
IgG Glycosylation Profiling of Peripheral Artery Diseases with Lectin Microarray


Abstract
:1. Introduction
2. Methods
2.1. Patients and Samples
2.2. Lectin Microarray Analysis
2.3. Lectin Blot Verification
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
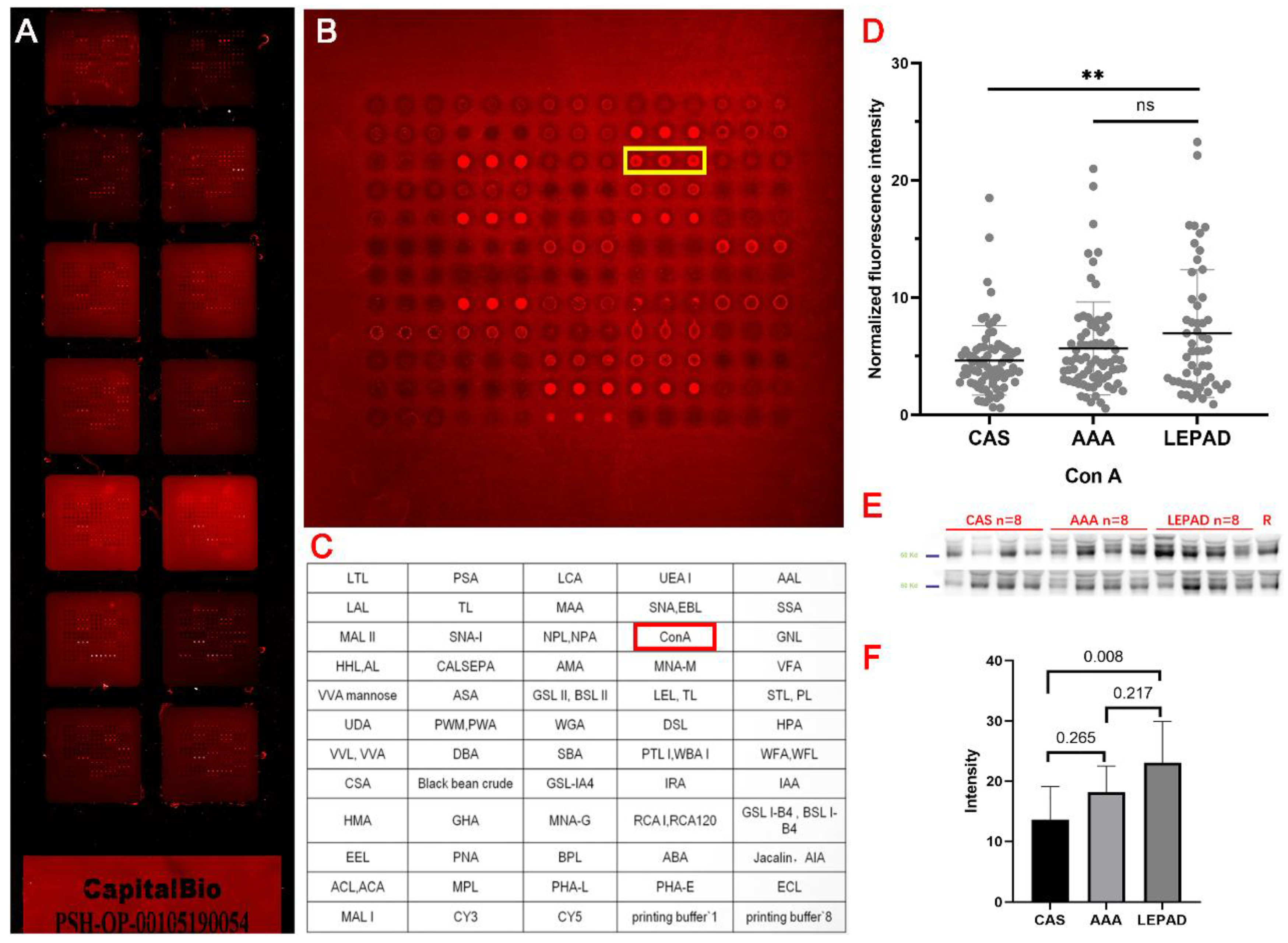
3.2. Lectin Microarray Results
3.3. Lectin Blot Analysis for LEPAD Patients
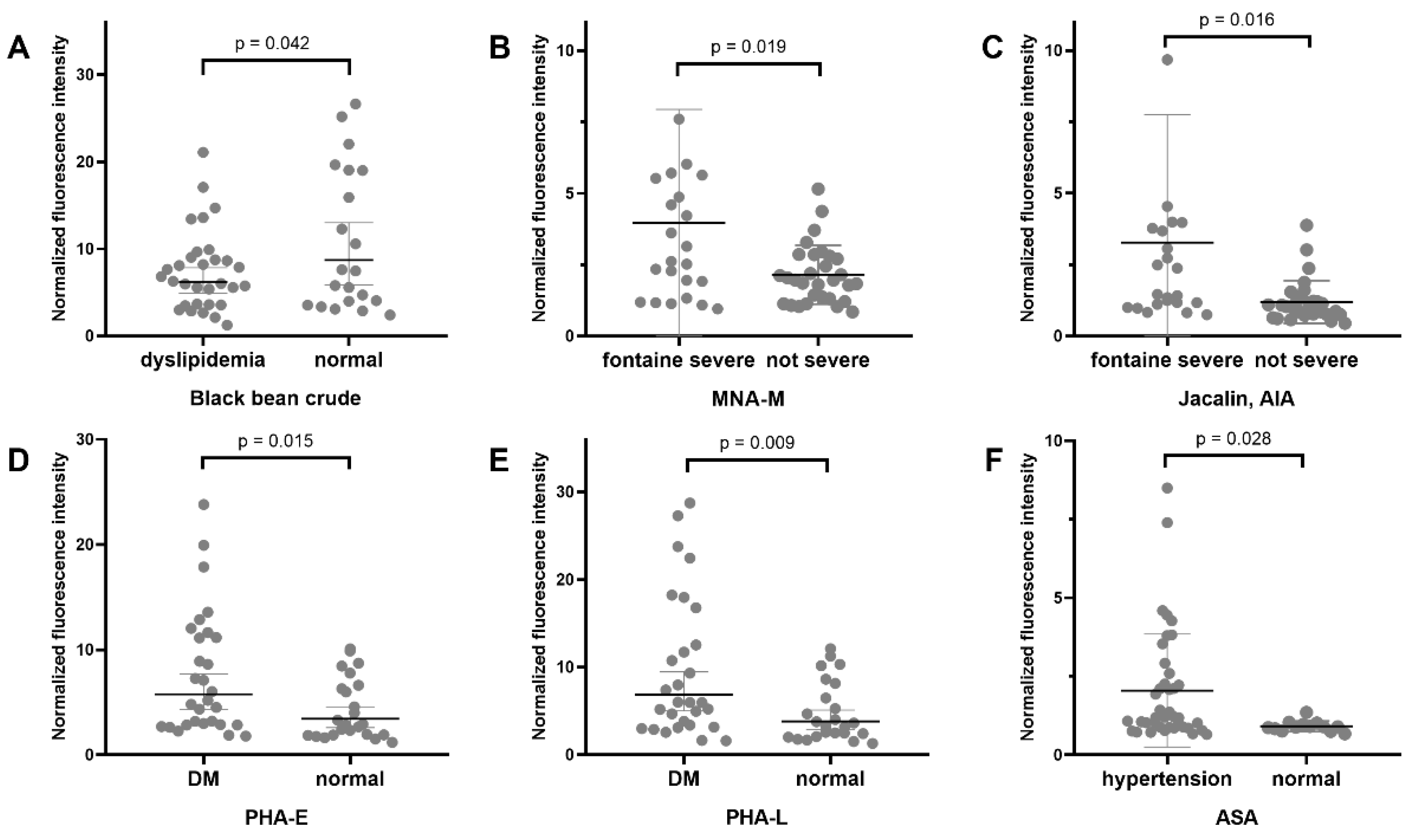
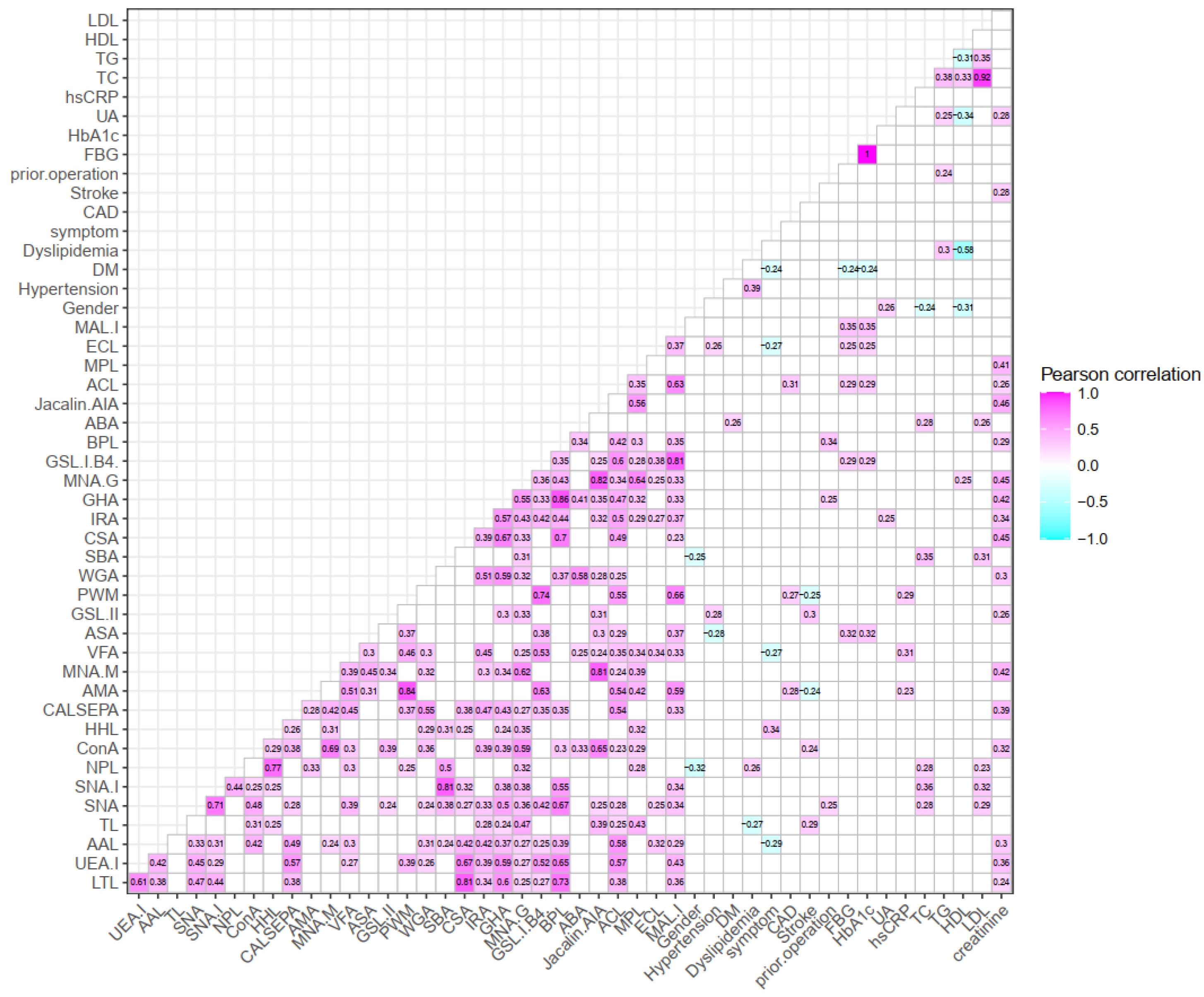
3.4. Clinical Relevance of Selective Lectins
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frank, U.; Nikol, S.; Belch, J.J.; Boc, V.; Brodmann, M.; Carpentier, P.H.; Chraim, A.; Canning, C.; Dimakakos, E.; Gottsäter, A.; et al. ESVM Guideline on peripheral arterial disease. Vasa 2019, 48 (Suppl. S102), 1–79. [Google Scholar] [CrossRef] [PubMed]
- Fowkes, F.G.R.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.A.; Williams, L.J.; Mensah, G.A.; et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef]
- Aday, A.W.; Matsushita, K. Epidemiology of Peripheral Artery Disease and Polyvascular Disease. Circ. Res. 2021, 128, 1818–1832. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.; Czerny, M.; de Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arter-ies Endorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar]
- Krist, A.H.; Davidson, K.W.; Mangione, C.M.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Donahue, K.; Doubeni, C.A.; Epling, J.W., Jr.; Kubik, M.; et al. Screening for Asymptomatic Carotid Artery Stenosis: US Preventive Services Task Force Recommendation Statement. Jama 2021, 325, 476–481. [Google Scholar]
- Hazarika, S.; Annex, B.H. Biomarkers and Genetics in Peripheral Artery Disease. Clin. Chem. 2017, 63, 236–244. [Google Scholar] [CrossRef]
- Saenz-Pipaon, G.; Martinez-Aguilar, E.; Orbe, J.; González Miqueo, A.; Fernandez-Alonso, L.; Paramo, J.A.; Roncal, C. The Role of Circulating Biomarkers in Peripheral Arterial Disease. Int. J. Mol. Sci. 2021, 22, 3601. [Google Scholar] [CrossRef]
- Gisterå, A.; Hansson, G.K. The immunology of atherosclerosis. Nat. Rev. Nephrol. 2017, 13, 368–380. [Google Scholar] [CrossRef]
- Ruparelia, N.; Choudhury, R. Inflammation and atherosclerosis: What is on the horizon? Heart 2020, 106, 80–85. [Google Scholar] [CrossRef]
- Tsiantoulas, D.; Diehl, C.; Witztum, J.L.; Binder, C.J. B Cells and Humoral Immunity in Atherosclerosis. Circ. Res. 2014, 114, 1743–1756. [Google Scholar] [CrossRef]
- Di Liu, D.; Chu, X.; Wang, H.; Dong, J.; Ge, S.-Q.; Zhao, Z.-Y.; Peng, H.-L.; Sun, M.; Wu, L.-J.; Song, M.-S.; et al. The changes of immunoglobulin G N-glycosylation in blood lipids and dyslipidaemia. J. Transl. Med. 2018, 16, 235. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Gudelj, I.; Macdonald-Dunlop, E.; Mangino, M.; Zierer, J.; Bešić, E.; Joshi, P.K.; Trbojević-Akmačić, I.; Chowienczyk, P.J.; Spector, T.D.; et al. Glycosylation Profile of Immunoglobulin G Is Cross-Sectionally Associated with Cardiovascular Disease Risk Score and Subclinical Atherosclerosis in Two Independent Cohorts. Circ. Res. 2018, 122, 1555–1564. [Google Scholar] [CrossRef] [PubMed]
- Hirabayashi, J.; Yamada, M.; Kuno, A.; Tateno, H. Lectin microarrays: Concept, principle and applications. Chem. Soc. Rev. 2013, 42, 4443–4458. [Google Scholar] [CrossRef] [PubMed]
- Dang, K.; Zhang, W.; Jiang, S.; Lin, X.; Qian, A. Application of Lectin Microarrays for Biomarker Discovery. ChemistryOpen 2020, 9, 285–300. [Google Scholar] [CrossRef]
- Sun, Y.; Cheng, L.; Gu, Y.; Xin, A.; Wu, B.; Zhou, S.; Guo, S.; Liu, Y.; Diao, H.; Shi, H.; et al. A Human Lectin Microarray for Sperm Surface Glycosylation Analysis. Mol. Cell. Proteom. 2016, 15, 2839–2851. [Google Scholar] [CrossRef]
- Li, Y.; Zhao, C.; Zhao, K.; Yu, N.; Yu, Y.; Zhang, Y.; Song, Z.; Huang, Y.; Lu, G.; Gao, Y.; et al. Glycosylation of Anti-Thyroglobulin IgG1 and IgG4 Subclasses in Thyroid Diseases. Eur. Thyroid J. 2020, 10, 114–124. [Google Scholar] [CrossRef]
- Eichler, J. Protein glycosylation. Curr. Biol. 2019, 29, R229–R231. [Google Scholar] [CrossRef]
- Quast, I.; Peschke, B.; Lünemann, J.D. Regulation of antibody effector functions through IgG Fc N-glycosylation. Cell. Mol. Life Sci. 2017, 74, 837–847. [Google Scholar] [CrossRef]
- Plomp, R.; Dekkers, G.; Rombouts, Y.; Visser, R.; Koeleman, C.A.; Kammeijer, G.S.; Jansen, B.C.; Rispens, T.; Hensbergen, P.J.; Vidarsson, G.; et al. Hinge-Region O-Glycosylation of Human Immunoglobulin G3 (IgG3). Mol. Cell. Proteom. 2015, 14, 1373–1384. [Google Scholar] [CrossRef]
- Hirabayashi, J.; Kuno, A.; Tateno, H. Development and Applications of the Lectin Microarray. In SialoGlyco Chemistry and Biology II; Springer: Cham, Switzerland, 2014; Volume 367, pp. 105–124. [Google Scholar] [CrossRef]
- Quast, I.; Keller, C.W.; Maurer, M.A.; Giddens, J.P.; Tackenberg, B.; Wang, L.X.; Münz, C.; Nimmerjahn, F.; Dalakas, M.C.; Lünemann, J.D. Sialylation of IgG Fc domain impairs comple-ment-dependent cytotoxicity. J. Clin. Investig. 2015, 125, 4160–4170. [Google Scholar] [CrossRef]
- Vattepu, R.; Sneed, S.L.; Anthony, R.M. Sialylation as an Important Regulator of Antibody Function. Front. Immunol. 2022, 13, 818736. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Zhao, Z.; Wang, A.; Ge, S.; Wang, H.; Zhang, X.; Sun, Q.; Cao, W.; Sun, M.; Wu, L.; et al. Ischemic stroke is associated with the pro-inflammatory potential of N-glycosylated immunoglobulin G. J. Neuroinflamm. 2018, 15, 123. [Google Scholar] [CrossRef] [PubMed]
- Russell, A.; Adua, E.; Ugrina, I.; Laws, S.; Wang, W. Unravelling Immunoglobulin G Fc N-Glycosylation: A Dynamic Marker Po-tentiating Predictive, Preventive and Personalised Medicine. Int. J. Mol. Sci. 2018, 19, 390. [Google Scholar] [CrossRef]
- De Haan, N.; Falck, D.; Wuhrer, M. Monitoring of immunoglobulin N- and O-glycosylation in health and disease. Glycobiology 2020, 30, 226–240. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Li, S.; Tang, S.; Li, X.; Zhang, G.; Li, M.; Zeng, X.; Hu, C. Changes of Serum IgG Glycosylation Patterns in Primary Biliary Cholangitis Patients. Front. Immunol. 2021, 12, 669137. [Google Scholar] [CrossRef] [PubMed]
- Stümer, J.; Biermann, M.H.C.; Knopf, J.; Magorivska, I.; Kastbom, A.; Svärd, A.; Janko, C.; Bilyy, R.; Schett, G.; Sjöwall, C.; et al. Altered glycan accessibility on native immuno-globulin G complexes in early rheumatoid arthritis and its changes during therapy. Clin. Exp. Immunol. 2017, 189, 372–382. [Google Scholar] [CrossRef]
- Wu, Z.; Li, H.; Liu, D.; Tao, L.; Zhang, J.; Liang, B.; Liu, X.; Wang, X.; Li, X.; Wang, Y.; et al. IgG Glycosylation Profile and the Glycan Score Are Associated with Type 2 Diabetes in Independent Chinese Populations: A Case-Control Study. J. Diabetes Res. 2020, 2020, 5041346. [Google Scholar] [CrossRef]
- Lemmers, R.F.; Vilaj, M.; Urda, D.; Agakov, F.; Šimurina, M.; Klarić, L.; Rudan, I.; Campbell, H.; Hayward, C.; Wilson, J.F.; et al. IgG glycan patterns are associated with type 2 diabetes in independent European populations. Biochim. Biophys. Acta Gen. Subj. 2017, 1861, 2240–2249. [Google Scholar] [CrossRef]
- Celebi, S.; Berkalp, B.; Amasyali, B. The association between thrombotic and inflammatory biomarkers and lower-extremity pe-ripheral artery disease. Int. Wound J. 2020, 17, 1346–1355. [Google Scholar] [CrossRef]
- Sjöwall, C.; Zapf, J.; Von Löhneysen, S.; Magorivska, I.; Biermann, M.; Janko, C.; Winkler, S.; Bilyy, R.; Schett, G.; Herrmann, M.; et al. Altered glycosylation of complexed native IgG molecules is associated with disease activity of systemic lupus erythematosus. Lupus 2014, 24, 569–581. [Google Scholar] [CrossRef]
- Riesberg, L.A.; McDonald, T.L.; Wang, Y.; Chen, X.-M.; Holzmer, S.W.; Tracy, S.M.; Drescher, K.M. Creatinine downregulates TNF-α in macrophage and T cell lines. Cytokine 2018, 110, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Can, Y.; Kocayigit, I. Hematological biomarkers for predicting carotid artery vasospasm during carotid stenting. Arch. Med. Sci. Atheroscler. Dis. 2020, 5, E206–E211. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. (%) or Mean ± SD | LEPAD (n = 53) | CAS (n = 75) | AAA (n = 75) | HC (n = 100) |
|---|---|---|---|---|
| Male, n% | 44 (83) | 63 (84) | 61 (81.3) | 81 (81) |
| Age (years) | 68.7 ± 9.2 | 65.8 ± 7.9 | 69.9 ± 8.6 | 66.5 ± 6.8 |
| Hypertension, n% | 40 (75.5) | 51 (68) | 60 (80) | 59 (59) |
| Dyslipidemia, n% | 31 (58.5) | 37 (49.3) | 42 (56) | 48 (48) |
| Diabetes, n% | 29 (54.7) | 27 (36) | 10 (13.3) | 22 (22) |
| CAD, n% | 19 (35.8) | 19 (25.3) | 29 (38.7) | NA |
| Stroke, n% | 14 (26.4) | 14 (18.7) | 11 (14.7) | NA |
| Ever smoked, n% | 31 (58.5) | 32 (42.7) | 42 (56) | NA |
| Total glycerol (mmol/L) | 1.3 ± 0.7 | 1.2 ± 0.6 | 1.5 ± 0.8 | 1.5 ± 0.8 |
| LDL cholesterol (mmol/L) | 2.3 ± 0.9 | 2.0 ± 0.7 | 2.6 ± 1.0 | 3.0 ± 3.1 |
| HDL cholesterol (mmol/L) | 1.1 ± 0.4 | 1.1 ± 0.3 | 1.0 ± 0.2 | 1.4 ± 0.6 |
| Total cholesterol (mmol/L) | 3.9 ± 1.0 | 3.6 ± 0.9 | 4.2 ± 1.2 | 4.6 ± 1.1 |
| HCY (μmol/L) | 15.8 ± 4.7 | 15.5 ± 5.2 | 17.4 ± 8.2 | 14.4 ± 3.2 |
| hsCRP (mg/L) | 6.2 ± 14.9 | 4.5 ± 14.2 | 6.1 ± 19.3 | 1.6 ± 3.6 |
| Blood creatinine (μmol/L) | 84.8 ± 30.8 | 81.9 ± 26.5 | 89.2 ± 33.3 | 82.8 ± 21.4 |
| Blood uric acid (μmol/L) | 365.8 ± 115.1 | 360.2 ± 81.8 | 378.4 ± 80.9 | 353.6 ± 84.8 |
| FBG (mmol/L) | 6.4 ± 2.2 | 6.1 ± 1.4 | 5.4 ± 1.3 | 6.1 ± 1.7 |
| HbA1c, % | 6.8 ± 1.2 | 6.1 ± 1.4 | 6.1 ± 1.2 | 5.9 ± 0.9 |
| Medication, n% | ||||
| Statin | 43 (81.1) | 74 (98.7) | 36 (48) | NA |
| Antiplatelet | 42 (50.6) | 73 (97.3) | 56 (74.7) | NA |
| Antihypertensive | 42 (50.6) | 42 (56) | 37 (49.3) | NA |
| No. (%) | All (n = 53) | Hypertension (n = 40) | Dyslipidemia (n = 31) | Diabetes (n = 29) | p | |
|---|---|---|---|---|---|---|
| Prior lowerextremity operation | 24 (45.3) | 19 (47.5) | 14 (45.2) | 16 (55.2) | 0.837 | |
| Fontaine classification | ||||||
| Not severe | IIa | 9 (17) | 7 (17.5) | 3 (9.7) | 2 (6.9) | 0.492 |
| IIb | 21 (39.6) | 16 (40) | 13 (41.9) | 13 (44.8) | 0.979 | |
| all | 30 (56.6) | 23 (57.5) | 16 (51.6) | 15 (51.7) | 0.935 | |
| Severe | III | 10 (18.9) | 8 (20) | 7 (22.6) | 7 (24.1) | 0.955 |
| IV | 13 (24.5) | 9 (22.5) | 8 (25.8) | 7 (24.1) | 0.993 | |
| all | 23 (43.4) | 17 (42.5) | 15 (48.4) | 14 (48.3) | 0.935 | |
| Lectin | Preferred Sugar | Normalized Fluorescence Intensity (Mean ± SD) | Fold Change | ||||||
|---|---|---|---|---|---|---|---|---|---|
| LEPAD | CAS | AAA | HC | LEPAD/CAS | LEPAD/AAA | CAS/AAA | LEPAD/HC | ||
| SNA | Sialic acid | 3.21 ± 2.06 | 2.47 ± 1.45 | 3.34 ± 2.42 | 3.23 ± 3.21 | 1.301 * | 0.963 | 0.740 * | 0.996 |
| ConA | Mannose | 6.95 ± 5.43 | 4.64 ± 2.96 | 5.50 ± 3.77 | 5.97 ± 3.65 | 1.497 ** | 1.262 | 0.843 | 1.165 |
| PSA | Fucose | 3.62 ± 3.06 | 2.78 ± 1.39 | 2.99 ± 2.65 | 3.17 ± 1.76 | 1.302 * | 1.215 | 0.931 | 1.142 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, S.; Meng, J.; Xu, F.; Wang, Q.; Tian, X.; Li, M.; Zeng, X.; Hu, C.; Zheng, Y. IgG Glycosylation Profiling of Peripheral Artery Diseases with Lectin Microarray. J. Clin. Med. 2022, 11, 5727. https://doi.org/10.3390/jcm11195727
Li S, Meng J, Xu F, Wang Q, Tian X, Li M, Zeng X, Hu C, Zheng Y. IgG Glycosylation Profiling of Peripheral Artery Diseases with Lectin Microarray. Journal of Clinical Medicine. 2022; 11(19):5727. https://doi.org/10.3390/jcm11195727
Chicago/Turabian StyleLi, Siting, Jingjing Meng, Fang Xu, Qian Wang, Xinping Tian, Mengtao Li, Xiaofeng Zeng, Chaojun Hu, and Yuehong Zheng. 2022. "IgG Glycosylation Profiling of Peripheral Artery Diseases with Lectin Microarray" Journal of Clinical Medicine 11, no. 19: 5727. https://doi.org/10.3390/jcm11195727
APA StyleLi, S., Meng, J., Xu, F., Wang, Q., Tian, X., Li, M., Zeng, X., Hu, C., & Zheng, Y. (2022). IgG Glycosylation Profiling of Peripheral Artery Diseases with Lectin Microarray. Journal of Clinical Medicine, 11(19), 5727. https://doi.org/10.3390/jcm11195727