
A Comparative Analysis of Robot-Assisted Laparoscopic Pyeloplasty in Pediatric and Adult Patients: Does Age Matter?

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Clinical Variables
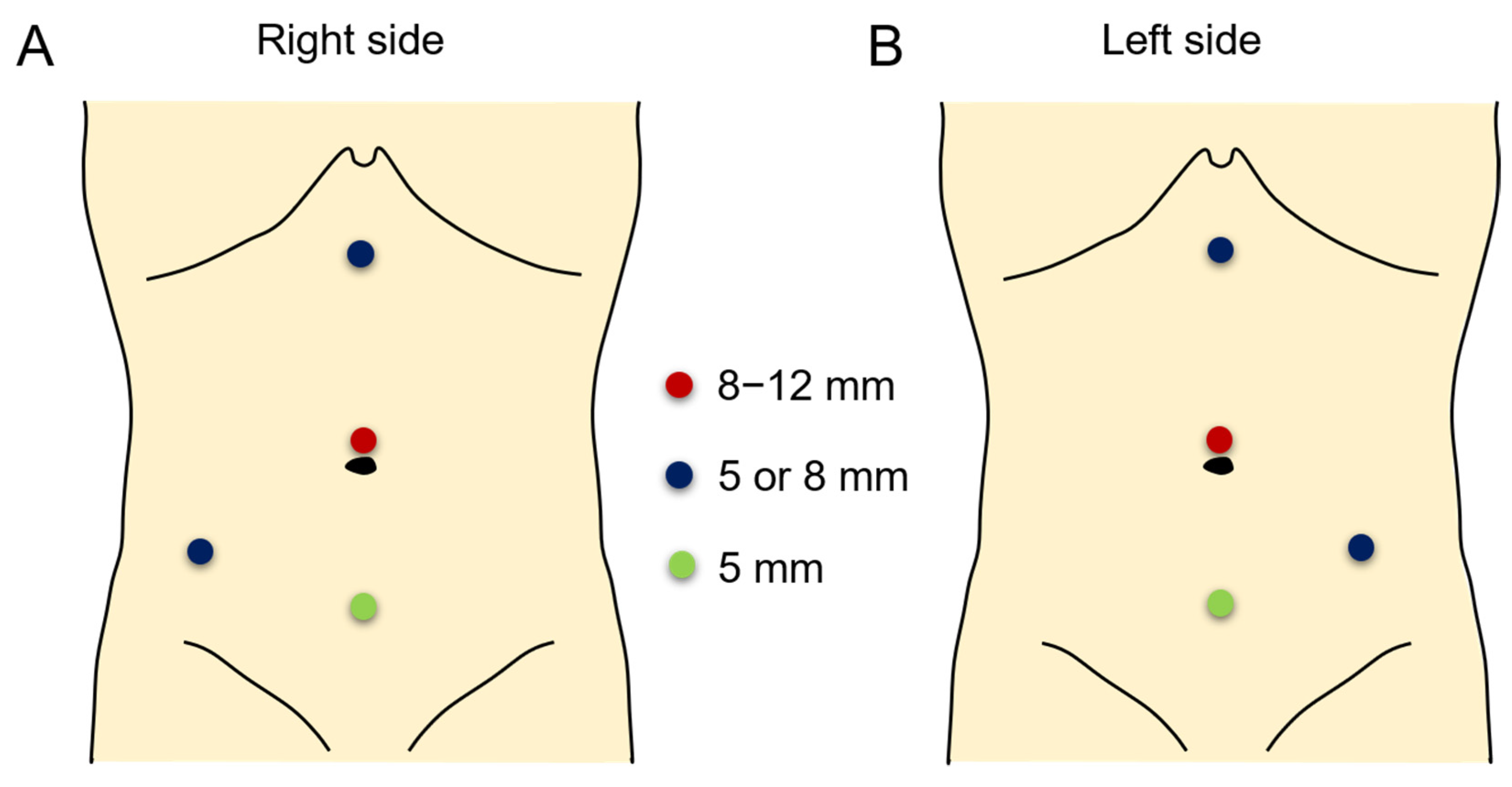
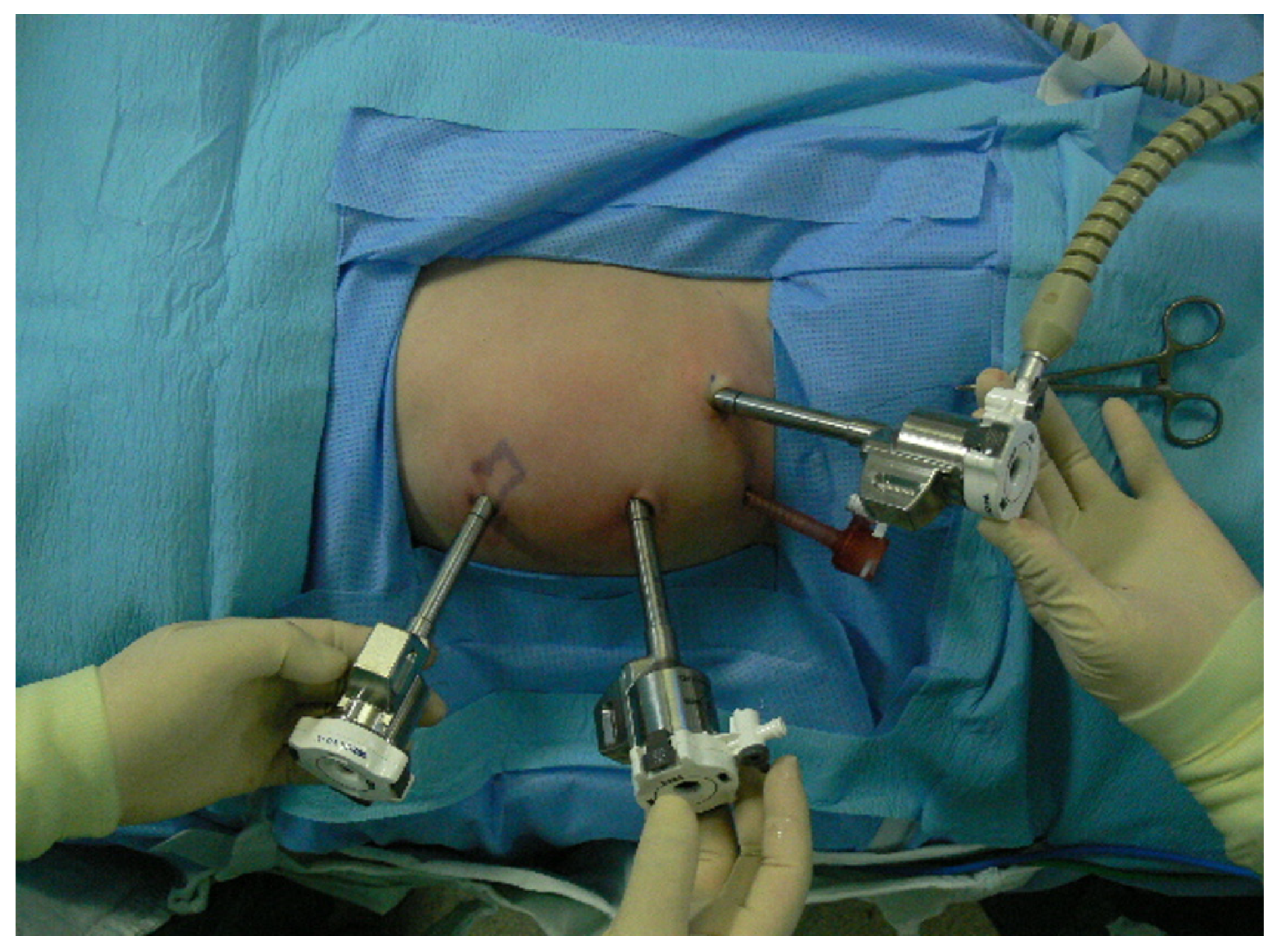
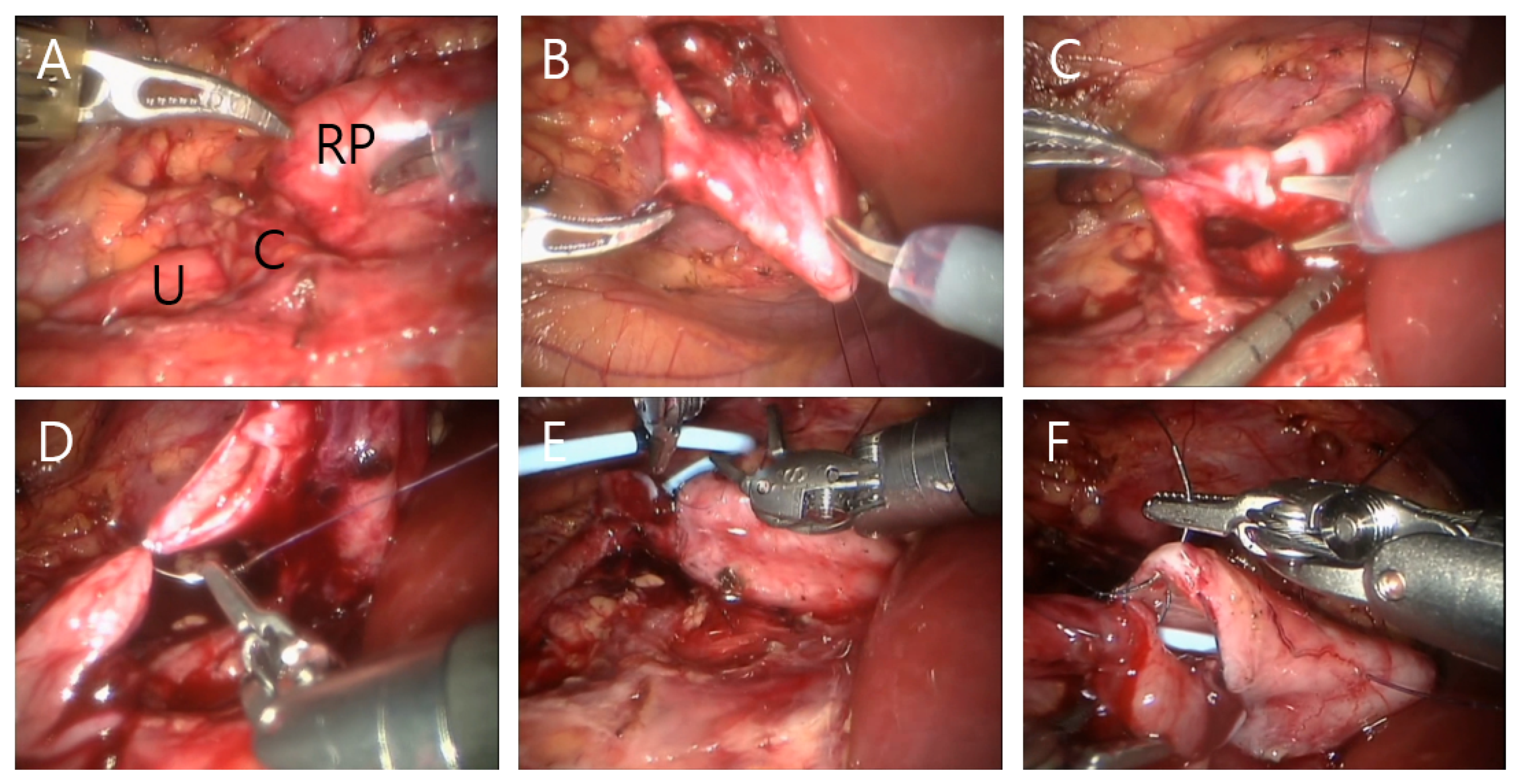
2.3. Surgical Techniques and Postoperative Management
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jackson, L.; Woodward, M.; Coward, R.J. The molecular biology of pelvi-ureteric junction obstruction. Pediatr. Nephrol. 2018, 33, 553–571. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, R.H. Clinical assessment of pelvic and ureteral function. Urology 1978, 12, 146–150. [Google Scholar] [CrossRef]
- Passoni, N.M.; Peters, C.A. Managing Ureteropelvic Junction Obstruction in the Young Infant. Front. Pediatr. 2020, 8, 242. [Google Scholar] [CrossRef] [PubMed]
- Vemulakonda, V.M.; Sevick, C.; Juarez-Colunga, E.; Chiang, G.; Janzen, N.; Saville, A.; Adams, P.; Beltran, G.; King, J.; Ewing, E.; et al. Treatment of infants with ureteropelvic junction obstruction: Findings from the PURSUIT network. Int. Urol. Nephrol. 2021, 53, 1485–1495. [Google Scholar] [CrossRef]
- Chen, C.J.; Peters, C.A. Robotic Assisted Surgery in Pediatric Urology: Current Status and Future Directions. Front. Pediatr. 2019, 7, 90. [Google Scholar] [CrossRef]
- Gettman, M.T.; Neururer, R.; Bartsch, G.; Peschel, R. Anderson-Hynes dismembered pyeloplasty performed using the da Vinci robotic system. Urology 2002, 60, 509–513. [Google Scholar] [CrossRef]
- Lee, R.S.; Retik, A.B.; Borer, J.G.; Peters, C.A. Pediatric robot assisted laparoscopic dismembered pyeloplasty: Comparison with a cohort of open surgery. J. Urol. 2006, 175, 683–687; discussion 687. [Google Scholar] [CrossRef]
- Yee, D.S.; Shanberg, A.M.; Duel, B.P.; Rodriguez, E.; Eichel, L.; Rajpoot, D. Initial comparison of robotic-assisted laparoscopic versus open pyeloplasty in children. Urology 2006, 67, 599–602. [Google Scholar] [CrossRef] [PubMed]
- Munver, R.; Sosa, R.E.; del Pizzo, J.J. Laparoscopic pyeloplasty: History, evolution, and future. J. Endourol. 2004, 18, 748–755. [Google Scholar] [CrossRef] [PubMed]
- Friedmacher, F.; Till, H. Robotic-Assisted Procedures in Pediatric Surgery: A Critical Appraisal of the Current Best Evidence in Comparison to Conventional Minimally Invasive Surgery. J. Laparoendosc. Adv. Surg. Tech. A 2015, 25, 936–943. [Google Scholar] [CrossRef] [PubMed]
- Jackson, H.T.; Kane, T.D. Advances in minimally invasive surgery in pediatric patients. Adv. Pediatr. 2014, 61, 149–195. [Google Scholar] [CrossRef] [PubMed]
- Andolfi, C.; Adamic, B.; Oommen, J.; Gundeti, M.S. Robot-assisted laparoscopic pyeloplasty in infants and children: Is it superior to conventional laparoscopy? World J. Urol. 2020, 38, 1827–1833. [Google Scholar] [CrossRef] [PubMed]
- Salo, M.; Bonnor, L.; Graneli, C.; Stenstrom, P.; Anderberg, M. Ten years of paediatric robotic surgery: Lessons learned. Int. J. Med. Robot. 2022, 18, e2386. [Google Scholar] [CrossRef] [PubMed]
- Song, S.H.; Lee, C.; Jung, J.; Kim, S.J.; Park, S.; Park, H.; Kim, K.S. A comparative study of pediatric open pyeloplasty, laparoscopy-assisted extracorporeal pyeloplasty, and robot-assisted laparoscopic pyeloplasty. PLoS ONE 2017, 12, e0175026. [Google Scholar] [CrossRef] [PubMed]
- Peters, C.A. Robotic Pyeloplasty in Infants: Eliminating Age Discrimination. J. Urol. 2022, 207, 276. [Google Scholar] [CrossRef] [PubMed]
- Minnillo, B.J.; Cruz, J.A.; Sayao, R.H.; Passerotti, C.C.; Houck, C.S.; Meier, P.M.; Borer, J.G.; Diamond, D.A.; Retik, A.B.; Nguyen, H.T. Long-term experience and outcomes of robotic assisted laparoscopic pyeloplasty in children and young adults. J. Urol. 2011, 185, 1455–1460. [Google Scholar] [CrossRef]
- Greenwald, D.; Mohanty, A.; Andolfi, C.; Gundeti, M.S. Systematic Review and Meta-Analysis of Pediatric Robot-Assisted Laparoscopic Pyeloplasty. J. Endourol. 2022, 36, 448–461. [Google Scholar] [CrossRef]
- Kawal, T.; Srinivasan, A.K.; Shrivastava, D.; Chu, D.I.; Van Batavia, J.; Weiss, D.; Long, C.; Shukla, A.R. Pediatric robotic-assisted laparoscopic pyeloplasty: Does age matter? J. Pediatr. Urol. 2018, 14, 540.e1–540.e6. [Google Scholar] [CrossRef]
- Autorino, R.; Eden, C.; El-Ghoneimi, A.; Guazzoni, G.; Buffi, N.; Peters, C.A.; Stein, R.J.; Gettman, M. Robot-assisted and laparoscopic repair of ureteropelvic junction obstruction: A systematic review and meta-analysis. Eur. Urol. 2014, 65, 430–452. [Google Scholar] [CrossRef]
- Mufarrij, P.W.; Woods, M.; Shah, O.D.; Palese, M.A.; Berger, A.D.; Thomas, R.; Stifelman, M.D. Robotic dismembered pyeloplasty: A 6-year, multi-institutional experience. J. Urol. 2008, 180, 1391–1396. [Google Scholar] [CrossRef]
- Mizuno, K.; Kojima, Y.; Kurokawa, S.; Kamisawa, H.; Nishio, H.; Moritoki, Y.; Nakane, A.; Maruyama, T.; Okada, A.; Kawai, N.; et al. Robot-assisted laparoscopic pyeloplasty for ureteropelvic junction obstruction: Comparison between pediatric and adult patients-Japanese series. J. Robot. Surg. 2017, 11, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Rosen, H.I.; Bergh, I.H.; Oden, A.; Martensson, L.B. Patients experiences of pain following day surgery—At 48 hours, seven days and three months. Open Nurs. J. 2011, 5, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Ceyhan, E.; Ileri, F.; Ceylan, T.; Aydin, A.M.; Dogan, H.S.; Tekgul, S. Predictors of Recurrence and Complications in Pediatric Pyeloplasty. Urology 2019, 126, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Cummings, L.J.; Waters, S.L.; Wattis, J.A.; Graham, S.J. The effect of ureteric stents on urine flow: Reflux. J. Math. Biol. 2004, 49, 56–82. [Google Scholar] [CrossRef]
- Vidovic, S.; Hayes, T.; Fowke, J.; Cline, J.K.; Cannon, G.M.; Colaco, M.A.; Swords, K.A.; Cornwell, L.B.; Villanueva, C.; Corbett, S.T.; et al. Pyeloplasty with ureteral stent placement in children: Do prophylactic antibiotics serve a purpose? J. Pediatr. Urol. 2022; online ahead of print. [Google Scholar] [CrossRef]
- Nayyar, R.; Gupta, N.P.; Hemal, A.K. Robotic management of complicated ureteropelvic junction obstruction. World J. Urol. 2010, 28, 599–602. [Google Scholar] [CrossRef]
- Kadihasanoglu, M.; Yucetas, U.; Karabay, E.; Sonmezay, E. Comparison of the outcomes of laparoscopic pyeloplasty with and without concomitant pyelolithotomy. Int. Braz. J. Urol. 2019, 45, 965–973. [Google Scholar] [CrossRef]
- Chow, A.K.; Rosenberg, B.J.; Capoccia, E.M.; Cherullo, E.E. Risk Factors and Management Options for the Adult Failed Ureteropelvic Junction Obstruction Repair in the Era of Minimally Invasive and Robotic Approaches: A Comprehensive Literature Review. J. Endourol. 2020, 34, 1112–1119. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, J.; Chen, W.; Xiong, L.; Huang, X.; Ye, X. Crossing vessels with suspension versus transposition in laparoscopic pyeloplasty of patients with ureteropelvic junction obstruction: A retrospective study. BMC Urol. 2021, 21, 77. [Google Scholar] [CrossRef]
- Muradi, T.; Turkyilmaz, Z.; Karabulut, R.; Sonmez, K.; Kaya, C.; Polat, F.; Basaklar, A.C. Our experience of operated pediatric ureteropelvic junction obstruction patients. Urologia, 2021; online ahead of print. [Google Scholar] [CrossRef]
- Tasian, G.E.; Wiebe, D.J.; Casale, P. Learning curve of robotic assisted pyeloplasty for pediatric urology fellows. J. Urol. 2013, 190, 1622–1626. [Google Scholar] [CrossRef]
- Kassite, I.; Braik, K.; Villemagne, T.; Lardy, H.; Binet, A. The learning curve of robot-assisted laparoscopic pyeloplasty in children: A multi-outcome approach. J. Pediatr. Urol. 2018, 14, 570.e1–570.e10. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pediatric Group (n = 48) | Adult Group (n = 69) | |
|---|---|---|
| Age at surgery, med (range), (year) | 7.5 (0–18) | 39.3 (19–74) |
| Height at surgery, med (range), (cm) | 122.5 (62.4–183.7) | 166.0 (149.3–186.8) |
| Weight at surgery, med (range), (kg) | 32.4 (7.1–110.3) | 63.3 (46.8–96.0) |
| Body mass index, med (range), (kg/m2) | 18.7 (12.8–35.6) | 22.9 (16.7–31.1) |
| * Obesity at surgery (%) | 13 (27.1) | 15 (21.7) |
| Gender (male:female) | 34:14 (70.8:29.2) | 31:38 (44.9:55.1) |
| Laterality (right:left) | 13:35 (27.1:72.9) | 28:41 (40.6:59.4) |
| s-Creatinine at surgery, med (range), (mg/dL) | 0.5 (0.2–1.5) | 0.9 (0.5–1.6) |
| SFU grade at surgery, n (%) | ||
| 1–2 | 2 (4.2) | 9 (13.0) |
| 3–4 | 46 (95.8) | 60 (87.0) |
| APPD at surgery, med (range), (cm) | 3.5 (0.7–6.7) | 4.1 (1.0–9.4) |
| SRF at surgery, med (range), (%) | 41.8 (5.5–56.6) | 36.5 (6.4–58.0) |
| No. presentation (%) | ||
| Prenatally detected | 17 (35.4) | 0 |
| Incidentally detected | 3 (6.3) | 19 (27.5) |
| Flank/abdominal pain | 20 (41.7) | 47 (68.1) |
| Gross hematuria | 5 (10.4) | 1 (1.4) |
| UTI | 3 (6.3) | 2 (2.9) |
| Pyeloplasty method (%) | ||
| Dismembered | 45 (93.8) | 69 (100) |
| Nondismembered | 3 (6.3) | 0 (0) |
| Surgical Approach (%) | ||
| Transmesenteric | 22 (45.8) | 16 (23.2) |
| Nontransmesenteric | 26 (54.2) | 53 (76.8) |
| Pediatric Group (n = 48) | Adult Group (n = 69) | p-Value | |
|---|---|---|---|
| Total operative time, median (range), (min) | 171 (70–324) | 148 (65–370) | 0.030 |
| Console time, median (range), (min) | 126 (78–220) | 110 (86–170) | 0.020 |
| Anastomosis time, median (range), (min) | 63 (15–100) | 45 (32–65) | 0.271 |
| Etiology, n (%) | 0.169 | ||
| Intrinsic-primary | 29 (60.4) | 34 (49.3) | |
| Intrinsic-polyp | 6 (12.5) | 5 (7.2) | |
| Crossing vessel | 13 (27.1) | 30 (43.5) | |
| Postoperative SRF, median (range), (%) | 41.7 (11.6–57.5) | 38.9 (12.0–59.8) | 0.418 |
| Postoperative s-Creatinine, median (range), (mg/dL) | 0.5 (0.2–1.1) | 0.8 (0.5–1.6) | 0.859 |
| Hospital day, median (range), (day) | 3.7 (2–12) | 4.7 (3–13) | 0.278 |
| Pain score ≥ 4 requires analgesics (%) | |||
| Postop day 0 | 17 (35.4) | 46 (66.7) | 0.648 |
| Postop day 1 | 4 (8.3) | 23 (33.3) | <0.001 |
| Postop day 2 | 1 (2.1) | 4 (5.8) | 0.049 |
| Morphine dose, median (range), (mg/kg) | |||
| Postop day 0 | 0.08 (0–0.25) | 0.15 (0–0.27) | 0.005 |
| Postop day 1 | 0.08 (0–0.33) | 0.24 (0–0.40) | 0.007 |
| Postop day 2 | 0.03 (0–0.30) | 0.11 (0–0.46) | 0.024 |
| Pediatric Group (n = 48) | Adult Group (n = 69) | p-Value | |
|---|---|---|---|
| Surgical complication * | 3 | 2 | 0.688 |
| Postoperative DJ insertion due to obstruction | 1 | 0 | |
| Ureteroscopic DJ removal due to DJ malposition | 1 | 0 | |
| DJ reposition due to DJ malposition at POD#1 | 1 | 0 | |
| Idiopathic hypoxia after surgery | 0 | 1 | |
| RIRS for recurred renal stone removal | 0 | 1 | |
| Secondary procedures needed | 3 | 3 | 0.688 |
| Surgical failure (%) | 2 (4.2) | 2 (2.9) | >0.999 |
| Redo pyeloplasty (%) | 0 (0.0) | 1 (1.4) | |
| Aggravation of hydronephrosis (%) | 1 (2.1) | 1 (1.4) | |
| Decrease in SRF in 36 months (%) | 1 (2.1) | 0 (0.0) | |
| Urolithiasis after pyeloplasty (%) | 3 (6.3) | 2 (2.9) | 0.400 |
| ESWL (%) | 2 (4.2) | 1 (1.4) | |
| RIRS (%) | 1 (2.1) | 1 (1.4) | |
| Urinary tract infection within 30 days after surgery | 3 | 0 | 0.066 |
| Univariate | Multivariable | |||||
|---|---|---|---|---|---|---|
| Odds | 95% CI | p-Value | Odds | 95% CI | p-Value | |
| * Obesity | 10.6 | 1.1–106.0 | 0.045 | * | * | 0.104 |
| Preop stone | 14.8 | 1.5–150.5 | 0.022 | 14.5 | 1.4–147.3 | 0.022 |
| ** Age (pediatric = 1) | 1.5 | 0.2–10.7 | 0.712 | |||
| *** Preop APPD | 1.0 | 0.5–1.8 | 0.965 | |||
| SRF (<30%) | 0.9 | 0.09–9.4 | 0.960 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, B.; Suh, J.; Lim, B.; Kim, K.S.; Song, S.H. A Comparative Analysis of Robot-Assisted Laparoscopic Pyeloplasty in Pediatric and Adult Patients: Does Age Matter? J. Clin. Med. 2022, 11, 5651. https://doi.org/10.3390/jcm11195651
Kang B, Suh J, Lim B, Kim KS, Song SH. A Comparative Analysis of Robot-Assisted Laparoscopic Pyeloplasty in Pediatric and Adult Patients: Does Age Matter? Journal of Clinical Medicine. 2022; 11(19):5651. https://doi.org/10.3390/jcm11195651
Chicago/Turabian StyleKang, Bosik, Jungyo Suh, Bumjin Lim, Kun Suk Kim, and Sang Hoon Song. 2022. "A Comparative Analysis of Robot-Assisted Laparoscopic Pyeloplasty in Pediatric and Adult Patients: Does Age Matter?" Journal of Clinical Medicine 11, no. 19: 5651. https://doi.org/10.3390/jcm11195651
APA StyleKang, B., Suh, J., Lim, B., Kim, K. S., & Song, S. H. (2022). A Comparative Analysis of Robot-Assisted Laparoscopic Pyeloplasty in Pediatric and Adult Patients: Does Age Matter? Journal of Clinical Medicine, 11(19), 5651. https://doi.org/10.3390/jcm11195651