
Psychological Flexibility Mediates Wellbeing for People with Adverse Childhood Experiences during COVID-19

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Depression, Anxiety, and Stress
2.2.2. Mental Wellbeing
2.2.3. Illness Perception
2.2.4. COVID-19 Specific Stress
2.2.5. Adverse Childhood Experiences
2.2.6. Psychological Flexibility
2.3. Statistical Analyses
2.4. Role of Funding Sources
3. Results
3.1. Changes within Each Group
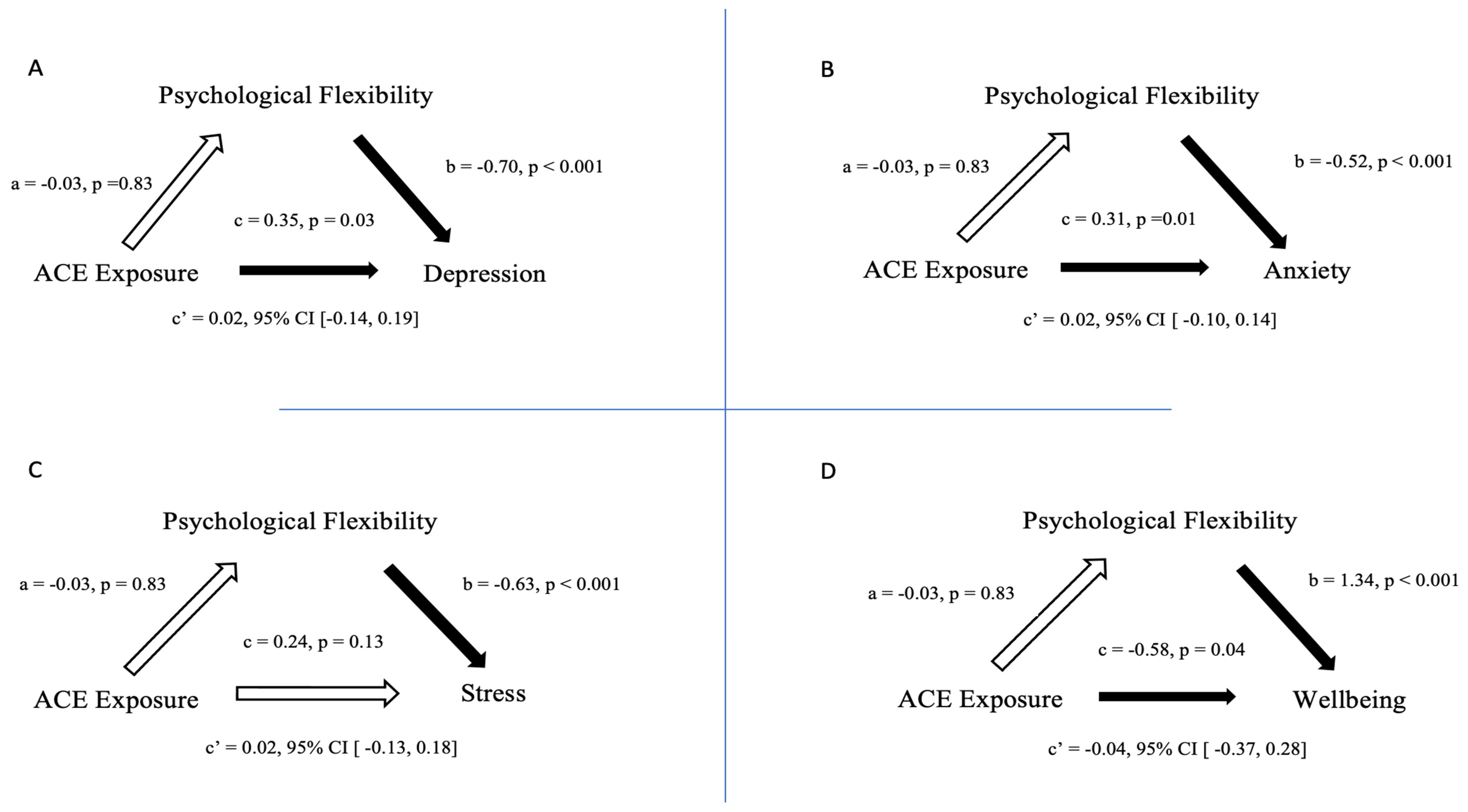
3.2. Mediational Analysis
4. Discussion
4.1. Longitudinal Change between and within Those with ACE and Those without ACE in Their Mental Health and Wellbeing
4.2. ACE-Distress Relationship, ACE-Wellbeing Relationship and Psychological Flexibility-Mediational Analyses
4.3. Limitations
4.4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Jeong, H.; Yim, H.W.; Song, Y.-J.; Ki, M.; Min, J.-A.; Cho, J.; Chae, J.-H. Mental health status of people isolated due to Middle East Respiratory Syndrome. Epidemiol. Health 2016, 38, e2016048. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Gavin, B.; Lyne, J.; Mcnicholas, F. Mental health and the COVID-19 pandemic. Ir. J. Psychol. Med. 2020, 37, 156–158. [Google Scholar] [CrossRef] [PubMed]
- Kelly, B.D. Plagues, pandemics and epidemics in Irish history prior to COVID-19 (coronavirus): What can we learn? Ir. J. Psychol. Med. 2020, 37, 269–274. [Google Scholar] [CrossRef] [Green Version]
- Lam, M.H.; Wing, Y.K.; Yu, M.W.; Leung, C.M.; Ma, R.C.; Kong, A.P.; So, W.Y.; Fong, S.Y.; Lam, S.P. Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors. Arch. Intern. Med. 2009, 169, 2142–2147. [Google Scholar] [CrossRef] [Green Version]
- Mak, I.W.C.; Chu, C.M.; Pan, P.C.; Yiu, M.G.C.; Chan, V.L. Long-term psychiatric morbidities among SARS survivors. Gen. Hosp. Psychiatry 2009, 31, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Burke, T.; Berry, A.; Taylor, L.K.; Stafford, O.; Murphy, E.; Shevlin, M.; McHugh, L.; Carr, A. Increased Psychological Distress during COVID-19 and Quarantine in Ireland: A National Survey. J. Clin. Med. 2020, 9, 3481. [Google Scholar] [CrossRef] [PubMed]
- Flynn, R.; Riches, E.; Reid, G.; Rosenberg, S.; Niedzwiedz, C. Rapid review of the impact of COVID-19 on mental health. Public Healh Scotl. 2020, 20, 1–133. [Google Scholar]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Holt-Lunstad, J.; Smith, T.B.; Baker, M.; Harris, T.; Stephenson, D. Loneliness and Social Isolation as Risk Factors for Mortality: A Meta-Analytic Review. Perspect. Psychol. Sci. 2015, 10, 227–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karatzias, T.; Shevlin, M.; Murphy, J.; McBride, O.; Ben-Ezra, M.; Bentall, R.P.; Vallières, F.; Hyland, P. Posttraumatic Stress Symptoms and Associated Comorbidity During the COVID-19 Pandemic in Ireland: A Population-Based Study. J. Trauma. Stress 2020, 33, 365–370. [Google Scholar] [CrossRef]
- McCracken, L.M.; Badinlou, F.; Buhrman, M.; Brocki, K.C. The role of psychological flexibility in the context of COVID-19: Associations with depression, anxiety, and insomnia. J. Context. Behav. Sci. 2020, 19, 28–35. [Google Scholar] [CrossRef]
- Nearchou, F.; Flinn, C.; Niland, R.; Subramaniam, S.S.; Hennessy, E. Exploring the Impact of COVID-19 on Mental Health Outcomes in Children and Adolescents: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 8479. [Google Scholar] [CrossRef]
- Smith, L.; Jacob, L.; Yakkundi, A.; McDermott, D.; Armstrong, N.C.; Barnett, Y.; López-Sánchez, G.F.; Martin, S.; Butler, L.; Tully, M.A. Correlates of symptoms of anxiety and depression and mental wellbeing associated with COVID-19: A cross-sectional study of UK-based respondents. Psychiatry Res. 2020, 291, 113138. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef]
- Hyland, P.; Shevlin, M.; McBride, O.; Murphy, J.; Karatzias, T.; Bentall, R.P.; Martinez, A.; Vallières, F. Anxiety and depression in the Republic of Ireland during the COVID-19 pandemic. Acta Psychiatr. Scand. 2020, 142, 249–256. [Google Scholar] [CrossRef]
- Kroska, E.B.; Roche, A.I.; Adamowicz, J.L.; Stegall, M.S. Psychological flexibility in the context of COVID-19 adversity: Associations with distress. J. Context. Behav. Sci. 2020, 18, 28–33. [Google Scholar] [CrossRef]
- Liu, X.; Kakade, M.; Fuller, C.J.; Fan, B.; Fang, Y.; Kong, J.; Guan, Z.; Wu, P. Depression after exposure to stressful events: Lessons learned from the severe acute respiratory syndrome epidemic. Compr. Psychiatry 2012, 53, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Zhong, W.; Bian, Z.; Li, Z.; Zhang, K.; Liang, B.; Zhong, Y.; Hu, M.; Lin, L.; Liu, J.; et al. A comparison of mortality-related risk factors of COVID-19, SARS, and MERS: A systematic review and meta-analysis. J. Infect. 2020, 81, e18–e25. [Google Scholar] [CrossRef]
- O’Connor, K.; Wrigley, M.; Jennings, R.; Hill, M.; Niazi, A. Mental health impacts of COVID-19 in Ireland and the need for a secondary care mental health service response. Ir. J. Psychol. Med. 2020, 38, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Stafford, O.; Berry, A.; Taylor, L.K.; Wearen, S.; Prendergast, C.; Murphy, E.; Shevlin, M.; McHugh, L.; Carr, A.; Burke, T. Comorbidity and COVID-19: Investigating the relationship between medical and psychological well-being. Ir. J. Psychol. Med. 2021, 38, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Hammen, C.; Henry, R.; Daley, S.E. Depression and sensitization to stressors among young women as a function of childhood adversity. J. Consult. Clin. Psychol. 2000, 68, 782–787. [Google Scholar] [CrossRef]
- Sonu, S.; Marvin, D.; Moore, C. The Intersection and Dynamics between COVID-19, Health Disparities, and Adverse Childhood Experiences: “Intersection/Dynamics between COVID-19, Health Disparities, and ACEs”. J. Child Adolesc. Trauma 2021, 14, 517–526. [Google Scholar] [CrossRef]
- Seitz, K.I.; Bertsch, K.; Herpertz, S.C. A Prospective Study of Mental Health During the COVID-19 Pandemic in Childhood Trauma–Exposed Individuals: Social Support Matters. J. Trauma. Stress 2021, 34, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.W.; Nyengerai, T.; Mendenhall, E. Evaluating the mental health impacts of the COVID-19 pandemic: Perceived risk of COVID-19 infection and childhood trauma predict adult depressive symptoms in urban South Africa. Psychol. Med. 2020, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Bellis, M.A.; Lowey, H.; Leckenby, N.; Hughes, K.; Harrison, D. Adverse childhood experiences: Retrospective study to determine their impact on adult health behaviours and health outcomes in a UK population. J. Public Health 2013, 36, 81–91. [Google Scholar] [CrossRef] [Green Version]
- Hughes, K.; Bellis, M.A.; Hardcastle, K.A.; Sethi, D.; Butchart, A.; Mikton, C.; Jones, L.; Dunne, M.P. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. Lancet Public Health 2017, 2, e356–e366. [Google Scholar] [CrossRef] [Green Version]
- Nelson, C.A.; Scott, R.D.; Bhutta, Z.A.; Harris, N.B.; Danese, A.; Samara, M. Adversity in childhood is linked to mental and physical health throughout life. BMJ 2020, 371, m3048. [Google Scholar] [CrossRef]
- Chi, X.; Becker, B.; Yu, Q.; Willeit, P.; Jiao, C.; Huang, L.; Hossain, M.M.; Grabovac, I.; Yeung, A.; Lin, J.; et al. Prevalence and Psychosocial Correlates of Mental Health Outcomes Among Chinese College Students During the Coronavirus Disease (COVID-19) Pandemic. Front. Psychiatry 2020, 11, 803. [Google Scholar] [CrossRef]
- Doom, J.R.; Seok, D.; Narayan, A.J.; Fox, K.R. Adverse and Benevolent Childhood Experiences Predict Mental Health During the COVID-19 Pandemic. Advers. Resil. Sci. 2021, 2, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Haydon, K.C.; Salvatore, J.E. A Prospective Study of Mental Health, Well-Being, and Substance Use During the Initial COVID-19 Pandemic Surge. Clin. Psychol. Sci. 2021, 21677026211013499. [Google Scholar] [CrossRef]
- Lahav, Y. Psychological distress related to COVID-19—The contribution of continuous traumatic stress. J. Affect. Disord. 2020, 277, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Sahle, B.W.; Ofori-Asenso, R.; Renzaho, A.M.N. Adverse Childhood Experiences Should Be Priority in Global Response to Covid-19. J. Paediatr. Child Health 2020, 56, 1656–1657. [Google Scholar] [CrossRef] [PubMed]
- Sonu, S.; Post, S.; Feinglass, J. Adverse childhood experiences and the onset of chronic disease in young adulthood. Prev. Med. 2019, 123, 163–170. [Google Scholar] [CrossRef]
- Tsur, N.; Abu-Raiya, H. COVID-19-related fear and stress among individuals who experienced child abuse: The mediating effect of complex posttraumatic stress disorder. Child Abus. Negl. 2020, 110, 104694. [Google Scholar] [CrossRef] [PubMed]
- Wade, M.; Prime, H.; Johnson, D.; May, S.S.; Jenkins, J.M.; Browne, D.T. The disparate impact of COVID-19 on the mental health of female and male caregivers. Soc. Sci. Med. 2021, 275, 113801. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, L.K.; Breiding, M.J.; Merrick, M.T.; Thompson, W.W.; Ford, D.C.; Dhingra, S.S.; Parks, S.E. Childhood adversity and adult chronic disease: An update from ten states and the District of Columbia, 2010. Am. J. Prev. Med. 2015, 48, 345–349. [Google Scholar] [CrossRef]
- Merrick, M.T.; Ports, K.A.; Ford, D.C.; Afifi, T.O.; Gershoff, E.T.; Grogan-Kaylor, A. Unpacking the impact of adverse childhood experiences on adult mental health. Child Abus. Negl. 2017, 69, 10–19. [Google Scholar] [CrossRef]
- Ports, K.A.; Holman, D.M.; Guinn, A.S.; Pampati, S.; Dyer, K.E.; Merrick, M.T.; Lunsford, N.B.; Metzler, M. Adverse Childhood Experiences and the Presence of Cancer Risk Factors in Adulthood: A Scoping Review of the Literature From 2005 to 2015. J. Pediatr. Nurs. 2019, 44, 81–96. [Google Scholar] [CrossRef]
- Thorgaard, M.V.; Frostholm, L.; Rask, C.U. Childhood and family factors in the development of health anxiety: A systematic review. Child. Health Care 2017, 47, 198–238. [Google Scholar] [CrossRef]
- Dienes, K.A.; Hammen, C.; Henry, R.M.; Cohen, A.N.; Daley, S.E. The stress sensitization hypothesis: Understanding the course of bipolar disorder. J. Affect. Disord. 2006, 95, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Pierce, M.; McManus, S.; Jessop, C.; John, A.; Hotopf, M.; Ford, T.; Hatch, S.; Wessely, S.C.; Abel, K.M. Says who? The significance of sampling in mental health surveys during COVID-19. Lancet Psychiatry 2020, 7, 567–568. [Google Scholar] [CrossRef]
- Dawson, D.L.; Golijani-Moghaddam, N. COVID-19: Psychological flexibility, coping, mental health, and wellbeing in the UK during the pandemic. J. Context. Behav. Sci. 2020, 17, 126–134. [Google Scholar] [CrossRef]
- Huang, C.; Xie, J.; Owusua, T.; Chen, Z.; Wang, J.; Qin, C.; He, Q. Is psychological flexibility a mediator between perceived stress and general anxiety or depression among suspected patients of the 2019 coronavirus disease (COVID-19)? Pers. Individ. Differ. 2021, 183, 111132. [Google Scholar] [CrossRef] [PubMed]
- Wielgus, B.; Urban, W.; Patriak, A.; Cichocki, Ł. Examining the Associations between Psychological Flexibility, Mindfulness, Psychosomatic Functioning, and Anxiety during the COVID-19 Pandemic: A Path Analysis. Int. J. Environ. Res. Public Health 2020, 17, 8764. [Google Scholar] [CrossRef]
- Makriyianis, H.M.; Adams, E.A.; Lozano, L.L.; Mooney, T.A.; Morton, C.; Liss, M. Psychological inflexibility mediates the relationship between adverse childhood experiences and mental health outcomes. J. Context. Behav. Sci. 2019, 14, 82–89. [Google Scholar] [CrossRef]
- Richardson, C.M.E.; Jost, S.A. Psychological flexibility as a mediator of the association between early life trauma and psychological symptoms. Pers. Individ. Differ. 2018, 141, 101–106. [Google Scholar] [CrossRef]
- Gloster, A.T.; Meyer, A.H.; Lieb, R. Psychological flexibility as a malleable public health target: Evidence from a representative sample. J. Context. Behav. Sci. 2017, 6, 166–171. [Google Scholar] [CrossRef] [Green Version]
- Heinrichs, R.W. The Primacy of Cognition in Schizophrenia. Am. Psychol. 2005, 60, 229–242. [Google Scholar] [CrossRef]
- Kashdan, T.B.; Rottenberg, J. Psychological flexibility as a fundamental aspect of health. Clin. Psychol. Rev. 2010, 30, 865–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nolen-Hoeksema, S.; Wisco, B.E.; Lyubomirsky, S. Rethinking Rumination. Perspect. Psychol. Sci. 2008, 3, 400–424. [Google Scholar] [CrossRef] [PubMed]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales; Psychology Foundation of Australia: Sydney, Australia, 1995; ISBN 7334-1423-0. [Google Scholar]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef] [Green Version]
- Broadbent, E.; Petrie, K.J.; Main, J.; Weinman, J. The Brief Illness Perception Questionnaire. J. Psychosom. Res. 2006, 60, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Gloster, A.T.; Block, V.J.; Klotsche, J.; Villanueva, J.; Rinner, M.T.B.; Benoy, C.; Walter, M.; Karekla, M.; Bader, K. Psy-Flex: A contextually sensitive measure of psychological flexibility. J. Context. Behav. Sci. 2021, 22, 13–23. [Google Scholar] [CrossRef]
- Lee, J.; Lee, E.-H.; Moon, S.H. Systematic review of the measurement properties of the Depression Anxiety Stress Scales–21 by applying updated COSMIN methodology. Qual. Life Res. 2019, 28, 2325–2339. [Google Scholar] [CrossRef]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Stewart-Brown, S.; Platt, S.; Tennant, A.; Maheswaran, H.; Parkinson, J.; Weich, S.; Tennant, R.; Taggart, F.; Clarke, A. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): A valid and reliable tool for measuring mental well-being in diverse populations and projects. J. Epidemiol. Community Healh 2011, 65, A38–A39. [Google Scholar] [CrossRef] [Green Version]
- Murphy, A.; Steele, M.; Dube, S.R.; Bate, J.; Bonuck, K.; Meissner, P.; Goldman, H.; Steele, H. Adverse Childhood Experiences (ACEs) Questionnaire and Adult Attachment Interview (AAI): Implications for parent child relationships. Child Abus. Negl. 2014, 38, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation and Conditional Processs Analysis: A Regression Based Approach; Guildford Press: New York, NY, USA, 2013; ISBN 978-1-60918-230-4. [Google Scholar]
- Sher, L. The impact of the COVID-19 pandemic on suicide rates. QJM 2020, 113, 707–712. [Google Scholar] [CrossRef]
- Yao, H.; Chen, J.H.; Xu, Y.F. Patients with mental health disorders in the COVID-19 epidemic. Lancet Psychiatry 2020, 7, e21. [Google Scholar] [CrossRef]
- Bambra, C.; Riordan, R.; Ford, J.; Matthews, F. The COVID-19 pandemic and health inequalities. J. Epidemiol. Community Health 2020, 74, 964–968. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, 19–21. [Google Scholar] [CrossRef] [Green Version]
- Robinson, E.; Sutin, A.R.; Daly, M.; Jones, A. A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. J. Affect. Disord. 2022, 296, 567–576. [Google Scholar] [CrossRef]
- Shevlin, M.; Butter, S.; McBride, O.; Murphy, J.; Gibson-Miller, J.; Hartman, T.K.; Levita, L.; Mason, L.; Martinez, A.P.; McKay, R.; et al. Refuting the myth of a “tsunami” of mental ill-health in populations affected by COVID-19: Evidence that response to the pandemic is heterogenous, not homogeneous. Psychol. Med. 2021, 1–9. [Google Scholar] [CrossRef]
- Cullen, W.; Gulati, G.; Kelly, B.D. Mental health in the COVID-19 pandemic. QJM 2020, 113, 311–312. [Google Scholar] [CrossRef]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair allocation of scarce medical resources in the time of COVID-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total Cohort (n = 231) | No ACEs (n = 75) | Low ACE 1-3 (n = 110) | High ACE 4 or More (n = 46) | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Time 1 | Time 2 | p | d | Time 1 | Time 2 | p | d | Time 1 | Time 2 | p | d | Time 1 | Time 2 | p | d | |||||||||
| M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | |||||||||
| Depression | 5.36 | 4.64 | 7.19 | 5.35 | 0.001 | −0.409 | 5.24 | 4.24 | 5.93 | 4.77 | 0.139 | −0.173 | 5.42 | 4.54 | 7.75 | 5.48 | 0.001 | −0.533 | 5.41 | 5.52 | 7.87 | 5.66 | 0.001 | −0.485 |
| Anxiety | 3.11 | 3.38 | 3.60 | 4.20 | 0.046 | −0.132 | 3.12 | 3.42 | 2.85 | 3.55 | 0.442 | −0.089 | 2.95 | 2.98 | 3.80 | 4.20 | 0.032 | −0.208 | 3.50 | 4.18 | 4.33 | 5.02 | 0.112 | −0.239 |
| Stress | 6.61 | 4.66 | 7.85 | 5.11 | 0.001 | −0.265 | 6.69 | 4.20 | 6.69 | 5.05 | 1.00 | 0.000 | 6.59 | 4.77 | 8.61 | 5.24 | 0.001 | −0.438 | 6.50 | 5.18 | 7.91 | 4.60 | 0.058 | −0.287 |
| Wellbeing | 46.88 | 8.32 | 43.80 | 9.58 | 0.001 | −0.367 | 47.89 | 7.17 | 45.55 | 9.36 | 0.001 | 0.266 | 46.65 | 8.03 | 43.35 | 9.80 | 0.001 | −0.404 | 45.78 | 42.02 | 42.02 | 9.10 | 0.001 | 0.452 |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| 1 ACE Questionnaire | 1 | - | - | - | - | - |
| 2 PsyFlex | −0.03 | 1 | - | - | - | - |
| 3 DASS-21: Depression | 0.35 * | −0.70 *** | 1 | - | - | - |
| 4 DASS-21: Anxiety | 0.31 ** | −0.52 *** | 0.65 *** | 1 | - | - |
| 5 DASS-21: Stress | 0.24 | −0.63 *** | 0.78 *** | 0.72 *** | 1 | - |
| 6 Well-being | −0.58 * | 1.34 *** | −0.77 *** | −0.58 *** | −0.70 *** | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Browne, A.; Stafford, O.; Berry, A.; Murphy, E.; Taylor, L.K.; Shevlin, M.; McHugh, L.; Carr, A.; Burke, T. Psychological Flexibility Mediates Wellbeing for People with Adverse Childhood Experiences during COVID-19. J. Clin. Med. 2022, 11, 377. https://doi.org/10.3390/jcm11020377
Browne A, Stafford O, Berry A, Murphy E, Taylor LK, Shevlin M, McHugh L, Carr A, Burke T. Psychological Flexibility Mediates Wellbeing for People with Adverse Childhood Experiences during COVID-19. Journal of Clinical Medicine. 2022; 11(2):377. https://doi.org/10.3390/jcm11020377
Chicago/Turabian StyleBrowne, Angela, Owen Stafford, Anna Berry, Eddie Murphy, Laura K. Taylor, Mark Shevlin, Louise McHugh, Alan Carr, and Tom Burke. 2022. "Psychological Flexibility Mediates Wellbeing for People with Adverse Childhood Experiences during COVID-19" Journal of Clinical Medicine 11, no. 2: 377. https://doi.org/10.3390/jcm11020377
APA StyleBrowne, A., Stafford, O., Berry, A., Murphy, E., Taylor, L. K., Shevlin, M., McHugh, L., Carr, A., & Burke, T. (2022). Psychological Flexibility Mediates Wellbeing for People with Adverse Childhood Experiences during COVID-19. Journal of Clinical Medicine, 11(2), 377. https://doi.org/10.3390/jcm11020377