
Simple Application and Adherence to Gout Guidelines Enables Disease Control: An Observational Study in French Referral Centres

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Baseline and Follow-Up Visits
2.3. Statistical Analysis
3. Results
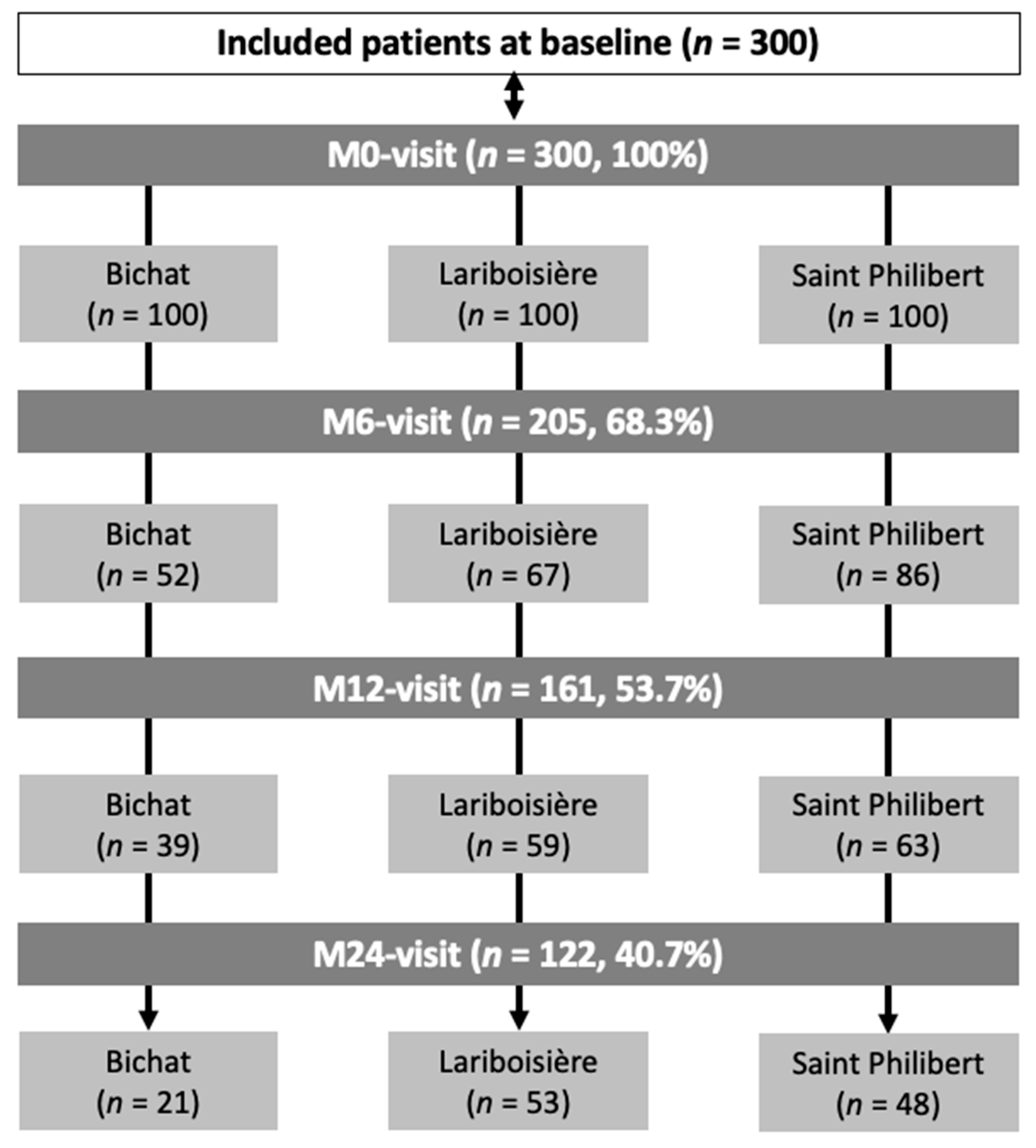
3.1. Study Population
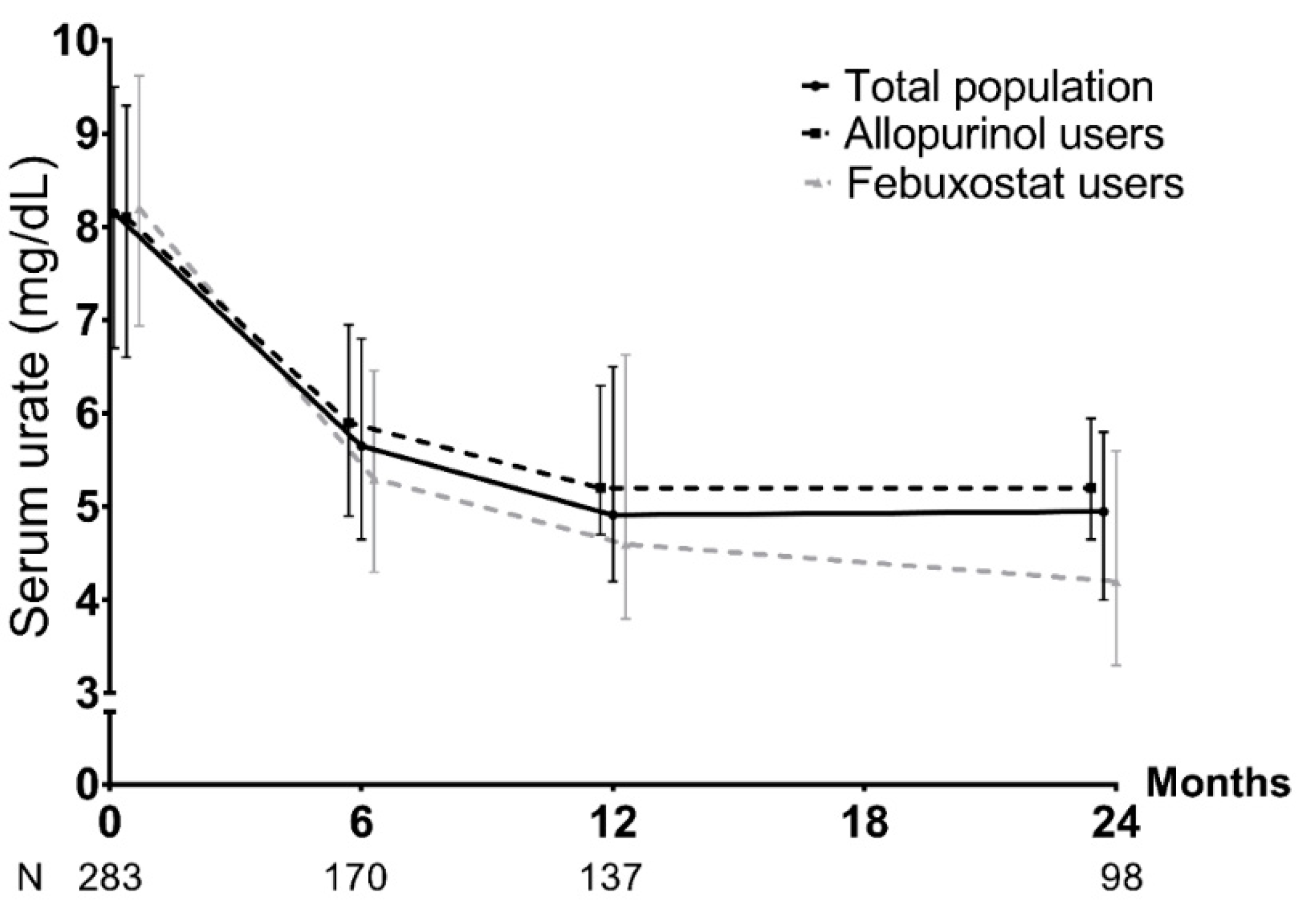
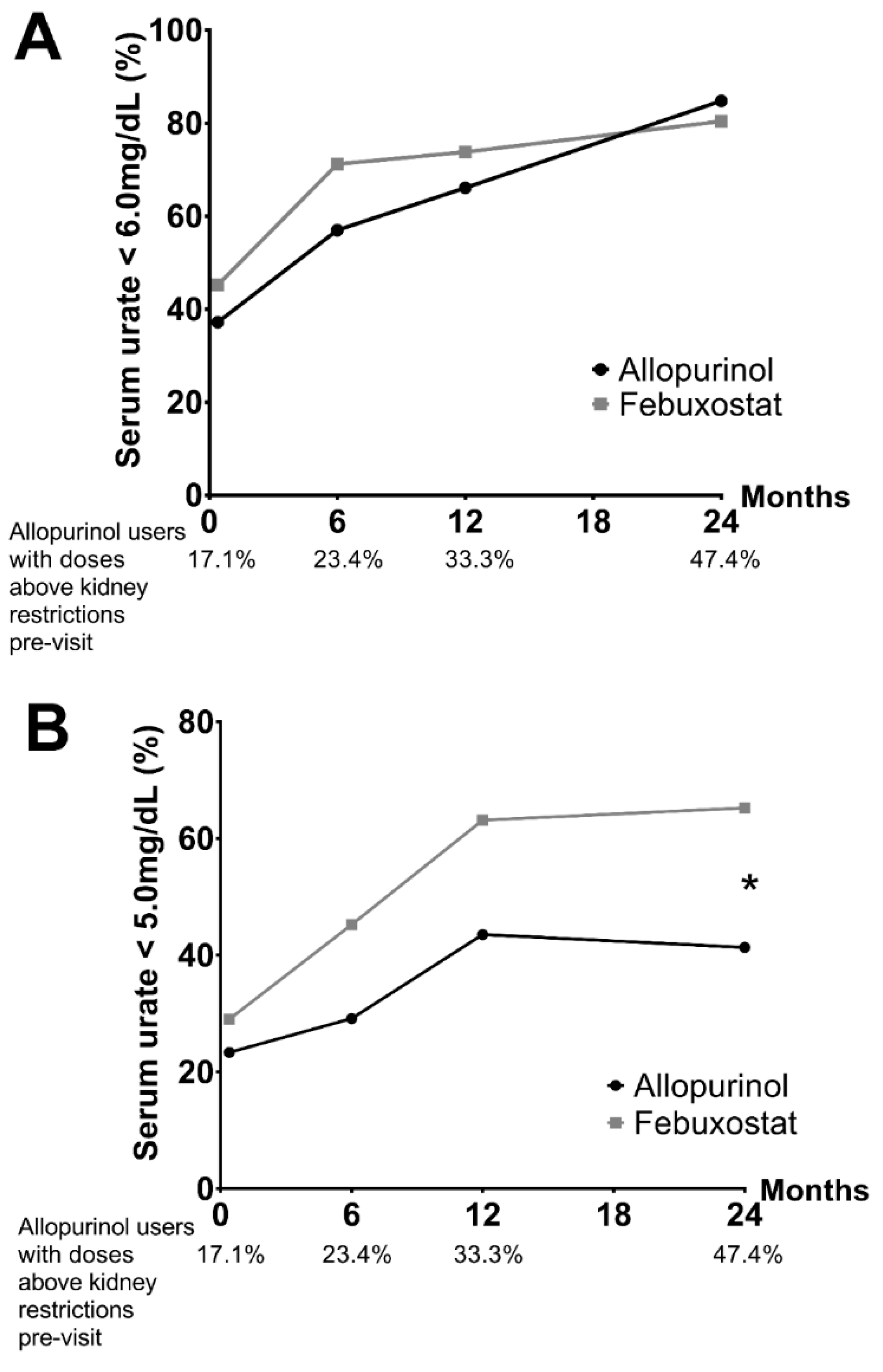
3.2. ULT Management
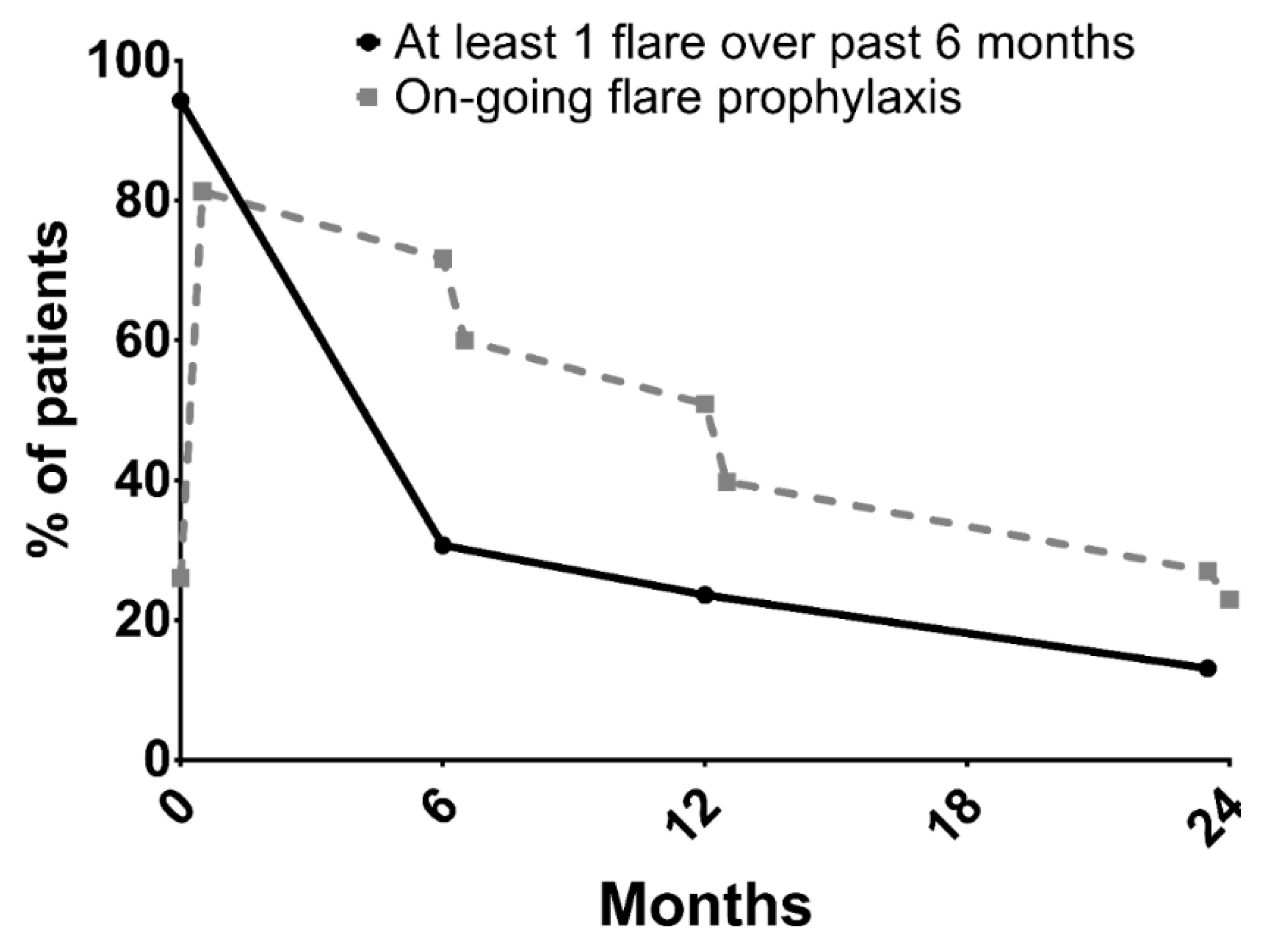
3.3. Flare Management
3.4. Predictive Factors of Reaching the Targeted Serum-Urate Levels
3.5. Factors Predictive of Being Lost to Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lioté, F.; Lancrenon, S.; Lanz, S.; Guggenbuhl, P.; Lambert, C.; Saraux, A.; Chiarelli, P.; Delva, C.; Aubert, J.P.; Ea, H.K. GOSPEL 1: Design and patient characteristics (n = 1003). Jt. Bone Spine 2012, 79, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Doherty, M.; Jansen, T.L.; Nuki, G.; Pascual, E.; Perez-Ruiz, F.; Punzi, L.; So, A.K.; Bardin, T. Gout: Why is this curable disease so seldom cured? Ann. Rheum. Dis. 2012, 71, 1765–1770. [Google Scholar] [CrossRef] [PubMed]
- Pascart, T.; Latourte, A.; Flipo, R.-M.; Chalès, G.; Coblentz-Baumann, L.; Cohen-Solal, A.; Ea, H.K.; Grichy, J.; Letavernier, E.; Lioté, F.; et al. 2020 recommendations from the French Society of Rheumatology for the management of gout: Urate-lowering therapy. Jt. Bone Spine 2020, 87, 395–404. [Google Scholar] [CrossRef]
- Richette, P.; Bardin, T. Gout. Lancet 2010, 375, 318–328. [Google Scholar] [CrossRef]
- Maravic, M.; Ea, H.-K. Hospital burden of gout, pseudogout and other crystal arthropathies in France. Jt. Bone Spine 2015, 82, 326–329. [Google Scholar] [CrossRef] [PubMed]
- Fields, T.R. The Challenges of Approaching and Managing Gout. Rheum. Dis. Clin. N. Am. 2019, 45, 145–157. [Google Scholar] [CrossRef]
- Pittman, J.R. Diagnosis and Management of Gout. Am. Fam. Physician 1999, 59, 1799–1806. [Google Scholar] [PubMed]
- Doherty, M.; Jenkins, W.; Richardson, H.; Sarmanova, A.; Abhishek, A.; Ashton, D.; Barclay, C.; Doherty, S.; Duley, L.; Hatton, R.; et al. Efficacy and cost-effectiveness of nurse-led care involving education and engagement of patients and a treat-to-target urate-lowering strategy versus usual care for gout: A randomised controlled trial. Lancet 2018, 392, 1403–1412. [Google Scholar] [CrossRef] [PubMed]
- Pascart, T.; Lioté, F. Gout: State of the art after a decade of developments. Rheumatology 2019, 58, 27–44. [Google Scholar] [CrossRef] [PubMed]
- Borghi, C.; Perez-Ruiz, F. Urate lowering therapies in the treatment of gout: A systematic review and meta-analysis. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 983–992. [Google Scholar] [PubMed]
- Scuiller, A.; Pascart, T.; Bernard, A.; Oehler, E. La maladie goutteuse. Rev. Médecine Interne 2020, 41, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Richette, P.; Doherty, M.; Pascual, E.; Barskova, V.; Becce, F.; Castañeda-Sanabria, J.; Coyfish, M.; Guillo, S.; Jansen, T.L.; Janssens, H.; et al. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann. Rheum. Dis. 2017, 76, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Latourte, A.; Pascart, T.; Flipo, R.-M.; Chalès, G.; Coblentz-Baumann, L.; Cohen-Solal, A.; Ea, H.-K.; Grichy, J.; Letavernier, E.; Lioté, F.; et al. 2020—Recommandations de la Société française de rhumatologie pour la prise en charge de la goutte: Traitement des crises de goutte. Rev. Rhum. 2020, 87, 324–331. [Google Scholar] [CrossRef]
- Hui, M.; Carr, A.; Cameron, S.; Davenport, G.; Doherty, M.; Forrester, H.; Jenkins, W.; Jordan, K.M.; Mallen, C.D.; McDonald, T.M.; et al. The British Society for Rheumatology Guideline for the Management of Gout. Rheumatology 2017, 56, e1–e20. [Google Scholar] [CrossRef]
- Voshaar, M.A.H.O.; Bardin, T.; van de Laar, M.A.F.J. The Human and Economic Burden of Difficult-to-Treat Gouty Arthritis. Jt. Bone Spine 2015, 82, eS2–eS8. [Google Scholar] [CrossRef]
- Pascart, T.; Norberciak, L.; Ea, H.-K.; Graf, S.; Guggenbuhl, P.; Lioté, F. Difficult-to-treat gout flares: Eligibility for interleukin-1 inhibition in private practice is uncommon according to current EMA approval. Rheumatology 2019, 58, 2181–2187. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Willett, W.; Curhan, G. Fructose-Rich Beverages and Risk of Gout in Women. JAMA 2010, 304, 2270. [Google Scholar] [CrossRef]
- Richette, P.; Flipo, R.N.; Patrikos, D.K. Characteristics and management of gout patients in Europe: Data from a large cohort of patients. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 630–639. [Google Scholar]
- Harrold, L.R.; Mazor, K.M.; Negron, A.; Ogarek, J.; Firneno, C.; Yood, R.A. Primary care providers’ knowledge, beliefs and treatment practices for gout: Results of a physician questionnaire. Rheumatology 2013, 52, 1623–1629. [Google Scholar] [CrossRef][Green Version]
- Bardin, T.; Richette, P. FAST: New look at the febuxostat safety profile. Lancet 2020, 396, 1704–1705. [Google Scholar] [CrossRef]
- Stamp, L.K.; Barclay, M.L. How to prevent allopurinol hypersensitivity reactions? Rheumatology 2018, 57, i35–i41. [Google Scholar] [CrossRef] [PubMed]
- Stamp, L.K.; Chapman, P.T.; Barclay, M.L.; Horne, A.; Frampton, C.; Tan, P.; Dalbeth, N. A randomised controlled trial of the efficacy and safety of allopurinol dose escalation to achieve target serum urate in people with gout. Ann. Rheum. Dis. 2017, 76, 1522–1528. [Google Scholar] [CrossRef] [PubMed]
- Ottaviani, S.; Moltó, A.; Ea, H.-K.; Neveu, S.; Gill, G.; Brunier, L.; Palazzo, E.; Meyer, O.; Richette, P.; Bardin, T.; et al. Efficacy of anakinra in gouty arthritis: A retrospective study of 40 cases. Arthritis Res. Ther. 2013, 15, R123. [Google Scholar] [CrossRef] [PubMed]
- Saag, K.G.; Khanna, P.P.; Keenan, R.T.; Ohlman, S.; Osterling Koskinen, L.; Sparve, E.; Åkerblad, A.C.; Wikén, M.; So, A.; Pillinger, M.H.; et al. A Randomized, Phase II Study Evaluating the Efficacy and Safety of Anakinra in the Treatment of Gout Flares. Arthritis Rheumatol. 2021, 73, 1533–1542. [Google Scholar] [CrossRef]
- Janssen, C.A.; Oude Voshaar, M.A.H.; Vonkeman, H.E.; Jansen, T.L.T.A.; Janssen, M.; Kok, M.R.; Radovits, B.; van Durme, C.; Baan, H.; van de Laar, M.A.F.J. Anakinra for the treatment of acute gout flares: A randomized, double-blind, placebo-controlled, active-comparator, non-inferiority trial. Rheumatology 2019, 58, 1344–1352. [Google Scholar] [CrossRef] [PubMed]
- te Kampe, R.; Boonen, A.; Jansen, T.L.; Elling, J.M.; Flendrie, M.; van Eijk-Hustings, Y.; Janssen, M.; van Durme, C.; de Vries, H. Development and usability of a web-based patient-tailored tool to support adherence to urate-lowering therapy in gout. BMC Med. Inf. Decis. Mak. 2022, 22, 95. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Missing Values (n) | |
|---|---|---|
| Centre | 0 | |
| Saint Philibert | 100 (33.3%) | |
| Bichat | 100 (33.3%) | |
| Lariboisière | 100 (33.3%) | |
| Male | 243 (81%) | 0 |
| Age at inclusion (years) | 62.2 ± 15.2 | 0 |
| Body-mass index (kg/m2) | 27.9 ± 4.9 | 53 |
| Ethnicity | 9 | |
| Caucasian | 163 (56%) | |
| North African | 49 (16.8%) | |
| Sub Saharan African | 48 (16.5%) | |
| Others | 31 (10.7%) | |
| Socio-economic status | 38 | |
| Managers | 14 (5.3%) | |
| Academic professions | 39 (14.9%) | |
| Workers, farmers | 35 (13.4%) | |
| Unemployed | 13 (5%) | |
| Home keeper, retired, or disabled | 161 (61.5%) | |
| Beverage intake | 1 | |
| No beverage consumption | 194 (64.9%) | |
| Current alcoholic intoxication a | 55 (18.4%) | |
| Former alcoholic intoxication | 26 (8.7%) | |
| Current excessive sweetened-beverage intake b | 7 (2.3%) | |
| Former excessive sweetened-beverage intake | 3 (1%) | |
| Current alcoholic intoxication and excessive sweetened- beverage intake | 13 (4.3%) | |
| Former alcoholic intoxication and excessive sweetened- beverage intake | 1 (0.3%) | |
| Smoking status | 1 | |
| No | 190 (63.5%) | |
| Current smoker | 41 (13.7%) | |
| Former smoker | 68 (22.7%) | |
| Diet high in purine and/or fructose | 116 (47%) | 53 |
| Practice of regular physical activity | 31 (12.6%) | 53 |
| Rheumatologic and non-rheumatologic comorbidities | ||
| Osteoarthritis | 72 (24%) | 1 |
| Diabetes mellitus | 84 (28.1%) | 1 |
| High blood pressure | 181 (60.5%) | 1 |
| History of major cardiovascular-event history (stroke, myocardial infarction, lower-limb arteriopathy) | 67 (22.3%) | 1 |
| Congestive heart failure | 38 (12.7%) | 1 |
| Dyslipidaemia | 100 (33.4%) | 1 |
| Liver disease | 11 (3.7%) | 1 |
| Obesity (body-mass index > 30 kg/m2) | 74 (30%) | 53 |
| Family history of c | 0 | |
| Gout (first or second degree) | 55 (18.3%) | |
| Renal colic (first or second degree) | 5 (1.7%) | |
| Hyperuricaemia (first or second degree) | 2 (0.7%) | |
| Background treatments for comorbidities | ||
| ≥2 hyper-uricaemic treatments d | 126 (42.1%) | 1 |
| ≥2 hypo-uricaemic treatments e | 78 (26.1%) | 1 |
| Kidney-failure treatment: dialysis, transplant | 4 (1.3%) | 1 |
| Gout duration (years) | 5.8 ± 8.6 | 14 |
| Number of flares in the 6 months before baseline | 1 [1; 2] | 18 |
| At least one gout complication at baseline | 229 (76.3%) | 0 |
| If gout complication, type c | 0 | |
| Ultrasound or subcutaneous tophi | 144 (62.9%) | |
| Kidney stones on imaging and/or renal colic | 35 (15.3%) | |
| Chronic kidney disease (CKD 3 and above) | 128 (55.9%) | |
| Gouty arthropathy | 58 (25.3%) | |
| On-going urate-lowering therapy (ULT) | 81 (27%) | 0 |
| If on-going ULT, name | 0 | |
| Allopurinol | 45 (55.6%) | |
| Febuxostat | 34 (42%) | |
| Benzobromarone, Probenecid | 2 (2.4%) | |
| Lesinurad | 0 (0%) | |
| Rasburicase, Pegloticase | 0 (0%) | |
| Bitherapy | 0 (0%) | |
| Serum-urate level (mg/dL) | 8.2 ± 2.4 | 17 |
| First visit context Outpatient referral In-care hospitalisation | 190 (63.3%) 110 (36.7%) | 0 |
| Patient specifically referred to expert centre | 178 (59.3%) | 0 |
| If specifically referred, reason | ||
| From primary care for treatment initiation | 9 (5.1%) | |
| From another hospital department | 140 (78.7%) | |
| Non-control at submaximal ULT dose in primary care | 8 (4.5%) | |
| Non-control at a maximal dose of ULT in primary care | 5 (2.8%) | |
| Non-control with non-referred management | 1 (0.6%) | |
| For initial hospital prescription | 1 (0.6%) | |
| Already follow in the expert centre for another reason | 9 (5.1%) | |
| From primary care, for diagnosis re-evaluation | 2 (1.1%) | |
| From primary care, for re-evaluation because of tolerance difficulties to standard ULT | 1 (0.6%) | |
| For personal convenience | 2 (1.1%) | |
| Mean ± SD, median [Q1; Q3], n (%). | ||
| Univariate OR (95% CI) | Multivariate OR (95% CI) | |
|---|---|---|
| Gout duration (years) | 0.996 (0.95–1.04) | - |
| No ULT at baseline | 1.38 (0.69–2.77) | - |
Alcohol/sweetened-beverage consumption
| - 0.69 (0.21–2.29) 1.12 (0.52–2.39) | - - - |
Ethnicity
| - 0.81 (0.31–2.12) 0.38 (0.12–1.15) a 0.36 (0.11–1.17) | - - - - |
| Body-mass index at baseline (kg/m2) | 0.995 (0.93–1.07) | - |
| High blood pressure | 1.47 (0.74–2.95) | - |
| Major cardiovascular event | 0.99 (0.46–2.12) | - |
| Diabetes mellitus | 1.24 (0.58–2.64) | - |
| Congestive heart failure | 0.77 (0.26–2.32) | - |
| Dyslipidaemia | 1.13 (0.55–2.31) | - |
| Hepatopathy | 0.39 (0.07–2.05) | - |
| Number of gout complications at baseline | 1.09 (0.77–1.55) | - |
| Ultrasound/subcutaneous tophi | 2.63 (1.20–5.74) b | 3.00 (0.99–9.08) |
| Double contour sign identified with joint ultrasound | 0.68 (0.32–1.48) | - |
| DECT MSU deposits at baseline | 0.73 (0.22–2.43) | - |
| Age at gout onset (per year) | 1.03 (1.01–1.06) b | 1.04 (1.00–1.08) |
| Age at baseline (per year) | 1.03 (1.01–1.06) b | - |
| Good compliance to ULT prior to visit: | 35.36 (5.46–229.08) d | - |
ULT:
| - 9.74 (3.87–24.53) d | - 7.49 (2.17–25.9) c |
| Hyperuricaemic therapy added to the patient’s background treatment since last visit | 0.78 (0.24–2.58) | - |
| Hyperuricaemic therapy removed from the patient’s background treatment since last visit | 0.29 (0.07–1.10) a | 0.18 (0.027–1.22) |
| ULT switch at previous visit | 0.83 (0.17–4.02) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jauffret, C.; Ottaviani, S.; Latourte, A.; Ea, H.-K.; Graf, S.; Lioté, F.; Bardin, T.; Richette, P.; Pascart, T. Simple Application and Adherence to Gout Guidelines Enables Disease Control: An Observational Study in French Referral Centres. J. Clin. Med. 2022, 11, 5742. https://doi.org/10.3390/jcm11195742
Jauffret C, Ottaviani S, Latourte A, Ea H-K, Graf S, Lioté F, Bardin T, Richette P, Pascart T. Simple Application and Adherence to Gout Guidelines Enables Disease Control: An Observational Study in French Referral Centres. Journal of Clinical Medicine. 2022; 11(19):5742. https://doi.org/10.3390/jcm11195742
Chicago/Turabian StyleJauffret, Charlotte, Sébastien Ottaviani, Augustin Latourte, Hang-Korng Ea, Sahara Graf, Frédéric Lioté, Thomas Bardin, Pascal Richette, and Tristan Pascart. 2022. "Simple Application and Adherence to Gout Guidelines Enables Disease Control: An Observational Study in French Referral Centres" Journal of Clinical Medicine 11, no. 19: 5742. https://doi.org/10.3390/jcm11195742
APA StyleJauffret, C., Ottaviani, S., Latourte, A., Ea, H.-K., Graf, S., Lioté, F., Bardin, T., Richette, P., & Pascart, T. (2022). Simple Application and Adherence to Gout Guidelines Enables Disease Control: An Observational Study in French Referral Centres. Journal of Clinical Medicine, 11(19), 5742. https://doi.org/10.3390/jcm11195742