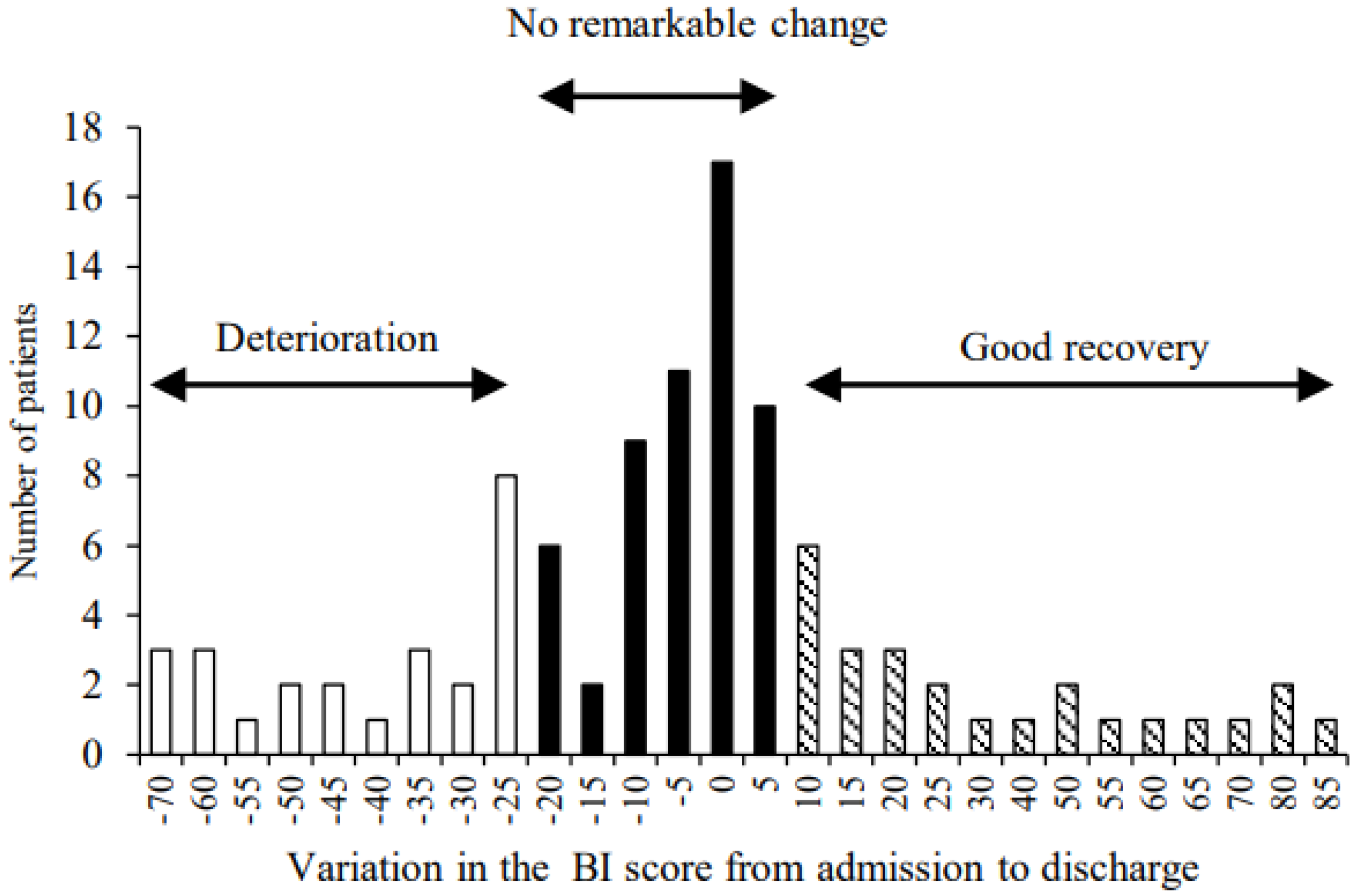
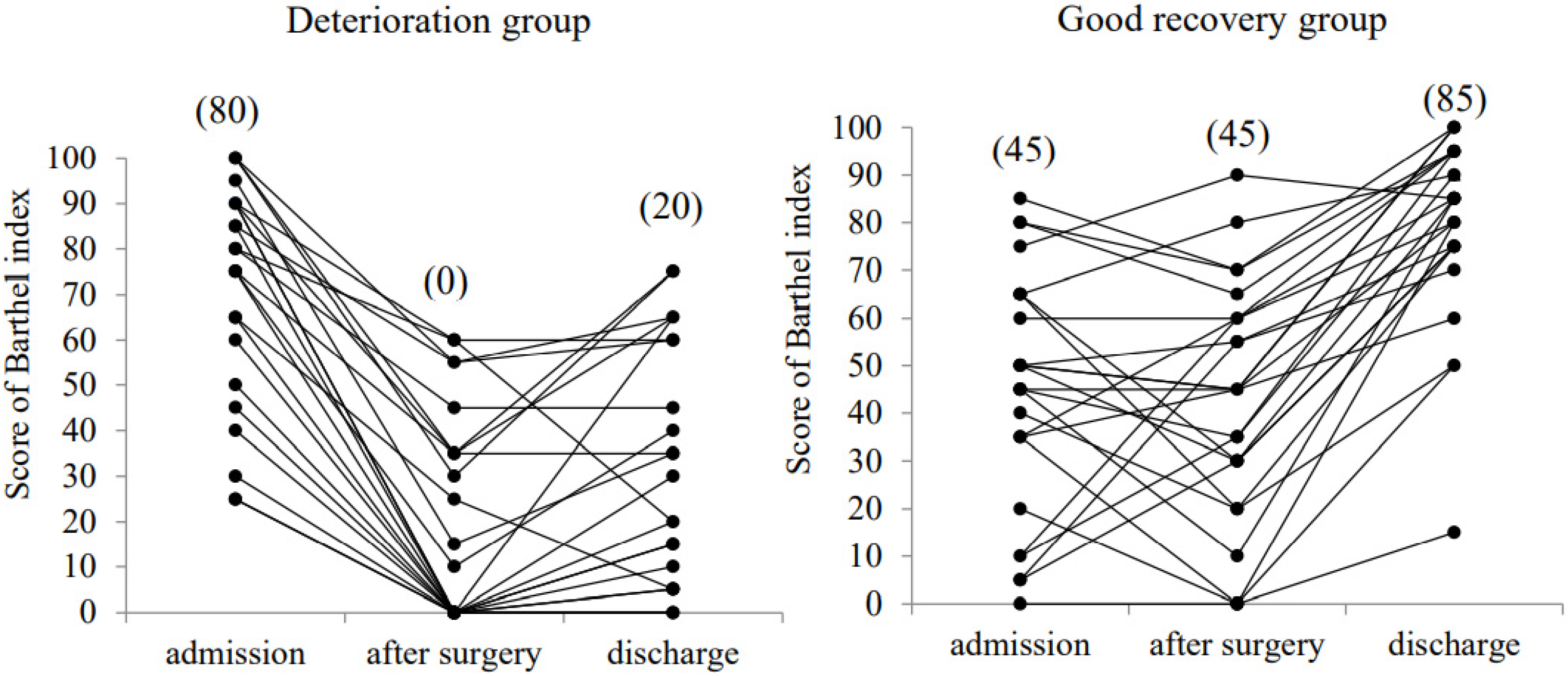
2.2. Patients Classification
2.3. Outcome Measures
2.4. Radio and Chemotherapy and Inpatient Rehabilitation
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Change of ADL Level between Deterioration and Good Recovery Groups
3.3. Comparison of the Deterioration and Good Recovery Groups in the Pre-Operative, Intra-Operative, Post-Operative, and Rehabilitation-Related Factors
3.4. Improvement of ADL Level and Overall Survival
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wrensch, M.; Minn, Y.; Chew, T.; Bondy, M.; Berger, M.S. Epidemiology of primary brain tumors: Current concepts and review of the literature. Neuro-Oncology 2002, 4, 278–299. [Google Scholar] [CrossRef]
- Crocetti, E.; Trama, A.; Stiller, C.; Caldarella, A.; Soffietti, R.; Jaal, J.; Weber, D.C.; Ricardi, U.; Slowinski, J.; Brandes, A. RARECARE working group. Epidemiology of glial and non-glial brain tumours in Europe. Eur. J. Cancer 2012, 48, 1532–1542. [Google Scholar] [CrossRef] [PubMed]
- Wann, A.; Tully, P.A.; Barnes, E.H.; Lwin, Z.; Jeffree, R.; Drummond, K.J.; Gan, H.; Khasraw, M. Outcomes after second surgery for recurrent glioblastoma: A retrospective case-control study. J. Neurooncol. 2018, 137, 409–415. [Google Scholar] [CrossRef]
- Liu, Z.Y.; Feng, S.S.; Zhang, Y.H.; Zhang, L.Y.; Xu, S.C.; Li, J.; Cao, H.; Huang, J.; Fan, F.; Cheng, L.; et al. Competing risk model to determine the prognostic factors and treatment strategies for elderly patients with glioblastoma. Sci. Rep. 2021, 1, 9321. [Google Scholar] [CrossRef]
- Montemurro, N.; Fanelli, G.N.; Scatena, C.; Ortenzi, V.; Pasqualetti, F.; Mazzanti, C.M.; Morganti, R.; Paiar, F.; Naccarato, A.G.; Perrini, P. Surgical outcome and molecular pattern characterization of recurrent glioblastoma multiforme: A single-center retrospective series. Clin. Neurol. Neurosurg. 2021, 207, 106735. [Google Scholar] [CrossRef]
- Bartolo, M.; Zucchella, C.; Pace, A.; Lanzetta, G.; Vecchione, C.; Bartolo, M.; Grillea, G.; Serrao, M.; Tassorelli, C.; Sandrini, G.; et al. Early rehabilitation after surgery improves functional outcome in inpatients with brain tumours. J. Neurooncol. 2012, 107, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Tang, V.; Rathbone, M.; Dorsay, J.P.; Jiang, S.; Harvey, D. Rehabilitation in primary and metastatic brain tumours: Impact of functional outcomes on survival. J. Neurol. 2008, 255, 820–827. [Google Scholar] [CrossRef] [PubMed]
- Dutta, D.; Vanere, P.; Gupta, T.; Munshi, A.; Jalali, R. Factors influencing activities of daily living using FIM-FAM scoring system before starting adjuvant treatment in patients with brain tumors: Results from a prospective study. J. Neurooncol. 2009, 94, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Amatya, B.; Drummond, K.; Galea, M. Effectiveness of integrated multidisciplinary rehabilitation in primary brain cancer survivors in an Australian community cohort: A controlled clinical trial. J. Rehabil. Med. 2014, 46, 754–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stark, A.M.; van de Bergh, J.; Hedderich, J.; Mehdorn, H.M.; Nabavi, A. Glioblastoma: Clinical characteristics, prognostic factors and survival in 492 patients. Clin. Neurol. Neurosurg. 2012, 114, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Fekete, B.; Werlenius, K.; Örndal, C.; Rydenhag, B. Prognostic factors for glioblastoma patients—A clinical population-based study. Acta Neurol. Scand. 2016, 133, 434–441. [Google Scholar] [CrossRef]
- Huang, M.E.; Wartella, J.E.; Kreutzer, J.S. Functional outcomes and quality of life in patients with brain tumors: A preliminary report. Arch. Phys. Med. Rehabil. 2001, 82, 1540–1546. [Google Scholar] [CrossRef]
- Pérez-Larraya, J.G.; Ducray, F. Treating glioblastoma patients with poor performance status: Where do we go from here? CNS Oncol. 2014, 3, 231–241. [Google Scholar] [CrossRef]
- Yates, J.W.; Chalmer, B.; McKegney, F.P. Evaluation of patients with advanced cancer using the Karnofsky performance status. Cancer 1980, 45, 2220–2224. [Google Scholar] [CrossRef]
- Chang, S.M.; Parney, I.F.; McDermott, M.; Barker, F.G., 2nd; Schmidt, M.H.; Huang, W.; Laws, E.R., Jr.; Lillehei, K.O.; Bernstein, M.; Brem, H.; et al. Glioma Outcomes Investigators. Perioperative complications and neurological outcomes of first and second craniotomies among patients enrolled in the Glioma Outcome Project. J. Neurosurg. 2003, 98, 1175–1181. [Google Scholar] [CrossRef] [Green Version]
- Roberts, P.S.; Nuño, M.; Sherman, D.; Asher, A.; Wertheimer, J.; Riggs, R.V.; Patil, C.G. The impact of inpatient rehabilitation on function and survival of newly diagnosed patients with glioblastoma. PM&R 2014, 6, 514–521. [Google Scholar]
- Brazil, L.; Thomas, R.; Laing, R.; Hines, F.; Guerrero, D.; Ashley, S.; Brada, M. Verbally administered Barthel Index as functional assessment in brain tumour patients. J. Neurooncol. 1997, 34, 187–192. [Google Scholar] [CrossRef]
- Marciniak, C.M.; Sliwa, J.A.; Heinemann, A.W.; Semik, P.E. Functional outcomes of persons with brain tumors after inpatient rehabilitation. Arch. Phys. Med. Rehabil. 2001, 82, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.B.; Parsons, H.A.; Shin, K.Y.; Guo, Y.; Konzen, B.S.; Yadav, R.R.; Smith, D.W. Comparison of functional outcomes in low- and high-grade astrocytoma rehabilitation inpatients. Am. J. Phys. Med. Rehabil. 2010, 89, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.; Søgaard, K.; Minet, L.R. Development of an exercise intervention as part of rehabilitation in a glioblastoma multiforme survivor during irradiation treatment: A case report. Disabil. Rehabil. 2019, 41, 1608–1614. [Google Scholar] [CrossRef] [Green Version]
- Cormie, P.; Nowak, A.K.; Chambers, S.K.; Galvão, D.A.; Newton, R.U. The potential role of exercise in neuro-oncology. Front. Oncol. 2015, 5, 85. [Google Scholar] [CrossRef] [Green Version]
- Olkowski, B.F.; Shah, S.O. Early Mobilization in the Neuro-ICU: How Far Can We Go? Neurocrit. Care. 2017, 27, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Tipping, C.J.; Harrold, M.; Holland, A.; Romero, L.; Nisbet, T.; Hodgson, C.L. The effects of active mobilisation and rehabilitation in ICU on mortality and function: A systematic review. Intensive Care Med. 2017, 43, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–1559. [Google Scholar] [CrossRef]
- Mercier, L.; Audet, T.; Hébert, R.; Rochette, A.; Dubois, M.F. Impact of motor, cognitive, and perceptual disorders on ability to perform activities of daily living after stroke. Stroke 2001, 32, 2602–2608. [Google Scholar] [CrossRef] [Green Version]
- Aprile, I.; Chiesa, S.; Padua, L.; Di Blasi, C.; Arezzo, M.F.; Valentini, V.; Di Stasio, E.; Balducci, M. Occurrence and predictors of the fatigue in high-grade glioma patients. Neurol. Sci. 2015, 36, 1363–1369. [Google Scholar] [CrossRef]
- Given, C.W.; Given, B.; Azzouz, F.; Kozachik, S.; Stommel, M. Predictors of pain and fatigue in the year following diagnosis among elderly cancer patients. J. Pain Symptom Manag. 2001, 21, 456–466. [Google Scholar] [CrossRef]
- Schwartz, A.L.; Nail, L.M.; Chen, S.; Meek, P.; Barsevick, A.M.; King, M.E.; Jones, L.S. Fatigue patterns observed in patients receiving chemotherapy and radiotherapy. Cancer Investig. 2000, 18, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Park, J.K.; Hodges, T.; Arko, L.; Shen, M.; Dello Iacono, D.; McNabb, A.; Bailey, N.O.; Kreisl, T.N.; Iwamoto, F.M.; Sul, J.; et al. Scale to predict survival after surgery for recurrent glioblastoma multiforme. J. Clin. Oncol. 2010, 28, 3838–3843. [Google Scholar] [CrossRef]
- Neuloh, G.; Pechstein, U.; Schramm, J. Motor tract monitoring during insular glioma surgery. J. Neurosurg. 2007, 106, 582–592. [Google Scholar] [CrossRef]
- Li, C.; Wang, H.; Liu, N.; Jia, M.; Zhang, H.; Xi, X.; Hou, X.; Beijing Acute Kidney Injury Trial (BAKIT) Workgroup. Early negative fluid balance is associated with lower mortality after cardiovascular surgery. Perfusion 2018, 33, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. European Organisation for Research and Treatment of Cancer Brain Tumor and Radiotherapy Groups; National Cancer Institute of Canada Clinical Trials Group. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- De Souza, R.M.; Shaweis, H.; Han, C.; Sivasubramaniam, V.; Brazil, L.; Beaney, R.; Sadler, G.; Al-Sarraj, S.; Hampton, T.; Logan, J.; et al. Has the survival of patients with glioblastoma changed over the years? Br. J. Cancer 2016, 114, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Scrutinio, D.; Monitillo, V.; Guida, P.; Nardulli, R.; Multari, V.; Monitillo, F.; Calabrese, G.; Fiore, P. Functional Gain after Inpatient Stroke Rehabilitation: Correlates and Impact on Long-Term Survival. Stroke 2015, 46, 2976–2980. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Overall (n = 105) | Deterioration Group (n = 25) | No Remarkable Change Group (n = 55) | Good Recovery Group (n = 25) | p Value | |
|---|---|---|---|---|---|
| Age (years) | 67.0 ± 14.1 | 71.0 ± 12.2 | 66.7 ± 11.5 | 64.6 ± 11.5 | 0.24 |
| Men/Women (n) | 59/46 | 11/14 | 31/24 | 16/9 | 0.34 |
| KPS at admission (median) | 57.9 ± 15.7 (60) | 61.2 ± 10.9 (60) | 59.6 ± 18.6 (60) | 50.4 ± 8.4 (50) | 0.01 |
| Extent of resection (n) | 0.14 | ||||
| Gross and near total resection | 65 | 14 | 30 | 21 | |
| Partial resection | 23 | 6 | 15 | 2 | |
| Biopsy | 17 | 5 | 10 | 2 | |
| Treatments (n) | 0.10 | ||||
| Surgery only | 5 | 1 | 4 | 0 | |
| Surgery + RT or TMZ or Bev | 10 | 4 | 6 | 0 | |
| Surgery + RT concomitant TMZ | 70 | 15 | 33 | 22 | |
| Surgery + RT concomitant TMZ + Bev | 20 | 5 | 12 | 3 | |
| Tumor location (n) † | |||||
| Frontal | 35 | 10 | 19 | 6 | 0.49 |
| Parietal | 23 | 7 | 8 | 8 | 0.15 |
| Temporal | 42 | 9 | 22 | 11 | 0.85 |
| Occipital | 7 | 3 | 3 | 1 | 0.46 |
| Others | 17 | 5 | 8 | 4 | 0.83 |
| Tumor hemisphere (n) | 0.16 | ||||
| Right | 45 | 11 | 24 | 10 | |
| Left | 49 | 9 | 25 | 15 | |
| Bilateral | 11 | 5 | 6 | 0 | |
| Tumor size (mm) | 44.5 ± 13.8 | 48.0 ± 14.0 | 42.6 ± 13.1 | 50.0 ± 9.8 | 0.14 |
| Lengths of hospital stay (days) | 60.3 ± 16.4 | 59.2 ± 16.8 | 62.3 ± 18.7 | 57.0 ± 8.8 | 0.40 |
| Deterioration Group | Good Recovery Group | p Value | Effect Size | |
|---|---|---|---|---|
| Preoperative factors | ||||
| Length from initial symptoms to surgery (days) | 67.3 ± 45.8 | 37.8 ± 19.9 | 0.01 | 0.83 |
| Initial Symptoms (n) † | ||||
| Motor paralysis and muscle weakness | 5 | 13 | 0.03 | 0.34 |
| Cognitive dysfunction | 14 | 10 | 0.25 | 0.23 |
| Headache | 3 | 3 | 1.00 | 0.19 |
| Visual field defect | 3 | 1 | 0.60 | 0.00 |
| Dysphagia | 0 | 1 | 1.00 | 0.14 |
| Fatigue | 0 | 1 | 1.00 | 0.14 |
| Intraoperative factors | ||||
| Surgery time (minutes) | 555.0 ± 133.9 | 526.9 ± 127.7 | 0.47 | 0.22 |
| Bleeding volume (mL) | 692.0 ± 588.3 | 644.3 ± 529.3 | 0.78 | 0.09 |
| Transfusion volume (mL) | 117.9 ± 234.5 | 73.0 ± 210.5 | 0.51 | 0.20 |
| Infusion volume (mL) | 4086.0 ± 1144.5 | 4096.0 ±1108.5 | 0.98 | 0.01 |
| Fluid balance (mL) | 1317.0 ± 771.3 | 796.3 ± 929.9 | 0.05 | 0.60 |
| Postoperative factors # | ||||
| Fever (n) | 6 | 4 | 0.73 | 0.10 |
| Infection (n) | 4 | 2 | 0.67 | 0.12 |
| Pneumonia (n) | 1 | 0 | 1.00 | 0.14 |
| Cerebral hemorrhage (n) | 9 | 4 | 0.20 | 0.23 |
| Ischemic stroke (n) | 5 | 1 | 0.10 | 0.24 |
| Motor paralysis (decreases BRS 2 stage or more) (n) | 9 | 1 | <0.01 | 0.43 |
| Length from surgery to chemoradiotherapy (days) | 19.1 ± 8.8 | 17.0 ± 4.3 | 0.28 | 0.30 |
| RT and TMZ tolerance (n) | ||||
| RT interruption or discontinuation | 3 | 1 | 0.11 | 0.29 |
| TMZ interruption or discontinuation | 8 | 3 | 0.14 | 0.28 |
| Deterioration Group | Good Recovery Group | p Value | Effect Size | |
|---|---|---|---|---|
| Length up to rehabilitation onset (days) | 2.6 ± 1.5 | 3.4 ± 2.3 | 0.17 | 0.39 |
| Length up to sitting training onset (days) | 4.8 ± 2.9 | 5.6 ± 5.1 | 0.54 | 0.19 |
| Length up to walking training onset (days) | 13.2 ± 16.7 | 8.4 ± 7.9 | 0.20 | 0.37 |
| Motor paralysis of (median of BRS) | ||||
| admission | 4.9 ± 1.2 (5) | 4.4 ± 1.4 (5) | 0.26 | 0.20 |
| after surgery | 3.7 ± 1.4 (4) | 4.3 ± 1.3 (5) | 0.19 | 0.22 |
| discharge | 4.0 ± 1.4 (4) | 5.5 ± 0.9 (6) | <0.01 | 0.55 |
| No motor paralysis (n) | ||||
| admission | 6 | 9 | 0.53 | 0.11 |
| after surgery | 2 | 9 | 0.04 | 0.32 |
| discharge | 2 | 10 | 0.02 | 0.36 |
| Change from admission to discharge (n) | ||||
| Deterioration of motor paralysis | 13 | 1 | <0.01 | 0.57 |
| Sever cognitive disorder or depression | 10 | 0 | <0.01 | 0.50 |
| Deterioration Group | Good Recovery Group | p Value | Effect Size | |||||
|---|---|---|---|---|---|---|---|---|
| Grade 0 | Grade 1–2 | Grade 3–4 | Grade 0 | Grade 1–2 | Grade 3–4 | |||
| Hematologic toxicity n (%) † | ||||||||
| Leukopenia | 10 (45) | 9 (41) | 3 (14) | 15 (60) | 9 (36) | 1 (4) | 0.26 | 0.29 |
| Neutropenia | 18 (78) | 2 (9) | 3 (13) | 16 (67) | 4 (17) | 4 (17) | 0.91 | 0.14 |
| Lymphocytopenia | 4 (17) | 11 (48) | 8 (35) | 7 (29) | 14 (58) | 3 (13) | 0.26 | 0.33 |
| Thrombocytopenia | 3 (13) | 20 (87) | 0 (0) | 5 (20) | 20 (80) | 0 (0) | 0.48 | 0.17 |
| Anemia | 3 (13) | 21 (87) | 0 (0) | 4 (16) | 19 (76) | 2 (8) | 0.18 | 0.35 |
| Non-hematologic toxicity n (%) | ||||||||
| Constipation | 9 (39) | 14 (61) | 0 (0) | 14 (56) | 10 (40) | 1 (4) | 0.36 | 0.26 |
| Fatigue | 6 (30) | 14 (70) | 0 (0) | 20 (80) | 5 (20) | 0 (0) | <0.01 | 0.50 |
| Fever | 11 (46) | 13 (54) | 0 (0) | 22 (88) | 3 (12) | 0 (0) | <0.01 | 0.45 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Natsume, K.; Sakakima, H.; Kawamura, K.; Yoshida, A.; Akihiro, S.; Yonezawa, H.; Yoshimoto, K.; Shimodozono, M. Factors Influencing the Improvement of Activities of Daily Living during Inpatient Rehabilitation in Newly Diagnosed Patients with Glioblastoma Multiforme. J. Clin. Med. 2022, 11, 417. https://doi.org/10.3390/jcm11020417
Natsume K, Sakakima H, Kawamura K, Yoshida A, Akihiro S, Yonezawa H, Yoshimoto K, Shimodozono M. Factors Influencing the Improvement of Activities of Daily Living during Inpatient Rehabilitation in Newly Diagnosed Patients with Glioblastoma Multiforme. Journal of Clinical Medicine. 2022; 11(2):417. https://doi.org/10.3390/jcm11020417
Chicago/Turabian StyleNatsume, Keisuke, Harutoshi Sakakima, Kentaro Kawamura, Akira Yoshida, Shintaro Akihiro, Hajime Yonezawa, Koji Yoshimoto, and Megumi Shimodozono. 2022. "Factors Influencing the Improvement of Activities of Daily Living during Inpatient Rehabilitation in Newly Diagnosed Patients with Glioblastoma Multiforme" Journal of Clinical Medicine 11, no. 2: 417. https://doi.org/10.3390/jcm11020417
APA StyleNatsume, K., Sakakima, H., Kawamura, K., Yoshida, A., Akihiro, S., Yonezawa, H., Yoshimoto, K., & Shimodozono, M. (2022). Factors Influencing the Improvement of Activities of Daily Living during Inpatient Rehabilitation in Newly Diagnosed Patients with Glioblastoma Multiforme. Journal of Clinical Medicine, 11(2), 417. https://doi.org/10.3390/jcm11020417