

Multiple Drilling with Recombinant Human Bone Morphogenetic Protein-2 in Korean Patients with Non-Traumatic Osteonecrosis of the Femoral Head: A Prospective Randomized Pilot Study with a Minimum Two-Year Follow-Up

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants Selection
2.2. Trial Design
2.3. Trial Intervention
2.4. Study End Points
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mont, M.A.; Zywiel, M.G.; Marker, D.R.; McGrath, M.S.; Delanois, R.E. The natural history of untreated asymptomatic osteonecrosis of the femoral head: A systematic literature review. J. Bone Jt. Surg. Am. 2010, 92, 2165–2170. [Google Scholar] [CrossRef]
- Mont, M.A.; Salem, H.S.; Piuzzi, N.S.; Goodman, S.B.; Jones, L.C. Nontraumatic osteonecrosis of the femoral head: Where do we stand today?: A 5-year update. J. Bone Jt. Surg. Am. 2020, 102, 1084–1099. [Google Scholar] [CrossRef]
- Moya-Angeler, J.; Gianakos, A.L.; Villa, J.C.; Ni, A.; Lane, J.M. Current concepts on osteonecrosis of the femoral head. World J. Orthop. 2015, 6, 590–601. [Google Scholar] [CrossRef]
- Ikeuchi, K.; Hasegawa, Y.; Seki, T.; Takegami, Y.; Amano, T.; Ishiguro, N. Epidemiology of nontraumatic osteonecrosis of the femoral head in Japan. Mod. Rheumatol. 2015, 25, 278–281. [Google Scholar] [CrossRef]
- Kang, J.S.; Moon, K.H.; Kwon, D.G.; Shin, B.K.; Woo, M.S. The natural history of asymptomatic osteonecrosis of the femoral head. Int. Orthop. 2013, 37, 379–384. [Google Scholar] [CrossRef]
- Atilla, B.; Bakırcıoğlu, S.; Shope, A.J.; Parvızı, J. Joint-preserving procedures for osteonecrosis of the femoral head. EFORT Open Rev. 2019, 4, 647–658. [Google Scholar] [CrossRef]
- Larson, E.; Jones, L.C.; Goodman, S.B.; Koo, K.H.; Cui, Q. Early-stage osteonecrosis of the femoral head: Where are we and where are we going in year 2018? Int. Orthop. 2018, 42, 1723–1728. [Google Scholar] [CrossRef]
- Cui, Q.; Jo, W.L.; Koo, K.H.; Cheng, E.Y.; Drescher, W.; Goodman, S.B.; Ha, Y.C.; Hernigou, P.; Jones, L.C.; Kim, S.Y.; et al. Arco consensus on the pathogenesis of non-traumatic osteonecrosis of the femoral head. J. Korean Med. Sci. 2021, 36, e65. [Google Scholar] [CrossRef]
- Petek, D.; Hannouche, D.; Suva, D. Osteonecrosis of the femoral head: Pathophysiology and current concepts of treatment. EFORT Open Rev. 2019, 4, 85–97. [Google Scholar] [CrossRef]
- Rezus, E.; Tamba, B.I.; Badescu, M.C.; Popescu, D.; Bratoiu, I.; Rezus, C. Osteonecrosis of the femoral head in patients with hypercoagulability-from pathophysiology to therapeutic implications. Int. J. Mol. Sci. 2021, 22, 6801. [Google Scholar] [CrossRef]
- Baig, S.A.; Baig, M.N. Osteonecrosis of the femoral head: Etiology, investigations, and management. Cureus 2018, 10, e3171. [Google Scholar] [CrossRef] [PubMed]
- Adesina, O.; Brunson, A.; Keegan, T.H.M.; Wun, T. Osteonecrosis of the femoral head in sickle cell disease: Prevalence, comorbidities, and surgical outcomes in california. Blood Adv. 2017, 1, 1287–1295. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Merchán, E.C. Effects of hemophilia on articulations of children and adults. Clin. Orthop. Relat. Res. 1996, 328, 7–13. [Google Scholar] [CrossRef]
- Simurda, T.; Kubisz, P.; Dobrotova, M.; Necas, L.; Stasko, J. Perioperative coagulation management in a patient with congenital afibrinogenemia during revision total hip arthroplasty. Semin. Thromb. Hemost. 2016, 42, 689–692. [Google Scholar]
- Thulasidhar, A.N.; Kumar, S.; Aroor, S.; Mundkur, S. Avascular necrosis of femoral head in a child with beta thalassaemia major. J. Clin. Diagn. Res. 2016, 10, Sl03. [Google Scholar] [CrossRef]
- Yoon, B.H.; Jones, L.C.; Chen, C.H.; Cheng, E.Y.; Cui, Q.; Drescher, W.; Fukushima, W.; Gangji, V.; Goodman, S.B.; Ha, Y.C.; et al. Etiologic classification criteria of arco on femoral head osteonecrosis part 1: Glucocorticoid-associated osteonecrosis. J. Arthroplast. 2019, 34, 163–168.e161. [Google Scholar] [CrossRef]
- Ficat, R.P. Idiopathic bone necrosis of the femoral head. Early diagnosis and treatment. J. Bone Jt. Surg. Br. 1985, 67, 3–9. [Google Scholar] [CrossRef]
- Hua, K.C.; Yang, X.G.; Feng, J.T.; Wang, F.; Yang, L.; Zhang, H.; Hu, Y.C. The efficacy and safety of core decompression for the treatment of femoral head necrosis: A systematic review and meta-analysis. J. Orthop. Surg. Res. 2019, 14, 306. [Google Scholar] [CrossRef]
- Roth, A.; Beckmann, J.; Bohndorf, K.; Fischer, A.; Heiß, C.; Kenn, W.; Jäger, M.; Maus, U.; Nöth, U.; Peters, K.M.; et al. S3-guideline non-traumatic adult femoral head necrosis. Arch. Orthop. Trauma Surg. 2016, 136, 165–174. [Google Scholar] [CrossRef]
- Brown, P.J.; Mannava, S.; Seyler, T.M.; Plate, J.F.; Van Sikes, C.; Stitzel, J.D.; Lang, J.E. Multiple small diameter drillings increase femoral neck stability compared with single large diameter femoral head core decompression technique for avascular necrosis of the femoral head. Surg. Technol. Int. 2016, 29, 247–254. [Google Scholar]
- Sallam, A.A.; Imam, M.A.; Salama, K.S.; Mohamed, O.A. Inverted femoral head graft versus standard core decompression in nontraumatic hip osteonecrosis at minimum 3 years follow-up. Hip Int. 2017, 27, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Calori, G.M.; Mazza, E.; Colombo, A.; Mazzola, S.; Colombo, M. Core decompression and biotechnologies in the treatment of avascular necrosis of the femoral head. EFORT Open Rev. 2017, 2, 41–50. [Google Scholar] [CrossRef]
- Kumar, P.; Shetty, V.D.; Dhillon, M.S. Efficacy of orthobiologic adjuvants to core decompression for hip preservation in avascular necrosis hip. J. Hip Preserv. Surg. 2020, 7, 423–438. [Google Scholar] [CrossRef] [PubMed]
- Zhu, S.; Zhang, X.; Chen, X.; Wang, Y.; Li, S.; Qian, W. Comparison of cell therapy and other novel adjunctive therapies combined with core decompression for the treatment of osteonecrosis of the femoral head: A systematic review and meta-analysis of 20 studies. Bone Jt. Res. 2021, 10, 445–458. [Google Scholar] [CrossRef]
- Smith, S.W.; Meyer, R.A.; Connor, P.M.; Smith, S.E.; Hanley, E.N., Jr. Interobserver reliability and intraobserver reproducibility of the modified ficat classification system of osteonecrosis of the femoral head. J. Bone Jt. Surg. Am. 1996, 78, 1702–1706. [Google Scholar] [CrossRef]
- Ha, Y.C.; Jung, W.H.; Kim, J.R.; Seong, N.H.; Kim, S.Y.; Koo, K.H. Prediction of collapse in femoral head osteonecrosis: A modified kerboul method with use of magnetic resonance images. J. Bone Jt. Surg. Am. 2006, 88 (Suppl. S3), 35–40. [Google Scholar] [CrossRef]
- Lane, N.E.; Hochberg, M.C.; Nevitt, M.C.; Simon, L.S.; Nelson, A.E.; Doherty, M.; Henrotin, Y.; Flechsenhar, K. Oarsi clinical trials recommendations: Design and conduct of clinical trials for hip osteoarthritis. Osteoarthr. Cartil. 2015, 23, 761–771. [Google Scholar] [CrossRef]
- Mont, M.A.; Ragland, P.S.; Etienne, G. Core decompression of the femoral head for osteonecrosis using percutaneous multiple small-diameter drilling. Clin. Orthop. Relat. Res. 2004, 429, 131–138. [Google Scholar] [CrossRef]
- Gao, F.; Sun, W.; Guo, W.; Wang, B.; Cheng, L.; Li, Z. Combined with bone marrow-derived cells and rhbmp-2 for osteonecrosis after femoral neck fractures in children and adolescents: A case series. Sci. Rep. 2016, 6, 30730. [Google Scholar] [CrossRef]
- Lieberman, J.R.; Conduah, A.; Urist, M.R. Treatment of osteonecrosis of the femoral head with core decompression and human bone morphogenetic protein. Clin. Orthop. Relat. Res. 2004, 429, 139–145. [Google Scholar] [CrossRef]
- Mont, M.A.; Marulanda, G.A.; Seyler, T.M.; Plate, J.F.; Delanois, R.E. Core decompression and nonvascularized bone grafting for the treatment of early stage osteonecrosis of the femoral head. Instr. Course Lect. 2007, 56, 213–220. [Google Scholar]
- Papanagiotou, M.; Malizos, K.N.; Vlychou, M.; Dailiana, Z.H. Autologous (non-vascularised) fibular grafting with recombinant bone morphogenetic protein-7 for the treatment of femoral head osteonecrosis: Preliminary report. Bone Jt. J. 2014, 96-B, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.E.; Wihbey, T.; Shah, R.P.; Garino, J.P.; Lee, G.C. Prophylactic decompression and bone grafting for small asymptomatic osteonecrotic lesions of the femoral head. Hip Int. 2011, 21, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, M.E.; Bands, R.E.; Parry, S.; Hoffman, E.; Chan, T.; Hartman, K.M. Does lesion size affect the outcome in avascular necrosis? Clin. Orthop. Relat. Res. 1999, 367, 262–271. [Google Scholar] [CrossRef]
- Yoon, T.R.; Song, E.K.; Rowe, S.M.; Park, C.H. Failure after core decompression in osteonecrosis of the femoral head. Int. Orthop. 2001, 24, 316–318. [Google Scholar] [CrossRef]
- Liu, Z.; Yang, X.; Li, Y.; Zeng, W.N.; Zhao, E.; Zhou, Z. Multiple drilling is not effective in reducing the rate of conversion to total hip arthroplasty in early-stage nontraumatic osteonecrosis of the femoral head: A case-control comparative study with a natural course. BMC Musculoskelet. Disord. 2021, 22, 535. [Google Scholar] [CrossRef]
- Sun, W.; Li, Z.; Gao, F.; Shi, Z.; Zhang, Q.; Guo, W. Recombinant human bone morphogenetic protein-2 in debridement and impacted bone graft for the treatment of femoral head osteonecrosis. PLoS ONE 2014, 9, e100424. [Google Scholar] [CrossRef]
- Yoon, P.W.; Kang, J.Y.; Kim, C.H.; Lee, S.J.; Yoo, J.J.; Kim, H.J.; Kang, S.K.; Min, J.H.; Yoon, K.S. Culture-expanded autologous adipose-derived mesenchymal stem cell treatment for osteonecrosis of the femoral head. Clin. Orthop. Surg. 2021, 13, 37–46. [Google Scholar] [CrossRef]
- Ripamonti, U.; Petit, J.C. Bone morphogenetic proteins, cementogenesis, myoblastic stem cells and the induction of periodontal tissue regeneration. Cytokine Growth Factor Rev. 2009, 20, 489–499. [Google Scholar] [CrossRef]
- Shi, L.; Sun, W.; Gao, F.; Cheng, L.; Li, Z. Heterotopic ossification related to the use of recombinant human bmp-2 in osteonecrosis of femoral head. Medicine 2017, 96, e7413. [Google Scholar] [CrossRef]
- Wen, P.; Zhang, Y.; Hao, L.; Yue, J.; Wang, J.; Wang, T.; Song, W.; Guo, W.; Ma, T. The effect of the necrotic area on the biomechanics of the femoral head—A finite element study. BMC Musculoskelet. Disord. 2020, 21, 211. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | MD Alone | MD with rhBMP-2 and β-TCP | p | |
|---|---|---|---|---|
| Number of hips | 10 | 10 | ||
| Age (years) | 49.3 ± 8.9 | 55.6 ± 7.9 | 0.06 | |
| Sex (n, %) | Male | 6 (60%) | 5 (50%) | 1.00 |
| Female | 4 (40%) | 5 (50%) | ||
| BMI (kg/m2) | 24.2 ± 2.2 | 24.5 ± 3.8 | 0.91 | |
| Side (n, %) | Left | 3 (30%) | 5 (50%) | 0.65 |
| Right | 7 (70%) | 5 (50%) | ||
| Ficat–Arlet classification (n, %) | Gr I | 3 (30%) | 3 (30%) | 1.00 |
| Gr IIA | 7 (70%) | 7 (70%) | ||
| Associated risk factor (n, %) | Alcohol | 1 (10%) | 3 (30%) | 0.25 |
| Idiopathic | 4 (40%) | 1 (10%) | ||
| Steroid | 5 (50%) | 6 (60%) | ||
| Kerboul combined necrotic angle (n, %) | Gr 1 | 3 (30%) | 1 (10%) | 0.54 |
| Gr 2 | 2 (20%) | 4 (40%) | ||
| Gr 3 | 3 (30%) | 4 (40%) | ||
| Gr 4 | 2 (20%) | 1 (10%) | ||
| Follow-up period (days) | 881.1 ± 213.7 | 916.1 ± 198.6 | 0.91 | |
| No. | Age | Sex | BMI | Risk Factor | Direction | Ficat Stage | Kerboul CN Angle | Survival Duration (Days) | Occurrence of FH Collapse |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 59 | M | 19.8 | Idiopathic | Left | 2A | 1 | 732 | No |
| 2 | 64 | M | 29.7 | Steroid | Right | 2A | 2 | 720 | No |
| 3 | 55 | F | 26.6 | Alcohol | Left | 1 | 3 | 1196 | No |
| 4 | 53 | M | 24.4 | Alcohol | Left | 2A | 3 | 1091 | No |
| 5 | 40 | M | 24.0 | Steroid | Right | 2A | 4 | 223 | Yes |
| 6 | 60 | F | 26.7 | Idiopathic | Left | 1 | 1 | 1170 | No |
| 7 | 59 | F | 20.4 | Steroid | Right | 2A | 4 | 183 | Yes |
| 8 | 52 | F | 26.5 | Steroid | Right | 1 | 1 | 734 | No |
| 9 | 61 | F | 23.1 | Steroid | Right | 2A | 3 | 412 | Yes |
| 10 | 52 | M | 25.7 | Idiopathic | Right | 2A | 2 | 267 | Yes |
| 11 | 54 | M | 24.4 | Steroid | Left | 2A | 3 | 183 | Yes |
| 12 | 32 | M | 25.6 | Steroid | Right | 2A | 4 | 132 | Yes |
| 13 | 48 | F | 24.0 | Steroid | Right | 2A | 3 | 87 | Yes |
| 14 | 57 | F | 21.5 | Idiopathic | Right | 2A | 1 | 708 | No |
| 15 | 49 | M | 24.8 | Alcohol | Left | 1 | 2 | 379 | Yes |
| 16 | 37 | F | 19.1 | Steroid | Right | 1 | 2 | 728 | No |
| 17 | 41 | M | 24.2 | Steroid | Right | 1 | 3 | 174 | Yes |
| 18 | 58 | M | 30.9 | Steroid | Right | 2A | 3 | 85 | Yes |
| 19 | 61 | F | 21.4 | Alcohol | Left | 2A | 2 | 181 | Yes |
| 20 | 57 | M | 23.9 | Idiopathic | Left | 2A | 2 | 839 | No |
| Characteristics | MD Alone | MD with rhBMP-2 and β-TCP | p | |
|---|---|---|---|---|
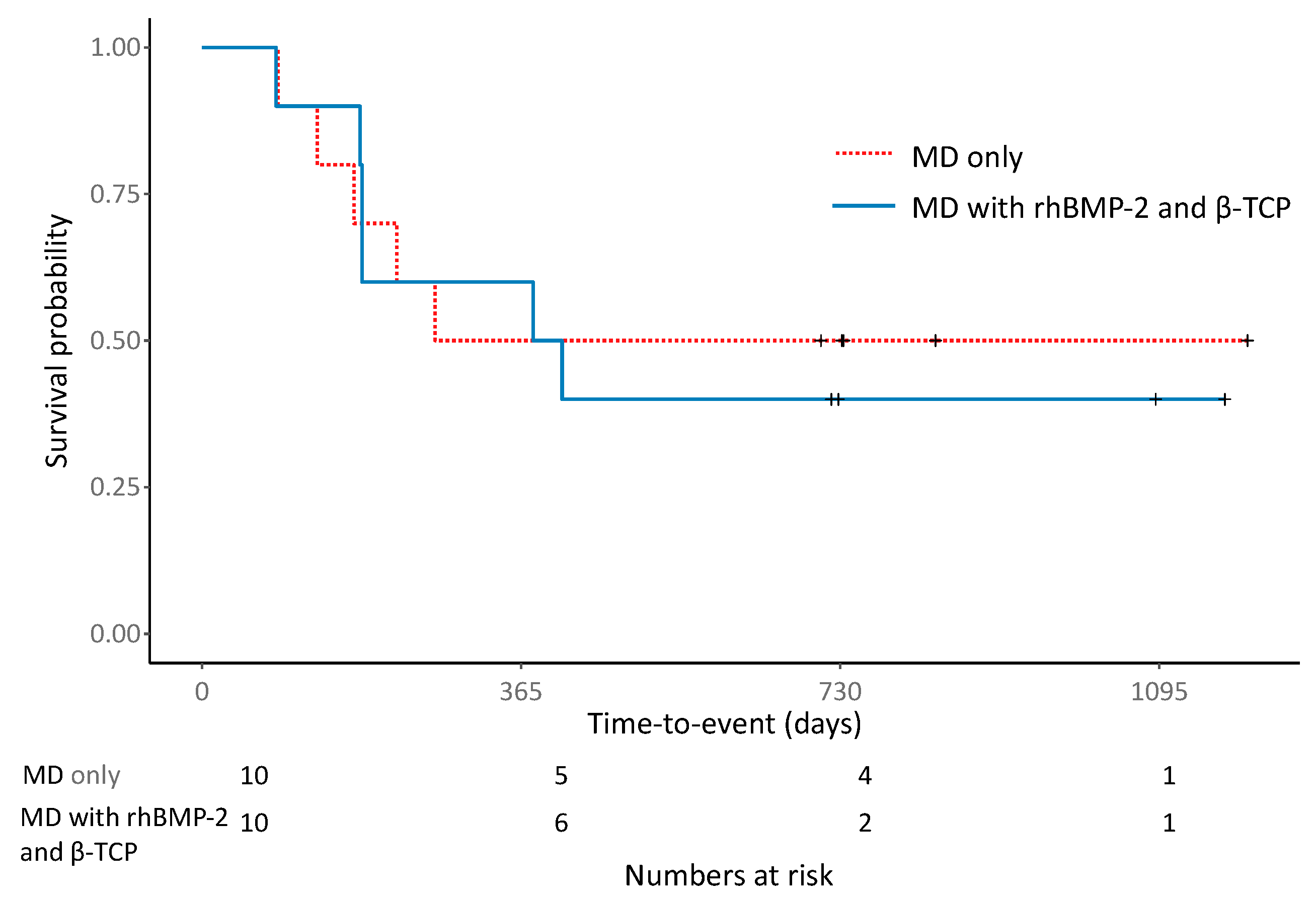
| Femoral head prognosis (n, %) | Preserved | 5 (50.0%) | 4 (40.0%) | 1.00 |
| Collapsed | 5 (50.0%) | 6 (60.0%) | ||
| Time to collapse(days) | 176.6 ± 71.3 | 237.2 ± 128.7 | 0.38 | |
| Conversion to THA (n, %) | 3 (30.0%) | 3 (30.0%) | 1.00 | |
| WOMAC | PreOp | 45.3 ± 19.6 | 39.6 ± 13.4 | 0.62 |
| Last f/u | 31.5 ± 29.1 | 36.8 ± 18.9 | 0.62 | |
| HHS | PreOp | 64.8 ± 10.4 | 59.0 ± 13.5 | 0.29 |
| Last f/u | 71.7 ± 16.2 | 61.3 ± 18.2 | 0.12 | |
| Characteristics | FH Survival | FH Collapse | p | |
|---|---|---|---|---|
| Number of hips | 9 | 11 | ||
| Treatment (n, %) | MD alone | 5 (55.6%) | 5 (45.5%) | 1.00 |
| MD with rhBMP-2 and β-TCP | 4 (44.4%) | 6 (54.5%) | ||
| Age (years) | 54.9 ± 7.6 | 50.5 ± 9.6 | 0.36 | |
| Sex (n, %) | Male | 4 (44.4%) | 7 (63.6%) | 0.68 |
| Female | 5 (55.6%) | 4 (36.4%) | ||
| BMI (kg/m2) | 24.2 ± 3.5 | 24.4 ± 2.7 | 0.91 | |
| Side (n, %) | Left | 5 (55.6%) | 3 (27.3%) | 0.41 |
| Right | 4 (44.4%) | 8 (72.7%) | ||
| Ficat–Arlet classification (n, %) | Gr I | 4 (44.4%) | 2 (18.2%) | 0.34 |
| Gr IIA | 5 (55.6%) | 9 (81.8%) | ||
| Associated risk factor (n, %) | Alcohol | 2 (22.3%) | 2 (18.2%) | 0.14 |
| Idiopathic | 4 (44.4%) | 1 (9.1%) | ||
| Steroid | 3 (33.3%) | 8 (72.7%) | ||
| Kerboul combined necrotic angle (n, %) | Gr 1 | 4 (44.4%) | 0 (0.0%) | 0.04 |
| Gr 2 | 3 (33.3%) | 3 (27.3%) | ||
| Gr 3 | 2 (22.3%) | 5 (45.4%) | ||
| Gr 4 | 0 (0.0%) | 3 (27.3%) | ||
| Time to collapse (days) | 209.6 ± 106.4 | |||
| WOMAC | PreOp | 39.6 ± 17.6 a | 44.8 ± 16.1 b | 0.62 |
| Last f/u | 10.9 ± 8.3 a | 53.2 ± 12.7 b | <0.001 | |
| HHS | PreOp | 62.7 ± 13.0 c | 61.2 ± 11.9 d | 0.97 |
| Last f/u | 83.4 ± 4.8 c | 52.7 ± 10.1 d | <0.001 | |
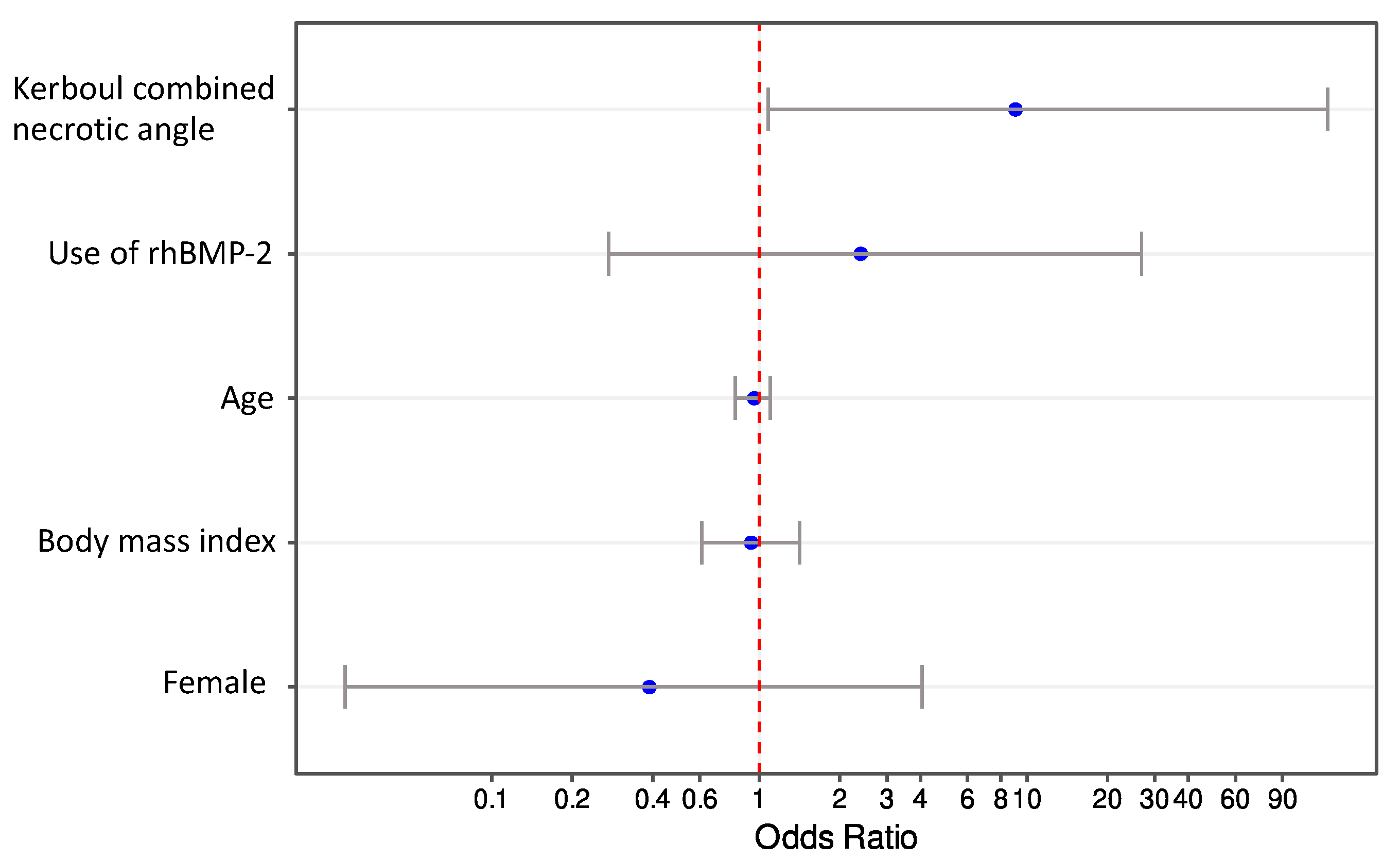
| Variables | Crude OR (95% CI) | p | Adjusted OR (95% CI) | p |
|---|---|---|---|---|
| Use of rhBMP-2 | ||||
| No | Reference | Reference | ||
| Yes | 1.5 (0.26, 8.82) | 0.654 | 2.4 (0.26, 21.79) | 0.431 |
| Age | 0.94 (0.83, 1.05) | 0.268 | 0.96 (0.83, 1.1) | 0.543 |
| Sex | ||||
| Male | Reference | Reference | ||
| Female | 0.46 (0.08, 2.76) | 0.394 | 0.39 (0.04, 4.15) | 0.427 |
| BMI | 1.02 (0.76, 1.38) | 0.901 | 0.93 (0.63, 1.39) | 0.732 |
| Kerboul combined necrotic angle | ||||
| Grade 1 and 2 | Reference | Reference | ||
| Grade 3 and 4 | 9.33 (1.19, 72.99) | 0.033 | 9.06 (0.92, 89.6) | 0.042 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.Y.; Cho, B.W.; Kwon, H.M.; Lee, W.-S.; Park, K.K. Multiple Drilling with Recombinant Human Bone Morphogenetic Protein-2 in Korean Patients with Non-Traumatic Osteonecrosis of the Femoral Head: A Prospective Randomized Pilot Study with a Minimum Two-Year Follow-Up. J. Clin. Med. 2022, 11, 5499. https://doi.org/10.3390/jcm11195499
Park JY, Cho BW, Kwon HM, Lee W-S, Park KK. Multiple Drilling with Recombinant Human Bone Morphogenetic Protein-2 in Korean Patients with Non-Traumatic Osteonecrosis of the Femoral Head: A Prospective Randomized Pilot Study with a Minimum Two-Year Follow-Up. Journal of Clinical Medicine. 2022; 11(19):5499. https://doi.org/10.3390/jcm11195499
Chicago/Turabian StylePark, Jun Young, Byung Woo Cho, Hyuck Min Kwon, Woo-Suk Lee, and Kwan Kyu Park. 2022. "Multiple Drilling with Recombinant Human Bone Morphogenetic Protein-2 in Korean Patients with Non-Traumatic Osteonecrosis of the Femoral Head: A Prospective Randomized Pilot Study with a Minimum Two-Year Follow-Up" Journal of Clinical Medicine 11, no. 19: 5499. https://doi.org/10.3390/jcm11195499
APA StylePark, J. Y., Cho, B. W., Kwon, H. M., Lee, W.-S., & Park, K. K. (2022). Multiple Drilling with Recombinant Human Bone Morphogenetic Protein-2 in Korean Patients with Non-Traumatic Osteonecrosis of the Femoral Head: A Prospective Randomized Pilot Study with a Minimum Two-Year Follow-Up. Journal of Clinical Medicine, 11(19), 5499. https://doi.org/10.3390/jcm11195499