
The Current Quality of Web-Based Information on the Treatment of Bipolar Disorder: A Systematic Search
 , , and
, , and 
Abstract
1. Introduction
2. Aims
3. Methods
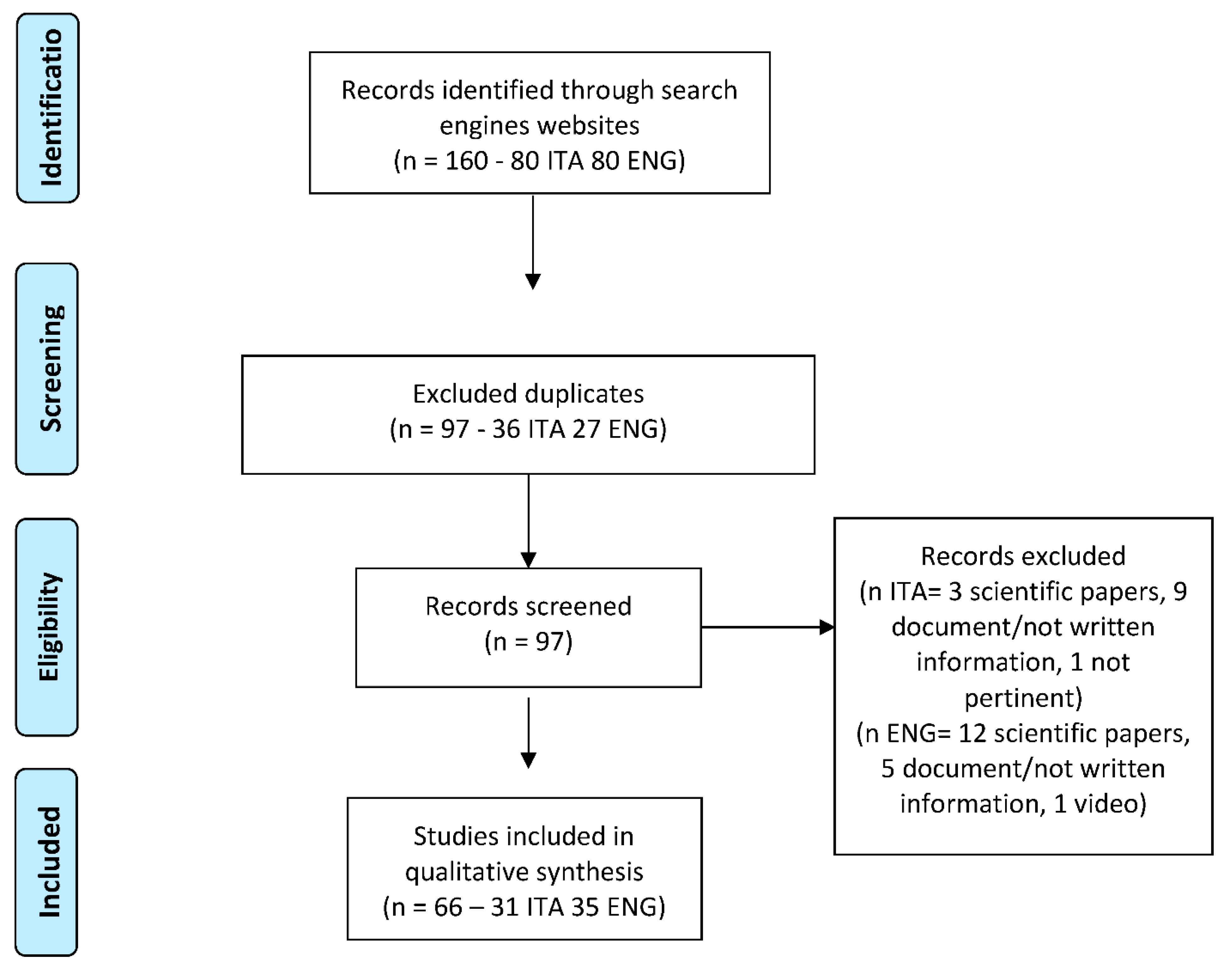
3.1. Search Strategy
3.2. Assessment
4. Statistics
5. Results
5.1. Google PageRank Score
5.2. Technological Quality of the Websites
5.3. Readability
5.4. Adherence to the HONCode
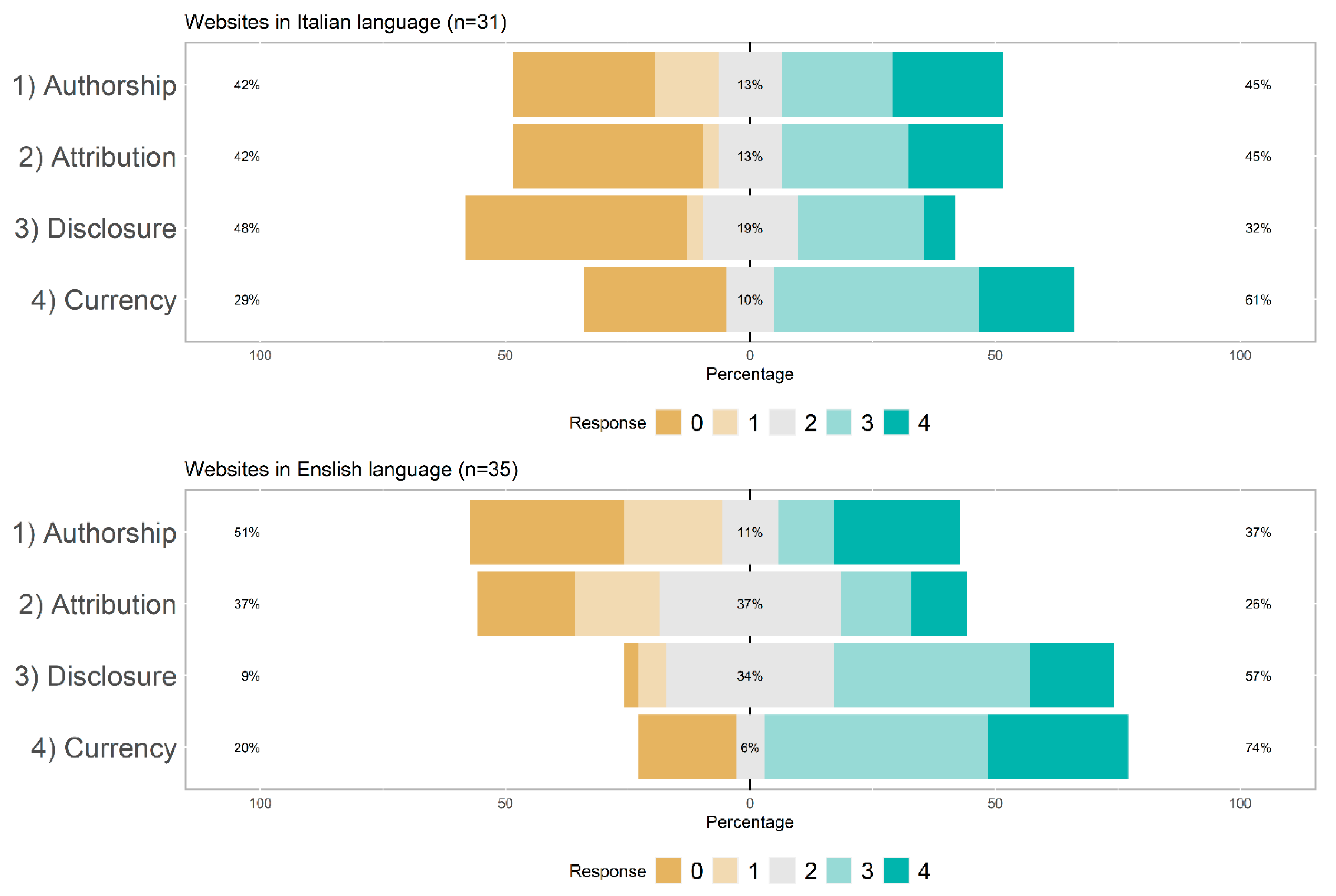
5.5. Information Quality According to the JAMA Benchmark Criteria
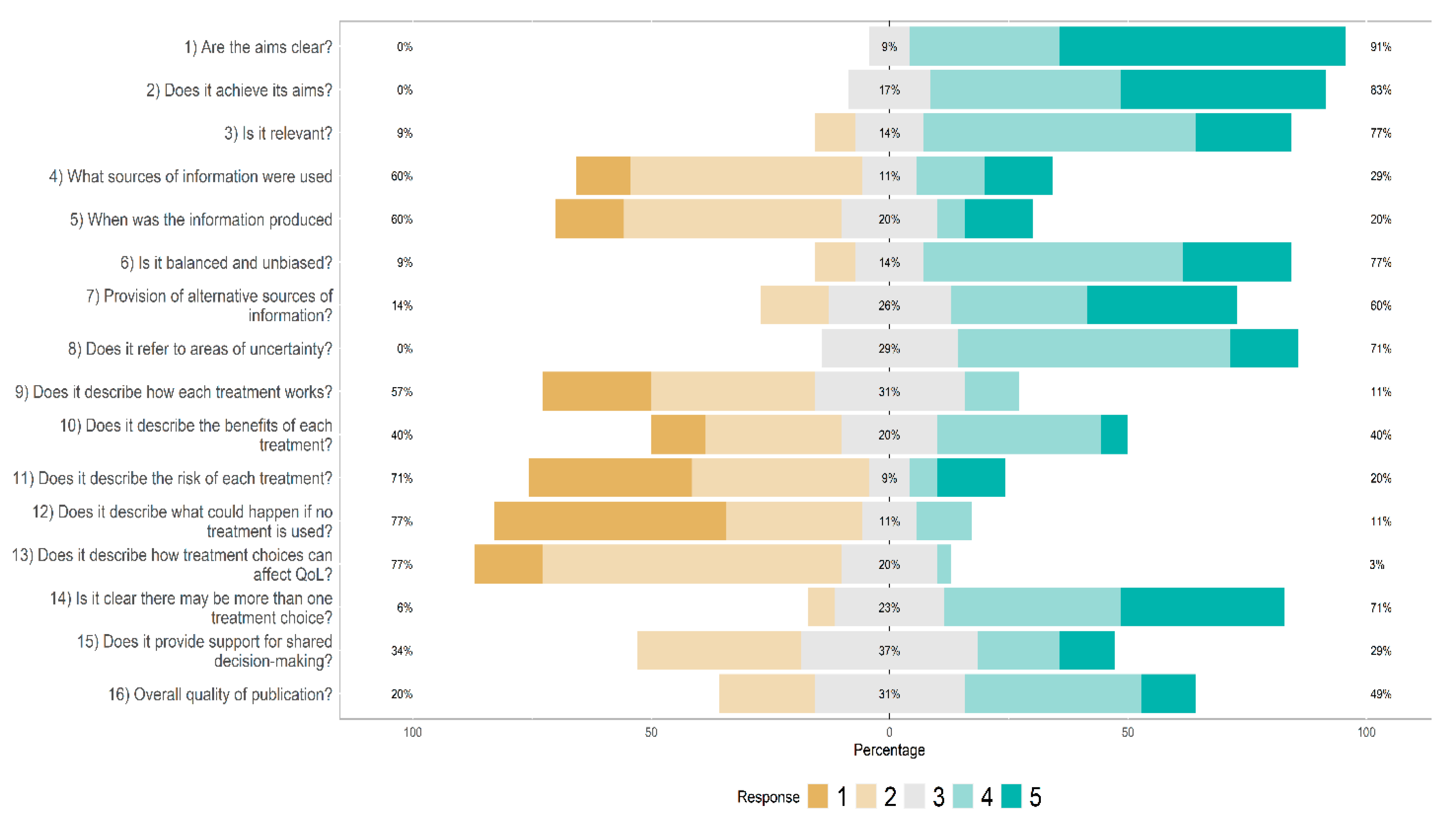
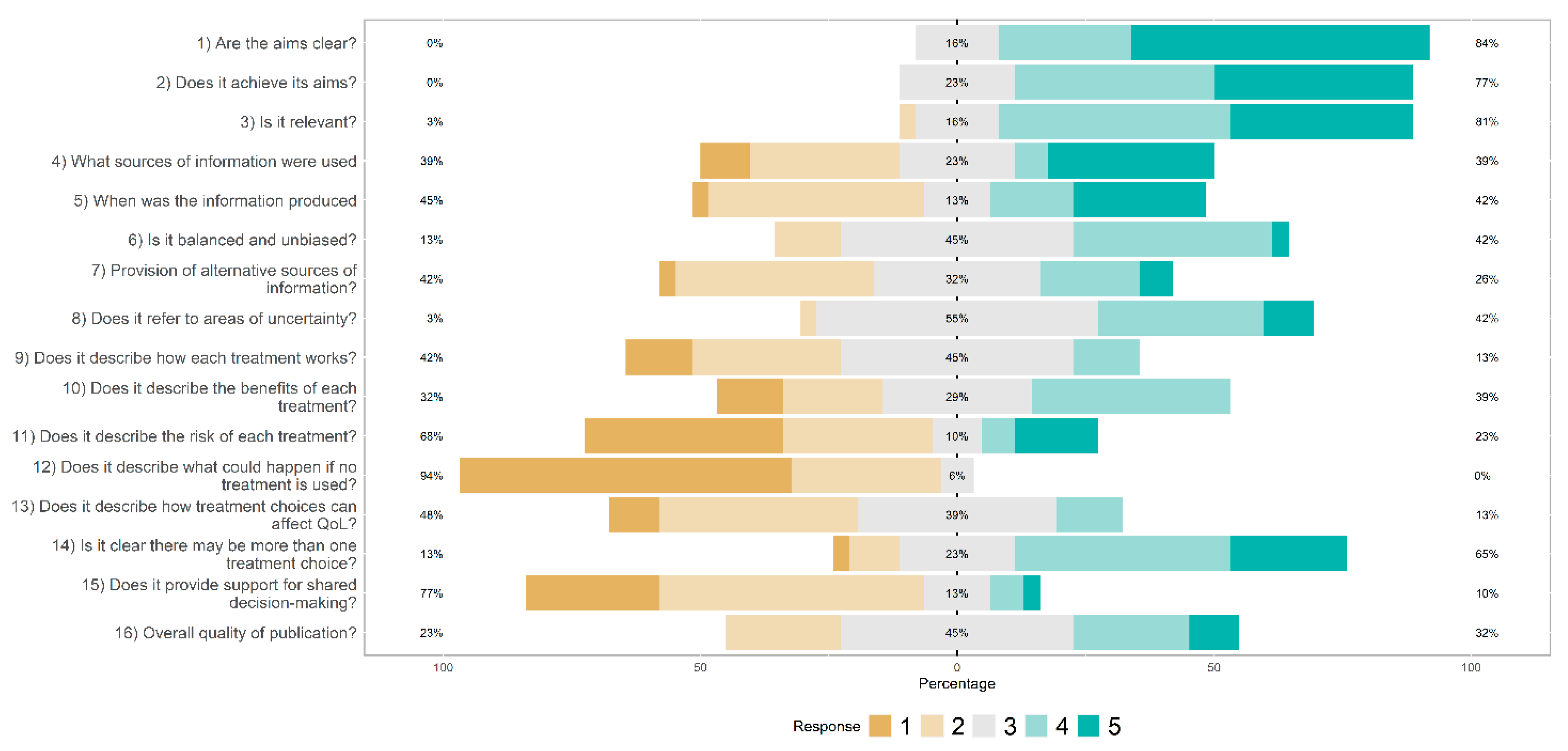
5.6. Information Quality According to the DISCERN Scale
5.7. Information Quality According to BD Treatment Guidelines
6. Discussion
Implications for the Clinics
7. Conclusions
8. Strengths and Limitations
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marwaha, S.; Durrani, A.; Singh, S. Employment outcomes in people with bipolar disorder: A systematic review. Acta Psychiatr. Scand. 2013, 128, 179–193. [Google Scholar] [CrossRef]
- Carta, M.G.; Ouali, U.; Perra, A.; Ben Cheikh Ahmed, A.; Boe, L.; Aissa, A.; Lorrai, S.; Cossu, G.; Aresti, A.; Preti, A.; et al. Living with Bipolar Disorder in the Time of COVID-19: Biorhythms During the Severe Lockdown in Cagliari, Italy, and the Moderate Lockdown in Tunis, Tunisia. Front. Psychiatry 2021, 12, 634765. [Google Scholar] [CrossRef]
- Carta, M.G.; Angst, J. Screening for bipolar disorders: A public health issue. J. Affect. Disord. 2016, 205, 139–143. [Google Scholar] [CrossRef]
- Maina, G.; Rosso, G.; Aguglia, A.; Chiodelli, D.F.; Bogetto, F. Anxiety and bipolar disorders: Epidemiological and clinical aspects. J. Psychopathol. 2011, 17, 365–375. [Google Scholar]
- Bebbington, P.; Ramana, R. The epidemiology of bipolar affective disorder. Soc. Psychiatry Psychiatr. Epidemiol. 1995, 30, 279–292. [Google Scholar] [CrossRef]
- Barbato, A.; Vallarino, M.; Rapisarda, F.; Lora, A.; Parabiaghi, A.; D’Avanzo, B.; Lesage, A. Do people with bipolar disorders have access to psychosocial treatments? A survey in Italy. Int. J. Soc. Psychiatry 2016, 62, 334–344. [Google Scholar] [CrossRef]
- Miklowitz, D.J.; Efthimiou, O.; Furukawa, T.A.; Scott, J.; McLaren, R.; Geddes, J.R.; Cipriani, A. Adjunctive Psychotherapy for Bipolar Disorder: A Systematic Review and Component Network Meta-analysis. JAMA Psychiatry 2021, 78, 141–150. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Yatham, L.; Grunze, H.; Vieta, E.; Young, A.; Blier, P.; Kasper, S.; Moeller, H.J. The International College of Neuro-Psychopharmacology (CINP) Treatment Guidelines for Bipolar Disorder in Adults (CINP-BD-2017), Part 2: Review, Grading of the Evidence, and a Precise Algorithm. Int. J. Neuropsychopharmacol. 2017, 20, 121–179. [Google Scholar] [CrossRef] [PubMed]
- Fountoulakis, K.N.; Grunze, H.; Vieta, E.; Young, A.; Yatham, L.; Blier, P.; Kasper, S.; Moeller, H.J. The International College of Neuro-Psychopharmacology (CINP) Treatment Guidelines for Bipolar Disorder in Adults (CINP-BD-2017), Part 3: The Clinical Guidelines. Int. J. Neuropsychopharmacol. 2017, 20, 180–195. [Google Scholar] [CrossRef]
- Yatham, L.N.; Kennedy, S.H.; Parikh, S.V.; Schaffer, A.; Bond, D.J.; Frey, B.N.; Sharma, V.; Goldstein, B.I.; Rej, S.; Beaulieu, S.; et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018, 20, 97–170. [Google Scholar] [CrossRef]
- Angst, J. Bipolar disorder—A seriously underestimated health burden. Eur. Arch. Psychiatry Clin. Neurosci. 2004, 254, 59–60. [Google Scholar] [CrossRef] [PubMed]
- Judd, L.L.; Akiskal, H.S. The prevalence and disability of bipolar spectrum disorders in the US population: Re-analysis of the ECA database taking into account subthreshold cases. J. Affect. Disord. 2003, 73, 123–131. [Google Scholar] [CrossRef]
- Krahn, G.L. WHO World Report on Disability: A review. Disabil. Health J. 2011, 4, 141–142. [Google Scholar] [CrossRef] [PubMed]
- Wittchen, H.U.; Jacobi, F.; Rehm, J.; Gustavsson, A.; Svensson, M.; Jönsson, B.; Olesen, J.; Allgulander, C.; Alonso, J.; Faravelli, C.; et al. The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur. Neuropsychopharmacol. 2011, 21, 655–679. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.F.; Miles, J.; Walters, K.; King, M.; Osborn, D.P. A systematic review and meta-analysis of premature mortality in bipolar affective disorder. Acta Psychiatr. Scand. 2015, 131, 417–425. [Google Scholar] [CrossRef]
- Crump, C.; Sundquist, K.; Winkleby, M.A.; Sundquist, J. Comorbidities and mortality in bipolar disorder: A Swedish national cohort study. JAMA Psychiatry 2013, 70, 931–939. [Google Scholar] [CrossRef]
- Fajutrao, L.; Locklear, J.; Priaulx, J.; Heyes, A. A systematic review of the evidence of the burden of bipolar disorder in Europe. Clin. Pract. Epidemiol. Ment. Health CP EMH 2009, 5, 3. [Google Scholar] [CrossRef]
- Greenhouse, W.J.; Meyer, B.; Johnson, S.L. Coping and medication adherence in bipolar disorder. J. Affect. Disord. 2000, 59, 237–241. [Google Scholar] [CrossRef]
- Scott, J.; Pope, M. Nonadherence with mood stabilizers: Prevalence and predictors. J. Clin. Psychiatry 2002, 63, 384–390. [Google Scholar] [CrossRef]
- Morton, E.; Ho, K.; Barnes, S.J.; Michalak, E.E. Digital Health Literacy in Bipolar Disorder: International Web-Based Survey. JMIR Ment. Health 2021, 8, e29764. [Google Scholar] [CrossRef]
- Khazaal, Y.; Chatton, A.; Zullino, D.; Khan, R. HON label and DISCERN as content quality indicators of health-related websites. Psychiatr. Q. 2012, 83, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Ellison, N.; Mason, O.; Scior, K. Bipolar disorder and stigma: A systematic review of the literature. J. Affect. Disord. 2013, 151, 805–820. [Google Scholar] [CrossRef]
- Clement, S.; Schauman, O.; Graham, T.; Maggioni, F.; Evans-Lacko, S.; Bezborodovs, N.; Morgan, C.; Rüsch, N.; Brown, J.S.; Thornicroft, G. What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychol. Med. 2015, 45, 11–27. [Google Scholar] [CrossRef]
- Pellegrini, C. Mental illness stigma in health care settings a barrier to care. CMAJ Can. Med. Assoc. J. 2014, 186, E17. [Google Scholar] [CrossRef]
- Angermeyer, M.C.; van der Auwera, S.; Carta, M.G.; Schomerus, G. Public attitudes towards psychiatry and psychiatric treatment at the beginning of the 21st century: A systematic review and meta-analysis of population surveys. World Psychiatry 2017, 16, 50–61. [Google Scholar] [CrossRef]
- Renwick, L.; Pedley, R.; Johnson, I.; Bell, V.; Lovell, K.; Bee, P.; Brooks, H. Mental health literacy in children and adolescents in low- and middle-income countries: A mixed studies systematic review and narrative synthesis. Eur. Child Adolesc. Psychiatry 2022. Advance online publication. [Google Scholar] [CrossRef]
- Link, B.G. Understanding labeling effects in the area of mental disorders: An assessment of the effects of expectations of rejection. Am. Sociol. Assoc. 1987, 52, 96–112. [Google Scholar] [CrossRef]
- Thomas, N.; McLeod, B.; Jones, N.; Abbott, J.-A. Developing internet interventions to target the individual impact of stigma in health conditions. Internet Interv. 2015, 2, 351–358. [Google Scholar] [CrossRef]
- Vogel, D.L.; Bitman, R.L.; Hammer, J.H.; Wade, N.G. Is stigma internalized? The longitudinal impact of public stigma on self-stigma. J. Couns. Psychol. 2013, 60, 311–316. [Google Scholar] [CrossRef]
- Jorm, A.F. Mental health literacy: Empowering the community to take action for better mental health. Am. Psychol. 2012, 67, 231–243. [Google Scholar] [CrossRef]
- Favre, S.; Aubry, J.M.; Richard-Lepouriel, H. Perceived public stigma and perceived public exposure by persons living with bipolar disorder: A qualitative study. Int. J. Soc. Psychiatry 2022. Advance online publication. [Google Scholar] [CrossRef]
- Perich, T.; Mitchell, P.B.; Vilus, B. Stigma in bipolar disorder: A current review of the literature. Aust. J. Psychiatry 2022, 56, 1060–1064. [Google Scholar] [CrossRef]
- Berger, M.; Wagner, T.H.; Baker, L.C. Internet use and stigmatized illness. Soc. Sci. Med. (1982) 2005, 61, 1821–1827. [Google Scholar] [CrossRef]
- Žaja, N.; Vukojević, J.; Žarko, T.; Marelić, M.; Vidović, D.; Vukušić Rukavina, T. Internet Use among Patients with Schizophrenia and Depression. Int. J. Environ. Res. Public Health 2022, 19, 5695. [Google Scholar] [CrossRef]
- Griffiths, K.M.; Carron-Arthur, B.; Parsons, A.; Reid, R. Effectiveness of programs for reducing the stigma associated with mental disorders. A meta-analysis of randomized controlled trials. World Psychiatry Off. J. World Psychiatr. Assoc. 2014, 13, 161–175. [Google Scholar] [CrossRef]
- Brashers, D.; Goldsmith, D.; Hsieh, E. Information Seeking and Avoiding in Health Contexts. Hum. Commun. Res. 2002, 28, 258–271. [Google Scholar] [CrossRef]
- Lambert, S.D.; Loiselle, C.G. Health information seeking behavior. Qual. Health Res. 2007, 17, 1006–1019. [Google Scholar] [CrossRef]
- Conell, J.; Bauer, R.; Glenn, T.; Alda, M.; Ardau, R.; Baune, B.T.; Berk, M.; Bersudsky, Y.; Bilderbeck, A.; Bocchetta, A.; et al. Online information seeking by patients with bipolar disorder: Results from an international multisite survey. Int. J. Bipolar Disord. 2016, 4, 17. [Google Scholar] [CrossRef]
- Giacco, D.; Luciano, M.; Del Vecchio, V.; Sampogna, G.; Slade, M.; Clarke, E.; Nagy, M.; Egerhazi, A.; Munk-Jørgensen, P.; Bording, M.F.; et al. CEDAR study group Desire for information of people with severe mental illness. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 1883–1891. [Google Scholar] [CrossRef]
- Hallett, C.; Gupta, S.; Priebe, S. What do outpatients with schizophrenia and mood disorders want to learn about their illness? Psychiatr. Serv. 2013, 64, 764–769. [Google Scholar] [CrossRef]
- Kerner, B.; Crisanti, A.S.; DeShaw, J.L.; Ho, J.G.; Jordan, K.; Krall, R.L.; Kuntz, M.J.; Mazurie, A.J.; Nestsiarovich, A.; Perkins, D.J.; et al. Preferences of Information Dissemination on Treatment for Bipolar Disorder: Patient-Centered Focus Group Study. JMIR Ment. Health 2019, 6, e12848. [Google Scholar] [CrossRef]
- Gaglio, B.; Glasgow, R.E.; Bull, S.S. Do patient preferences for health information vary by health literacy or numeracy? A qualitative assessment. J. Health Commun. 2012, 17 (Suppl. S3), 109–121. [Google Scholar] [CrossRef]
- Hesse, B.W.; Nelson, D.E.; Kreps, G.L.; Croyle, R.T.; Arora, N.K.; Rimer, B.K.; Viswanath, K. Trust and sources of health information: The impact of the Internet and its implications for health care providers: Findings from the first Health Information National Trends Survey. Arch. Intern. Med. 2005, 165, 2618–2624. [Google Scholar] [CrossRef]
- Horgan, A.; Sweeney, J. Young students’ use of the Internet for mental health information and support. J. Psychiatr. Ment. Health Nurs. 2010, 17, 117–123. [Google Scholar] [CrossRef]
- Powell, J.; Clarke, A. The WWW of the World Wide Web: Who, What, and Why? J. Med. Internet Res. 2002, 4, e4. [Google Scholar] [CrossRef]
- Baker, L.; Wagner, T.H.; Singer, S.; Bundorf, M.K. Use of the Internet and e-mail for health care information: Results from a national survey. JAMA 2003, 289, 2400–2406. [Google Scholar] [CrossRef]
- Powell, J.; Clarke, A. Internet information-seeking in mental health: Population survey. Br. J. Psychiatry J. Ment. Sci. 2006, 189, 273–277. [Google Scholar] [CrossRef]
- Morel, V.; Chatton, A.; Cochand, S.; Zullino, D.; Khazaal, Y. Quality of web-based information on bipolar disorder. J. Affect. Disord. 2008, 110, 265–269. [Google Scholar] [CrossRef]
- Hall, A.K.; Bernhardt, J.M.; Dodd, V.; Vollrath, M.W. The digital health divide: Evaluating online health information access and use among older adults. Health Educ. Behav. Off. Publ. Soc. Public Health Educ. 2015, 42, 202–209. [Google Scholar] [CrossRef]
- Grohol, J.M.; Slimowicz, J.; Granda, R. The quality of mental health information commonly searched for on the Internet. Cyberpsychology Behav. Soc. Netw. 2014, 17, 216–221. [Google Scholar] [CrossRef]
- Korp, P. Health on the Internet: Implications for health promotion. Health Educ. Res. 2006, 21, 78–86. [Google Scholar] [CrossRef]
- McKearney, R.M.; MacKinnon, R.C.; Smith, M.; Baker, R. Tinnitus information online—Does it ring true? J. Laryngol. Otol. 2018, 132, 984–989. [Google Scholar] [CrossRef]
- Chan, J.K.; Farrer, L.M.; Gulliver, A.; Bennett, K.; Griffiths, K.M. University Students’ Views on the Perceived Benefits and Drawbacks of Seeking Help for Mental Health Problems on the Internet: A Qualitative Study. JMIR Hum. Factors 2016, 3, e3. [Google Scholar] [CrossRef]
- Christensen, H.; Griffiths, K.M.; Jorm, A.F. Delivering interventions for depression by using the internet: Randomised controlled trial. BMJ (Clin. Res. Ed.) 2004, 328, 265. [Google Scholar] [CrossRef]
- Griffiths, K.M.; Christensen, H. Quality of web based information on treatment of depression: Cross sectional survey. BMJ (Clin. Res. Ed.) 2000, 321, 1511–1515. [Google Scholar] [CrossRef]
- Griffiths, K.M.; Christensen, H.; Jorm, A.F.; Evans, K.; Groves, C. Effect of web-based depression literacy and cognitive-behavioral therapy interventions on stigmatizing attitudes to depression: Randomized controlled trial. Br. J. Psychiatry J. Ment. Sci. 2004, 185, 342–349. [Google Scholar] [CrossRef]
- Perra, A.; Preti, A.; De Lorenzo, V.; Nardi, A.E.; Carta, M.G. Quality of information of websites dedicated to obesity: A systematic search to promote high level of information for Internet users and professionals. Eat Weight. Disord. EWD 2021. Advance online publication. [Google Scholar] [CrossRef]
- Bernstein, M.T.; Reynolds, K.A.; Jakobson, L.S.; Petty, S.K.; Pryor, T.; Stoesz, B.M.; Alcolado, G.M.; Furer, P. Do anxiety websites have the answers people are looking for? Patient Educ. Couns. 2022, 105, 933–941. [Google Scholar] [CrossRef]
- Andersson, G.; Bergström, J.; Holländare, F.; Carlbring, P.; Kaldo, V.; Ekselius, L. Internet-based self-help for depression: Randomised controlled trial. Br. J. Psychiatry J. Ment. Sci. 2005, 187, 456–461. [Google Scholar] [CrossRef]
- Eysenbach, G.; Powell, J.; Kuss, O.; Sa, E.R. Empirical studies assessing the quality of health information for consumers on the world wide web: A systematic review. JAMA 2002, 287, 2691–2700. [Google Scholar] [CrossRef]
- Goodwin, G.M.; Haddad, P.M.; Ferrier, I.N.; Aronson, J.K.; Barnes, T.; Cipriani, A.; Coghill, D.R.; Fazel, S.; Geddes, J.R.; Grunze, H.; et al. Evidence-based guidelines for treating bipolar disorder: Revised third edition recommendations from the British Association for Psychopharmacology. J. Psychopharmacol. 2016, 30, 495–553. [Google Scholar] [CrossRef]
- Reavley, N.J.; Jorm, A.F. The quality of mental disorder information websites: A review. Patient Educ. Couns. 2011, 85, e16–e25. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Yatham, L.N.; Grunze, H.; Vieta, E.; Young, A.H.; Blier, P.; Tohen, M.; Kasper, S.; Moeller, H.J. The CINP Guidelines on the Definition and Evidence-Based Interventions for Treatment-Resistant Bipolar Disorder. Int. J. Neuropsychopharmacol. 2020, 23, 230–256. [Google Scholar] [CrossRef]
- StatCounter Global Stats 2020 Top 5 Desktop, Tablet, Mobile & Console Search Engines from January 2019 to April 2020. Available online: https://gs.statcounter.com/search-engine-market-share#monthly-201901-202004 (accessed on 12 April 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Chen, P.; Xie, H.; Maslov, S.; Redner, S. Finding scientific gems with Google’s PageRank algorithm. J. Inform. 2007, 1, 8–15. [Google Scholar] [CrossRef]
- Al Wattar, B.H.; Pidgeon, C.; Learner, H.; Zamora, J.; Thangaratinam, S. Online health information on obesity in pregnancy: A systematic review. Eur. J. Obs. Gynecol. Reprod Biol. 2016, 206, 147–152. [Google Scholar] [CrossRef]
- D’Alessandro, D.M.; Kingsley, P.; Johnson-West, J. The readability of pediatric patient education materials on the World Wide Web. Arch. Pediatrics Adolesc. Med. 2001, 155, 807–812. [Google Scholar] [CrossRef]
- Lucisano, P.; Piemontese, M.E. Gulpease: A formula to predict readability of texts written in Italian Language. Sc. Città 1988, 39. [Google Scholar]
- Tonelli, S.; Tran, K.M.; Pianta, E. Making readability indices readable. In Proceedings of the First Workshop on Predicting and Improving Text Readability for target reader populations, Montreal, QC, Canada, 7 June 2012; pp. 40–48. [Google Scholar]
- Charnock, D. The DISCERN Handbook; Radcliffe Medical Press: Abingdon, UK, 1998. [Google Scholar]
- Charnock, D.; Shepperd, S.; Needham, G.; Gann, R. DISCERN: An instrument for judging the quality of written consumer health information on treatment choices. J. Epidemiol. Community Health 1999, 53, 105–111. [Google Scholar] [CrossRef]
- Silberg, W.M.; Lundberg, G.D.; Musacchio, R.A. Assessing, controlling, and assuring the quality of medical information on the Internet: Caveant lector et viewor—Let the reader and viewer beware. JAMA 1997, 277, 1244–1245. [Google Scholar] [CrossRef]
- Boyer, C.; Baujard, V.; Geissbuhler, A. Evolution of health web certification through the HONcode experience. Stud. Health Technol. Inform. 2011, 169, 53–57. [Google Scholar]
- Brennan, P.; Silman, A. Statistical methods for assessing observer variability in clinical measures. BMJ (Clin. Res. Ed.) 1992, 304, 1491–1494. [Google Scholar] [CrossRef]
- American Psychiatric Association Practice guideline for the treatment of patients with bipolar disorder (revision). Am. J. Psychiatry 2002, 159 (Suppl. S4), 1–50.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Italian (n = 31) | English (n = 35) | Tot (n = 66) | ||
|---|---|---|---|---|
| Search engine | 16 | 17 | 33 | |
| Yahoo | 11 | 8 | 19 | |
| Bing | 4 | 1 | 5 | |
| DuckDuckGo | 0 | 9 | 9 |
| English Websites (n = 31) | Italian Websites (n = 35) | Statistics | |
|---|---|---|---|
| Drugs | 27 (87%) | 28 (80%) | χ2 = 0.59; df = 1; p = 0.44 |
| Psychotherapy | 25 (80%) | 23 (67%) | χ2 = 1.85; df = 1; p = 0.17 |
| Psychosocial Interventions | 23 (73%) | 9 (27%) | χ2 = 15.5; df = 1; p < 0.0001 |
| Only one treatment | 6 (20%) | 16 (47%) | χ2 = 5.14; df = 1; p = 0.02 |
| Two treatments | 6 (20%) | 12 (33%) | χ2 = 1.85; df = 1; p = 0.17 |
| All types of interventions | 19 (60%) | 7 (20%) | χ2 = 11.7; df = 1; p < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piras, M.; Perra, A.; Gureje, O.; Preti, A.; Carta, M.G. The Current Quality of Web-Based Information on the Treatment of Bipolar Disorder: A Systematic Search. J. Clin. Med. 2022, 11, 5427. https://doi.org/10.3390/jcm11185427
Piras M, Perra A, Gureje O, Preti A, Carta MG. The Current Quality of Web-Based Information on the Treatment of Bipolar Disorder: A Systematic Search. Journal of Clinical Medicine. 2022; 11(18):5427. https://doi.org/10.3390/jcm11185427
Chicago/Turabian StylePiras, Martina, Alessandra Perra, Oye Gureje, Antonio Preti, and Mauro Giovanni Carta. 2022. "The Current Quality of Web-Based Information on the Treatment of Bipolar Disorder: A Systematic Search" Journal of Clinical Medicine 11, no. 18: 5427. https://doi.org/10.3390/jcm11185427
APA StylePiras, M., Perra, A., Gureje, O., Preti, A., & Carta, M. G. (2022). The Current Quality of Web-Based Information on the Treatment of Bipolar Disorder: A Systematic Search. Journal of Clinical Medicine, 11(18), 5427. https://doi.org/10.3390/jcm11185427