
Long-Term Effects of Hospitalization for COVID-19 on Frailty and Quality of Life in Older Adults ≥80 Years

 , , ,
, , , 
Abstract
1. Impact Statement
1.1. Key Points
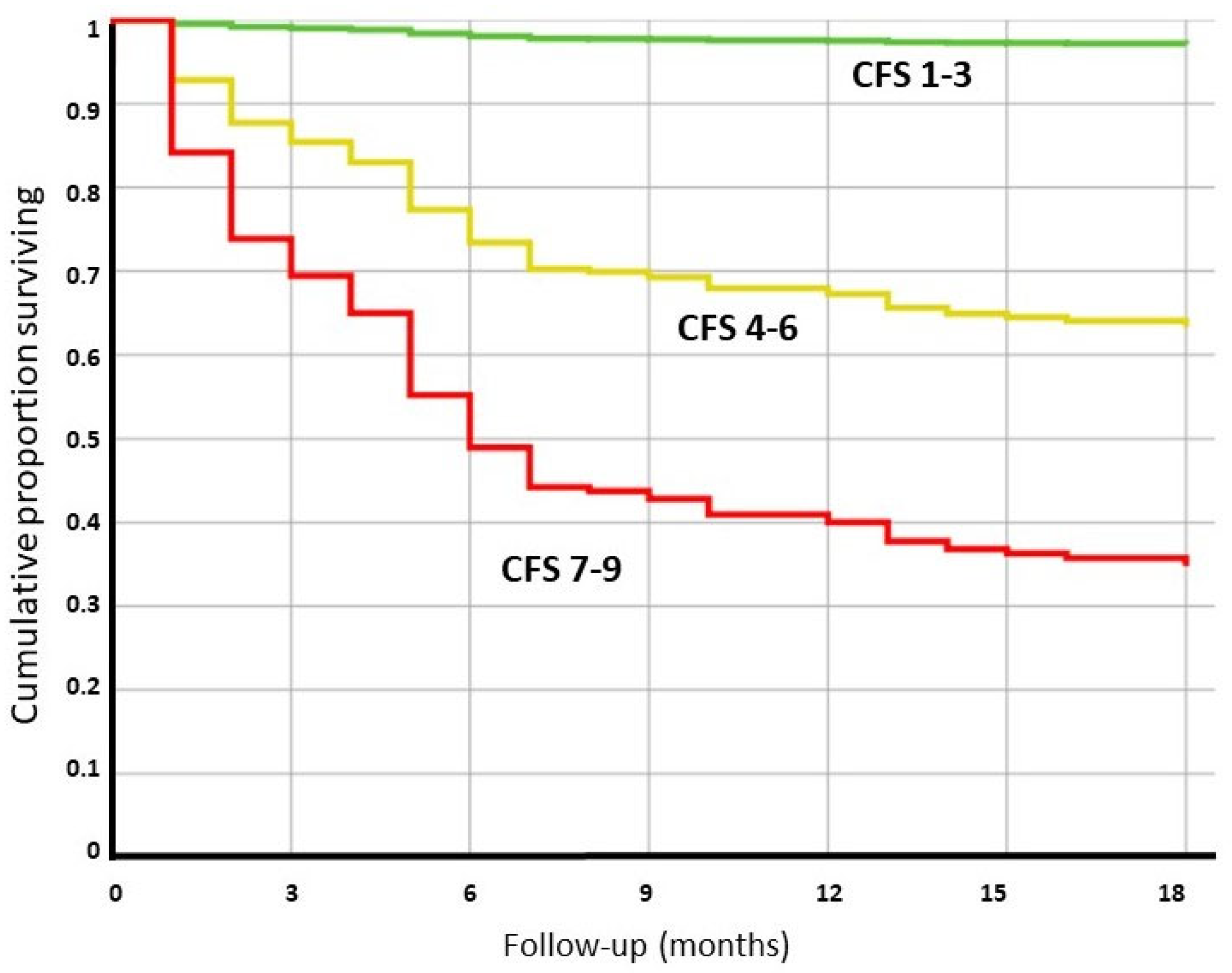
- In patients ≥80 years the stratification of frailty by the Clinical Frailty Scale (CFS) could predict the long-term survival after hospitalization for COVID-19.
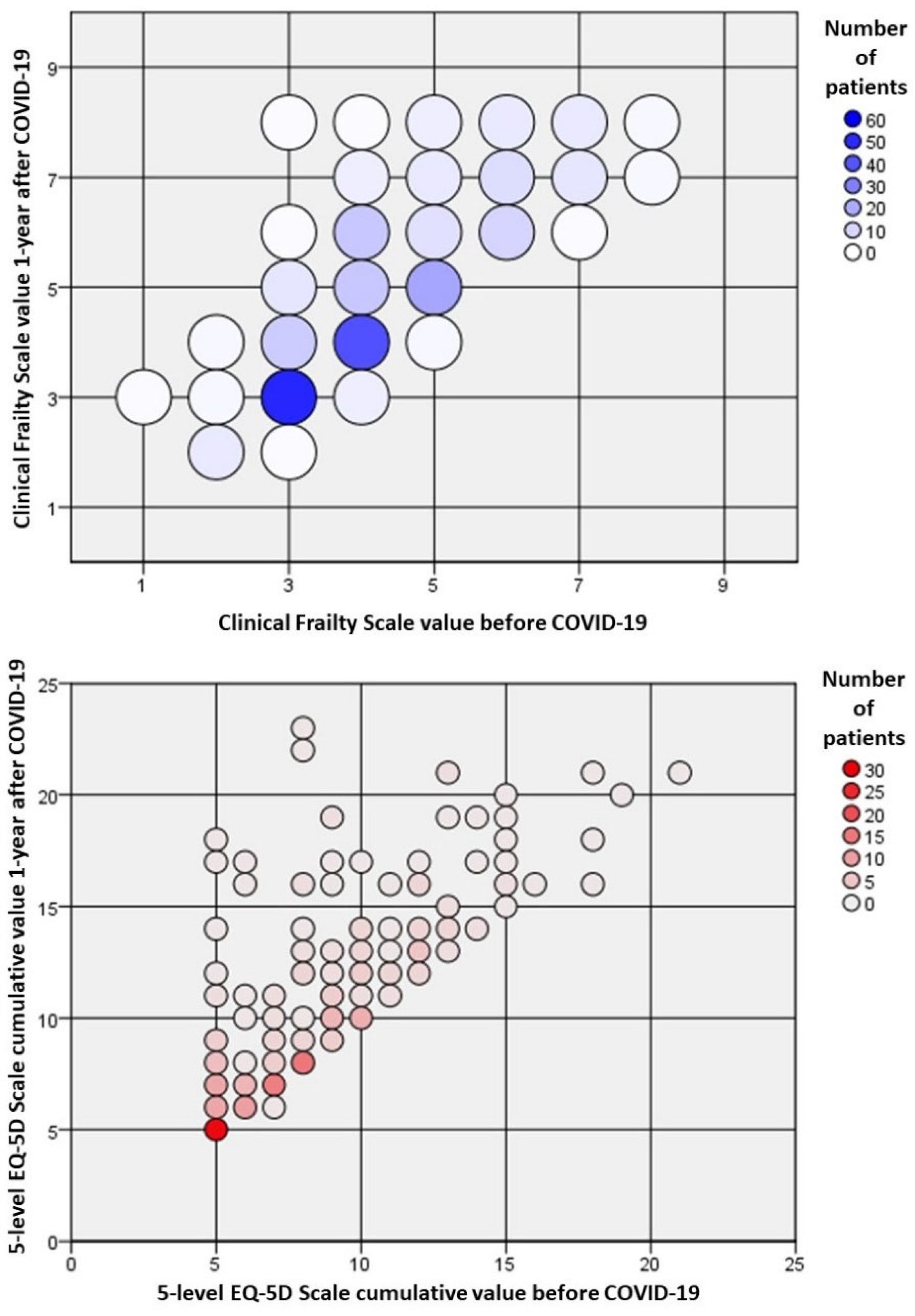
- A long-term reduction in the perceived QOL could be expected in the majority of older COVID-19 survivors.
1.2. Why This Matters
2. Introduction
3. Methods
3.1. Study Design
3.2. Study Variables
- Age and gender.
- Overall frailty as assessed by the Clinical Frailty Scale (CSF) [23]. According to the CSF scale, patients were further categorized as fit for CSF 1–3 (corresponding to fit and mild vulnerability), vulnerable for CSF 4–6 (corresponding to vulnerable or mild frail), and frail for CSF 7–9 (corresponding to moderate to severe frailty).
- Quality of life, assessed based on the five-level EUROQOL questionnaire (EQ-5D-5L) [24]. The EQ-5D-5L is a standardized measure of health status validated to provide a simple and reproducible generic measure of QOL. We considered, in our analysis, the crude sum of all the points (best (1) to worst (5)) assigned to the five domains ascertained: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.
- Dependency on activities of daily life (ADL) based on the clinical status before the SARS-CoV-2 infection.
- Delirium occurrence, assessed based on the Richmond Agitation–Sedation Scale [25] during the first 24 h of ED admission.
- Physiological parameters, including body temperature, heart rate, respiratory rate, blood pressure, Glasgow Coma Scale, and peripheral oxygen saturation. Based on these measures, the NEWS score was calculated for each patient [26].
- The need for mechanical ventilation (MV), defined as the need for MV including non-invasive techniques and high-flow oxygen therapy for more than 24 h.
- Clinical history and comorbidities, including cognitive impairment, assessed based on the Charlson Comorbidity Index (CCI) for each patient [27], calculated at the time of index ED access.
- A laboratory evaluation and a blood gas determination in the ED of all patients. The values considered in the study were the first values obtained at ED admission.
- The length of hospital stay of the index admission, calculated from ED access to death or hospital discharge. The overall follow-up was calculated from ED access to the last follow-up assessment or death.
- The number of persisting post-COVID symptoms, ascertained by a standard questionnaire, including fatigue, dyspnea, joint pain/myalgia, chest pain, cough/sputum, anosmia/dysgeusia, sore throat, and diarrhea. The symptoms were included in the count if present for at least 1 month and not present before hospitalization.
3.3. Study Endpoints
3.4. Statistical Analysis
3.5. Statement of Ethics
4. Results
4.1. Study Cohort and Baseline Characteristics
4.2. Factors Associated with Long-Term All-Cause Death after Hospital Discharge
4.3. Factors Associated with a Worsening in Frailty Status at One Year
4.4. Factors Associated with a Worsening in the QOL Status at One Year
5. Discussion
Study Limitations
6. Conclusions and Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet Lond. Engl. 2020, 395, 497–506. [Google Scholar] [CrossRef]
- WHO Coronavirus (COVID-19) Dashboard—WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 30 May 2022).
- Ministero Della Salute. Available online: https://www.salute.gov.it/portale/home.html (accessed on 30 May 2022).
- Hwang, J.; Ryu, H.-S.; Kim, H.A.; Hyun, M.; Lee, J.Y.; Yi, H.-A. Prognostic Factors of COVID-19 Infection in Elderly Patients: A Multicenter Study. J. Clin. Med. 2020, 9, 3932. [Google Scholar] [CrossRef] [PubMed]
- Becerra-Muñoz, V.M.; Núñez-Gil, I.J.; Eid, C.M.; Aguado, M.G.; Romero, R.; Huang, J.; Mulet, A.; Ugo, F.; Rametta, F.; Liebetrau, C.; et al. Clinical profile and predictors of in-hospital mortality among older patients hospitalised for COVID-19. Age Ageing 2021, 50, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Covino, M.; De Matteis, G.; Santoro, M.; Sabia, L.; Simeoni, B.; Candelli, M.; Ojetti, V.; Franceschi, F. Clinical characteristics and prognostic factors in COVID-19 patients aged ≥80 years. Geriatr. Gerontol. Int. 2020, 20, 704–708. [Google Scholar] [CrossRef]
- Covino, M.; De Matteis, G.; Burzo, M.L.; Russo, A.; Forte, E.; Carnicelli, A.; Piccioni, A.; Simeoni, B.; Gasbarrini, A.; Franceschi, F.; et al. Predicting In-Hospital Mortality in COVID-19 Older Patients with Specifically Developed Scores. J. Am. Geriatr. Soc. 2021, 69, 37–43. [Google Scholar] [CrossRef]
- Blagosklonny, M.V. From causes of aging to death from COVID-19. Aging 2020, 12, 10004–10021. [Google Scholar] [CrossRef]
- Zuccaro, V.; Celsa, C.; Sambo, M.; Battaglia, S.; Sacchi, P.; Biscarini, S.; Valsecchi, P.; Pieri, T.C.; Gallazzi, I.; Colaneri, M.; et al. Competing-risk analysis of coronavirus disease 2019 in-hospital mortality in a Northern Italian centre from SMAtteo COVID19 REgistry (SMACORE). Sci. Rep. 2021, 11, 1137. [Google Scholar] [CrossRef]
- Mueller, A.L.; McNamara, M.S.; Sinclair, D.A. Why does COVID-19 disproportionately affect older people? Aging 2020, 12, 9959–9981. [Google Scholar] [CrossRef]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated with Mortality Among Patients with COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Aliberti, M.J.R.; Szlejf, C.; Avelino-Silva, V.I.; Suemoto, C.K.; Apolinario, D.; Dias, M.B.; Garcez, F.B.; Trindade, C.B.; Amaral, J.R.d.G.; de Melo, L.R.; et al. COVID-19 is not over and age is not enough: Using frailty for prognostication in hospitalized patients. J. Am. Geriatr. Soc. 2021, 69, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Vermeiren, S.; Vella-Azzopardi, R.; Beckwée, D.; Habbig, A.; Scafoglieri, A.; Jansen, B.; Bautmans, I.; Gerontopole Brussels Study Group. Frailty and the Prediction of Negative Health Outcomes: A Meta-Analysis. J. Am. Med. Dir. Assoc. 2016, 17, 1163.e1–1163.e17. [Google Scholar] [CrossRef] [PubMed]
- Dumitrascu, F.; Branje, K.E.; Hladkowicz, E.S.; Lalu, M.; McIsaac, D.I. Association of frailty with outcomes in individuals with COVID-19: A living review and meta-analysis. J. Am. Geriatr. Soc. 2021, 69, 2419–2429. [Google Scholar] [CrossRef] [PubMed]
- Covino, M.; Russo, A.; Salini, S.; de Matteis, G.; Simeoni, B.; della Polla, D.; Sandroni, C.; Landi, F.; Gasbarrini, A.; Franceschi, F. Frailty Assessment in the Emergency Department for Risk Stratification of COVID-19 Patients Aged ≥80 Years. J. Am. Med. Dir. Assoc. 2021, 22, 1845–1852.e1. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.-M.; Jiao, J.; Cao, J.; Huo, X.-P.; Zhu, C.; Wu, X.-J.; Xie, X.-H. Frailty as a predictor of mortality among patients with COVID-19: A systematic review and meta-analysis. BMC Geriatr. 2021, 21, 186. [Google Scholar] [CrossRef] [PubMed]
- Aliberti, M.J.R.; Covinsky, K.E.; Garcez, F.B.; Smith, A.K.; Curiati, P.K.; Lee, S.J.; Dias, M.B.; Melo, V.J.D.; Rego-Júnior, O.F.d.; Richinho, V.d.; et al. A fuller picture of COVID-19 prognosis: The added value of vulnerability measures to predict mortality in hospitalised older adults. Age Ageing 2021, 50, 32–39. [Google Scholar] [CrossRef]
- Blomaard, L.C.; van der Linden, C.M.J.; van der Bol, J.M.; Jansen, S.W.M.; Polinder-Bos, H.A.; Willems, H.C.; Festen, J.; Barten, D.G.; Borgers, A.J.; Bos, J.C.; et al. Frailty is associated with in-hospital mortality in older hospitalised COVID-19 patients in the Netherlands: The COVID-OLD study. Age Ageing 2021, 50, 631–640. [Google Scholar] [CrossRef]
- Al Sayah, F.; Lahtinen, M.; Simon, R.; Higgins, B.; Ohinmaa, A.; Johnson, J.A. The impact of COVID-19 pandemic on health-related quality of life of adults visiting emergency departments and primary care settings in Alberta. Can. J. Public Health 2022, 113, 96–106. [Google Scholar] [CrossRef]
- Hodgson, C.L.; Higgins, A.M.; Bailey, M.J.; Mather, A.M.; Beach, L.; Bellomo, R.; Bissett, B.; Boden, I.J.; Bradley, S.; Burrell, A.; et al. The impact of COVID-19 critical illness on new disability, functional outcomes and return to work at 6 months: A prospective cohort study. Crit. Care 2021, 25, 382. [Google Scholar] [CrossRef]
- Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (2019-nCoV) Infection is Suspected: Interim Guidance, 28 January 2020. Available online: https://apps.who.int/iris/handle/10665/330893 (accessed on 30 May 2022).
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef]
- EuroQol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Sessler, C.N.; Gosnell, M.S.; Grap, M.J.; Brophy, G.M.; O’Neal, P.V.; Keane, K.A.; Tesoro, E.P.; Elswick, R.K. The Richmond Agitation-Sedation Scale: Validity and reliability in adult intensive care unit patients. Am. J. Respir. Crit. Care. Med. 2002, 166, 1338–1344. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.B.; Prytherch, D.R.; Meredith, P.; Schmidt, P.E.; Featherstone, P.I. The ability of the National Early Warning Score (NEWS) to discriminate patients at risk of early cardiac arrest, unanticipated intensive care unit admission, and death. Resuscitation 2013, 84, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Tavole di Mortalità. Available online: http://dati.istat.it/Index.aspx?DataSetCode=DCIS_MORTALITA1 (accessed on 30 May 2022).
- Carrillo-Garcia, P.; Garmendia-Prieto, B.; Cristofori, G.; Lozano-Montoya, I.; Gómez-Pavón, J. Health impact on the elderly survivors of COVID-19: Six months follow up. Rev. Esp. Geriatr. Gerontol. 2022, 57, 146–149. [Google Scholar] [CrossRef]
- Huang, L.; Yao, Q.; Gu, X.; Wang, Q.; Ren, L.; Wang, Y.; Hu, P.; Guo, L.; Liu, M.; Xu, J.; et al. 1-year outcomes in hospital survivors with COVID-19: A longitudinal cohort study. Lancet 2021, 398, 747–758. [Google Scholar] [CrossRef]
- Walle-Hansen, M.M.; Ranhoff, A.H.; Mellingsæter, M.; Wang-Hansen, M.S.; Myrstad, M. Health-related quality of life, functional decline, and long-term mortality in older patients following hospitalisation due to COVID-19. BMC Geriatr. 2021, 21, 199. [Google Scholar] [CrossRef]
- Betschart, M.; Rezek, S.; Unger, I.; Ott, N.; Beyer, S.; Böni, A.; Gisi, D.; Shanno, H.; Spruit, M.A.; Sieber, C. One year follow-up of physical performance and quality of life in patients surviving COVID-19: A prospective cohort study. Swiss. Med. Wkly. 2021, 151, w30072. [Google Scholar] [CrossRef]
- Vlake, J.H.; Wesselius, S.; van Genderen, M.E.; van Bommel, J.; Boxma-de Klerk, B.; Wils, E.-J. Psychological distress and health-related quality of life in patients after hospitalization during the COVID-19 pandemic: A single-center, observational study. PLoS ONE 2021, 16, e0255774. [Google Scholar] [CrossRef]
- Carenzo, L.; Protti, A.; Dalla Corte, F.; Aceto, R.; Iapichino, G.; Milani, A.; Santini, A.; Chiurazzi, C.; Ferrari, M.; Heffler, E.; et al. Short-term health-related quality of life, physical function and psychological consequences of severe COVID-19. Ann. Intensive Care 2021, 11, 91. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Putri, C.; Arisa, J.; Situmeang, R.F.V.; Kurniawan, A. Dementia and outcomes from coronavirus disease 2019 (COVID-19) pneumonia: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2020, 93, 104299. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Pan, L.; Ni, H. Impact of delirium on clinical outcome in critically ill patients: A meta-analysis. Gen. Hosp. Psychiatry 2012, 35, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Millett, E.R.; De Stavola, B.L.; Quint, J.K.; Smeeth, L.; Thomas, S.L. Risk factors for hospital admission in the 28 days following a community-acquired pneumonia diagnosis in older adults, and their contribution to increasing hospitalisation rates over time: A cohort study. BMJ Open 2015, 5, e008737. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Tang, W.; Sun, Y.; Jiang, C. Impact of frailty on 30-day and 1-year mortality in hospitalised elderly patients with community-acquired pneumonia: A prospective observational study. BMJ Open 2020, 10, e038370. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Wang, Y.; Chen, L.; Chen, X. Use of a frailty index based upon routine laboratory data to predict complication and mortality in older community-acquired pneumonia patients. Arch. Gerontol. Geriatr. 2022, 101, 104692. [Google Scholar] [CrossRef]
- Garcez, F.B.; Aliberti, M.J.R.; Poco, P.C.E.; Hiratsuka, M.; Takahashi, S.d.; Coelho, V.A.; Salotto, D.B.; Moreira, M.L.V.; Jacob-Filho, W.; Avelino-Silva, T.J. Delirium and Adverse Outcomes in Hospitalized Patients with COVID-19. J. Am. Geriatr. Soc. 2020, 68, 2440–2446. [Google Scholar] [CrossRef]
- Juma, S.; Taabazuing, M.-M.; Montero-Odasso, M. Clinical Frailty Scale in an Acute Medicine Unit: A Simple Tool That Predicts Length of Stay. Can. Geriatr. J. 2016, 19, 34–39. [Google Scholar] [CrossRef]
- Sablerolles, R.S.G.; Lafeber, M.; van Kempen, J.A.L.; van de Loo, B.P.A.; Boersma, E.; Rietdijk, W.J.R.; Polinder-Bos, H.A.; Mooijaart, S.P.; van der Kuy, H.; Versmissen, J.; et al. Association between Clinical Frailty Scale score and hospital mortality in adult patients with COVID-19 (COMET): An international, multicentre, retrospective, observational cohort study. Lancet Heal. Longev. 2021, 2, e163–e170. [Google Scholar] [CrossRef]
- Hussien, H.; Nastasa, A.; Apetrii, M.; Nistor, I.; Petrovic, M.; Covic, A. Different aspects of frailty and COVID-19: Points to consider in the current pandemic and future ones. BMC Geriatr. 2021, 21, 389. [Google Scholar] [CrossRef]
- Rotshild, V.; Hirsh-Raccah, B.; Miskin, I.; Muszkat, M.; Matok, I. Comparing the clinical efficacy of COVID-19 vaccines: A systematic review and network meta-analysis. Sci. Rep. 2021, 11, 22777. [Google Scholar] [CrossRef]
- Zheng, C.; Shao, W.; Chen, X.; Zhang, B.; Wang, G.; Zhang, W. Real-world effectiveness of COVID-19 vaccines: A literature review and meta-analysis. Int. J. Infect. Dis. 2022, 114, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Sandmann, F.G.; Tessier, E.; Lacy, J.; Kall, M.; van Leeuwen, E.; Charlett, A.; Eggo, R.M.; Dabrera, G.; Edmunds, W.J.; Ramsay, M.; et al. Long-term health-related quality of life in non-hospitalised COVID-19 cases with confirmed SARS-CoV-2 infection in England: Longitudinal analysis and cross-sectional comparison with controls. Clin. Infect. Dis. 2022, 75, e962–e973. [Google Scholar] [CrossRef] [PubMed]
- Bechmann, N.; Barthel, A.; Schedl, A.; Herzig, S.; Varga, Z.; Gebhard, C.; Mayr, M.; Hantel, C.; Beuschlein, F.; Wolfrum, C.; et al. Sexual dimorphism in COVID-19: Potential clinical and public health implications. Lancet Diabetes Endocrinol 2022, 10, 221–230. [Google Scholar] [CrossRef]
- Pelà, G.; Goldoni, M.; Solinas, E.; Cavalli, C.; Tagliaferri, S.; Ranzieri, S.; Frizzelli, A.; Marchi, L.; Mori, P.A.; Majori, M.; et al. Sex-Related Differences in Long-COVID-19 Syndrome. J. Womens Health 2022, 31, 620–630. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All cases N 368 | Survived N 236 | Deceased N 132 | p Value | Hazard Ratio [95% Confidence Interval] | ||
|---|---|---|---|---|---|---|
| Age | 85 [82, 89] | 84 [81, 87] | 87 [83, 91] | <0.01 | 1.08 [0.97, 1.21] | 0.16 |
| Age 80–85 years | 177 (48.1%) | 131 (74.0%) | 46 (26.0%) | |||
| Age 85–89 years | 111 (30.2%) | 73 (65.8%) | 38 (34.2%) | <0.01 | ||
| Age 90–94 years | 66 (17.9%) | 29 (44.9%) | 37 (56.1%) | |||
| Age ≥ 95 years | 14 (3.8%) | 3 (21.4%) | 11 (78.6%) | |||
| Expected Survival/1 year | 49.7% [49.7, 69.4] | 69.4% [49.7, 69.4] | 49.7% [29.6, 69.4] | <0.01 | 3.97 [0.25, 62.29] | 0.33 |
| Follow-up (months) | 15 [6, 18] | 17 [15, 18] | 4 [2, 6] | |||
| Sex (male) | 163 (44.3%) | 115 (70.6%) | 48 (29.4%) | 0.02 | 0.89 [0.62, 1.30] | 0.58 |
| Frailty and self-reported quality of life before COVID | ||||||
| Clinical Frailty Scale (CFS) | 5 [4, 6] | 5 [4, 6] | 6 [6, 7] | <0.01 | ||
| CFS 1–3 | 52 (14.4%) | 50 (96.2%) | 2 (3.8%) | Reference category | ||
| CFS 4–6 | 237 (64.4%) | 165 (69.6%) | 72 (30.4%) | <0.01 | 4.91 [1.16, 20.70] | 0.03 |
| CFS 7–9 | 79 (21.5%) | 21 (26.6%) | 58 (73.4%) | 6.61 [1.47, 29.80] | 0.01 | |
| Resident in nursing home | 92 (25.0%) | 42 (45.7%) | 50 (54.3%) | <0.01 | 1.06 [0.72, 1.55] | 0.77 |
| Autonomous in ADL (not) | 213 (57.9%) | 182 (85.4%) | 31 (14.6%) | <0.01 | 3.55 [2.20, 5.78] | <0.01 |
| EQ-5D-5L cumulative value | 8 [5, 10] | 9 [7, 13] | / | / | ||
| Clinical characteristics of the COVID-19 disease | ||||||
| PaO2/FiO2 at ED admission | 295 [233, 357] | 290 [233, 344] | 304 [228, 376] | 0.42 | ||
| NEWS at ED admission | 5 [4, 7] | 5 [4.75, 6.25] | 5 [4, 8] | 0.80 | ||
| NEWS > 5 at ED admission | 16 (4.3%) | 6 (37.5%) | 10 (62.5%) | 0.02 | 1.41 [0.73, 2.70] | 0.29 |
| Consolidation at chest X-ray | 304 (82.6%) | 201 (66.1%) | 103 (33.9%) | 0.08 | ||
| Delirium | 34 (9.2%) | 14 (41.2%) | 20 (58.5%) | <0.01 | 1.41 [0.83, 2.72] | 0.22 |
| Mechanical ventilation | 119 (32.3%) | 81 (68.1%) | 38 (31.9%) | 0.28 | ||
| Length of hospital stay (days) | 14.3 [8.5, 22.5] | 13.1 [8.1, 22.2] | 17.3 [10.0, 23.1] | 0.02 | 1.00 [0.97, 1.01] | 0.89 |
| Comorbidities | ||||||
| CCI | 5 [4, 6] | 5 [4, 6] | 5 [4, 6] | <0.01 | ||
| Comorbidities ≥ 3 | 127 (34.5%) | 69 (54.3%) | 58 (45.7%) | <0.01 | 1.08 [0.75, 1.55] | 0.68 |
| Hypertension | 162 (44.0%) | 120 (74.1%) | 42 (25.9%) | <0.01 | ||
| History of CAD | 54 (14.7%) | 37 (68.5%) | 17 (31.5%) | 0.47 | ||
| Congestive heart failure | 56 (15.2%) | 32 (57.1%) | 24 (42.9%) | 0.24 | ||
| Cerebrovascular disease | 13 (3.5%) | 6 (46.2%) | 7 (53.8%) | 0.17 | ||
| Dementia | 73 (19.8%) | 21 (53.8%) | 52 (46.2%) | <0.01 | ||
| COPD | 57 (15.5%) | 36 (63.2%) | 21 (36.8%) | 0.87 | ||
| Diabetes | 90 (24.5%) | 53 (58.9%) | 37 (41.1%) | 0.23 | ||
| Chronic kidney disease | 34 (9.2%) | 19 (55.9%) | 15 (44.1%) | 0.29 | ||
| Malignancy | 9 (2.4%) | 3 (33.3%) | 6 (66.7%) | 0.07 | ||
| Stable Frailty N 149 | Increased Frailty N 87 | p Value | Odds Ratio [95% Confidence Interval] | Multivariate p-Value | |
|---|---|---|---|---|---|
| Age | 84 [81, 86] | 84 [81, 88] | 0.06 | 1.04 [0.96, 1.12] | 0.35 |
| Age 80–85 years | 87 (66.2%) | 44 (6%) | |||
| Age 85–89 years | 44 (58.7%) | 31 (41.3%) | 0.37 | ||
| Age 90–94 years | 13 (54.2%) | 11 (45.8%) | |||
| Age ≥ 95 years | 5 (83.3%) | 1 (16.7%) | |||
| Expected Survival/1 year | 69.4% [49.7, 69.4] | 69.4% [49.7, 69.4] | 0.30 | ||
| Sex (male) | 81 (69.8%) | 34 (30.2%) | 0.02 | 0.61 [0.35, 1.07] | 0.10 |
| CFS pre-COVID | 4 [3, 5] | 4 [3, 5] | 0.12 | 0.96 [0.75, 1.24] | 0.77 |
| Resident in nursing home | 23 (54.8%) | 19 (45.2%) | 0.26 | ||
| Autonomous in ADL pre-COVID | 121 (65.0%) | 61 (35.0%) | 0.05 | 0.51 [0.17, 1.50] | 0.20 |
| EQ-5D-5L before COVID | 7 [5, 10] | 9 [6.75, 12] | <0.01 | 1.12 [1.01, 1.24] | 0.03 |
| Clinical characteristics of the COVID-19 disease | |||||
| PaO2/FiO2 at ED admission | 290 [259, 335] | 290 [213, 359] | 0.72 | ||
| NEWS at ED admission | 5 [4.5, 6] | 6 [4.5, 7] | 0.36 | ||
| NEWS > 5 at ED admission | 2 (33.3%) | 4 (66.7%) | 0.12 | ||
| Consolidation at chest X-ray | 125 (61.5%) | 76 (38.5%) | 0.47 | ||
| Delirium | 10 (71.4%) | 4 (28.6%) | 0.51 | ||
| Mechanical ventilation | 55 (67.9%) | 26 (32.1%) | 0.27 | ||
| Length of hospital stay (days) | 12.7 [7.4, 19.4] | 14.0 [8.4, 27.3] | 0.05 | ||
| Comorbidities | |||||
| CCI | 5 [4, 6] | 5 [4, 6] | 0.73 | ||
| Comorbidities ≥ 3 | 47 (68.1%) | 22 (31.9%) | 0.31 | ||
| Hypertension | 74 (61.7%) | 46 (38.3%) | 0.63 | ||
| History of CAD | 27 (72.9%) | 10 (27.1%) | 0.18 | ||
| Congestive heart failure | 20 (62.5%) | 12 (37.5%) | 0.94 | ||
| Cerebrovascular disease | 3 (50.0%) | 3 (50.0%) | 0.67 | ||
| Dementia | 15 (53.6%) | 13 (46.4%) | 0.26 | ||
| COPD | 19 (52.8%) | 17 (47.2%) | 0.16 | ||
| Diabetes | 34 (64.1%) | 19 (35.8%) | 0.86 | ||
| Chronic kidney disease | 12 (63.1%) | 7 (26.9%) | 0.99 | ||
| Malignancy | 1 (33.3%) | 2 (66.7%) | 0.28 | ||
| Outcomes at Follow-up | |||||
| Follow-up (months) | 16 [15, 18] | 17 [16, 18] | 0.06 | ||
| CFS post-COVID | 4 [3, 5] | 6 [6, 7] | <0.01 | ||
| EQ-5D-5L 1 year after COVID | 8 [6, 11] | 12 [9, 16] | <0.01 | ||
| Persistent COVID symptoms | 0 [0, 1] | 0.5 [0, 1] | 0.01 | ||
| Re-hospitalization <1 year | 31 (63.2%) | 18 (36.7%) | 0.97 | ||
| Stable QOL N 100 | Worsened QOL N 136 | p Value | Hazard Ratio [95% Confidence Interval] | Multivariate p Value | |
|---|---|---|---|---|---|
| Age | 83 [81, 86] | 84 [81, 87] | 0.11 | 1.01 [0.96, 1.06] | 0.65 |
| Age 80–85 years | 62 (47.7%) | 69 (52.3%) | |||
| Age 85–89 years | 24 (32.0%) | 51 (68.05%) | 0.03 | ||
| Age 90–94 years | 9 (37.5%) | 15 (62.5%) | |||
| Age ≥ 95 years | 5 (83.3%) | 1 (16.7%) | |||
| Expected Survival/1 year | 69.4% [49.7, 69.4] | 69.4% [49.7, 69.4] | 0.22 | ||
| Sex (male) | 60 (52.2%) | 55 (47.8%) | <0.01 | 0.69 [0.48, 0.98] | 0.04 |
| CFS pre-COVID | 4 [3, 5] | 5 [4, 5] | 0.03 | 1.01 [0.87, 1.17] | 0.896 |
| Resident in nursing home | 16 (38.1%) | 26 (71.9%) | 0.59 | ||
| Autonomous in ADL pre-COVID | 80 (43.9%) | 102 (56.1%) | 0.37 | ||
| EQ-5D-5L before COVID (cumulative) | 7 [5, 9] | 12 [8, 14] | 0.03 | 1.00 [0.95, 1.05] | 0.91 |
| Clinical characteristics of the COVID-19 disease | |||||
| PaO2/FiO2 at ED admission | 290 [233, 346] | 288 [226, 346] | 0.96 | ||
| NEWS at ED admission | 5 [4, 6] | 5.5 [5, 7] | 0.39 | ||
| NEWS > 5 at ED admission | 3 (50.0%) | 3 (50.0%) | 0.70 | ||
| Consolidation at chest X-ray | 80 (39.8%) | 121 (60.2%) | 0.05 | ||
| Delirium | 7 (50.0%) | 7 (50.0%) | 0.55 | ||
| Mechanical ventilation | 33 (40.7%) | 48 (59.3%) | 0.71 | ||
| Length of hospital stay (days) | 13.6 [9.0, 21.3] | 12.4 [7.26, 22.4] | 0.46 | ||
| Comorbidities | |||||
| CCI | 5 [4, 6] | 5 [4, 6] | 0.78 | ||
| Comorbidities ≥ 3 | 32 (45.7%) | 38 (54.3%) | 0.43 | ||
| Hypertension | 46 (58.3%) | 74 (61.7%) | 0.20 | ||
| History of CAD | 20 (54.0%) | 17 (66.0%) | 0.12 | ||
| Congestive heart failure | 13 (40.6%) | 19 (59.4%) | 0.83 | ||
| Cerebrovascular disease | 3 (50.0%) | 3 (50.0%) | 0.70 | ||
| Dementia | 11 (39.3%) | 17 (60.7%) | 0.72 | ||
| COPD | 15 (41.7%) | 21 (58.3%) | 0.93 | ||
| Diabetes | 21 (39.6%) | 32 (60.4%) | 0.64 | ||
| Chronic kidney disease | 8 (42.1%) | 11 (57.9%) | 0.98 | ||
| Malignancy | 0 | 3 (2.2%) | 0.26 | ||
| Outcomes at Follow-up | |||||
| Total follow-up (months) | 17 [15, 18.7] | 17 [15, 18] | 0.13 | ||
| CFS 1-year after COVID | 4 [3, 5] | 5 [4, 7] | <0.01 | ||
| EQ-5D-5L 1-year after COVID | 8 [6, 11] | 12 [9, 16] | <0.01 | ||
| Persistent COVID symptoms | 0 [0, 1] | 0 [0, 1] | <0.01 | ||
| Re-hospitalization <1 year | 14 (40.0%) | 35 (60.0%) | 0.05 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Covino, M.; Russo, A.; Salini, S.; De Matteis, G.; Simeoni, B.; Pirone, F.; Massaro, C.; Recupero, C.; Landi, F.; Gasbarrini, A.; et al. Long-Term Effects of Hospitalization for COVID-19 on Frailty and Quality of Life in Older Adults ≥80 Years. J. Clin. Med. 2022, 11, 5787. https://doi.org/10.3390/jcm11195787
Covino M, Russo A, Salini S, De Matteis G, Simeoni B, Pirone F, Massaro C, Recupero C, Landi F, Gasbarrini A, et al. Long-Term Effects of Hospitalization for COVID-19 on Frailty and Quality of Life in Older Adults ≥80 Years. Journal of Clinical Medicine. 2022; 11(19):5787. https://doi.org/10.3390/jcm11195787
Chicago/Turabian StyleCovino, Marcello, Andrea Russo, Sara Salini, Giuseppe De Matteis, Benedetta Simeoni, Flavia Pirone, Claudia Massaro, Carla Recupero, Francesco Landi, Antonio Gasbarrini, and et al. 2022. "Long-Term Effects of Hospitalization for COVID-19 on Frailty and Quality of Life in Older Adults ≥80 Years" Journal of Clinical Medicine 11, no. 19: 5787. https://doi.org/10.3390/jcm11195787
APA StyleCovino, M., Russo, A., Salini, S., De Matteis, G., Simeoni, B., Pirone, F., Massaro, C., Recupero, C., Landi, F., Gasbarrini, A., & Franceschi, F. (2022). Long-Term Effects of Hospitalization for COVID-19 on Frailty and Quality of Life in Older Adults ≥80 Years. Journal of Clinical Medicine, 11(19), 5787. https://doi.org/10.3390/jcm11195787