


Composition of the Gut Microbiota Associated with the Response to Immunotherapy in Advanced Cancer Patients: A Chinese Real-World Pilot Study

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Medications
2.2. DNA Extraction
2.3. The 16S rRNA Amplicon Pyrosequencing
2.4. Sequence Analysis
2.5. Bioinformatics and Statistical Analysis
2.6. Statistical Analyses
3. Results
3.1. Characteristics of the Study Population
3.2. Taxonomic Profiles of Cancer Patients Pre- and Post-Immunotherapy
3.3. Overall Microbial Richness and Diversity of Cancer Patients
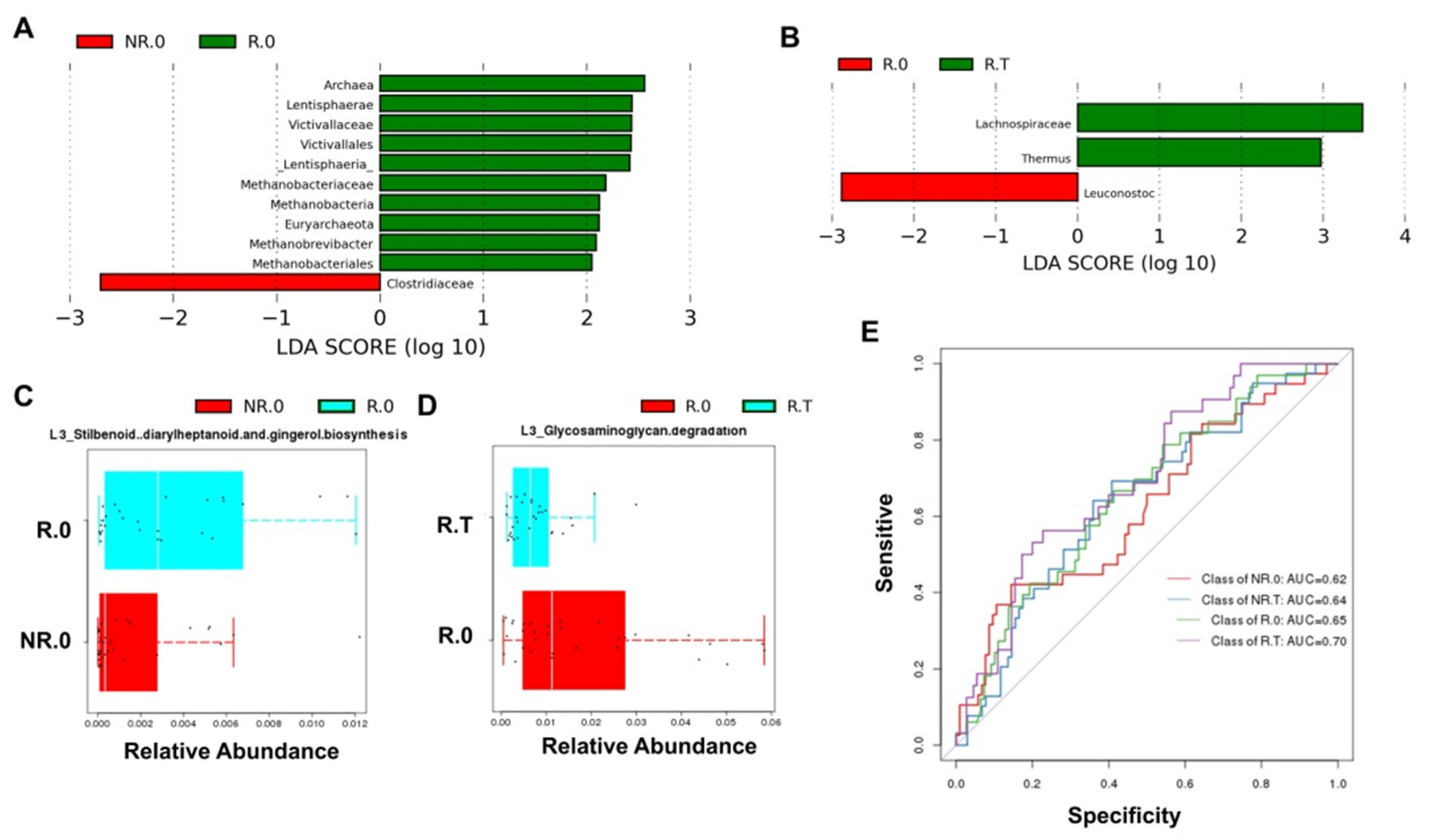
3.4. Significantly Enriched Microbiome and Functional Pathways in the Responder Group
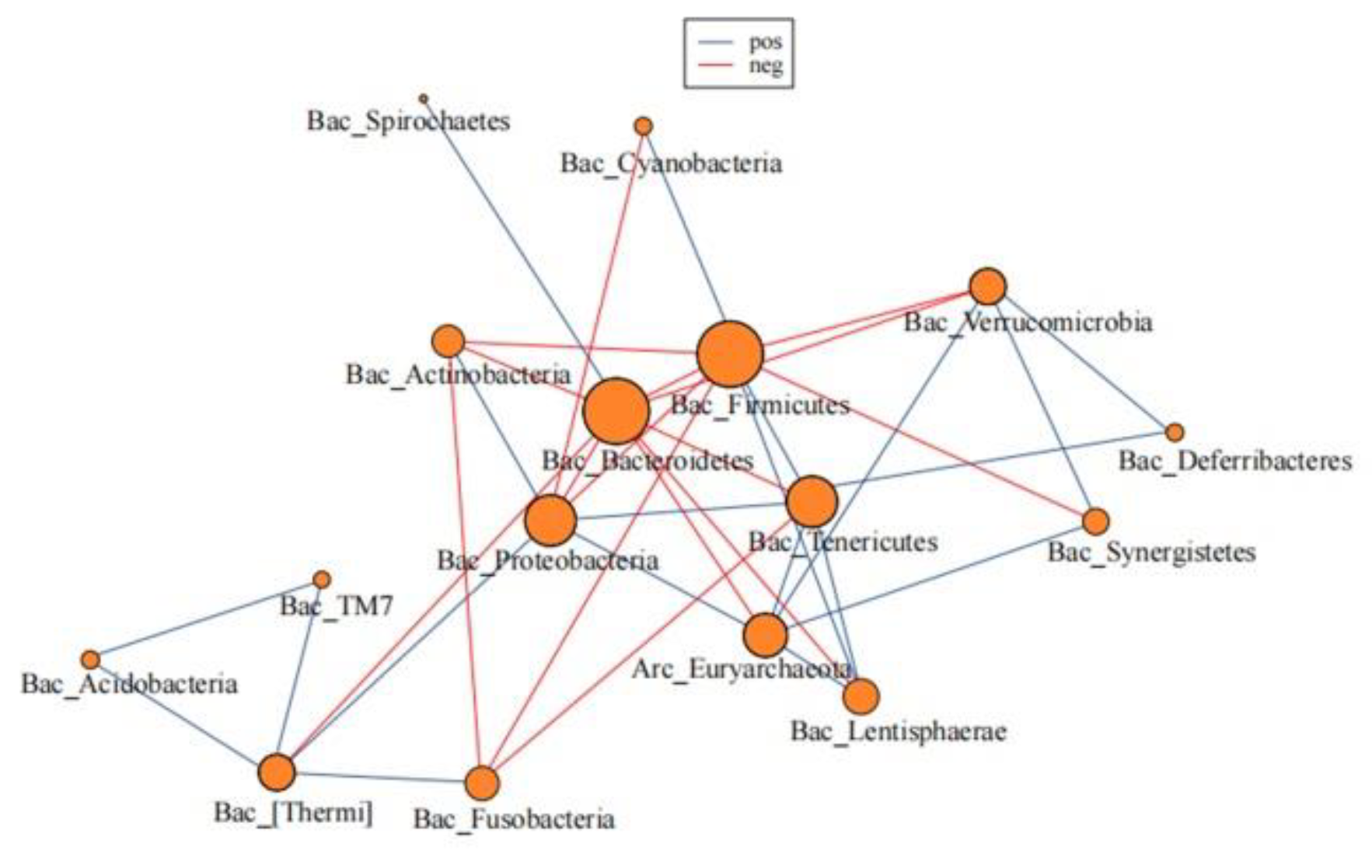
3.5. The Microbial Network of the Gut Microbiome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kalbasi, A.; Ribas, A. Tumour-intrinsic resistance to immune checkpoint blockade. Nat. Rev. Immunol. 2020, 20, 25–39. [Google Scholar] [CrossRef]
- Clavel, T.; Gomes-Neto, J.C.; Lagkouvardos, I.; Ramer-Tait, A.E. Deciphering interactions between the gut microbiota and the immune system via microbial cultivation and minimal microbiomes. Immunol. Rev. 2017, 279, 8–22. [Google Scholar] [CrossRef] [PubMed]
- Zitvogel, L.; Ma, Y.; Raoult, D.; Kroemer, G.; Gajewski, T.F. The microbiome in cancer immunotherapy: Diagnostic tools and therapeutic strategies. Science 2018, 359, 1366–1370. [Google Scholar] [CrossRef] [PubMed]
- Sivan, A.; Corrales, L.; Hubert, N.; Williams, J.B.; Aquino-Michaels, K.; Earley, Z.M.; Benyamin, F.W.; Lei, Y.M.; Jabri, B.; Alegre, M.-L.; et al. Commensal Bifidobacterium promotes antitumor immunity and facilitates anti-PD-L1 efficacy. Science 2015, 350, 1084–1089. [Google Scholar] [CrossRef] [PubMed]
- Matson, V.; Fessler, J.; Bao, R.; Chongsuwat, T.; Zha, Y.; Alegre, M.-L.; Luke, J.J.; Gajewski, T.F. The commensal microbiome is associated with anti-PD-1 efficacy in metastatic melanoma patients. Science 2018, 359, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Gopalakrishnan, V.; Spencer, C.N.; Nezi, L.; Reuben, A.; Andrews, M.C.; Karpinets, T.V.; Prieto, P.A.; Vicente, D.; Hoffman, K.; Wei, S.C.; et al. Gut microbiome modulates response to anti-PD-1 immunotherapy in melanoma patients. Science 2018, 359, 97–103. [Google Scholar] [CrossRef]
- Frankel, A.E.; Coughlin, L.A.; Kim, J.; Froehlich, T.W.; Xie, Y.; Frenkel, E.P.; Koh, A.Y. Metagenomic Shotgun Sequencing and Unbiased Metabolomic Profiling Identify Specific Human Gut Microbiota and Metabolites Associated with Immune Checkpoint Therapy Efficacy in Melanoma Patients. Neoplasia 2017, 19, 848–855. [Google Scholar] [CrossRef] [PubMed]
- Routy, B.; Le Chatelier, E.; Derosa, L.; Duong, C.P.M.; Alou, M.T.; Daillère, R.; Fluckiger, A.; Messaoudene, M.; Rauber, C.; Roberti, M.P.; et al. Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science 2018, 359, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Iida, N.; Dzutsev, A.; Stewart, C.A.; Smith, L.; Bouladoux, N.; Weingarten, R.A.; Molina, D.A.; Salcedo, R.; Back, T.; Cramer, S.; et al. Commensal bacteria control cancer response to therapy by modulating the tumor microenvironment. Science 2013, 342, 967–970. [Google Scholar] [CrossRef]
- Cramer, P.; Bresalier, R.S. Gastrointestinal and Hepatic Complications of Immune Checkpoint Inhibitors. Curr. Gastroenterol. Rep. 2017, 19, 3. [Google Scholar] [CrossRef] [PubMed]
- Aarnoutse, R.; Ziemons, J.; Penders, J.; Rensen, S.S.; De Vos-Geelen, J.; Smidt, M.L. The Clinical Link between Human Intestinal Microbiota and Systemic Cancer Therapy. Int. J. Mol. Sci. 2019, 20, 4145. [Google Scholar] [CrossRef] [PubMed]
- Ervin, S.M.; Ramanan, S.V.; Bhatt, A.P. Relationship Between the Gut Microbiome and Systemic Chemotherapy. Dig. Dis. Sci. 2020, 65, 874–884. [Google Scholar] [CrossRef] [PubMed]
- Secombe, K.R.; Coller, J.K.; Gibson, R.J.; Wardill, H.R.; Bowen, J.M. The bidirectional interaction of the gut microbiome and the innate immune system: Implications for chemotherapy-induced gastrointestinal toxicity. Int. J. Cancer 2019, 144, 2365–2376. [Google Scholar] [CrossRef]
- Rezasoltani, S.; Yadegar, A.; Aghdaei, H.A.; Zali, M.R. Modulatory effects of gut microbiome in cancer immunotherapy: A novel paradigm for blockade of immune checkpoint inhibitors. Cancer Med. 2021, 10, 1141–1154. [Google Scholar] [CrossRef] [PubMed]
- Shui, L.; Yang, X.; Li, J.; Yi, C.; Sun, Q.; Zhu, H. Gut Microbiome as a Potential Factor for Modulating Resistance to Cancer Immunotherapy. Front. Immunol. 2020, 10, 2989. [Google Scholar] [CrossRef] [PubMed]
- Sims, T.T.; El Alam, M.B.; Karpinets, T.V.; Dorta-Estremera, S.; Hegde, V.L.; Nookala, S.; Yoshida-Court, K.; Wu, X.; Biegert, G.W.G.; Medrano, A.Y.D.; et al. Gut microbiome diversity is an independent predictor of survival in cervical cancer patients receiving chemoradiation. Commun. Biol. 2021, 4, 237. [Google Scholar] [CrossRef]
- Pushalkar, S.; Hundeyin, M.; Daley, D.; Zambirinis, C.P.; Kurz, E.; Mishra, A.; Mohan, N.; Aykut, B.; Usyk, M.; Torres, L.E.; et al. The pancreatic cancer microbiome promotes oncogenesis by induction of innate and adaptive immune suppression. Cancer Discov. 2018, 8, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Cristiana, G.; Vicari, A.P.; Sabina, S.; Giorgio, T.; Colombo, M.P. Redirecting in vivo elicited tumor infiltrating macrophages and dendritic cells towards tumor rejection. Cancer Res. 2005, 65, 3437–3446. [Google Scholar]
- Sheng, Q.; Du, H.; Cheng, X.; Cheng, X.; Tang, Y.; Pan, L.; Wang, Q.; Lin, J. Characteristics of fecal gut microbiota in patients with colorectal cancer at different stages and different sites. Oncol. Lett. 2019, 18, 4834–4844. [Google Scholar] [CrossRef] [PubMed]
- Dahmus, J.D.; Kotler, D.L.; Kastenberg, D.M.; Kistler, C.A. The gut microbiome and colorectal cancer: A review of bacterial pathogenesis. J. Gastrointest. Oncol. 2018, 9, 769–777. [Google Scholar] [CrossRef]
- Vivarelli, S.; Salemi, R.; Candido, S.; Falzone, L.; Santagati, M.; Stefani, S.; Torino, F.; Banna, G.L.; Tonini, G.; Libra, M. Gut Microbiota and Cancer: From Pathogenesis to Therapy. Cancers 2019, 11, 38. [Google Scholar] [CrossRef]
- Jin, Y.; Dong, H.; Xia, L.; Yang, Y.; Zhu, Y.; Shen, Y.; Zheng, H.; Yao, C.; Wang, Y.; Lu, S. The Diversity of Gut Microbiome is Associated with Favorable Responses to Anti-Programmed Death 1 Immunotherapy in Chinese Patients With NSCLC. J. Thorac. Oncol. 2019, 14, 1378–1389. [Google Scholar] [CrossRef]
- Song, P.; Yang, D.; Wang, H.; Cui, X.; Si, X.; Zhang, X.; Zhang, L. Relationship between intestinal flora structure and metabolite analysis and immunotherapy efficacy in Chinese NSCLC patients. Thorac. Cancer 2020, 11, 1621–1632. [Google Scholar] [CrossRef] [PubMed]
- Baruch, E.N.; Youngster, I.; Ben-Betzalel, G.; Ortenberg, R.; Lahat, A.; Katz, L.; Adler, K.; Dick-Necula, D.; Raskin, S.; Bloch, N.; et al. Fecal microbiota transplant promotes response in immunotherapy-refractory melanoma patients. Science 2021, 371, 602–609. [Google Scholar] [CrossRef]
- Davar, D.; Dzutsev, A.K.; McCulloch, J.A.; Rodrigues, R.R.; Chauvin, J.-M.; Morrison, R.M.; Deblasio, R.N.; Menna, C.; Ding, Q.; Pagliano, O.; et al. Fecal microbiota transplant overcomes resistance to anti–PD-1 therapy in melanoma patients. Science 2021, 371, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wiesnoski, D.H.; Helmink, B.A.; Gopalakrishnan, V.; Choi, K.; DuPont, H.L.; Jiang, Z.D.; Abu-Sbeih, H.; Sanchez, C.A.; Chang, C.C.; et al. Fecal microbiota transplantation for refractory immune checkpoint inhibitor-associated colitis. Nat. Med. 2018, 24, 1804–1808. [Google Scholar] [CrossRef]
- Yang, Y.; Weng, W.; Peng, J.; Hong, L.; Yang, L.; Toiyama, Y.; Gao, R.; Liu, M.; Yin, M.; Pan, C.; et al. Fusobacterium nucleatum Increases Proliferation of Colorectal Cancer Cells and Tumor Development in Mice by Activating Toll-Like Receptor 4 Signaling to Nuclear Factor-κB, and Up-regulating Expression of MicroRNA-21. Gastroenterology 2017, 152, 851–866. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Peng, Y.; Yu, J.; Chen, T.; Wu, Y.; Shi, L.; Li, Q.; Wu, J.; Fu, X. Invasive Fusobacterium nucleatum activates beta-catenin signaling in colorectal cancer via a TLR4/P-PAK1 cascade. Oncotarget 2017, 8, 31802–31814. [Google Scholar] [CrossRef] [PubMed]
- Berger, N.A. Obesity and cancer pathogenesis. Ann. N. Y. Acad. Sci. 2014, 1311, 57–76. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | n (%) |
|---|---|
| Age | |
| Median (range) | 63 (29–81) |
| Gender | |
| Male | 51 (70.83%) |
| Female | 21 (29.17%) |
| Cancer | |
| Non-squamous non-small cell lung cancer | 18 (25.00%) |
| Lung squamous cell carcinoma | 14 (19.44%) |
| Hepatocellular carcinoma | 7 (9.72%) |
| Gastric cancer | 5 (6.94%) |
| Colorectal carcinoma | 5 (6.94%) |
| Melanoma | 5 (6.94%) |
| Nasopharyngeal carcinoma | 4 (5.56%) |
| Cervical cancer | 3 (4.17%) |
| Small-cell lung cancer | 2 (2.78%) |
| Other cancer | 9 (12.50%) |
| Immunotherapy monotherapy or combined with chemotherapy | |
| Immunotherapy monotherapy | 16 (22.22%) |
| Immunotherapy combined with chemotherapy | 56 (77.78%) |
| Received chemotherapy prior to immunotherapy | |
| Yes | 45 (62.50%) |
| No | 27 (37.50%) |
| Received radiotherapy prior to immunotherapy | |
| Yes | 28 (38.89%) |
| No | 44 (61.11%) |
| Underwent surgery prior to immunotherapy | |
| Yes | 41 (56.94%) |
| No | 31 (43.06%) |
| Received targeted-therapy prior to immunotherapy | |
| Yes | 26 (36.11%) |
| No | 46 (63.89%) |
| Responders (n = 33) | Non-Responders (n = 39) | p Value | |
|---|---|---|---|
| Age | |||
| Median (range) | 66 (42–81) | 61 (29–79) | |
| Gender | 0.059 | ||
| Male | 27 (81.82%) | 24 (61.54%) | |
| Female | 6 (18.18%) | 15 (38.46%) | |
| Cancer | 0.639 | ||
| Non-squamous non-small cell lung cancer | 8 (24.24%) | 10 (25.64%) | |
| Lung squamous cell carcinoma | 6 (18.18%) | 8 (20.51%) | |
| Hepatocellular carcinoma | 2 (6.06%) | 5 (12.82%) | |
| Gastric cancer | 3 (9.09%) | 2 (5.13%) | |
| Colorectal carcinoma | 1 (3.03%) | 4 (10.26%) | |
| Melanoma | 2 (6.06%) | 3 (7.69%) | |
| Nasopharyngeal carcinoma | 3 (9.09%) | 1 (2.56%) | |
| Cervical cancer | 1 (3.03%) | 2 (5.13%) | |
| Small-cell lung cancer | 2 (6.06%) | 0 (0.00%) | |
| Other cancer | 5 (15.15%) | 4 (10.26%) | |
| Immunotherapy monotherapy or combined with chemotherapy | 0.850 | ||
| Immunotherapy monotherapy | 7 (21.21%) | 9 (23.08%) | |
| Immunotherapy combined with chemotherapy | 26 (78.79%) | 30 (76.92%) | |
| Received chemotherapy prior to immunotherapy | 0.077 | ||
| Yes | 17 (51.52%) | 28 (71.79%) | |
| No | 16 (48.48%) | 11 (28.21%) | |
| Received radiotherapy prior to immunotherapy | 0.169 | ||
| Yes | 10 (30.30%) | 18 (46.15%) | |
| No | 23 (69.70%) | 21 (53.85%) | |
| Underwent surgery prior to immunotherapy | 0.705 | ||
| Yes | 18 (54.55%) | 23 (58.97%) | |
| No | 15 (45.45%) | 16 (41.03%) | |
| Received targeted-therapy prior to immunotherapy | 0.054 | ||
| Yes | 8 (24.24%) | 18 (46.15%) | |
| No | 25 (75.76%) | 21 (53.85%) |
| PD_Whole_Tree | Chao1 | Goods_Coverage | Observed_Species | Shannon | Simpson | |
|---|---|---|---|---|---|---|
| R.T | 20.07 | 677.15 | 0.94 | 464 | 4.89 | 0.90 |
| R.0 | 18.77 | 594.96 | 0.94 | 414 | 4.95 | 0.90 |
| NR.0 | 17.11 | 555.62 | 0.94 | 372 | 4.75 | 0.90 |
| NR.T | 19.19 | 627.71 | 0.95 | 433 | 4.75 | 0.88 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, X.; Wang, J.; Gong, L.; Dong, Y.; Shou, J.; Pan, H.; Yu, Z.; Fang, Y. Composition of the Gut Microbiota Associated with the Response to Immunotherapy in Advanced Cancer Patients: A Chinese Real-World Pilot Study. J. Clin. Med. 2022, 11, 5479. https://doi.org/10.3390/jcm11185479
Cheng X, Wang J, Gong L, Dong Y, Shou J, Pan H, Yu Z, Fang Y. Composition of the Gut Microbiota Associated with the Response to Immunotherapy in Advanced Cancer Patients: A Chinese Real-World Pilot Study. Journal of Clinical Medicine. 2022; 11(18):5479. https://doi.org/10.3390/jcm11185479
Chicago/Turabian StyleCheng, Xi, Jiawei Wang, Liu Gong, Yong Dong, Jiawei Shou, Hongming Pan, Zhaonan Yu, and Yong Fang. 2022. "Composition of the Gut Microbiota Associated with the Response to Immunotherapy in Advanced Cancer Patients: A Chinese Real-World Pilot Study" Journal of Clinical Medicine 11, no. 18: 5479. https://doi.org/10.3390/jcm11185479
APA StyleCheng, X., Wang, J., Gong, L., Dong, Y., Shou, J., Pan, H., Yu, Z., & Fang, Y. (2022). Composition of the Gut Microbiota Associated with the Response to Immunotherapy in Advanced Cancer Patients: A Chinese Real-World Pilot Study. Journal of Clinical Medicine, 11(18), 5479. https://doi.org/10.3390/jcm11185479