
Respiratory Subsets in Patients with Moderate to Severe Acute Respiratory Distress Syndrome for Early Prediction of Death †

 ,
,  , , , , , , , and add
Show full author list
, , , , , , , and add
Show full author list
Abstract
1. Introduction
2. Methods
2.1. Patient Population, Study Design, and Oversight
2.2. Data Collection and Outcomes
2.3. Statistical Analysis
3. Results
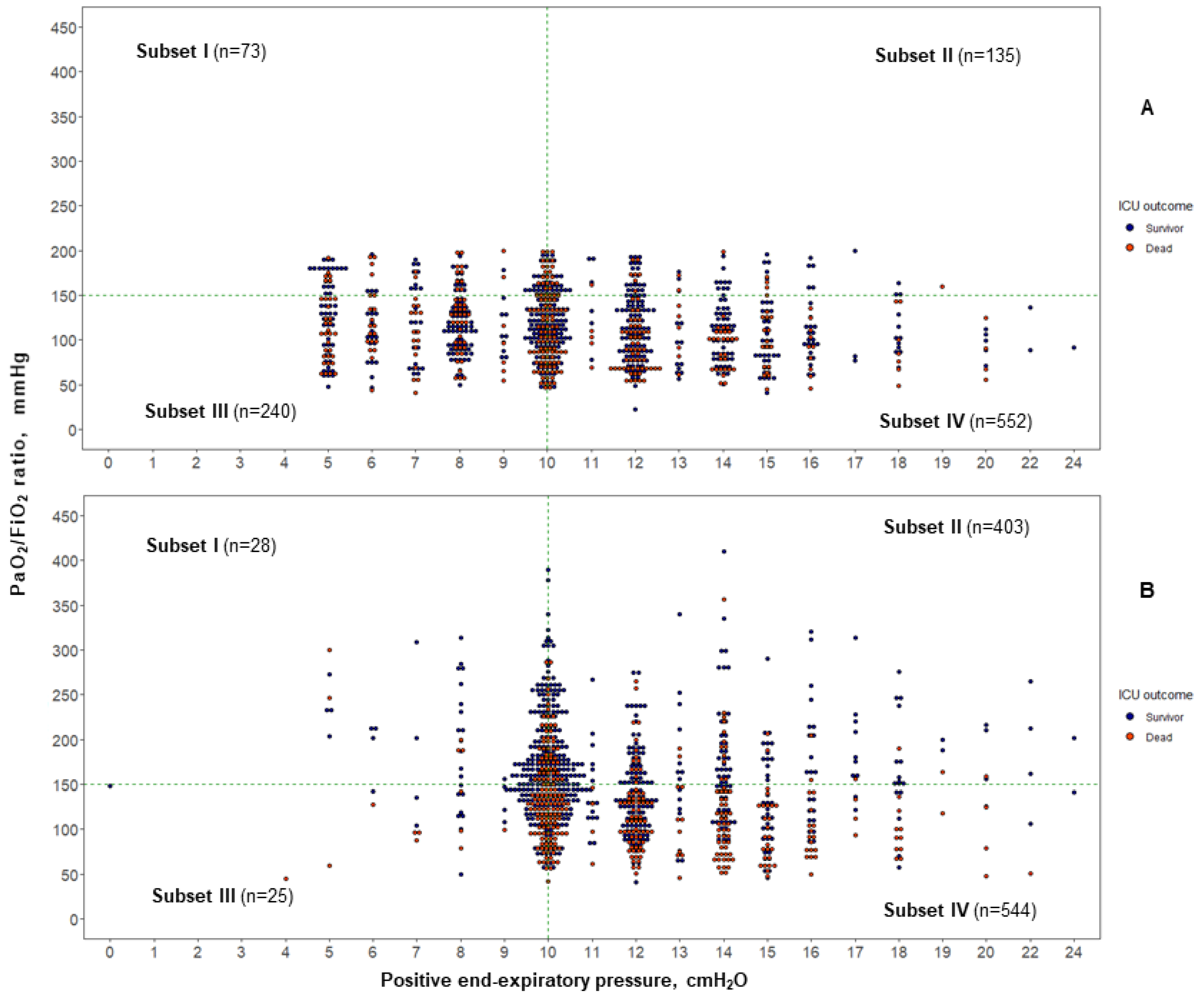
3.1. ARDS Subsets at Baseline
3.2. ARDS Subsets at 24 h after Moderate/Severe ARDS Diagnosis
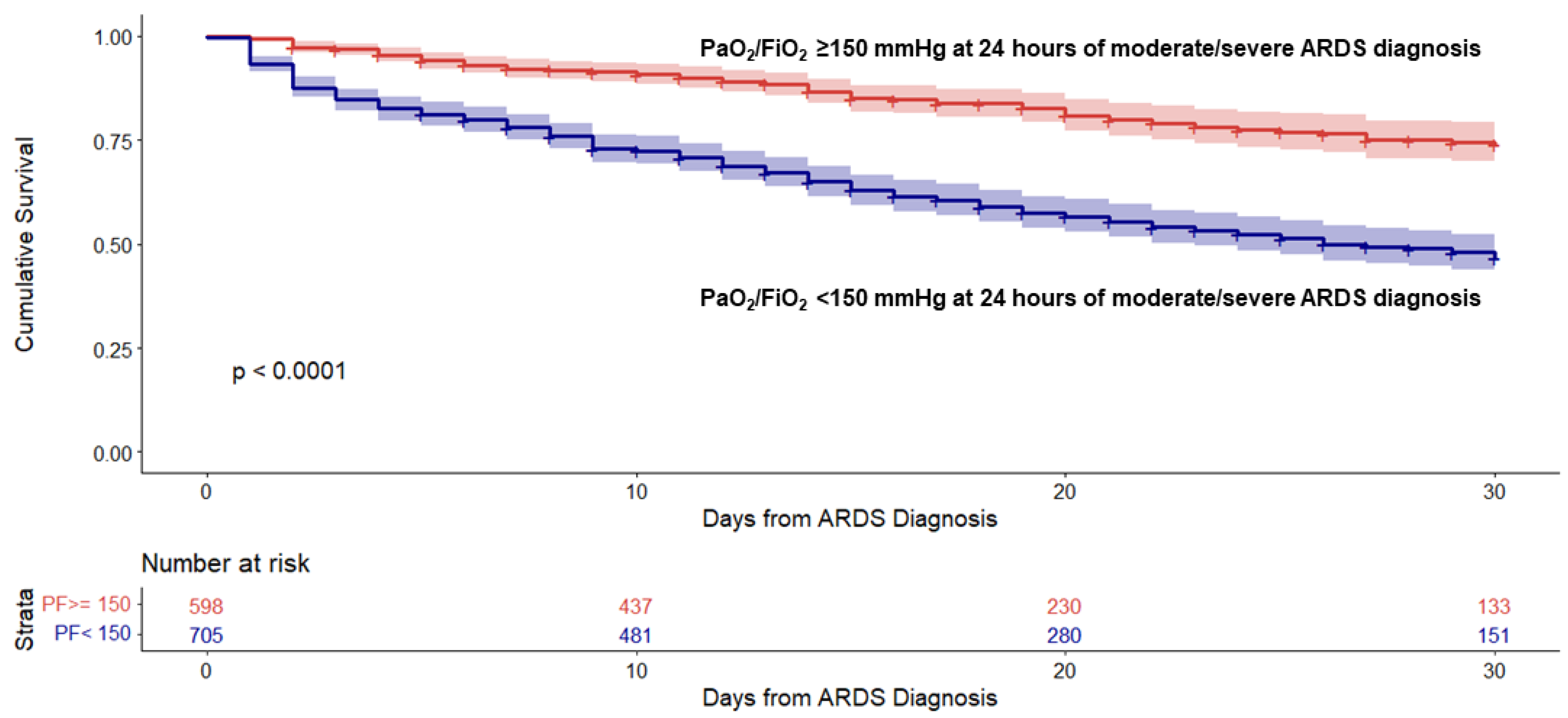
3.3. Probability of ICU Survival to Day 30
3.4. Additional Analysis with Different PaO2/FiO2 Cutoff Values
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
Appendix A. Members of the SIESTA Network Are Listed below
- Jesús Villar, Rosa L. Fernández, Cristina Fernández, Jesús M. González-Martin, Pedro Rodríguez-Suárez (Hospital Universitario Dr. Negrín, Las Palmas de Gran Canaria, Spain);
- Alfonso Ambrós, Rafael del Campo, Carmen Martín-Rodríguez, Ana Bueno-González, Carmen Hornos-López (Hospital General Universitario, Ciudad Real, Spain);
- Fernando Mosteiro, Ana M. Díaz-Lamas, Regina Arrojo, Lidia Pita-García (Complejo Hospitalario Universitario de La Coruña, La Coruña, Spain);
- Lorena Fernández, Jesús Sánchez-Ballesteros, Jesús Blanco, Arturo Muriel, Pablo Blanco-Schweizer, José Ángel de Ayala, César Aldecoa, Jesús Rico-Feijoo, Alba Pérez, Silvia Martín-Alfonso (Hospital Universitario Río Hortega, Valladolid, Spain);
- Domingo Martínez, Juan A. Soler, Ana M. del Saz-Ortiz, Luís A. Conesa-Cayuela (Hospital Universitario Virgen de Arrixaca, Murcia, Spain);
- Demetrio Carriedo, Ana M. Domínguez-Berrot, Francisco J. Díaz-Domínguez, Raúl I. González-Luengo (Complejo Hospitalario Universitario de León, León, Spain);
- Lucia Capilla (Hospital General Universitario Rafael Méndez, Lorca, Murcia, Spain);
- David Andaluz, Leonor Nogales, Laura Parra (Hospital Clínico Universitario, Valladolid, Spain);
- Elena González-Higueras, Rosario Solano, María J. Bruscas (Hospital Virgen de la Luz, Cuenca, Spain);
- Blanca Arocas, Marina Soro, Javier Belda, Andrea Gutiérrez, Ernesto Pastor, Gerardo Aguilar (Hospital Clínico Universitario, Valencia, Spain);
- Carlos Ferrando (Hospital Clinic, Barcelona, Spain);
- José M. Añón, Belén Civantos, Mónica Hernández (Hospital Universitario La Paz, Madrid, Spain);
- Raquel Montiel, Dácil Parrilla, Eduardo Peinado, Lina Pérez-Méndez (Hospital Universitario NS de Candelaria, Tenerife, Spain);
- Anxela Vidal, Denis Robaglia, César Pérez (Hospital Universitario Fundación Jiménez Díaz, Madrid, Spain);
- María del Mar Fernández (Hospital Universitario Mutua Terrassa, Terrassa, Barcelona, Spain);
- Eleuterio Merayo, Chanel Martínez-Jiménez, Ángeles de Celis-Álvarez (Hospital del Bierzo, Ponferrada, León, Spain);
- Juan M. Mora-Ordoñez, J. Francisco Martínez-Carmona, Álvaro Valverde-Monto, Victoria Olea-Jiménez (Hospital Regional Universitario de Málaga, Málaga, Spain);
- Concepción Tarancón, Silvia Cortés-Díaz (Hospital Virgen de la Concha, Zamora, Spain);
- Carmen Martín-Delgado (Hospital La Mancha Centro, Alcázar de San Juan, Ciudad Real, Spain);
- Francisca Prieto (Hospital Santa Bárbara, Puertollano, Ciudad Real, Spain);
- Isidro Prieto, Mario Chico, Darío Toral (Hospital Universitario 12 de Octubre, Madrid, Spain);
- Miguel A. Romera, Carlos Chamorro-Jambrina (Hospital Universitario Puerta de Hierro, Majadahonda, Madrid, Spain);
- Alec Tallet, Santiago Macías, Noelia Lázaro (Hospital General de Segovia, Segovia, Spain);
- Isabel Murcia, Ángel E. Pereyra (Hospital General Universitario de Albacete, Albacete, Spain);
- Francisco Alba, Ruth Corpas (Hospital NS del Prado, Talavera de la Reina, Toledo, Spain);
- David Pestaña, Pilar Cobeta, Adrián Mira (Hospital Universitario Ramón y Cajal, Madrid, Spain);
- Francisca Prieto (Hospital Santa Barbara, Puertollano, Ciudad Real, Spain);
- Lluis Blanch, Gemma Gomá, Gisela Pili (Corporació Sanitaria Parc Taulí, Sabadell, Barcelona, Spain);
- Antonio Santos-Bouza, Cristina Domínguez (Complejo Hospitalario Universitario de Santiago, Santiago de Compostela, La Coruña, Spain);
- Javier Collado, José I. Alonso (Hospital Río Carrión, Palencia, Spain);
- Alberto Indarte, María E. Perea (Hospital General Yagüe, Burgos, Spain);
- Ricardo Fernández, José I. Lozano (Hospital de Hellín, Albacete, Spain)
- Ewout W. Steyerberg (Department of Biomedical Data Sciences, Leiden University Medical Center, Leiden, The Netherlands);
- Robert M. Kacmarek (deceased), Lorenzo Berra (Massachussets General Hospital, Boston, Massachusetts, USA);
- Arthur S. Slutsky (Li Ka Shing Knowledge Institute, St. Michael’s Hospital, Toronto, Ontario, Canada).
References
- Villar, J. What is the acute respiratory distress syndrome? Respir. Care 2011, 56, 1539–1545. [Google Scholar] [CrossRef] [PubMed]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [PubMed]
- Villar, J.; Pérez-Méndez, L.; Kacmarek, R.M. The Berlin definition met our needs: No. Intensive Care Med. 2016, 42, 648–650. [Google Scholar] [CrossRef]
- Peng, J.M.; Qian, C.Y.; Yu, X.Y.; Zhao, M.Y.; Li, S.S.; Ma, X.C.; Kang, Y.; Zhou, F.C.; He, Z.H.; Qin, T.H.; et al. Does training improve diagnostic accuracy and inter-rater agreement in applying the Berlin radiographic definition of acute respiratory distress syndrome? A multicenter prospective study. Crit. Care 2017, 21, 12. [Google Scholar] [CrossRef] [PubMed]
- Fountain, S.; Assar, S.; Heise, C.; Curry, S.; Raschke, R.A. What’s in a chest radiograph? Inter-rater variability in determining acute respiratory distress syndrome. Am. J. Resp. Crit. Care Med. 2018, 197, A5063. [Google Scholar]
- Villar, J.; Slutsky, A.S. GOLDEN anniversary of the acute respiratory distress syndrome: Still much work to do! Curr. Opin. Crit. Care 2017, 23, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Blanco, J.; del Campo, R.; Andaluz-Ojeda, D.; Díaz-Domínguez, F.J.; Muriel, A.; Córcoles, V.; Suárez-Sipmann, F.; Tarancón, C.; González-Higueras, E.; et al. Assessment of PaO2/FiO2 for stratification of patients with moderate and severe acute respiratory distress syndrome. BMJ Open 2015, 5, 1006812. [Google Scholar] [CrossRef]
- Hernu, R.; Wallet, F.; Thiolliére, F.; Martin, O.; Richard, J.C.; Schmitt, Z.; Wallon, G.; Delannoy, B.; Rimmelé, T.; Démeret, C.; et al. An attempt to validate the modification of the American-European consensus definition of acute lung injury/acute respiratory distress syndrome by the Berlin definition in a university hospital. Intensive Care Med. 2013, 39, 2161–2170. [Google Scholar] [CrossRef]
- Villar, J.; Pérez-Méndez, L.; Blanco, J.; Añón, J.M.; Blanch, L.; Belda, J.; Santos-Souza, A.; Fernández, R.L.; Kacmarek, R.M.; Spanish Initiative for Epidemiology, Stratification, and Therapies for ARDS (SIESTA) Network. A universal definition of ARDS: The PaO2/FiO2 ratio under a standard ventilatory setting—A prospective, multicenter validation study. Intensive Care Med. 2013, 39, 583–592. [Google Scholar] [CrossRef]
- Huber, W.; Findeissen, M.; Lahmer, T.; Herner, A.; Rasch, S.; Mayr, U.; Hoppmann, P.; Jaitner, J.; Okrojek, R.; Brettner, F.; et al. Prediction of outcome in patients with ARDS: A prospective cohort study comparing ARDS-definitions and other ARDS-associated parameters, ratios and scores at intubation and over time. PLoS ONE 2020, 15, e0232720. [Google Scholar] [CrossRef]
- Phillips, C.R. The Berlin definition: Real change or the emperor’s new clothes? Crit. Care 2013, 17, 174. [Google Scholar] [CrossRef]
- Villar, J.; Pérez-Méndez, L.; López, J.; Belda, J.; Blanco, J.; Saralegui, I.; Suárez-Sipmann, F.; López, J.; Lubillo, S.; Kacmarek, R.M.; et al. An early PEEP/FiO2 trial identifies different degrees of lung injury in patients with acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2007, 176, 795–804. [Google Scholar] [CrossRef] [PubMed]
- Kamo, T.; Tasaka, S.; Susuki, T.; Asakura, T.; Susuki, S.; Yagi, K.; Namkoong, H.; Ishii, M.; Morisaki, H.; Betsuyaku, T. Prognostic values of the Berlin definition criteria, blood lactate levels, and fibroproliferative changes on high-resolution computed tomography in ARDS patients. BMC Pulm. Med. 2019, 19, 37. [Google Scholar] [CrossRef]
- Shapiro, B.A.; Cane, R.D.; Harrison, R.A. Positive end-expiratory pressure therapy in adults with special reference to acute lung injury: A review of the literature and suggested clinical correlations. Crit. Care Med. 1984, 12, 127–141. [Google Scholar] [CrossRef]
- Cove, M.E.; Pinsky, M.R.; Marini, J.J. Are we ready to think differently about setting PEEP? Crit. Care 2022, 26, 222. [Google Scholar] [CrossRef]
- Briel, M.; Meade, M.; Mercat, A.; Brower, R.G.; Talmor, D.; Walter, S.D.; Slutsky, A.S.; Pullenayegum, E.; Zhou, Q.; Cook, D.; et al. Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: Systematic review and meta-analysis. JAMA 2010, 303, 865–873. [Google Scholar] [CrossRef]
- Kang, M.; Kempker, J.A. Definitions, epidemiology, clinical risk factors, and health disparities in acute respiratory distress syndrome. Sem. Respir. Crit. Care Med. 2019, 40, 3–11. [Google Scholar] [CrossRef]
- Bone, R.C.; Maunder, R.; Slotman, G.; Silverman, H.; Hyers, T.M.; Kerstein, M.D.; Ursprung, J.J. Prostaglandin E1 Study Group. An early test of survival in patients with the adult respiratory distress syndrome. The PaO2/FiO2 ratio and its differential response to conventional therapy. Chest 1989, 96, 849–851. [Google Scholar] [CrossRef] [PubMed]
- Artigas, A.; Carlet, J.; LeGall, J.R.; Chastang, C.; Blanch, L.; Fernández, R. Clinical presentation, prognostic factors and outcome of ARDS in the European Collaborative Study (1985–1987). In Adult Respiratory Distress Syndrom; Zapol, W.M., Lemaire, F., Eds.; A preliminary report; Dekker: New York, NY, USA, 1991; pp. 37–64. [Google Scholar]
- Villar, J.; Pérez-Méndez, L.; Kacmarek, R.M. Current definitions of acute lung injury and the acute respiratory distress syndrome do not reflect their true severity and outcome. Intensive Care Med. 1999, 25, 930–935. [Google Scholar] [CrossRef] [PubMed]
- Papazian, L.; Forel, J.M.; Gacouin, A.; Penot-Ragon, C.; Perrin, G.; Loundou, A.; Jaber, S.; Arnal, J.M.; Perez, D.; Seghboyan, J.M.; et al. Neuromuscular blockers in early acute respiratory distress syndrome. N. Engl. J. Med. 2010, 363, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Guérin, C.; Reignier, J.; Richard, J.C.; Beuret, P.; Gacouin, A.; Boulain, T.; Clavel, M.; Chatellier, D.; Jaber, S.; Rosselli, S.; et al. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef] [PubMed]
- Maiolo, G.; Collino, F.; Vasques, F.; Rapetti, F.; Tonetti, T.; Romitti, F.; Cressoni, M.; Chiumello, D.; Moerer, O.; Herrmann, P.; et al. Reclassifying acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2018, 197, 1586–1595. [Google Scholar] [CrossRef] [PubMed]
- The National Heart, Lung, and Blood Institute Petal Clinical Trials Network; Moss, M.; Huang, D.; Brower, R.G.; Ferguson, N.D.; Ginde, A.A.; Gong, M.N.; Grissom, C.K.; Gundel, S.; Hayden, D.; et al. Early neuromuscular blockade in the acute respiratpry distress syndrome. N. Engl. J. Med. 2019, 380, 1997–2008. [Google Scholar] [PubMed]
- Villar, J.; Fernández, R.L.; Ambrós, A.; Parra, L.; Blanco, J.; Domínguez-Berrot, A.M.; Gutiérrez, J.M.; Blanch, L.; Añón, J.M.; Martín, C.; et al. A clinical classification of the acute respiratory distress syndrome for predicting outcome and guiding therapy. Crit. Care Med. 2015, 43, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Bos, L.D.; Cremer, O.L.; Ong, D.S.Y.; Caser, E.B.; Barbas, C.S.V.; Villar, J.; Kacmarek, R.M.; Schultz, M.J.; MARS Consortium. External validation confirms the legitimacy of a new clinical classification of ARDS for predicting outcome. Intensive Care Med. 2015, 41, 2004–2005. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Martínez, D.; Mosteiro, F.; Ambrós, A.; Añón, J.M.; Ferrando, C.; Soler, J.A.; Montiel, R.; Vidal, A.; Conesa-Cayuela, L.A.; et al. Stratification and Outcome of Acute Respiratory Distress Syndrome (STANDARDS) Network. Is overall mortality the right composite endpoint in clinical trials of acute respiratory distress syndrome? Crit. Care Med. 2018, 46, 892–899. [Google Scholar] [CrossRef]
- Villar, J.; Mora-Ordoñez, J.M.; Soler, J.A.; Mosteiro, F.; Vidal, A.; Ambrós, A.; Fernández, L.; Murcia, I.; Civantos, B.; Romera, M.A.; et al. The PANDORA study: Prevalence and outcome of acute hypoxemic respiratory failure in the pre-COVID era. Crit. Care Explor. 2022, 4, e0684. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; for the STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4(e296). [Google Scholar] [CrossRef]
- Vergouwe, Y.; Steyerberg, E.W.; Eijkemans, M.J.C.; Habbema, J.D.F. Substantial effective sample sizes were required for external validation studies of predictive logistic regression models. J. Clin. Epidemiol. 2005, 58, 475–483. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Vincent, J.L.; de Mendonça, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.M.; Sprung, C.L.; Colardyn, F.; Blecher, S. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: Results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Cri. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef] [PubMed]
- Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef]
- Fan, E.; Del Sorbo, L.; Goligher, E.C.; Hodgson, C.L.; Munshi, L.; Walkey, A.J.; Adhikari, N.K.J.; Amato, M.B.P.; Branson, R.; Brower, R.G.; et al. American Thoracic Society, European Society of Intensive Care Medicine, and Society of Critical Care Medicine. An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical ventilation in adult patients with acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2017, 195, 1253–1263. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A. The importance of predefined rules and prespecified statistical analyses. Do not abandon significance. JAMA 2019, 321, 2067–2068. [Google Scholar] [CrossRef]
- Villar, J.; Ambrós, A.; Mosteiro, F.; Martínez, D.; Fernández, L.; Ferrando, C.; Carriedo, D.; Soler, J.A.; Parrilla, D.; Hernández, M.; et al. A prognostic enrichment strategy for selection of patients with acute respiratory distress syndrome in clinical trials. Crit. Care Med. 2019, 47, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, J.P.A. The proposal to lower p value thresholds to 0.005. JAMA 2018, 319, 1429–1430. [Google Scholar] [CrossRef] [PubMed]
- Matthay, M.A.; McAuley, D.F.; Ware, L.B. Clinical trials in acute respiratory distress syndrome: Challenges and opportunities. Lancet Respir. Med. 2017, 5, 524–534. [Google Scholar] [CrossRef]
- Villar, J.; Ferrando, C.; Tusman, G.; Berra, L.; Rodríguez-Suárez, P.; Suárez-Sipmann, F. Unsuccessful and successful clinical trials in acute respiratory distress syndrome: Addressing physiology-based gaps. Front. Physiol 2021, 12, 774025. [Google Scholar] [CrossRef]
- Juschten, J.; Tuinman, P.R.; Guo, T.; Juffermans, N.P.; Schultz, M.J.; Loer, S.A.; Girbes, A.R.J.; de Grooth, H.J. Between-trial heterogeneity in ARDS research. Intensive Care Med. 2021, 47, 422–434. [Google Scholar] [CrossRef]
- Forrester, J.S.; Diamond, G.A.; Swan, H.J.C. Correlative classification of clinical and hemodynamic function after acute myocardial infarction. Am. J. Cardiol. 1977, 39, 137–145. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Vergouwe, Y. Towards better clinical prediction models: Seven steps for development and an ABCD for validation. Eur. Heart J. 2014, 35, 1925–1931. [Google Scholar] [CrossRef] [PubMed]
- Qadir, N.; Bartz, R.R.; Cooter, M.L.; Hough, C.L.; Lanspa, M.J.; Banner-Goodspeed, V.M.; Chen, J.T.; Giovanni, S.; Gomaa, D.; Sjoding, M.W.; et al. Variation in early management practices in moderate-to-severe ADS in the United States. The Severe ARDS-generating evidence study. Chest 2021, 160, 1304–1315. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Suárez-Sipmann, F.; Kacmarek, R.M. Should the ART trial change our practice? J. Thorac. Dis. 2017, 9, 4871–4877. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Pérez-Méndez, L.; Aguirre-Jaime, A.; Kacmarek, R.M. Why are physicians so skeptical about positive randomized controlled trials in critical care medicine? Intensive Care Med. 2005, 31, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Bernard, G. Acute lung failure—our evolving understanding of ARDS. N. Engl. J. Med. 2017, 377, 507–509. [Google Scholar] [CrossRef] [PubMed]
- Schenck, E.J.; Oromendia, C.; Torres, L.K.; Berlin, D.A.; Choi, A.M.K.; Siempos, I.I. Rapidly improving ARDS in therapeutic randomized controlled trials. Chest 2019, 155, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Rezoagli, E.; Bellani, G. How I set up positive end-expiratory pressure: Evidence- and physiology-based. Crit. Care 2019, 23, 412. [Google Scholar] [CrossRef]
- Amato, M.B.; Meade, M.O.; Slutsky, A.S.; Brochard, L.; Costa, E.L.; Schoenfeld, D.A.; Stewerst, T.E.; Briel, M.; Talmor, D.; Mercat, A.; et al. Driving pressure and survival in the acute respiratory distress syndrome. N. Engl. J. Med. 2015, 372, 747–755. [Google Scholar] [CrossRef]
- Metkus, T.S.; Guallar, E.; Sokoll, L.; Morrow, D.; Tomaselli, G.; Brower, R.; Schulman, S.; Korley, F.K. Prevalence and prognostic association of circulating troponin in acute respiratory distress syndrome. Crit. Care Med. 2017, 45, 1709–1717. [Google Scholar] [CrossRef]
- Zhang, R.; Wang, Z.; Tejera, P.; Frank, A.J.; Wei, Y.; Su, L.; Zhu, Z.; Guo, Y.; Chen, F.; Bajwa, E.K.; et al. Late-onset moderate to severe acute respiratory distress syndrome is associated with shorter survival and higher mortality: A two-stage association study. Intensive Care Med. 2017, 43, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Hall, J.B.; Slutsky, A.S. Ten big mistakes in intensive care medicine. Intensive Care Med. 2015, 41, 505–507. [Google Scholar] [CrossRef] [PubMed]
- Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators; Cavalcanti, A.B.; Suzumura, E.A.; Laranjeira, L.N.; Paisani, D.M.; Damiani, L.P.; Guimarães, H.P.; Romano, E.R.; Regenga, M.M.; Taniguchi, L.N.T.; et al. Effect of lung recruitment and titrated positive end-expiratory pressure (PEEP) vs low PEEP on mortality in patients with acute respiratory distress syndrome: A randomized clinical trial. JAMA 2017, 318, 1335–1345. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Variables | Testing Cohort (n = 1000) | Confirmatory Cohort (n = 303) |
|---|---|---|
| Age, years, mean (SD) | 57 ± 16 | 58 ± 15 |
| Sex | n (%) | n (%) |
| Male | 680 (68.0) | 223 (73.6) |
| Female | 320 (32.0) | 80 (26.4) |
| Etiology | n (%) | n (%) |
| Pneumonia | 480 (48.0) | 110 (36.3) |
| Sepsis | 286 (28.6) | 78 (25.7) |
| Aspiration | 94 (9.4) | 47 (15.5) |
| Trauma | 74 (7.4) | 38 (12.5) |
| Acute pancreatitis | 32 (3.2) | 13 (4.3) |
| Multiple transfusions | 10 (1.0) | 3 (1.0) |
| Others | 24 (2.4) | 14 (4.6) |
| Degree of ARDS severity | n (%) | n (%) |
| Severe | 410 (41.0) | 107 (35.3) |
| Moderate | 590 (59.0) | 196 (64.7) |
| APACHE II score, mean ± SD | 20.8 ± 6.7 | 21.3 ± 7.8 ¶ |
| SOFA score, mean ± SD | 9.1 ± 3.5 | 9.8 ± 3.5 |
| PaO2/FiO2, mm Hg, mean ± SD | 114.3 ± 38.4 | 120.4 ± 41.0 |
| FiO2, mean ± SD | 0.79 ± 0.19 | 0.76 ± 0.20 |
| PaO2, mm Hg, mean ± SD | 85.9 ± 26.3 | 86.3 ± 24.9 |
| PaCO2, mm Hg, mean ± SD | 49.0 ±12.5 | 50.6 ± 13.8 |
| pH, mean ± SD | 7.30 ± 0.11 | 7.29 ± 0.11 |
| VT, mL/kg PBW, mean ± SD | 6.8 ± 1.0 | 6.7 ± 1.1 |
| Respiratory rate, resp/min, mean ± SD | 21.3 ± 4.9 | 22.3 ± 4.6 |
| Minute ventilation, L/min, mean ± SD | 9.1 ± 2.2 | 9.5 ± 2.0 |
| PEEP, cm H2O, mean ± SD | 12 ± 3 | 11 ± 3 |
| Plateau pressure, cm H2O, mean ± SD | 26.5 ± 4.8 § | 25.2 ± 4.9 |
| Driving pressure, cm H2O, mean ± SD | 14.5 ± 4.8 § | 14.3 ± 4.8 |
| No. extrapulmonary OF, mean ± SD | 1.7 ± 1.1 | 1.8 ± 1.1 |
| Length of ICU stay, d, median (P25–P75) | 19 (11–31) | 16 (9–27) |
| Duration of MV from ARDS diagnosis, d, mean ± SD | 17.6 ± 17.0 | 14.0 ± 16.6 |
| VFDs, d, mean ± SD | 7.9 ± 9.1 | 9.2 ± 9.7 |
| Days from ICU admission to ARDS onset, median (P25–P75) | 1 (0–3) | 1 (0–2) |
| Days from ARDS onset to ICU discharge, median (P25–P75) | 16 (9–28) | 14 (7–23) |
| All-cause ICU mortality, n (%) | 375 (37.5) | 112 (37.0) |
| All-cause hospital mortality, n (%) | 415 (41.5) | 124 (40.9) |
| Cohort | Timing | Subset I PaO2/FiO2 ≥ 150 at PEEP < 10 | Subset II PaO2/FiO2 ≥ 150 at PEEP ≥ 10 | Subset III PaO2/FiO2 < 150 at PEEP < 10 | Subset IV PaO2/FiO2 < 150 at PEEP ≥ 10 | p-Value |
|---|---|---|---|---|---|---|
| Testing Cohort | At moderate/severe ARDS diagnosis | |||||
| No. of subjects | 73 | 135 | 240 | 552 | ||
| No. events (ICU deaths) | 25 | 41 | 97 | 212 | ||
| Event rate (95% CI) | 34.3(23.4–45.1) | 30.4(22.6–38.1) | 40.4(34.2–46.6) | 38.4(34.4–42.5) | 0.184 | |
| Risk ratio (95% CI) | 1 (Ref) | 0.9 (0.6–1.3) | 1.2 (0.8–1.7) | 1.1 (0.8–1.6) | 0.229 | |
| At 24 h after onset | ||||||
| No. of subjects | 28 | 403 | 25 | 544 | ||
| No. events (ICU deaths) | 5 | 92 | 10 | 268 | ||
| Event rate (95% CI) | 17.9 (3.7–32.0) | 22.8(18.7–26.9) | 40.0(20.8–59.2) | 49.3(45.0–53.6) | <0.001 | |
| Risk ratio (95% CI) | 1 (Ref) | 1.6 (0.6–2.9) | 2.2 (0.9–5.7) | 2.8 (1.2–6.1) | <0.001 | |
| Confirmatory Cohort | At moderate/severe ARDS diagnosis | |||||
| No. of subjects | 32 | 48 | 78 | 145 | ||
| No. events (ICU deaths) | 9 | 18 | 34 | 51 | ||
| Event rate (95% CI) | 28.1(12.6–43.7) | 37.5(24.0–52.7) | 43.6(32.4–55.3) | 35.2(27.4–42.9) | 0.745 | |
| Risk ratio (95% CI) | 1 (Ref) | 1.3 (0.7–2.6) | 1.6 (0.8–2.8) | 1.3 (0.7–2.3) | 0.434 | |
| At 24 h after onset | ||||||
| No. of subjects | 28 | 139 | 14 | 122 | ||
| No. events (ICU deaths) | 4 | 28 | 7 | 73 | ||
| Event rate (95% CI) | 14.3 (1.3–27.3) | 20.1(13.5–26.8) | 50.0(23.8–76.2) | 59.8(51.1–68.5) | <0.001 | |
| Risk ratio (95% CI) | 1 (Ref) | 1.4 (0.5–3.7) | 3.5 (1.2–10.0) | 4.2 (1.7–10.5) | <0.001 |
| Variables | Values | ||||
|---|---|---|---|---|---|
| Subset I n = 28 | Subset II n = 403 | Subset III n = 25 | Subset IV n = 544 | p-Value | |
| APACHE II ¶ | |||||
| Mean ± SD | 16.4 ± 4.2 | 17.5 ± 7.2 | 20.1 ± 6.4 | 20.4 ± 7.0 | <0.001 |
| Mean difference (95% CI) | 0 (Ref) | 1.1 (−1.6 to 3.8) | 3.7 (0.7 to 6.7) | 4.0 (1.4 to 6.6) | <0.001 |
| Age, mean ± SD | 66 ± 13 | 56 ± 16 | 60 ± 19 | 57 ± 16 | 0.011 |
| Sex, No. (%) | 0.046 | ||||
| Men | 15 (53.6) | 263 (65.3) | 21 (84.0) | 381 (70.0) | |
| Women | 13 (46.4) | 140 (34.7) | 4 (16.0) | 163 (30.0) | |
| VT, mL/kg PBW | |||||
| Mean ± SD | 6.8 ± 0.9 | 6.7 ± 0.9 | 6.7 ± 0.8 | 6.6 ± 0.9 | 0.285 |
| Mean difference (95% CI) | 0 (Ref) | −0.1 (−0.4 to 0.2) | −0.1 (−0.6 to 0.4) | −0.2 (−0.5 to 0.1) | 0.252 |
| Plateau pressure, cm H2O | |||||
| Mean ± SD | 24.4 ± 5.0 | 25.2 ± 4.6 | 26.2 ± 4.6 | 28.0 ± 4.3 | <0.001 |
| Mean difference (95% CI) | 0 (Ref) | 0.8 (−1.0 to 2.6) | 1.8 (−0.9 to 4.5) | 3.6 (2.0 to 5.3) | <0.001 |
| PEEP, cm H2O | |||||
| Mean ± SD | 7.6 ± 1.7 | 12.5 ± 2.8 | 7.4 ± 2.1 | 13.0 ± 2.8 | <0.001 |
| Mean difference (95% CI) | 0 (Ref) | 4.9 (3.8 to 6.0) | −0.2 (−1.2 to 0.8) | 5.4 (4.4 to 6.5) | <0.001 |
| Driving pressure, cm H2O | |||||
| Mean ± SD | 16 ± 5 | 12 ± 4 | 18 ± 5 | 15 ± 4 | <0.001 |
| Mean difference (95% CI) | 0 (Ref) | −4 (−6 to −3) | 2 (−1 to 5) | −1 (−2 to 1) | <0.001 |
| FiO2 | |||||
| Mean ± SD | 0.53 ± 0.11 | 0.55 ± 0.11 | 0.77 ± 0.16 | 0.75 ± 0.18 | <0.001 |
| Mean difference (95% CI) | 0 (Ref) | 0.02(−0.1 to 0.1) | 0.24 (0.2 to 0.7) | 0.22 (0.1 to 0.3) | <0.001 |
| PaO2/FiO2, mm Hg | |||||
| Mean ± SD | 228 ± 45 | 200 ± 46 | 110 ± 30 | 107 ± 27 | <0.001 |
| Mean difference (95% CI) | 0 (Ref) | −28 (−46 to −10) | −118(−139 to −97) | −121(−132 to −110) | <0.001 |
| SOFA score | |||||
| Mean ± SD | 7.3 ± 3.5 | 8.1 ± 3.3 | 8.2 ± 3.3 | 9.9 ±3.8 | <0.001 |
| Mean difference (95% CI) | 0 (Ref) | 0.8 (−0.5 to 2.1) | 0.9 (−1.0 to 2.8) | 2.6 (1.2 to 4.0) | <0.001 |
| Days on MV from ARDS diagnosis | |||||
| Mean ± SD | 12.3 ± 13.1 | 16.2 ± 14.9 | 16.3 ± 14.3 | 19.0 ± 18.5 | 0.025 |
| Mean difference (95% CI) | 0 (Ref) | 3.9 (−1.8 to 9.6) | 4.0(−3.6 to 11.6) | 6.7(−0.3 to 13.7) | 0.059 |
| VFDs, d | |||||
| Mean ± SD | 13.7 ± 11. | 11.1 ± 9.5 | 6.8 ± 8.8 | 5.2 ± 7.8 | <0.001 |
| Mean difference (95% CI) | 0 (Ref) | −2.6 (−6.3 to 1.1) | −6.9(−12.4 to −1.4) | −8.5(−11.5 to −5.5) | <0.001 |
| ICU deaths | |||||
| No. events | 5 | 92 | 10 | 268 | |
| Event rate (95% CI) | 17.9 (3.7–32.0) | 22.8 (18.7–26.9) | 40.0 (20.8–59.2) | 49.3 (45.1–53.5) | <0.001 |
| Risk ratio (95% CI) | 1 (Ref) | 1.3 (0.6–2.9) | 2.2 (0.9–5.7) | 2.8 (1.2–6.1) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villar, J.; Fernández, C.; González-Martín, J.M.; Ferrando, C.; Añón, J.M.; del Saz-Ortíz, A.M.; Díaz-Lamas, A.; Bueno-González, A.; Fernández, L.; Domínguez-Berrot, A.M.; et al. Respiratory Subsets in Patients with Moderate to Severe Acute Respiratory Distress Syndrome for Early Prediction of Death. J. Clin. Med. 2022, 11, 5724. https://doi.org/10.3390/jcm11195724
Villar J, Fernández C, González-Martín JM, Ferrando C, Añón JM, del Saz-Ortíz AM, Díaz-Lamas A, Bueno-González A, Fernández L, Domínguez-Berrot AM, et al. Respiratory Subsets in Patients with Moderate to Severe Acute Respiratory Distress Syndrome for Early Prediction of Death. Journal of Clinical Medicine. 2022; 11(19):5724. https://doi.org/10.3390/jcm11195724
Chicago/Turabian StyleVillar, Jesús, Cristina Fernández, Jesús M. González-Martín, Carlos Ferrando, José M. Añón, Ana M. del Saz-Ortíz, Ana Díaz-Lamas, Ana Bueno-González, Lorena Fernández, Ana M. Domínguez-Berrot, and et al. 2022. "Respiratory Subsets in Patients with Moderate to Severe Acute Respiratory Distress Syndrome for Early Prediction of Death" Journal of Clinical Medicine 11, no. 19: 5724. https://doi.org/10.3390/jcm11195724
APA StyleVillar, J., Fernández, C., González-Martín, J. M., Ferrando, C., Añón, J. M., del Saz-Ortíz, A. M., Díaz-Lamas, A., Bueno-González, A., Fernández, L., Domínguez-Berrot, A. M., Peinado, E., Andaluz-Ojeda, D., González-Higueras, E., Vidal, A., Fernández, M. M., Mora-Ordoñez, J. M., Murcia, I., Tarancón, C., Merayo, E., ... The Spanish Initiative for Epidemiology, Stratification and Therapies of ARDS (SIESTA) Network. (2022). Respiratory Subsets in Patients with Moderate to Severe Acute Respiratory Distress Syndrome for Early Prediction of Death. Journal of Clinical Medicine, 11(19), 5724. https://doi.org/10.3390/jcm11195724