
Combining Awake Anesthesia with Minimal Invasive Surgery Optimizes Intraoperative Surgical Spinal Cord Stimulation Lead Placement
 ,
,  , ,
, ,  , , and
, , and  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
- -
- SCS temporal resolution has been the subject of intensive research, making new waveforms available for the last generation of internal pulse generators (IPG). This modulates temporal resolution of the electrical signal in view of obtaining better pain relief, less discomfort and more personalized therapy by selecting or even combining several signals at the same time [18,19,20,21,22,23]. This also identifies new SCS mechanisms of action conveyed by different patterns from the classical gate control theory [24,25,26,27]. oudmanth, Foremanste 2016, Goudman et al. supériorité., Billot Mns sa pratique cliniquetifique afin de les synthétiser.
- -
2. Materials and Methods
2.1. Objectives
2.2. Study Design
2.3. Study Population
2.4. Procedures
2.5. Subgroup Analysis
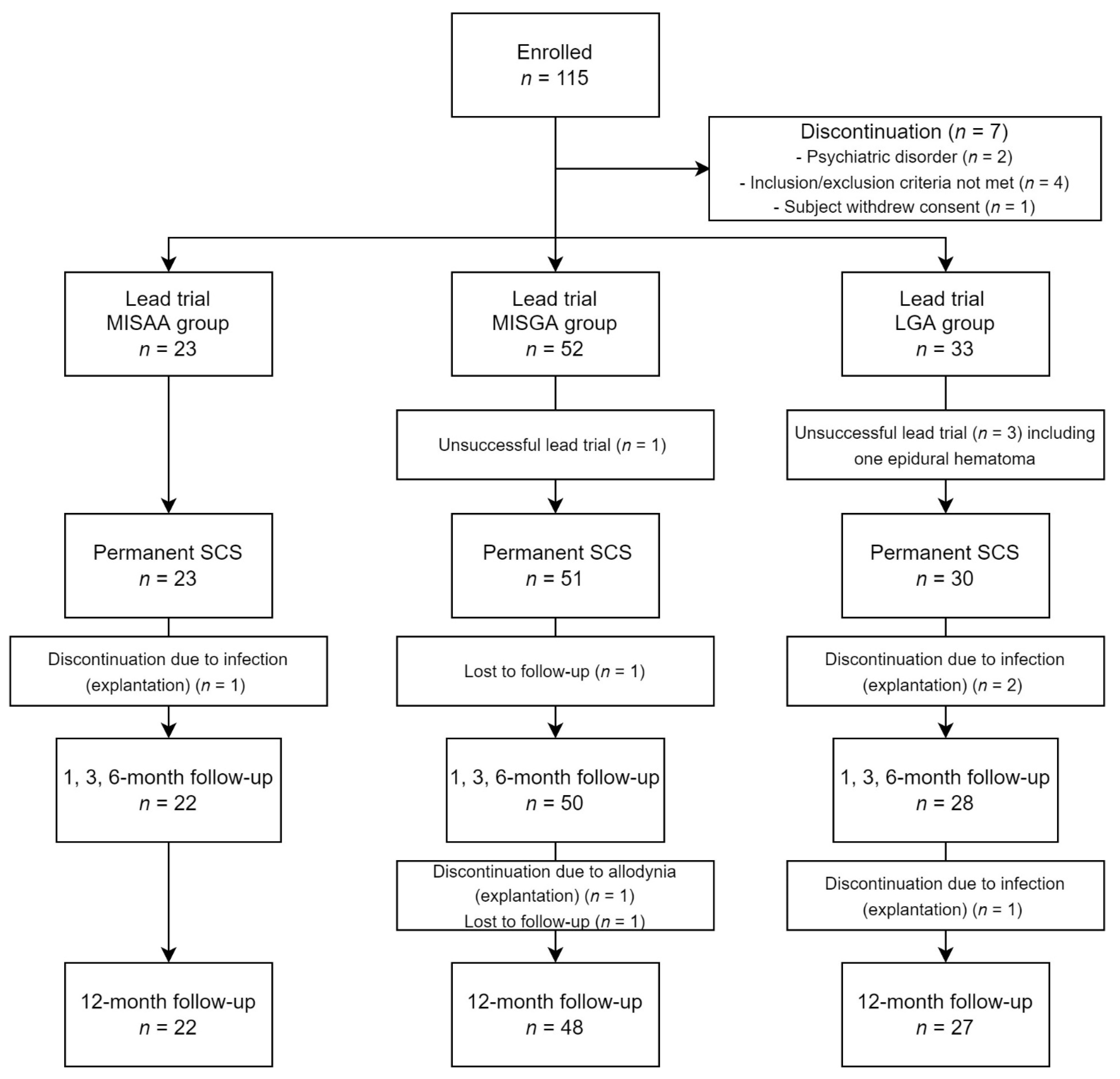
- (1)
- The first sub-group includes patients having undergone optimized lead positioning through minimal invasive surgery under awake anesthesia (MISAA group) using TCIVA.
- (2)
- The second group includes patients having undergone lead placement through minimal invasive surgery under general anesthesia (MISGA group).
- (3)
- The third sub-group includes patients having undergone anatomic lead placement with laminectomy under general anesthesia (LGA group).
2.6. Study Outcomes
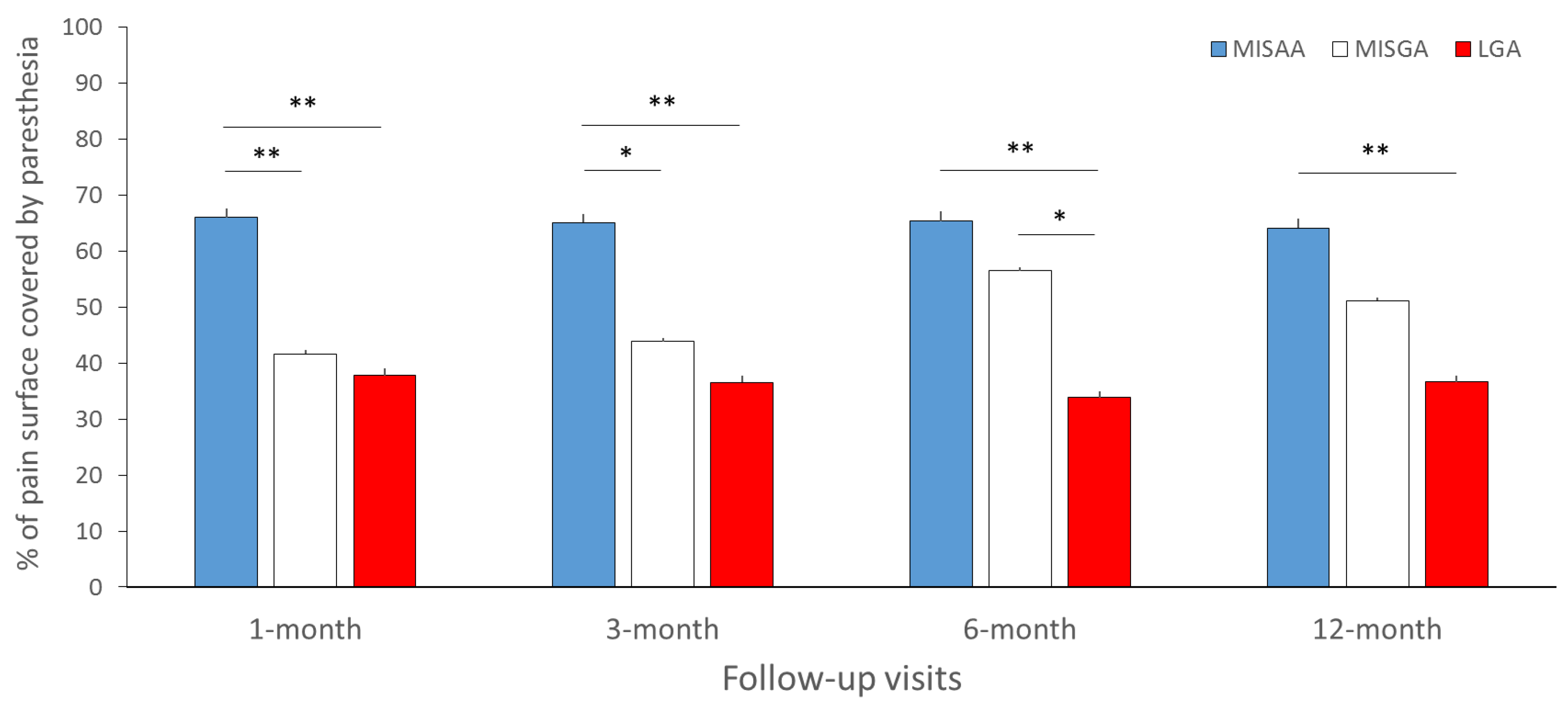
- Paresthesia coverage was evaluated as the percentage of pain covered by paresthesia. This percentage was calculated as the surface of pain (in cm²) covered by paresthesia divided by the total pain surface.
- Selectivity was evaluated as the percentage of paresthesia covering pain (i.e., the surface of pain covered by paresthesia divided by the total paresthesia surface).
- Global pain relief was evaluated by the percentage of global pain decrease and the percentage of patients with a 50% pain decrease.
- Back pain relief was evaluated by the percentage of back pain decrease.
- Leg pain relief was evaluated by the percentage of leg pain decrease.
- Functional improvement was evaluated by the percentage of decrease of the Oswestry disability questionnaire (ODI).
- Quality of life improvement was assessed using the absolute increase in EuroQoL-5 dimensions 3 level (EQ-5D-3L) index.
- Depression level was evaluated using the Montgomery–Asberg depression scale (MADRS).
- Holistic composite evaluation was used to provide a score representing the patient’s Global Health Score (GHS). This score includes pain intensity (VAS), functional disability (ODI), quality of life (EQ5D), depression (MADRS) and pain surface. The score was calculated based on a principal component analysis (PCA) by including these 5 variables [5,42]. The first principal component served as the global multidimensional score. The score was then scaled to 0 (worst global health) to 10 (best global health) for easier interpretations. The absolute difference between baseline and each follow-up was used to evaluate overall health improvement.
- Complication rates following the lead implantation were also reported and compared between the three groups.
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Comparison of Pain Mapping Outcomes between the Groups
3.3. Comparison of Clinical Outcomes between Groups after 6 and 12 Months
3.3.1. Overall Pain Relief
3.3.2. Back Pain Relief
3.3.3. Leg Pain Relief
3.3.4. Functional Capacity Improvement (ODI Score)
3.3.5. Health-Related Quality of Life Improvement (EQ-5D-3L)
3.3.6. Depression Score Decrease (MADRS)
3.3.7. Global Health Score Improvement (GHS)
3.4. Safety Analysis
4. Discussions
4.1. Potential Added-Value of MIS to Allow Surgical SCS Placement under Awake Conditions
4.2. Combining MIS with TCIVA for Surgical SCS Implantation to Facilitate Patient Intraoperative Feedback
4.3. The Use of an Intraoperative Pain Mapping Tool Can Help to Optimize Lead Placement and Programming, Including Waveform Selection
4.4. To What Extent Could Hypnosis Impact Patient Comfort during Awake Procedure?
4.5. Study Limitations and Technical Considerations
4.6. Does Optimized Lead Positioning Matter in 2022?
4.7. The Use of Intraoperative Assessment by Pain Mapping Tool Combined with Awake and MIS Surgical SCS Implantation As a Surrogate for Lead-Trial Phase
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schug, S.A.; Lavand’homme, P.; Barke, A.; Korwisi, B.; Rief, W.; Treede, R.-D.; IASP Taskforce for the Classification of Chronic Pain. The IASP Classification of Chronic Pain for ICD-11: Chronic Postsurgical or Posttraumatic Pain. Pain 2019, 160, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Naiditch, N.; Billot, M.; Goudman, L.; Cornet, P.; Roulaud, M.; Ounajim, A.; Page, P.; Lorgeoux, B.; Baron, S.; Nivole, K.; et al. Professional Status of Persistent Spinal Pain Syndrome Patients after Spinal Surgery (PSPS-T2): What Really Matters? A Prospective Study Introducing the Concept of “Adapted Professional Activity” Inferred from Clinical, Psychological and Social Influence. J. Clin. Med. 2021, 10, 5055. [Google Scholar] [CrossRef] [PubMed]
- Naiditch, N.; Billot, M.; Moens, M.; Goudman, L.; Cornet, P.; Le Breton, D.; Roulaud, M.; Ounajim, A.; Page, P.; Lorgeoux, B.; et al. Persistent Spinal Pain Syndrome Type 2 (PSPS-T2), a Social Pain? Advocacy for a Social Gradient of Health Approach to Chronic Pain. J. Clin. Med. 2021, 10, 2817. [Google Scholar] [CrossRef] [PubMed]
- Ounajim, A.; Billot, M.; Louis, P.-Y.; Slaoui, Y.; Frasca, D.; Goudman, L.; Roulaud, M.; Naiditch, N.; Lorgeoux, B.; Baron, S.; et al. Finite Mixture Models Based on Pain Intensity, Functional Disability and Psychological Distress Composite Assessment Allow Identification of Two Distinct Classes of Persistent Spinal Pain Syndrome after Surgery Patients Related to Their Quality of Life. J. Clin. Med. 2021, 10, 4676. [Google Scholar] [CrossRef]
- Rigoard, P.; Ounajim, A.; Goudman, L.; Louis, P.-Y.; Slaoui, Y.; Roulaud, M.; Naiditch, N.; Bouche, B.; Page, P.; Lorgeoux, B.; et al. A Novel Multi-Dimensional Clinical Response Index Dedicated to Improving Global Assessment of Pain in Patients with Persistent Spinal Pain Syndrome after Spinal Surgery, Based on a Real-Life Prospective Multicentric Study (PREDIBACK) and Machine Learning Techniques. J. Clin. Med. 2021, 10, 4910. [Google Scholar] [CrossRef]
- Duarte, R.V.; Nevitt, S.; McNicol, E.; Taylor, R.S.; Buchser, E.; North, R.B.; Eldabe, S. Systematic Review and Meta-Analysis of Placebo/Sham Controlled Randomised Trials of Spinal Cord Stimulation for Neuropathic Pain. Pain 2020, 161, 24–35. [Google Scholar] [CrossRef]
- Deer, T.R.; Grider, J.S.; Lamer, T.J.; Pope, J.E.; Falowski, S.; Hunter, C.W.; Provenzano, D.A.; Slavin, K.V.; Russo, M.; Carayannopoulos, A.; et al. A Systematic Literature Review of Spine Neurostimulation Therapies for the Treatment of Pain. Pain Med. 2020, 21, 1421–1432. [Google Scholar] [CrossRef]
- Rigoard, P.; Billot, M.; Ingrand, P.; Durand-Zaleski, I.; Roulaud, M.; Peruzzi, P.; Dam Hieu, P.; Voirin, J.; Raoul, S.; Page, P.; et al. How Should We Use Multicolumn Spinal Cord Stimulation to Optimize Back Pain Spatial Neural Targeting? A Prospective, Multicenter, Randomized, Double-Blind, Controlled Trial (ESTIMET Study). Neuromodulation Technol. Neural Interface 2021, 24, 86–101. [Google Scholar] [CrossRef]
- Rigoard, P.; Basu, S.; Desai, M.; Taylor, R.; Annemans, L.; Tan, Y.; Johnson, M.J.; Van den Abeele, C.; North, R.; PROMISE. Study Group Multicolumn Spinal Cord Stimulation for Predominant Back Pain in Failed Back Surgery Syndrome Patients: A Multicenter Randomized Controlled Trial. Pain 2019, 160, 1410–1420. [Google Scholar] [CrossRef]
- Kumar, K.; Taylor, R.S.; Jacques, L.; Eldabe, S.; Meglio, M.; Molet, J.; Thomson, S.; O’Callaghan, J.; Eisenberg, E.; Milbouw, G.; et al. Spinal Cord Stimulation versus Conventional Medical Management for Neuropathic Pain: A Multicentre Randomised Controlled Trial in Patients with Failed Back Surgery Syndrome. Pain 2007, 132, 179–188. [Google Scholar] [CrossRef]
- North, R.B.; Kidd, D.H.; Farrokhi, F.; Piantadosi, S.A. Spinal Cord Stimulation versus Repeated Lumbosacral Spine Surgery for Chronic Pain: A Randomized, Controlled Trial. Neurosurgery 2005, 56, 98–106, discussion 106–107. [Google Scholar] [CrossRef]
- Christelis, N.; Simpson, B.; Russo, M.; Stanton-Hicks, M.; Barolat, G.; Thomson, S.; Schug, S.; Baron, R.; Buchser, E.; Carr, D.B.; et al. Persistent Spinal Pain Syndrome: A Proposal for Failed Back Surgery Syndrome and ICD-11. Pain Med. 2021, 22, 807–818. [Google Scholar] [CrossRef]
- Rigoard, P.; Delmotte, A.; D’Houtaud, S.; Misbert, L.; Diallo, B.; Roy-Moreau, A.; Durand, S.; Royoux, S.; Giot, J.-P.; Bataille, B. Back Pain: A Real Target for Spinal Cord Stimulation? Neurosurgery 2012, 70, 574–584, discussion 584–585. [Google Scholar] [CrossRef]
- Goudman, L.; Rigoard, P.; Billot, M.; Duarte, R.V.; Eldabe, S.; Moens, M. Patient Selection for Spinal Cord Stimulation in Treatment of Pain: Sequential Decision-Making Model—A Narrative Review. J. Pain Res. 2022, 15, 1163–1171. [Google Scholar] [CrossRef]
- Taylor, R.S.; Taylor, R.J.; Van Buyten, J.-P.; Buchser, E.; North, R.; Bayliss, S. The Cost Effectiveness of Spinal Cord Stimulation in the Treatment of Pain: A Systematic Review of the Literature. J. Pain Symptom Manag. 2004, 27, 370–378. [Google Scholar] [CrossRef]
- Taylor, R.S.; Van Buyten, J.-P.; Buchser, E. Spinal Cord Stimulation for Chronic Back and Leg Pain and Failed Back Surgery Syndrome: A Systematic Review and Analysis of Prognostic Factors. Spine 2005, 30, 152–160. [Google Scholar] [CrossRef]
- Taylor, R.S. Spinal Cord Stimulation in Complex Regional Pain Syndrome and Refractory Neuropathic Back and Leg Pain/Failed Back Surgery Syndrome: Results of a Systematic Review and Meta-Analysis. J. Pain Symptom Manag. 2006, 31, S13–S19. [Google Scholar] [CrossRef]
- Deer, T.; Slavin, K.V.; Amirdelfan, K.; North, R.B.; Burton, A.W.; Yearwood, T.L.; Tavel, E.; Staats, P.; Falowski, S.; Pope, J.; et al. Success Using Neuromodulation With BURST (SUNBURST) Study: Results From a Prospective, Randomized Controlled Trial Using a Novel Burst Waveform. Neuromodulation Technol. Neural Interface 2018, 21, 56–66. [Google Scholar] [CrossRef]
- Deer, T.R.; Grigsby, E.; Weiner, R.L.; Wilcosky, B.; Kramer, J.M. A Prospective Study of Dorsal Root Ganglion Stimulation for the Relief of Chronic Pain. Neuromodulation 2013, 16, 67–71, discussion 71–72. [Google Scholar] [CrossRef]
- Goudman, L.; De Smedt, A.; Eldabe, S.; Rigoard, P.; Linderoth, B.; De Jaeger, M.; Moens, M.; Discover Consortium. High-Dose Spinal Cord Stimulation for Patients with Failed Back Surgery Syndrome: A Multicenter Effectiveness and Prediction Study. Pain 2021, 162, 582–590. [Google Scholar] [CrossRef]
- Rigoard, P.; Ounajim, A.; Goudman, L.; Banor, T.; Héroux, F.; Roulaud, M.; Babin, E.; Bouche, B.; Page, P.; Lorgeoux, B.; et al. The Challenge of Converting “Failed Spinal Cord Stimulation Syndrome” Back to Clinical Success, Using SCS Reprogramming as Salvage Therapy, through Neurostimulation Adapters Combined with 3D-Computerized Pain Mapping Assessment: A Real Life Retrospective Study. J. Clin. Med. 2022, 11, 272. [Google Scholar] [CrossRef]
- Billot, M.; Naiditch, N.; Brandet, C.; Lorgeoux, B.; Baron, S.; Ounajim, A.; Roulaud, M.; Roy-Moreau, A.; de Montgazon, G.; Charrier, E.; et al. Comparison of Conventional, Burst and High-Frequency Spinal Cord Stimulation on Pain Relief in Refractory Failed Back Surgery Syndrome Patients: Study Protocol for a Prospective Randomized Double-Blinded Cross-over Trial (MULTIWAVE Study). Trials 2020, 21, 696. [Google Scholar] [CrossRef]
- Rigoard, P.; Ounajim, A.; Goudman, L.; Roulaud, M.; Lorgeoux, B.; Baron, S.; Nivole, K.; Many, M.; Johnson, S.; David, R.; et al. Which Waveform for Which Patient? A Prospective Randomized Double-Blinded Cross-over Trial Comparing Pain Relief Using Tonic, Burst and High Frequency in PSPS-T2 Patients Implanted with Spinal Cord Stimulation (MULTIWAVE Study). Neuromodulation Technol. Neural Interface 2022. Submitted. [Google Scholar]
- Linderoth, B.; Foreman, R.D. Physiology of Spinal Cord Stimulation: Review and Update. Neuromodulation Technol. Neural Interface 1999, 2, 150–164. [Google Scholar] [CrossRef]
- Linderoth, B.; Foreman, R.D. Conventional and Novel Spinal Stimulation Algorithms: Hypothetical Mechanisms of Action and Comments on Outcomes. Neuromodulation Technol. Neural Interface 2017, 20, 525–533. [Google Scholar] [CrossRef]
- Goudman, L.; De Groote, S.; Linderoth, B.; De Smedt, A.; Eldabe, S.; Duarte, R.V.; Moens, M. Exploration of the Supraspinal Hypotheses about Spinal Cord Stimulation and Dorsal Root Ganglion Stimulation: A Systematic Review. J. Clin. Med. 2021, 10, 2766. [Google Scholar] [CrossRef]
- De Ridder, D.; Vanneste, S. Burst and Tonic Spinal Cord Stimulation: Different and Common Brain Mechanisms. Neuromodulation Technol. Neural Interface 2016, 19, 47–59. [Google Scholar] [CrossRef]
- Veizi, E.; Hayek, S.M.; North, J.; Chafin, T.B.; Yearwood, T.L.; Raso, L.; Frey, R.; Cairns, K.; Berg, A.; Brendel, J.; et al. Spinal Cord Stimulation (SCS) with Anatomically Guided (3D) Neural Targeting Shows Superior Chronic Axial Low Back Pain Relief Compared to Traditional SCS-LUMINA Study. Pain Med. 2017, 18, 1534–1548. [Google Scholar] [CrossRef]
- Wood, C.; Martiné, G.; Espagne-Dubreuilh, G.; Le Goff, K.; Moens, M.; Goudman, L.; Baron, S.; David, R.; Naïditch, N.; Billot, M.; et al. The Added Value of Intraoperative Hypnosis during Spinal Cord Stimulation Lead Implantation under Awake Anesthesia in Patients Presenting with Refractory Chronic Pain. Medicina 2022, 58, 220. [Google Scholar] [CrossRef]
- Wager, M.; Rigoard, P.; Bouyer, C.; Baudiffier, V.; Stal, V.; Bataille, B.; Gil, R.; Du Boisgueheneuc, F. Operating Environment for Awake Brain Surgery—Choice of Tests. Neurochirurgie 2017, 63, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Wager, M.; Rigoard, P.; Bataille, B.; Guenot, C.; Supiot, A.; Blanc, J.-L.; Stal, V.; Pluchon, C.; Bouyer, C.; Gil, R.; et al. Designing an Operating Theatre for Awake Procedures: A Solution to Improve Multimodality Information Input. Br. J. Neurosurg. 2015, 29, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Monlezun, O.; Voirin, J.; Roulaud, M.; Ingrand, P.; Veyrieras, C.; Brandet, C.; Bataille, B.; Guetarni, F.; Prévost, A.; Rigoard, P.; et al. “MAST” Prospective Study: Value of Minimal Access Spine Technologies Technique for Multicolumn Spinal Cord Stimulation Surgical Lead Implantation in the Context of a French Multicentre Randomized Controlled Trial (ESTIMET Study). Neurochirurgie 2015, 61 (Suppl. 1), S125–S130. [Google Scholar] [CrossRef] [PubMed]
- Rigoard, P.; Luong, A.T.; Delmotte, A.; Raaholt, M.; Roulaud, M.; Monlezun, O.; Triphose, A.; Guetarni, F.; Brugière, B.; Misbert, L.; et al. Multicolumn Spinal Cord Stimulation Lead Implantation Using an Optic Transligamentar Minimally Invasive Technique. Neurosurgery 2013, 73, 550–553. [Google Scholar] [CrossRef]
- Guetarni, F.; Rigoard, P. The “Neuro-Mapping Locator” Software. A Real-Time Intraoperative Objective Paraesthesia Mapping Tool to Evaluate Paraesthesia Coverage of the Painful Zone in Patients Undergoing Spinal Cord Stimulation Lead Implantation. Neurochirurgie 2015, 61 (Suppl. 1), S90–S98. [Google Scholar] [CrossRef] [PubMed]
- Rigoard, P.; Nivole, K.; Blouin, P.; Monlezun, O.; Roulaud, M.; Lorgeoux, B.; Bataille, B.; Guetarni, F. A Novel, Objective, Quantitative Method of Evaluation of the Back Pain Component Using Comparative Computerized Multi-Parametric Tactile Mapping before/after Spinal Cord Stimulation and Database Analysis: The “Neuro-Pain’t” Software. Neurochirurgie 2015, 61 (Suppl. 1), S99–S108. [Google Scholar] [CrossRef]
- Rigoard, P.; Ounajim, A.; Goudman, L.; Bouche, B.; Roulaud, M.; Page, P.; Lorgeoux, B.; Baron, S.; Nivole, K.; Many, M.; et al. The Added Value of Subcutaneous Peripheral Nerve Field Stimulation Combined with SCS, as Salvage Therapy, for Refractory Low Back Pain Component in Persistent Spinal Pain Syndrome Implanted Patients: A Randomized Controlled Study (CUMPNS Study) Based on 3D-Mapping Composite Pain Assessment. J. Clin. Med. 2021, 10, 5094. [Google Scholar] [CrossRef]
- Roulaud, M.; Durand-Zaleski, I.; Ingrand, P.; Serrie, A.; Diallo, B.; Peruzzi, P.; Hieu, P.D.; Voirin, J.; Raoul, S.; Page, P.; et al. Multicolumn Spinal Cord Stimulation for Significant Low Back Pain in Failed Back Surgery Syndrome: Design of a National, Multicentre, Randomized, Controlled Health Economics Trial (ESTIMET Study). Neurochirurgie 2015, 61 (Suppl. 1), S109–S116. [Google Scholar] [CrossRef] [PubMed]
- Deer, T.R.; Russo, M.A.; Grider, J.S.; Pope, J.; Rigoard, P.; Hagedorn, J.M.; Naidu, R.; Patterson, D.G.; Wilson, D.; Lubenow, T.R.; et al. The Neurostimulation Appropriateness Consensus Committee (NACC): Recommendations for Surgical Technique for Spinal Cord Stimulation. Neuromodulation Technol. Neural Interface 2022, 25, 1–34. [Google Scholar] [CrossRef]
- Quinones-Hinojosa, A. Schmidek and Sweet: Operative Neurosurgical Techniques E-Book: Indications, Methods and Results; Elsevier Health Sciences: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Rigoard, P.; Moens, M.; Goudman, L.; Le Tutor, T.; Dany, J.; Et Talby, M.; Hervochon, R.; Roulaud, M.; Ounajim, A.; Frasca, D.; et al. The “Neuro-Fiber-Mapping”: An Original Concept of Spinal Cord Neural Activation Spatial Targeting Using Live Electrostimulation Mapping to (Re)Explore the Conus Medullaris Anatomy. IJERPH 2022. Submitted. [Google Scholar]
- Rigoard, P.; Roulaud, M.; Goudman, L.; Adjali, N.; Ounajim, A.; Voirin, J.; Perruchoud, C.; Bouche, B.; Page, P.; Guillevin, R.; et al. Comparison of Spinal Cord Stimulation vs. Dorsal Root Ganglion Stimulation vs. Association of Both in Patients with Refractory Chronic Back and/or Lower Limb Neuropathic Pain: An International, Prospective, Randomized, Double-Blinded, Crossover Trial (BOOST-DRG Study). Medicina 2021, 58, 7. [Google Scholar] [CrossRef]
- Goudman, L.; Billot, M.; Duarte, R.V.; Eldabe, S.; Rigoard, P.; Moens, M. Gradation of Clinical Holistic Response as New Composite Outcome to Evaluate Success in Spinal Cord Stimulation Studies for Pain. Neuromodulation Technol. Neural Interface 2021, S1094–S7159. [Google Scholar] [CrossRef]
- Dhall, S.S.; Wang, M.Y.; Mummaneni, P.V. Clinical and Radiographic Comparison of Mini-Open Transforaminal Lumbar Interbody Fusion with Open Transforaminal Lumbar Interbody Fusion in 42 Patients with Long-Term Follow-Up. J. Neurosurg. Spine 2008, 9, 560–565. [Google Scholar] [CrossRef]
- Holly, L.T.; Schwender, J.D.; Rouben, D.P.; Foley, K.T. Minimally Invasive Transforaminal Lumbar Interbody Fusion: Indications, Technique, and Complications. Neurosurg. Focus 2006, 20, E6. [Google Scholar] [CrossRef]
- Park, Y.; Ha, J.W. Comparison of One-Level Posterior Lumbar Interbody Fusion Performed with a Minimally Invasive Approach or a Traditional Open Approach. Spine 2007, 32, 537–543. [Google Scholar] [CrossRef]
- Park, P.; Foley, K.T. Minimally Invasive Transforaminal Lumbar Interbody Fusion with Reduction of Spondylolisthesis: Technique and Outcomes after a Minimum of 2 Years’ Follow-Up. Neurosurg. Focus 2008, 25, E16. [Google Scholar] [CrossRef]
- Rahman, M.; Summers, L.E.; Richter, B.; Mimran, R.I.; Jacob, R.P. Comparison of Techniques for Decompressive Lumbar Laminectomy: The Minimally Invasive versus the “Classic” Open Approach. Minim. Invasive Neurosurg. 2008, 51, 100–105. [Google Scholar] [CrossRef]
- Schwender, J.D.; Holly, L.T.; Rouben, D.P.; Foley, K.T. Minimally Invasive Transforaminal Lumbar Interbody Fusion (TLIF): Technical Feasibility and Initial Results. J. Spinal Disord. Tech. 2005, 18, S1–S6. [Google Scholar] [CrossRef]
- Falowski, S.M.; Sharan, A.; McInerney, J.; Jacobs, D.; Venkatesan, L.; Agnesi, F. Nonawake vs. Awake Placement of Spinal Cord Stimulators: A Prospective, Multicenter Study Comparing Safety and Efficacy. Neurosurgery 2019, 84, 198–205. [Google Scholar] [CrossRef]
- Gewandter, J.S.; McDermott, M.P.; Evans, S.; Katz, N.P.; Markman, J.D.; Simon, L.S.; Turk, D.C.; Dworkin, R.H. Composite Outcomes for Pain Clinical Trials: Considerations for Design and Interpretation. Pain 2021, 162, 1899–1905. [Google Scholar] [CrossRef]
- Delmotte, A.; Jacques, L.; Kumar, K.; Poon, K.; Monlezun, O.; Roulaud, M.; Prevost, A.; Munson, R.; Guetarni, F.; Bataille, B.; et al. The Franco-Canadian Multicolumn Spinal Cord Stimulation Prospective Study: A Subgroup Analysis Focusing on the Decisive Role of Lead Positioning. Neurochirurgie 2015, 61 (Suppl. 1), S83–S89. [Google Scholar] [CrossRef]
- Bendersky, D.; Yampolsky, C. Is Spinal Cord Stimulation Safe? A Review of Its Complications. World Neurosurg. 2014, 82, 1359–1368. [Google Scholar] [CrossRef]
- Mekhail, N.; Levy, R.M.; Deer, T.R.; Kapural, L.; Li, S.; Amirdelfan, K.; Hunter, C.W.; Rosen, S.M.; Costandi, S.J.; Falowski, S.M.; et al. Long-Term Safety and Efficacy of Closed-Loop Spinal Cord Stimulation to Treat Chronic Back and Leg Pain (Evoke): A Double-Blind, Randomised, Controlled Trial. Lancet Neurol. 2020, 19, 123–134. [Google Scholar] [CrossRef]
- North, R.; Desai, M.J.; Vangeneugden, J.; Raftopoulos, C.; Van Havenbergh, T.; Deruytter, M.; Remacle, J.-M.; Shipley, J.; Tan, Y.; Johnson, M.J.; et al. Postoperative Infections Associated With Prolonged Spinal Cord Stimulation Trial Duration (PROMISE RCT). Neuromodulation Technol. Neural Interface 2020, 23, 620–625. [Google Scholar] [CrossRef]
- Falowski, S.M.; Celii, A.; Sestokas, A.K.; Schwartz, D.M.; Matsumoto, C.; Sharan, A. Awake vs. Asleep Placement of Spinal Cord Stimulators: A Cohort Analysis of Complications Associated with Placement. Neuromodulation Technol. Neural Interface 2011, 14, 130–134, discussion 134–135. [Google Scholar] [CrossRef] [PubMed]
- García-Pérez, M.L.; Badenes, R.; García-March, G.; Bordes, V.; Belda, F.J. Epidural Anesthesia for Laminectomy Lead Placement in Spinal Cord Stimulation. Anesth. Analg. 2007, 105, 1458–1461. [Google Scholar] [CrossRef]
- Lind, G.; Meyerson, B.A.; Winter, J.; Linderoth, B. Implantation of Laminotomy Electrodes for Spinal Cord Stimulation in Spinal Anesthesia with Intraoperative Dorsal Column Activation. Neurosurgery 2003, 53, 1150–1153, discussion 1153–1154. [Google Scholar] [CrossRef]
- Garcia, R.; Bouleti, C.; Li, A.; Frasca, D.; El Harrouchi, S.; Marechal, J.; Roumegou, P.; Corbi, P.; Christiaens, L.; Le Gal, F.; et al. Hypnosis Versus Placebo During Atrial Flutter Ablation: The PAINLESS Study: A Randomized Controlled Trial. JACC Clin. Electrophysiol. 2020, 6, 1551–1560. [Google Scholar] [CrossRef] [PubMed]
- Noergaard, M.W.; Håkonsen, S.J.; Bjerrum, M.; Pedersen, P.U. The Effectiveness of Hypnotic Analgesia in the Management of Procedural Pain in Minimally Invasive Procedures: A Systematic Review and Meta-Analysis. J. Clin. Nurs. 2019, 28, 4207–4224. [Google Scholar] [CrossRef] [PubMed]
- Billot, M.; Wood, C.; Moens, M.; Goudman, L.; Naiditch, N.; Roulaud, M.; Ounajim, A.; Rigoard, P. The Added Value of Intraoperative Hypnosis for Refractory Pain Patients Implanted with Spinal Cord Stimulation under Awake Conditions: A Retrospective Cohort Study. IJERPH 2022. Submitted. [Google Scholar]
- Mosso-Vázquez, J.L.; Gao, K.; Wiederhold, B.K.; Wiederhold, M.D. Virtual Reality for Pain Management in Cardiac Surgery. Cyberpsychology Behav. Soc. Netw. 2014, 17, 371–378. [Google Scholar] [CrossRef]
- Sweta, V.R.; Abhinav, R.P.; Ramesh, A. Role of Virtual Reality in Pain Perception of Patients Following the Administration of Local Anesthesia. Ann. Maxillofac. Surg. 2019, 9, 110–113. [Google Scholar] [CrossRef]
- Hoffman, H.G.; Chambers, G.T.; Meyer, W.J.; Arceneaux, L.L.; Russell, W.J.; Seibel, E.J.; Richards, T.L.; Sharar, S.R.; Patterson, D.R. Virtual Reality as an Adjunctive Non-Pharmacologic Analgesic for Acute Burn Pain During Medical Procedures. Ann. Behav. Med. 2011, 41, 183–191. [Google Scholar] [CrossRef]
- Hoxhallari, E.; Behr, I.J.; Bradshaw, J.S.; Morkos, M.S.; Haan, P.S.; Schaefer, M.C.; Clarkson, J.H.W. Virtual Reality Improves the Patient Experience during Wide-Awake Local Anesthesia No Tourniquet Hand Surgery: A Single-Blind, Randomized, Prospective Study. Plast. Reconstr. Surg. 2019, 144, 408–414. [Google Scholar] [CrossRef]
- Vangeneugden, J. Implantation of Surgical Electrodes for Spinal Cord Stimulation: Classical Midline Laminotomy Technique versus Minimal Invasive Unilateral Technique Combined with Spinal Anaesthesia. Acta Neurochir. 2007, 97, 111–114. [Google Scholar] [CrossRef]
- Zhao, Z.; Ahmadi, A.; Hoover, C.; Grado, L.; Peterson, N.; Wang, X.; Freeman, D.; Murray, T.; Lamperski, A.; Darrow, D.; et al. Optimization of Spinal Cord Stimulation Using Bayesian Preference Learning and Its Validation. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 1987–1997. [Google Scholar] [CrossRef]
- Bennett, G.J.; Xie, Y.-K. A Peripheral Mononeuropathy in Rat That Produces Disorders of Pain Sensation like Those Seen in Man. Pain 1988, 33, 87–107. [Google Scholar] [CrossRef]
- National Institute for Health and Clinical Excellence (Great Britain) Spinal Cord Stimulation for Chronic Pain of Neuropathic or Ischaemic Origin|Guidance|NICE. Available online: https://www.nice.org.uk/guidance/ta159/informationforpublic (accessed on 24 August 2022).
- Centers for Medicare & Medicaid Services National Coverage Determination (NCD) Electrical Nerve Stimulators. 100-3. 160.7. Available online: https://www.cms.gov/medicare-coverage-database/view/ncd.aspx?NCDId=240 (accessed on 24 August 2022).
- Haute Autorité de Santé BON USAGE DES TECHNOLOGIES DE SANTÉ—Neurostimulateurs Médullaires Implantables: Une Technique de Dernier Recours. Available online: https://www.has-sante.fr/plugins/ModuleXitiKLEE/types/FileDocument/doXiti.jsp?id=c_1734189 (accessed on 20 July 2022).
- Eldabe, S.; Duarte, R.V.; Gulve, A.; Thomson, S.; Baranidharan, G.; Houten, R.; Jowett, S.; Sandhu, H.; Chadwick, R.; Brookes, M.; et al. Does a Screening Trial for Spinal Cord Stimulation in Patients with Chronic Pain of Neuropathic Origin Have Clinical Utility and Cost-Effectiveness (TRIAL-STIM)? A Randomised Controlled Trial. Pain 2020, 161, 2820–2829. [Google Scholar] [CrossRef]
- Ounajim, A.; Billot, M.; Goudman, L.; Louis, P.-Y.; Slaoui, Y.; Roulaud, M.; Bouche, B.; Page, P.; Lorgeoux, B.; Baron, S.; et al. Machine Learning Algorithms Provide Greater Prediction of Response to SCS Than Lead Screening Trial: A Predictive AI-Based Multicenter Study. J. Clin. Med. 2021, 10, 4764. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| KERRYPNX | MISAA Group n = 23 | MISGA Group n = 52 | LGA Group n = 33 | p-Value of the Difference |
|---|---|---|---|---|
| Age (years) | 46.4 ± 7.6 | 46.2 ± 9.4 | 50.7 ± 9.5 | 0.21 |
| Sex male/female n (%) | 9/14 (39.1%) | 26/26 (50%) | 17/16 (51.5%) | 0.62 |
| BMI (kg/m²) | 26.7 ± 4.3 | 26.8 ± 4.7 | 28.0 ± 6.3 | 0.72 |
| Pain duration (years) | 11.7 ± 9.2 | 11.3 ± 9.7 | 12.8 ± 12.5 | 0.8 |
| Global VAS (mm) | 71.5 ± 13.3 | 76.0 ± 11.5 | 75.7 ± 14.2 | 0.33 |
| Back pain VAS (mm) | 71.1 ± 18.1 | 74.1 ± 16.9 | 75.9 ± 14.8 | 0.62 |
| Leg pain VAS (mm) | 75.7 ± 9.0 | 78.7 ± 11.1 | 73.9 ± 15.1 | 0.20 |
| Pain surface in cm² (median (IQR)) | 522.7 (921.6) | 807 (969.5) | 503.4 (924.6) | 0.12 |
| Patients with predominant back pain back/leg n (%) | 9/14 (39.1%) | 15/37 (28.8%) | 15/18 (45.5%) | 0.28 |
| Patients with a neuropathic component (%) | ||||
| Back pain n (%) | 13/10 (56.5%) | 29/23 (55.8%) | 18/15 (56.3%) | 0.99 |
| Leg pain n (%) | 22/1 (95.7%) | 52/0 (100%) | 33/0 (100%) | 0.21 |
| Number of previous spinal surgeries (median (min–max)) | 1 (1–3) | 2 (1–5) | 2 (1–5) | 0.026 |
| MADRS depression score | 20.0 ± 9.8 | 14.1 ± 9.7 | 21.3 ± 11.8 | 0.005 |
| BAS anxiety score | 19.5 ± 8.2 | 17.7 ± 8.1 | 18.3 ± 6.5 | 0.57 |
| MISAA Group n = 23 | MISGA Group n = 52 | LGA Group n = 33 | p-Value of the Difference | |
|---|---|---|---|---|
| Vertebral level projection of the conus medullaris | 0.12 | |||
| T11-T12 | 0 (0%) | 5 (9.6%) | 0 (0%) | |
| T12-L1 | 15 (65.2%) | 28 (53.8%) | 25 (75.8%) | |
| L1-L2 | 8 (34.8%) | 16 (30.8%) | 7 (21.2%) | |
| L2-L3 | 0 (0%) | 0 (0%) | 1 (3.0%) | |
| Unknown | 0 (0%) | 3 (5.8%) | 0 (0%) | |
| Lead lateralization (Upper/lower) (n, %) | 0.003 | |||
| Right/Right | 2 (8.7%) | 9 (17.3%) | 1 (3.0%) | |
| Right/Left | 0 (0%) | 0 (0%) | 1 (3.0%) | |
| Right/Midline | 7 (30.5%) | 3 (5.8%) | 6 (18.2%) | |
| Left/Right | 0 (0%) | 0 (0%) | 0 (0%) | |
| Left/Left | 0 (0%) | 5 (9.6%) | 1 (3.0%) | |
| Left/Midline | 5 (21.7%) | 3 (5.8%) | 1 (3.0%) | |
| Midline/Right | 1 (4.3%) | 0 (0%) | 1 (3.0%) | |
| Midline/Left | 3 (13.0%) | 3 (5.8%) | 0 (0%) | |
| Midline/Midline | 5 (21.7%) | 29 (55.8%) | 20 (60.6%) | |
| Unknown | 0 (0%) | 0 (0%) | 2 (6.1%) | |
| Vertebral level projection of the central contact “number 8” of the 5-6-5 lead. | 0.32 | |||
| T11 | 1 (4.3%) | 1 (1.9%) | 0 (0%) | |
| T10 | 2 (8.7%) | 8 (15.4%) | 5 (15.2%) | |
| T9 | 16 (69.6%) | 22 (42.3%) | 14 (42.4%) | |
| T8 | 4 (17.4%) | 15 (28.8%) | 9 (27.3%) | |
| T7 | 0 (0%) | 6 (11.5%) | 1 (3%) | |
| T6 | 0 (0%) | 0 (0%) | 1 (3%) | |
| Unknown | 0 (0%) | 0 (0%) | 3 (9.1%) | |
| IPG type | 0.0006 | |||
| Non rechargeable | 16 (69.6%) | 23 (44.2%) | 26 (78.8%) | |
| Rechargeable | 7 (30.4%) | 28 (53.8%) | 4 (12.1%) | |
| Not implanted permanently | 0 (0%) | 1 (1.9%) | 3 (9.1%) |
| Follow-Up Visits | MISAA Group | MISGA Group | LGA Group | Adjusted p-Value * |
|---|---|---|---|---|
| 1-month | n = 22 | n = 50 | n = 28 | |
| Paresthesia coverage (%) Selectivity (%) % of pain surface decrease | 66.0% ± 34.6% a 31.2% ± 28.0% 76.2% ± 30.5% a | 41.6% ± 34.0% b 53.6% ± 38.3% 54.0% ± 38.1% b | 37.8% ± 33.0% b 41.3% ± 37.8% 56.3% ± 41.4% a,b | 0.010 0.11 0.038 |
| 3-month | n = 22 | n = 50 | n = 28 | |
| Paresthesia coverage (%) Selectivity (%) % of pain surface decrease | 65.1% ± 33.7% a 30.8% ± 27.2% a 68.5% ± 38.6% a | 43.8% ± 31.8% b 59.4% ± 33.4% b 44.0% ± 37.8% b | 36.5% ± 36.0% b 42.4% ± 37.1% a,b 57.8% ± 34.6% a,b | 0.014 0.011 0.019 |
| 6-month | n = 22 | n = 50 | n = 28 | |
| Paresthesia coverage (%) Selectivity (%) % of pain surface decrease | 65.3% ± 38.2% a 26.5% ± 23.7% a 50.5% ± 44.4% | 56.5% ± 32.1% a 61.8% ± 33.6% b 53.1% ± 41.7% | 33.8% ± 31.9% b 37.2% ± 36.6% a 50.3% ± 38.4% | 0.0033 0.0008 0.9 |
| 12-month | n = 22 | n = 48 | n = 27 | |
| Paresthesia coverage (%) Selectivity (%) % of pain surface decrease | 64.1% ± 36.7% a 27.5% ± 22.7% a 64.6% ± 40.3% | 51.1% ± 34.5% a,b 55.3% ± 36.0% b 61.3% ± 34.8% | 36.6% ± 37.4% b 30.1% ± 34.9% a 51.6% ± 42.4% | 0.032 0.011 0.42 |
| Clinical Outcomes at the 6-Month Follow-Up | MISAA Group n = 22 | MISGA Group n = 50 | LGA Group n = 28 | Adjusted p-Value * |
|---|---|---|---|---|
| % of decrease in global VAS % of decrease in back VAS % of decrease in leg VAS % of decrease in ODI Absolute increase in EQ-5D-3L Absolute decrease in MADRS | 60.4% ± 31.9% a 52.6% ± 35.6% a 79.0% ± 22.3% a 44.4% ± 32.5% a 0.31 ± 0.19 a 12.3 ± 12.0 a | 45.5% ± 32.8% a,b 43.2% ± 34.1% a,b 55.7% ± 34.3% b,a 26.8% ± 34.0% a,b 0.14 ± 0.25 a,b 1.8 ± 7.2 b,a | 35.4% ± 39.4% b 18.9% ± 39.3% b 54.2% ± 44.2% b 22.3% ± 25.4% b 0.17 ± 0.26 b 3.5 ± 10.2 a | 0.047 0.0037 0.016 0.028 0.039 0.0003 |
| Clinical outcomes at the 12-month follow-up | MISAA group n = 22 | MISGA group n = 48 | LGA group n = 27 | Adjusted p-value * |
| % of decrease in global VAS % of decrease in back VAS % of decrease in leg VAS % of decrease in ODI Absolute increase in EQ-5D-3L Absolute decrease in MADRS | 59.0% ± 31.7% a 55.9% ± 38.0% a 73.5% ± 26.5% a 48.0% ± 28.3% a 0.26 ± 0.16 a 12.2 ± 9.4 a | 44.0% ± 36.2% a 42.7% ± 39.0% a 52.9% ± 31.7% b 27.5% ± 36.5% a,b 0.12 ± 0.27 b 2.9 ± 9.9 b | 35.9% ± 38.1% a 27.7% ± 44.0% a 46.4% ± 36.7% b 31.4% ± 28.8% b 0.25 ± 0.22 a 6.5 ± 10.5 a | 0.076 0.080 0.012 0.033 0.015 0.0005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rigoard, P.; Ounajim, A.; Goudman, L.; Wood, C.; Roulaud, M.; Page, P.; Lorgeoux, B.; Baron, S.; Nivole, K.; Many, M.; et al. Combining Awake Anesthesia with Minimal Invasive Surgery Optimizes Intraoperative Surgical Spinal Cord Stimulation Lead Placement. J. Clin. Med. 2022, 11, 5575. https://doi.org/10.3390/jcm11195575
Rigoard P, Ounajim A, Goudman L, Wood C, Roulaud M, Page P, Lorgeoux B, Baron S, Nivole K, Many M, et al. Combining Awake Anesthesia with Minimal Invasive Surgery Optimizes Intraoperative Surgical Spinal Cord Stimulation Lead Placement. Journal of Clinical Medicine. 2022; 11(19):5575. https://doi.org/10.3390/jcm11195575
Chicago/Turabian StyleRigoard, Philippe, Amine Ounajim, Lisa Goudman, Chantal Wood, Manuel Roulaud, Philippe Page, Bertille Lorgeoux, Sandrine Baron, Kevin Nivole, Mathilde Many, and et al. 2022. "Combining Awake Anesthesia with Minimal Invasive Surgery Optimizes Intraoperative Surgical Spinal Cord Stimulation Lead Placement" Journal of Clinical Medicine 11, no. 19: 5575. https://doi.org/10.3390/jcm11195575
APA StyleRigoard, P., Ounajim, A., Goudman, L., Wood, C., Roulaud, M., Page, P., Lorgeoux, B., Baron, S., Nivole, K., Many, M., Cuny, E., Voirin, J., Fontaine, D., Raoul, S., Mertens, P., Peruzzi, P., Caire, F., Buisset, N., David, R., ... Billot, M. (2022). Combining Awake Anesthesia with Minimal Invasive Surgery Optimizes Intraoperative Surgical Spinal Cord Stimulation Lead Placement. Journal of Clinical Medicine, 11(19), 5575. https://doi.org/10.3390/jcm11195575