

Impact of Early Proteinuria Reduction in Glomerular Disease and Decline of Kidney Function: A Retrospective Cohort
 , and
, and
Abstract
1. Background
2. Materials and Methods
2.1. Participants
2.2. Variables and Outcomes
2.3. Statistical Methods
3. Results
3.1. Decline of Kidney Function
3.2. Predictors of Kidney Function Decline
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Chen, T.K.; Sperati, C.J.; Thavarajah, S.; Grams, M.E. Reducing Kidney Function Decline in Patients With CKD: Core Curriculum 2021. Am. J. Kidney Dis. 2021, 77, 969–983. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, M.; Wiebe, N.; Culleton, B.; House, A.; Rabbat, C.; Fok, M.; McAlister, F.; Garg, A.X. Chronic kidney disease and mortality risk: A systematic review. J. Am. Soc. Nephrol. 2006, 17, 2034–2047. [Google Scholar] [CrossRef] [PubMed]
- Kunwar, D.; Kunwar, R.; Shrestha, B.; Amatya, R.; Risal, A. Depression and Quality of Life among the Chronic Kidney Disease Patients. J. Nepal. Health Res. Counc. 2020, 18, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Vart, P.; Powe, N.R.; McCulloch, C.E.; Saran, R.; Gillespie, B.W.; Saydah, S.; Crews, D.C. National Trends in the Prevalence of Chronic Kidney Disease Among Racial/Ethnic and Socioeconomic Status Groups, 1988–2016. JAMA Netw. Open 2020, 3, e207932. [Google Scholar] [CrossRef] [PubMed]
- Floege, J.; Amann, K. Primary glomerulonephritides. Lancet 2016, 387, 2036–2048. [Google Scholar] [CrossRef]
- Saran, R.; Robinson, B.; Abbott, K.C.; Lawrence, Y.C.; Albertus, P.; Ayanian, J.; Balkrishnan, R.; Bragg-Gresham, J.; Cao, J.; Chen, J.L.T.; et al. US Renal Data System 2016 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2017, 69 (Suppl. S1), A7–A8. [Google Scholar] [CrossRef]
- Chadban, S.J.; Atkins, R.C. Glomerulonephritis. Lancet 2005, 365, 1797–1806. [Google Scholar] [CrossRef]
- Remuzzi, G.; Ruggenenti, P.; Benigni, A. Understanding the nature of renal disease progression. Kidney Int. 1997, 51, 2–15. [Google Scholar] [CrossRef]
- Ruggenenti, P.; Perna, A.; Mosconi, L.; Pisoni, R.; Remuzzi, G. Urinary protein excretion rate is the best independent predictor of ESRF in non-diabetic proteinuric chronic nephropathies. “Gruppo Italiano di Studi Epidemiologici in Nefrologia” (GISEN). Kidney Int. 1998, 53, 1209–1216. [Google Scholar] [CrossRef]
- Minutolo, R.; Gabbai, F.B.; Provenzano, M.; Chiodini, P.; Borrelli, S.; Garofalo, C.; Sasso, F.C.; Santoro, D.; Bellizzi, V.; Conte, G.; et al. Cardiorenal prognosis by residual proteinuria level in diabetic chronic kidney disease: Pooled analysis of four cohort studies. Nephrol. Dial. Transplant. 2018, 33, 1942–1949. [Google Scholar] [CrossRef]
- Coresh, J.; Heerspink, H.J.L.; Sang, Y.; Matsushita, K.; Arnlov, J.; Astor, B.C.; Black, C.; Brunskill, N.J.; Carrero, J.-J.; Feldman, H.I.; et al. Change in albuminuria and subsequent risk of end-stage kidney disease: An individual participant-level consortium meta-analysis of observational studies. Lancet Diabetes Endocrinol. 2019, 7, 115–127. [Google Scholar] [CrossRef]
- Haider, M.Z.; Aslam, A. Proteinuria. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- CKD-EPI Creatinine Equation. 2021. Available online: https://www.kidney.org/content/ckd-epi-creatinine-equation-2021 (accessed on 6 February 2022).
- Cattran, D.C.; Feehally, J.; Cook, H.T.; Liu, Z.H.; Fervenza, F.C.; Mezzano, S.A.; Floege, J.; Nachman, P.H.; Gipson, D.S.; Praga, M.; et al. Kidney Disease: Improving Global Outcomes (KDIGO) Glomerulonephritis Work Group. KDIGO Clinical Practice Guideline for Glomerulonephritis. Kidney Inter. Suppl. 2012, 2, 139–274. [Google Scholar]
- Berhane, A.M.; Weil, E.J.; Knowler, W.C.; Nelson, R.G.; Hanson, R.L. Albuminuria and estimated glomerular filtration rate as predictors of diabetic end-stage renal disease and death. Clin. J. Am. Soc. Nephrol. 2011, 6, 2444–2451. [Google Scholar] [CrossRef] [PubMed]
- Ali, I.; Chinnadurai, R.; Ibrahim, S.T.; Green, D.; Kalra, P.A. Predictive factors of rapid linear renal progression and mortality in patients with chronic kidney disease. BMC Nephrol. 2020, 21, 345. [Google Scholar] [CrossRef]
- Reich, H.N.; Troyanov, S.; Scholey, J.W.; Cattran, D.C.; Toronto Glomerulonephritis Registry. Remission of proteinuria improves prognosis in IgA nephropathy. J. Am. Soc. Nephrol. 2007, 18, 3177–3183. [Google Scholar]
- Wang, Y.; Rangan, G.K.; Tay, Y.C.; Wang, Y.; Harris, D.C. Induction of monocyte chemoattractant protein-1 by albumin is mediated by nuclear factor kappaB in proximal tubule cells. J. Am. Soc. Nephrol. 1999, 10, 1204–1213. [Google Scholar] [CrossRef]
- Nakajima, H.; Takenaka, M.; Kaimori, J.-Y.; Hamano, T.; Iwatani, H.; Sugaya, T.; Ito, T.; Hori, M.; Imai, E. Activation of the signal transducer and activator of transcription signaling pathway in renal proximal tubular cells by albumin. J. Am. Soc. Nephrol. 2004, 15, 276–285. [Google Scholar] [CrossRef]
- Okada, T.; Nagao, T.; Matsumoto, H.; Nagaoka, Y.; Wada, T.; Nakao, T. Histological predictors for renal prognosis in diabetic nephropathy in diabetes mellitus type 2 patients with overt proteinuria. Nephrology 2012, 17, 68–75. [Google Scholar] [CrossRef]
- Sandokji, I.; Greenberg, J.H. Plasma and Urine Biomarkers of CKD: A Review of Findings in the CKiD Study. Semin. Nephrol. 2021, 41, 416–426. [Google Scholar] [CrossRef]
- Wang, Y.-N.; Ma, S.-X.; Chen, Y.-Y.; Chen, L.; Liu, B.-L.; Liu, Q.-Q.; Zhao, Y.-Y. Chronic kidney disease: Biomarker diagnosis to therapeutic targets. Clin. Chim. Acta 2019, 499, 54–63. [Google Scholar] [CrossRef]
- Zhang, W.R.; Parikh, C.R. Biomarkers of Acute and Chronic Kidney Disease. Annu. Rev. Physiol. 2019, 81, 309–333. [Google Scholar] [CrossRef] [PubMed]
- Ix, J.H.; Shlipak, M.G. The Promise of Tubule Biomarkers in Kidney Disease: A Review. Am. J. Kidney Dis. 2021, 78, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Mihai, S.; Codrici, E.; Popescu, I.D.; Enciu, A.-M.; Albulescu, L.; Necula, L.G.; Mambet, C.; Anton, G.; Tanase, C. Inflammation-Related Mechanisms in Chronic Kidney Disease Prediction, Progression, and Outcome. J. Immunol. Res. 2018, 2018, 2180373. [Google Scholar] [CrossRef] [PubMed]
- Jalal, D.; Sanford, B.; Renner, B.; Eyck, P.T.; Laskowski, J.; Cooper, J.; Sun, M.; Zakharia, Y.; Spitz, D.; Dokun, A.; et al. Detection of pro angiogenic and inflammatory biomarkers in patients with CKD. Sci. Rep. 2021, 11, 8786. [Google Scholar] [CrossRef]
- Rysz, J.; Gluba-Brzózka, A.; Franczyk, B.; Jabłonowski, Z.; Ciałkowska-Rysz, A. Novel Biomarkers in the Diagnosis of Chronic Kidney Disease and the Prediction of Its Outcome. Int. J. Mol. Sci. 2017, 18, 1702. [Google Scholar] [CrossRef]
- Pontillo, C.; Mischak, H. Urinary biomarkers to predict CKD: Is the future in multi-marker panels? Nephrol. Dial. Transplant. 2016, 31, 1373–1375. [Google Scholar] [CrossRef]
- Woo, K.T.; Lau, Y.K.; Wong, K.S.; Chiang, G.S. ACEI/ATRA therapy decreases proteinuria by improving glomerular permselectivity in IgA nephritis. Kidney Int. 2000, 58, 2485–2491. [Google Scholar] [CrossRef]
- Morelli, E.; Loon, N.; Meyer, T.; Peters, W.; Myers, B.D. Effects of converting-enzyme inhibition on barrier function in diabetic glomerulopathy. Diabetes 1990, 39, 76–82. [Google Scholar] [CrossRef]
- Hou, F.F.; Zhang, X.; Zhang, G.H.; Xie, D.; Chen, P.Y.; Zhang, W.R.; Jiang, J.P.; Liang, M.; Wang, G.B.; Liu, Z.R.; et al. Efficacy and safety of benazepril for advanced chronic renal insufficiency. N. Engl. J. Med. 2006, 354, 131–140. [Google Scholar] [CrossRef]
- Ruggenenti, P.; Perna, A.; Gherardi, G.; Garini, G.; Zoccali, C.; Salvadori, M.; Scolari, F.; Schena, F.P.; Remuzzi, G. Renoprotective properties of ACE-inhibition in non-diabetic nephropathies with non-nephrotic proteinuria. Lancet 1999, 354, 359–364. [Google Scholar] [CrossRef]
- Currie, G.; Taylor, A.H.M.; Fujita, T.; Ohtsu, H.; Lindhardt, M.; Rossing, P.; Boesby, L.; Edwards, N.C.; Ferro, C.; Townend, J.; et al. Effect of mineralocorticoid receptor antagonists on proteinuria and progression of chronic kidney disease: A systematic review and meta-analysis. BMC Nephrol. 2016, 17, 127. [Google Scholar] [CrossRef] [PubMed]
- Cherney, D.Z.I.; Zinman, B.; Inzucchi, S.E.; Koitka-Weber, A.; Mattheus, M.; von Eynatten, M.; Wanner, C. Effects of empagliflozin on the urinary albumin-to-creatinine ratio in patients with type 2 diabetes and established cardiovascular disease: An exploratory analysis from the EMPA-REG OUTCOME randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. 2017, 5, 610–621. [Google Scholar] [CrossRef]
- Heerspink, H.J.; Johnsson, E.; Gause-Nilsson, I.; Cain, V.A.; Sjöström, C.D. Dapagliflozin reduces albuminuria in patients with diabetes and hypertension receiving renin-angiotensin blockers. Diabetes Obes Metab. 2016, 18, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Petrykiv, S.I.; Laverman, G.D.; de Zeeuw, D.; Heerspink, H.J.L. The albuminuria-lowering response to dapagliflozin is variable and reproducible among individual patients. Diabetes Obes Metab. 2017, 19, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Jongs, N.; Greene, T.; Chertow, G.M.; McMurray, J.J.V.; Langkilde, A.M.; Correa-Rotter, R.; Rossing, P.; Sjöström, C.D.; Stefansson, B.V.; Toto, R.D.; et al. Effect of dapagliflozin on urinary albumin excretion in patients with chronic kidney disease with and without type 2 diabetes: A prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. 2021, 9, 755–766. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Patients with Glomerular Disease N = 197 |
|---|---|
| Demographics: | |
| Age (years) | 41.7 ± 19.7 |
| Gender (male), n (%) | 109 (55.3) |
| At the diagnosis: | |
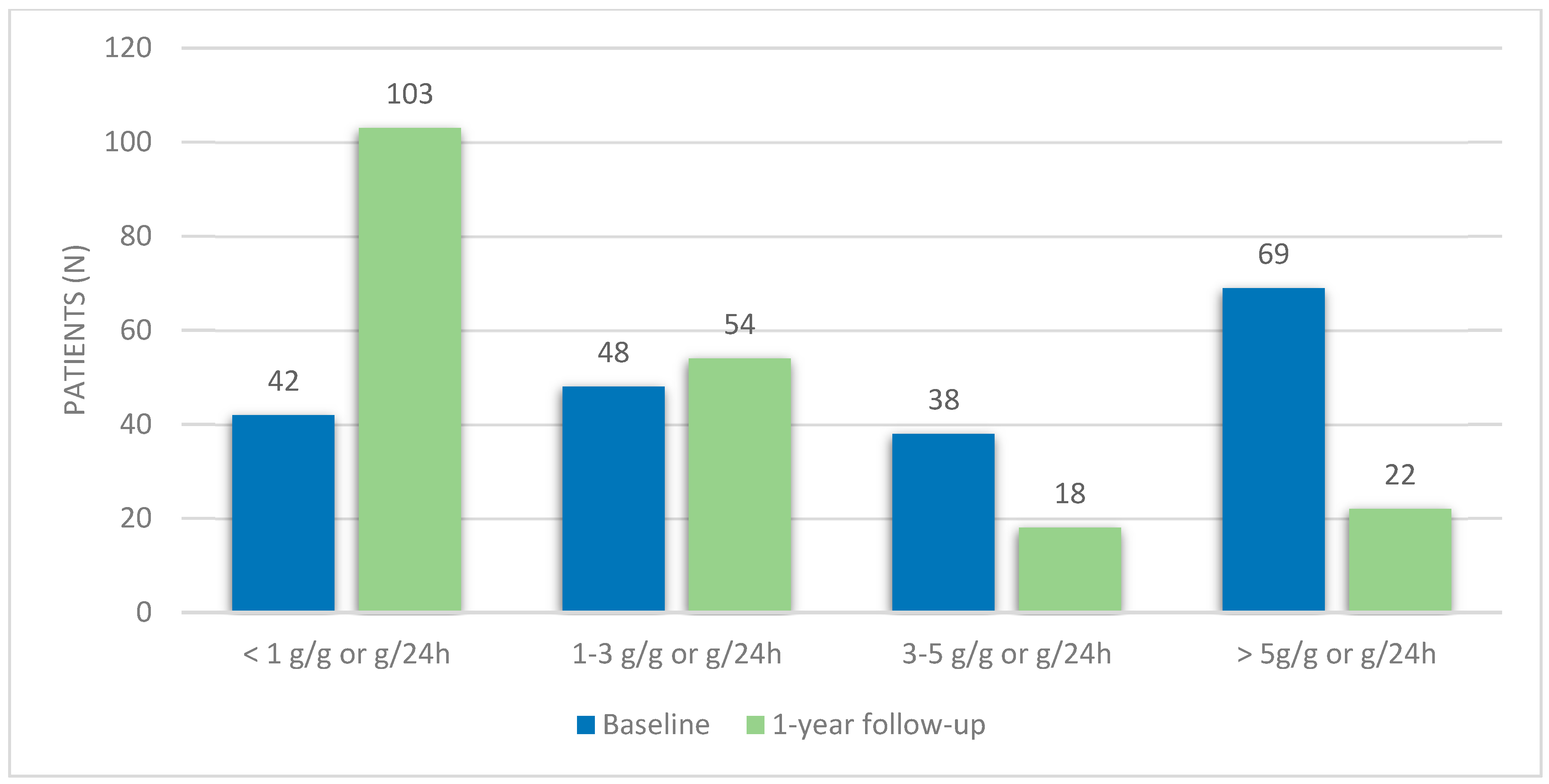
| Proteinuria | 3.5 (IQR 5.8) |
| eGFR (mL/min/1.73 m2) | 81.5 ± 49.8 |
| eGFR < 60 mL/min/1.73 m2 | 82 (41.6) |
| Hematuria, n (%) | 140 (71.1) |
| RAAS inhibitors, n (%) | 197 (100) |
| Immunosuppressive therapy, n (%) | 106 (53.8) |
| At one-year follow-up: | |
| Proteinuria | 0.9 (IQR 2.4) |
| Proteinuria variation (g/g or g/24 h) | 1.2 (IQR 4.0) |
| Proteinuria reduction ≥ 25%, n (%) | 126 (64.0) |
| Proteinuria reduction ≥ 50%, n (%) | 98 (49.7) |
| Complete remission, n (%) | 54 (27.4) |
| Partial remission, n (%) | 95 (48.2) |
| Long-term follow-up: | |
| Time of follow-up (years) | 6.5 ± 5.3 |
| eGFR at the end of the follow-up (mL/min/1.73 m2) | 72.1 ± 43.3 |
| eGFR variation (mL/min/1.73 m2) | 9.3 (IQR 26.6) |
| eGFR < 60 mL/min/1.73 m2, n (%) | 84 (42.6) |
| eGFR decline, n (%) | 134 (68.0) |
| Annual decline of eGFR (mL/min/1.73 m2) | 1.4 (IQR 5.2) |
| Decline of the eGFR ≥ 25%, n (%) | 64 (32.5) |
| Decline of the eGFR ≥ 50%, n (%) | 26 (13.2) |
| Glomerular Disease | Minimal Change Disease | Focal Segmental Glomerulosclerosis | Membranoproliferative Glomerulonephritis | IgA Nephropathy | Membranous Nephropathy | p Value |
|---|---|---|---|---|---|---|
| Frequency, n (%) | 36 (18.3%) | 63 (31.9%) | 21 (10.7%) | 56 (28.4%) | 21 (10.7%) | |
| Baseline proteinuria (g/g or g/24 h) | 5.8 (IQR 7.2) | 4.0 (IQR 5.7) | 3.6 (IQR 3.6) | 0.9 (IQR 1.4) | 6.1 (IQR 4.5) | <0.001 |
| Baseline eGFR (mL/min/1.73 m2) | 100.9 ± 46.2 | 75.2 ± 57.0 | 52.3 ± 20.3 | 87.8 ± 25.2 | 79.2 ± 37.3 | 0.005 |
| 1-year proteinuria (g/g or g/24 h) | 0.8 (IQR 2.5) | 1.4 (IQR 3.0) | 1.1 (IQR 1.5) | 0.7 (IQR 1.2) | 0.9 (IQR 3.9) | 0.070 |
| eGFR decline (mL/min/1.73 m2) | 3.3 (IQR 29.5) | 6.3 (IQR 31.0) | 2.4 (IQR 41.0) | 12.8 (IQR 23.9) | 10.5 (IQR 33.0) | 0.007 |
| eGFR ≥ 25%, n (%) | 5 (13.9%) | 25 (39.7%) | 8 (38.1%) | 20 (35.7%) | 6 (28.6%) | 0.096 |
| Characteristics | eGFR Decline < 25%, N = 133 | eGFR Decline ≥ 25%, N = 64 | p Value |
|---|---|---|---|
| Demographics: | |||
| Age (years) | 40.2 ± 18.8 | 45.4 ± 20.7 | 0.082 |
| Gender (male), n (%) | 72 (54.1) | 37 (57.8) | 0.627 |
| Baseline Characteristics: | |||
| eGFR (mL/min/1.73 m2) | 81.9 ± 44.3 | 80.7 ± 59.9 | 0.880 |
| eGFR < 60 mL/min/1.73 m2 | 51 (38.3) | 31 (48.4) | 0.178 |
| Hematuria, n (%) | 92 (69.1) | 48 (75.0) | 0.398 |
| Proteinuria (g/g or g/24 h) | 3.5 (IQR 6.8) | 2.8 (IQR 6.4) | 0.435 |
| Proteinuria < 1 g/g or g/24 h, n (%) | 30 (22.6) | 12 (18.8) | 0.541 |
| Proteinuria 1–3 g/g or g/24 h, n (%) | 26 (19.5) | 22 (34.4) | 0.023 |
| Proteinuria 3–5 g/g or g/24 h, n (%) | 26 (19.5) | 12 (18.8) | 0.249 |
| Proteinuria > 5 g/g or g/24 h, n (%) | 51 (38.3) | 18 (28.1) | 0.159 |
| Immunosuppressive therapy, n (%) | 73 (54.9) | 33 (51.5) | 0.828 |
| At one-year follow-up: | |||
| Proteinuria reduction ≥ 25%, n (%) | 88 (66.1) | 38 (59.3) | 0.353 |
| Proteinuria reduction ≥ 50%, n (%) | 72 (54.1) | 26 (40.6) | 0.076 |
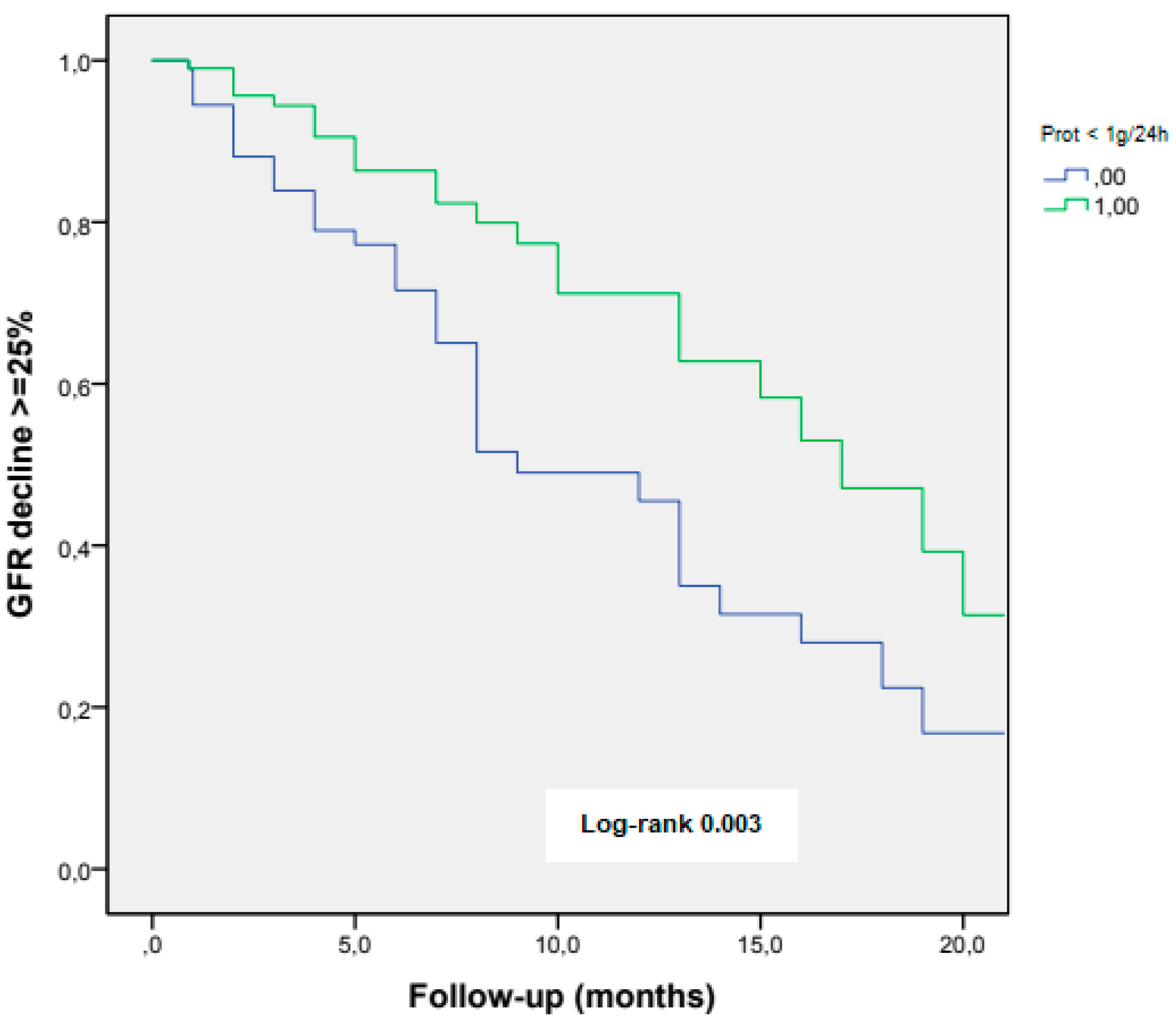
| Proteinuria < 1 g/g or g/24 h, n (%) | 78 (58.6) | 25 (39.1) | 0.010 |
| Proteinuria 1–3 g/g or g/24 h, n (%) | 31 (23.3) | 23 (35.9) | 0.047 |
| Proteinuria < 3 g/g or g/24 h, n (%) | 109 (82.0) | 48 (75.0) | 0.171 |
| Proteinuria 3–5 g/g or g/24 h, n (%) | 9 (6.8) | 9 (14.1) | 0.083 |
| Proteinuria ≥ 5 g/g or g/24 h, n (%) | 15 (11.3) | 7 (10.9) | 0.576 |
| Partial remission, n (%) | 69 (51.9) | 26 (40.6) | 0.092 |
| Complete remission, n (%) | 40 (30.1) | 14 (21.9) | 0.149 |
| Long-term follow-up: | |||
| Follow-up time (years) | 6.1 ± 5.2 | 7.4 ± 5.3 | 0.141 |
| eGFR (mL/min/1.73 m2) | 85.6 ± 39.1 | 43.4 ± 37.5 | <0.001 |
| eGFR < 60 mL/min/1.73 m2, n (%) | 40 (30.1) | 36 (56.3) | <0.001 |
| eGFR decline (mL/min/1.73 m2) | 1.8 (IQR 22,7) | 31.6 (IQR 28.8) | <0.001 |
| eGFR annual decline (mL/min/1.73 m2) | 0.4 (IQR 3.3) | 5.1 (IQR 5.1) | <0.001 |
| Characteristics | Hazard Ratio (95% CI) | p Value |
|---|---|---|
| Baseline Characteristics: | ||
| Age (years) | 1.01 (1.00–1.03) | 0.083 |
| Gender (male) | 1.16 (0.64–2.12) | 0.627 |
| eGFR (mL/min/1.73 m2) | 1.00 (0.99–1.01) | 0.880 |
| eGFR < 60 mL/min/1.73 m2 | 1.51 (0.83–2.76) | 0.179 |
| Hematuria | 1.34 (0.68–2.63) | 0.339 |
| Proteinuria (g/g or g/24 h) | 0.97 (0.91–1.04) | 0.434 |
| Proteinuria < 1 g/g or g/24 h Proteinuria 1–3 g/g or g/24 h Proteinuria 3–5 g/g or g/24 h Proteinuria ≥ 5 g/g or g/24 h | 0.79 (0.38–1.67) 2.16 (1.10–4.22) 0.70 (0.39–1.28) 0.63 (0.33–1.20) | 0.542 0.025 0.249 0.161 |
| Immunosuppressive therapy | 0.94 (0.51–1.71) | 0.828 |
| At one-year follow-up: | ||
| Proteinuria reduction ≥ 25% | 0.75 (0.40–1.38) | 0.353 |
| Proteinuria reduction ≥ 50% | 0.58 (0.32–1.06) | 0.077 |
| Proteinuria < 1 g/g or g/24 h | 0.45 (0.25–0.83) | 0.011 |
| Partial remission | 0.64 (0.35–1.16) | 0.140 |
| Complete remission | 1.22 (0.32–1.31) | 0.229 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marques, F.; Reis, J.; Godinho, I.; Pereira, M.; Fernandes, P.; Jorge, S.; Lopes, J.A.; Gameiro, J. Impact of Early Proteinuria Reduction in Glomerular Disease and Decline of Kidney Function: A Retrospective Cohort. J. Clin. Med. 2022, 11, 5968. https://doi.org/10.3390/jcm11195968
Marques F, Reis J, Godinho I, Pereira M, Fernandes P, Jorge S, Lopes JA, Gameiro J. Impact of Early Proteinuria Reduction in Glomerular Disease and Decline of Kidney Function: A Retrospective Cohort. Journal of Clinical Medicine. 2022; 11(19):5968. https://doi.org/10.3390/jcm11195968
Chicago/Turabian StyleMarques, Filipe, Joana Reis, Iolanda Godinho, Marta Pereira, Paulo Fernandes, Sofia Jorge, José António Lopes, and Joana Gameiro. 2022. "Impact of Early Proteinuria Reduction in Glomerular Disease and Decline of Kidney Function: A Retrospective Cohort" Journal of Clinical Medicine 11, no. 19: 5968. https://doi.org/10.3390/jcm11195968
APA StyleMarques, F., Reis, J., Godinho, I., Pereira, M., Fernandes, P., Jorge, S., Lopes, J. A., & Gameiro, J. (2022). Impact of Early Proteinuria Reduction in Glomerular Disease and Decline of Kidney Function: A Retrospective Cohort. Journal of Clinical Medicine, 11(19), 5968. https://doi.org/10.3390/jcm11195968