


Effects of Transcranial Direct Current Stimulation on Sleep in Athletes: A Protocol of a Randomized Controlled Trial
 ,
,  ,
,  and
and 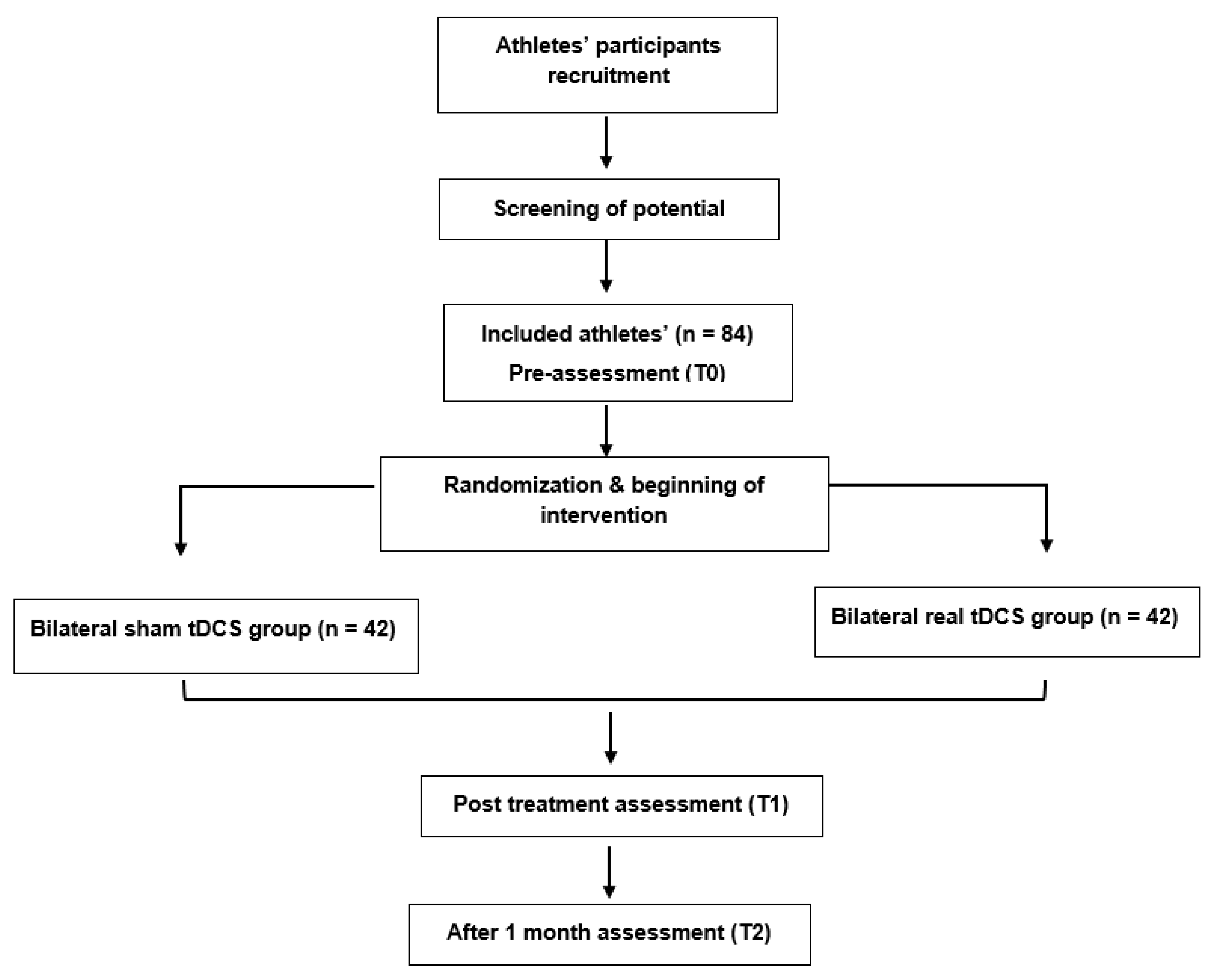{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Randomization Allocation and Blinding
2.4. Sample Size Calculation
2.5. Procedures
2.6. Assessments and Outcome Measures
2.7. Primary Outcome Measures
2.7.1. A-Sleep Monitoring
- i.
- Time in bed: the time between the ‘Lights Out’ and ‘Got Up’ times;
- ii.
- Actual sleep time: the total time spent sleeping according to the epoch-by-epoch wake or sleep categorization, excluding sleep latency and waking after sleep onset;
- iii.
- Wake after sleep onset: the amount of time a person spends awake, starting from when he or she first falls asleep to becoming fully awake and not attempting to go back to sleep;
- iv.
- Sleep efficiency: the ratio between the actual sleep time and time in bed.
2.7.2. B-Insomnia Severity Index (ISI)
2.7.3. C-Epworth Sleepiness Scale (ESS)
2.8. Secondary Outcome Measures
2.8.1. A-PSQI
2.8.2. B-Depression Anxiety Stress Scale-21 (DASS-21)
2.8.3. C-Medical Outcome Study Short-Form Survey 12-Item (SF-12)
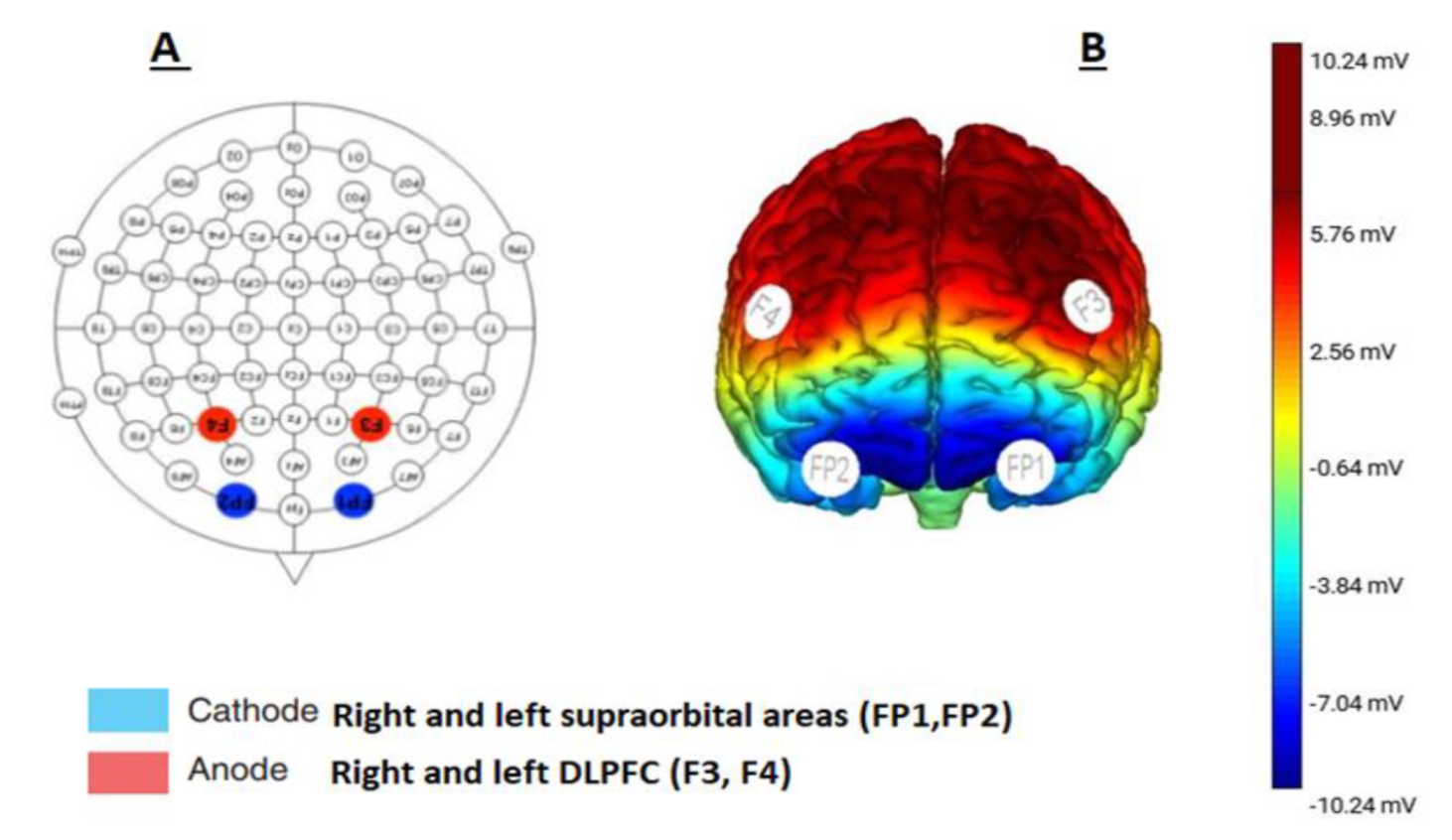
2.9. Intervention
2.10. Treatment Group (Real tDCS Group)
2.11. Control Group (Sham tDCS Group)
2.12. Statistical Analysis
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walsh, N.P.; Halson, S.L.; Sargent, C.; Roach, G.D.; Nédélec, M.; Gupta, L.; Leeder, J.; Fullagar, H.H.; Coutts, A.J.; Edwards, B.J.; et al. Sleep and the Athlete: Narrative Review and 2021 Expert Consensus Recommendations. Br. J. Sports Med. 2021, 55, 356–368. [Google Scholar] [CrossRef]
- Swinbourne, R.; Gill, N.; Vaile, J.; Smart, D. Prevalence of Poor Sleep Quality, Sleepiness and Obstructive Sleep Apnoea Risk Factors in Athletes. Eur. J. Sport Sci. 2016, 16, 850–858. [Google Scholar] [CrossRef]
- Bender, A.; Van Dongen, H.; Samuels, C. Sleep Quality and Chronotype Differences between Elite Athletes and Non-Athlete Controls. Clocks Sleep 2018, 1, 3–12. [Google Scholar] [CrossRef]
- Rodrigues, D.F.; Silva, A.; Rosa, J.P.P.; Ruiz, F.S.; Veríssimo, A.W.; Winckler, C.; Da Rocha, E.A.; Parsons, A.; Tufik, S.; De Mello, M.T. Sleep Quality and Psychobiological Aspects of Brazilian Paralympic Athletes in the London 2012 Pre-Paralympics Period. Motriz. Rev. Educ. Fis. 2015, 21, 168–176. [Google Scholar] [CrossRef]
- Roberts, S.S.H.; Teo, W.P.; Warmington, S.A. Effects of Training and Competition on the Sleep of Elite Athletes: A Systematic Review and Meta-Analysis. Br. J. Sports Med. 2019, 53, 513–522. [Google Scholar] [CrossRef]
- Gupta, L.; Morgan, K.; Gilchrist, S. Does Elite Sport Degrade Sleep Quality? A Systematic Review. Sport. Med. 2017, 47, 1317–1333. [Google Scholar] [CrossRef]
- Fowler, P.; Duffield, R.; Howle, K.; Waterson, A.; Vaile, J. Effects of Northbound Long-Haul International Air Travel on Sleep Quantity and Subjective Jet Lag and Wellness in Professional Australian Soccer Players. Int. J. Sports Physiol. Perform. 2015, 10, 648–654. [Google Scholar] [CrossRef]
- Kölling, S.; Steinacker, J.M.; Endler, S.; Ferrauti, A.; Meyer, T.; Kellmann, M. The Longer the Better: Sleep-Wake Patterns during Preparation of the World Rowing Junior Championships. Chronobiol. Int. 2016, 33, 73–84. [Google Scholar] [CrossRef]
- Nedelec, M.; Dawson, B.; Dupont, G. Influence of Night Soccer Matches on Sleep in Elite Players. J. Strength Cond. Res. 2019, 33, 174–179. [Google Scholar] [CrossRef]
- de Blasiis, K.; Joncheray, H.; Elefteriou, J.; Lesenne, C.; Nedelec, M. Sleep-Wake Behavior in Elite Athletes: A Mixed-Method Approach. Front. Psychol. 2021, 12, 3337. [Google Scholar] [CrossRef]
- Erlacher, D.; Ehrlenspiel, F.; Adegbesan, O.A.; El-Din, H.G. Sleep Habits in German Athletes before Important Competitions or Games. J. Sports Sci. 2011, 29, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Desseilles, M.; Dang-Vu, T.; Schabus, M.; Sterpenich, V.; Maquet, P.; Schwartz, S. Neuroimaging Insights into the Pathophysiology of Sleep Disorders. Sleep 2008, 31, 777–794. [Google Scholar] [CrossRef] [PubMed]
- Drummond, S.P.A.; Brown, G.G. The Effects of Total Sleep Deprivation on Cerebral Responses to Cognitive Performance. Neuropsychopharmacology 2001, 25, S68–S73. [Google Scholar] [CrossRef]
- Durmer, J.S.; Dinges, D.F. Neurocognitive Consequences of Sleep Deprivation. Semin. Neurol. 2005, 25, 117–129. [Google Scholar] [CrossRef]
- Thomas, M.; Sing, H.; Belenky, G.; Holcomb, H.; Mayberg, H.; Dannals, R.; Wagner, H.; Thorne, D.; Popp, K.; Rowland, L.; et al. Neural Basis of Alertness and Cognitive Performance Impairments during Sleepiness. I. Effects of 24 h of Sleep Deprivation on Waking Human Regional Brain Activity. J. Sleep Res. 2000, 9, 335–352. [Google Scholar] [CrossRef] [PubMed]
- Dondé, C.; Brunelin, J.; Micoulaud-Franchi, J.A.; Maruani, J.; Lejoyeux, M.; Polosan, M.; Geoffroy, P.A. The Effects of Transcranial Electrical Stimulation of the Brain on Sleep: A Systematic Review. Front. Psychiatry 2021, 12, 710. [Google Scholar] [CrossRef]
- Paßmann, S.; Külzow, N.; Ladenbauer, J.; Antonenko, D.; Grittner, U.; Tamm, S.; Flöel, A. Boosting Slow Oscillatory Activity Using TDCS during Early Nocturnal Slow Wave Sleep Does Not Improve Memory Consolidation in Healthy Older Adults. Brain Stimul. 2016, 9, 730–739. [Google Scholar] [CrossRef]
- Marshall, L.; Helgadóttir, H.; Mölle, M.; Born, J. Boosting Slow Oscillations during Sleep Potentiates Memory. Nature 2006, 444, 610–613. [Google Scholar] [CrossRef]
- Tononi, G.; Cirelli, C. Sleep and the Price of Plasticity: From Synaptic and Cellular Homeostasis to Memory Consolidation and Integration. Neuron 2014, 81, 12–34. [Google Scholar] [CrossRef]
- Halson, S.L. Sleep in Elite Athletes and Nutritional Interventions to Enhance Sleep. Sport. Med. 2014, 44, 13. [Google Scholar] [CrossRef]
- Halson, S.L.; Burke, L.M.; Pearce, J. Nutrition for Travel: From Jet Lag to Catering. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 228–235. [Google Scholar] [CrossRef]
- Blanchfield, A.W.; Lewis-Jones, T.M.; Wignall, J.R.; Roberts, J.B.; Oliver, S.J. The Influence of an Afternoon Nap on the Endurance Performance of Trained Runners. Eur. J. Sport Sci. 2018, 18, 1177–1184. [Google Scholar] [CrossRef]
- Charest, J.; Marois, A.; Bastien, C.H. Can a TDCS Treatment Enhance Subjective and Objective Sleep among Student-Athletes? J. Am. Coll. Health 2021, 69, 378–389. [Google Scholar] [CrossRef]
- Boutron, I.; Moher, D.; Altman, D.G.; Schulz, K.F.; Ravaud, P. Extending the CONSORT Statement to Randomized Trials of Nonpharmacologic Treatment: Explanation and Elaboration. Ann. Intern. Med. 2008, 148, 295–309. [Google Scholar] [CrossRef]
- Cabré-Riera, A.; Torrent, M.; Donaire-Gonzalez, D.; Vrijheid, M.; Cardis, E.; Guxens, M. Telecommunication Devices Use, Screen Time and Sleep in Adolescents. Environ. Res. 2019, 171, 341–347. [Google Scholar] [CrossRef]
- Aili, K.; Åström-Paulsson, S.; Stoetzer, U.; Svartengren, M.; Hillert, L. Reliability of Actigraphy and Subjective Sleep Measurements in Adults: The Design of Sleep Assessments. J. Clin. Sleep Med. 2017, 13, 39–47. [Google Scholar] [CrossRef]
- Suleiman, K.H.; Yates, B.C. Translating the Insomnia Severity Index into Arabic. J. Nurs. Scholarsh. 2011, 43, 49–53. [Google Scholar] [CrossRef]
- Ahmed, A.E.; Fatani, A.; Al-Harbi, A.; Al-Shimemeri, A.; Ali, Y.Z.; Baharoon, S.; Al-Jahdali, H. Validation of the Arabic Version of the Epworth Sleepiness Scale. J. Epidemiol. Glob. Health 2014, 4, 297–302. [Google Scholar] [CrossRef]
- Suleiman, K.H.; Yates, B.C.; Berger, A.M.; Pozehl, B.; Meza, J. Translating the Pittsburgh Sleep Quality Index into Arabic. West. J. Nurs. Res. 2010, 32, 250–268. [Google Scholar] [CrossRef]
- Claudino, J.G.; Gabbet, T.J.; De Sá Souza, H.; Simim, M.; Fowler, P.; De Alcantara Borba, D.; Melo, M.; Bottino, A.; Loturco, I.; D’Almeida, V.; et al. Which Parameters to Use for Sleep Quality Monitoring in Team Sport Athletes? A Systematic Review and Meta-Analysis. BMJ Open Sport Exerc. Med. 2019, 5. [Google Scholar] [CrossRef]
- Moussa, M.T.; Lovibond, P.; Laube, R.; Megahead, H.A. Psychometric Properties of an Arabic Version of the Depression Anxiety Stress Scales (DASS). Res. Soc. Work Pract. 2017, 27, 375–386. [Google Scholar] [CrossRef]
- Vaughan, R.S.; Edwards, E.J.; MacIntyre, T.E. Mental Health Measurement in a Post Covid-19 World: Psychometric Properties and Invariance of the DASS-21 in Athletes and Non-Athletes. Front. Psychol. 2020, 11, 590559. [Google Scholar] [CrossRef]
- Haddad, C.; Sacre, H.; Obeid, S.; Salameh, P.; Hallit, S. Validation of the Arabic Version of the “12-Item Short-Form Health Survey” (SF-12) in a Sample of Lebanese Adults. Arch. Public Health 2021, 79, 1–8. [Google Scholar] [CrossRef]
- Jurcak, V.; Tsuzuki, D.; Dan, I. 10/20, 10/10, and 10/5 Systems Revisited: Their Validity as Relative Head-Surface-Based Positioning Systems. Neuroimage 2007, 34, 1600–1611. [Google Scholar] [CrossRef]
- Taylor, L.; Chrismas, B.C.R.; Dascombe, B.; Chamari, K.; Fowler, P.M. Sleep Medication and Athletic Performance-The Evidence for Practitioners and Future Research Directions. Front. Physiol. 2016, 7, 83. [Google Scholar] [CrossRef]
- Perrier, J.; Clochon, P.; Bertran, F.; Couque, C.; Bulla, J.; Denise, P.; Bocca, M.L. Specific EEG Sleep Pattern in the Prefrontal Cortex in Primary Insomnia. PLoS ONE 2015, 10, e0116864. [Google Scholar] [CrossRef]
- Frase, L.; Piosczyk, H.; Zittel, S.; Jahn, F.; Selhausen, P.; Krone, L.; Feige, B.; Mainberger, F.; Maier, J.G.; Kuhn, M.; et al. Modulation of Total Sleep Time by Transcranial Direct Current Stimulation (TDCS). Neuropsychopharmacology 2016, 41, 2577–2586. [Google Scholar] [CrossRef]
- Steriade, M.; Timofeev, I. Neuronal Plasticity in Thalamocortical Networks during Sleep and Waking Oscillations. Neuron 2003, 37, 563–576. [Google Scholar] [CrossRef]
- Bolling, A.J.; King, V.L.; Enam, T.; McDonough, I.M. Using Transcranial Direct Current Stimulation (TDCS) on the Dorsolateral Prefrontal Cortex to Promote Long-Term Foreign Language Vocabulary Learning. Brain Cogn. 2021, 154, 105789. [Google Scholar] [CrossRef]
- Bikson, M.; Grossman, P.; Thomas, C.; Zannou, A.L.; Jiang, J.; Adnan, T.; Mourdoukoutas, A.P.; Kronberg, G.; Truong, D.; Boggio, P.; et al. Safety of Transcranial Direct Current Stimulation: Evidence Based Update 2016. Brain Stimul. 2016, 9, 641–661. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Etoom, M.; Alwardat, M.; Alghwiri, A.; Lena, F.; Romigi, A. Effects of Transcranial Direct Current Stimulation on Sleep in Athletes: A Protocol of a Randomized Controlled Trial. J. Clin. Med. 2022, 11, 5883. https://doi.org/10.3390/jcm11195883
Etoom M, Alwardat M, Alghwiri A, Lena F, Romigi A. Effects of Transcranial Direct Current Stimulation on Sleep in Athletes: A Protocol of a Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(19):5883. https://doi.org/10.3390/jcm11195883
Chicago/Turabian StyleEtoom, Mohammad, Mohammad Alwardat, Alia Alghwiri, Francesco Lena, and Andrea Romigi. 2022. "Effects of Transcranial Direct Current Stimulation on Sleep in Athletes: A Protocol of a Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 19: 5883. https://doi.org/10.3390/jcm11195883
APA StyleEtoom, M., Alwardat, M., Alghwiri, A., Lena, F., & Romigi, A. (2022). Effects of Transcranial Direct Current Stimulation on Sleep in Athletes: A Protocol of a Randomized Controlled Trial. Journal of Clinical Medicine, 11(19), 5883. https://doi.org/10.3390/jcm11195883