
The Role of Presepsin and Procalcitonin in Early Diagnosis of Bacterial Infections in Cirrhotic Patients with Acute-on-Chronic Liver Failure

 , ,
, ,  ,
,  , , , , , , , , , ,
, , , , , , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
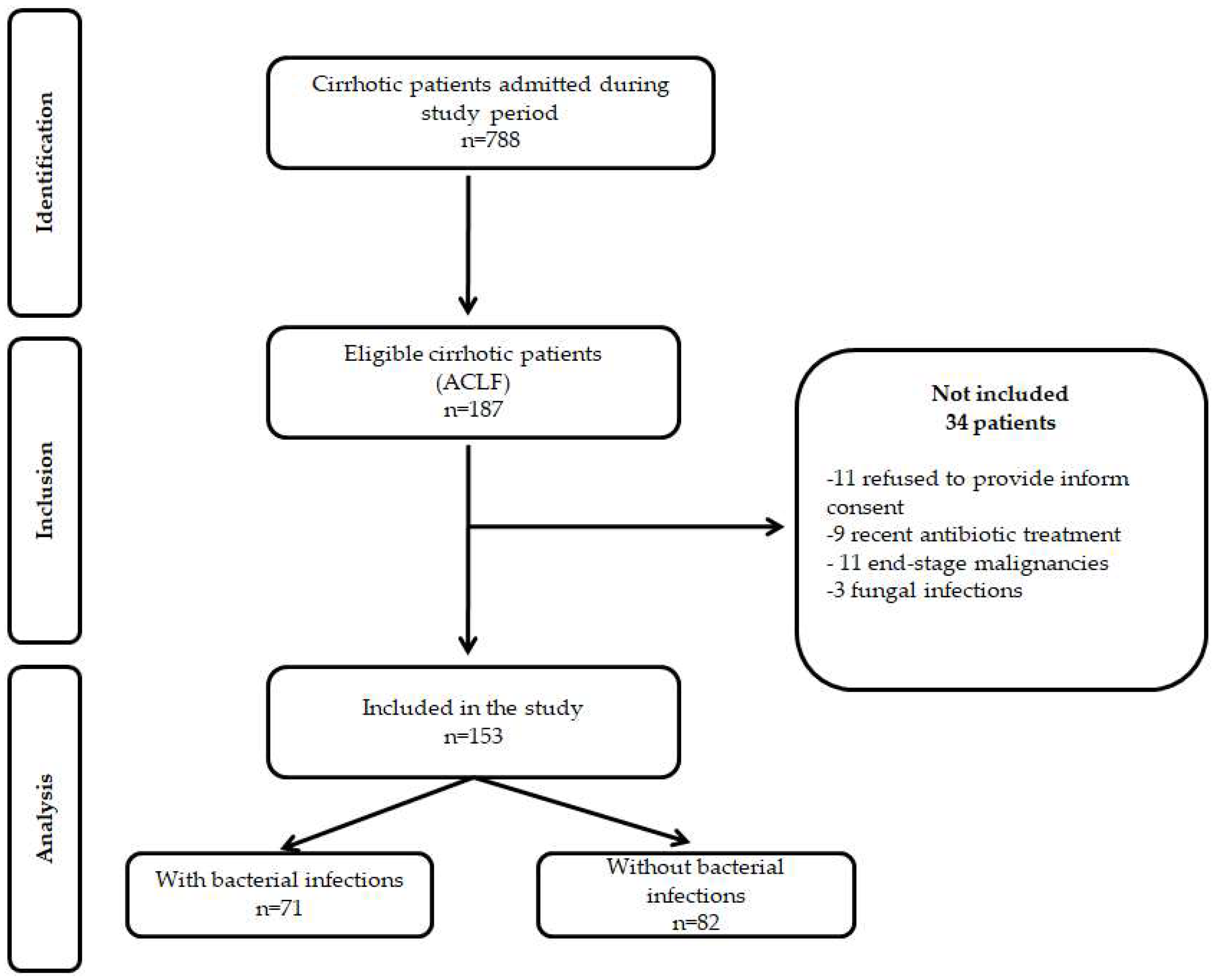
2.1. Patients
2.2. Clinical and Laboratory Assessment
2.3. Statistical Analysis
3. Results
3.1. Patients Characteristics
3.2. Infectious Complications
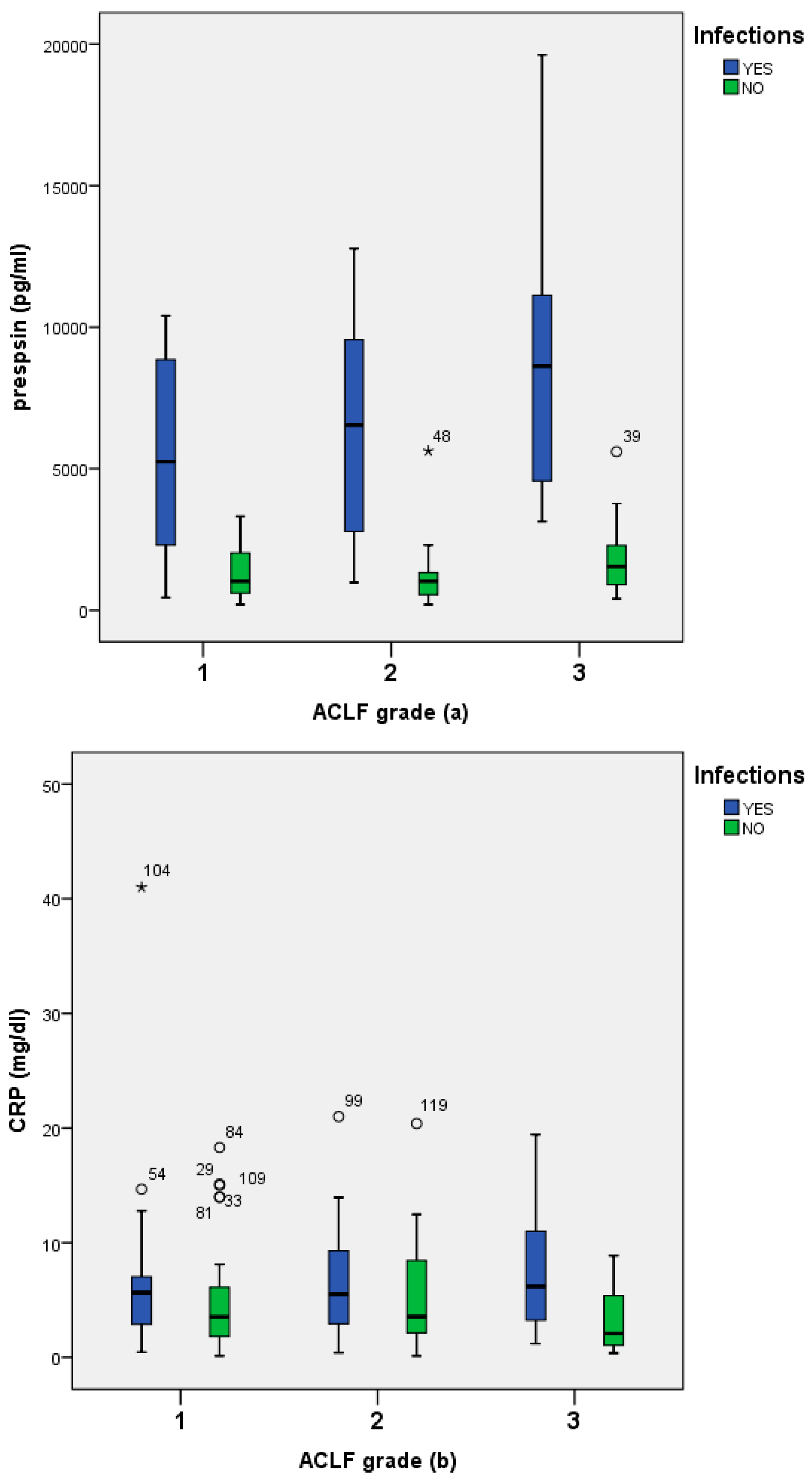
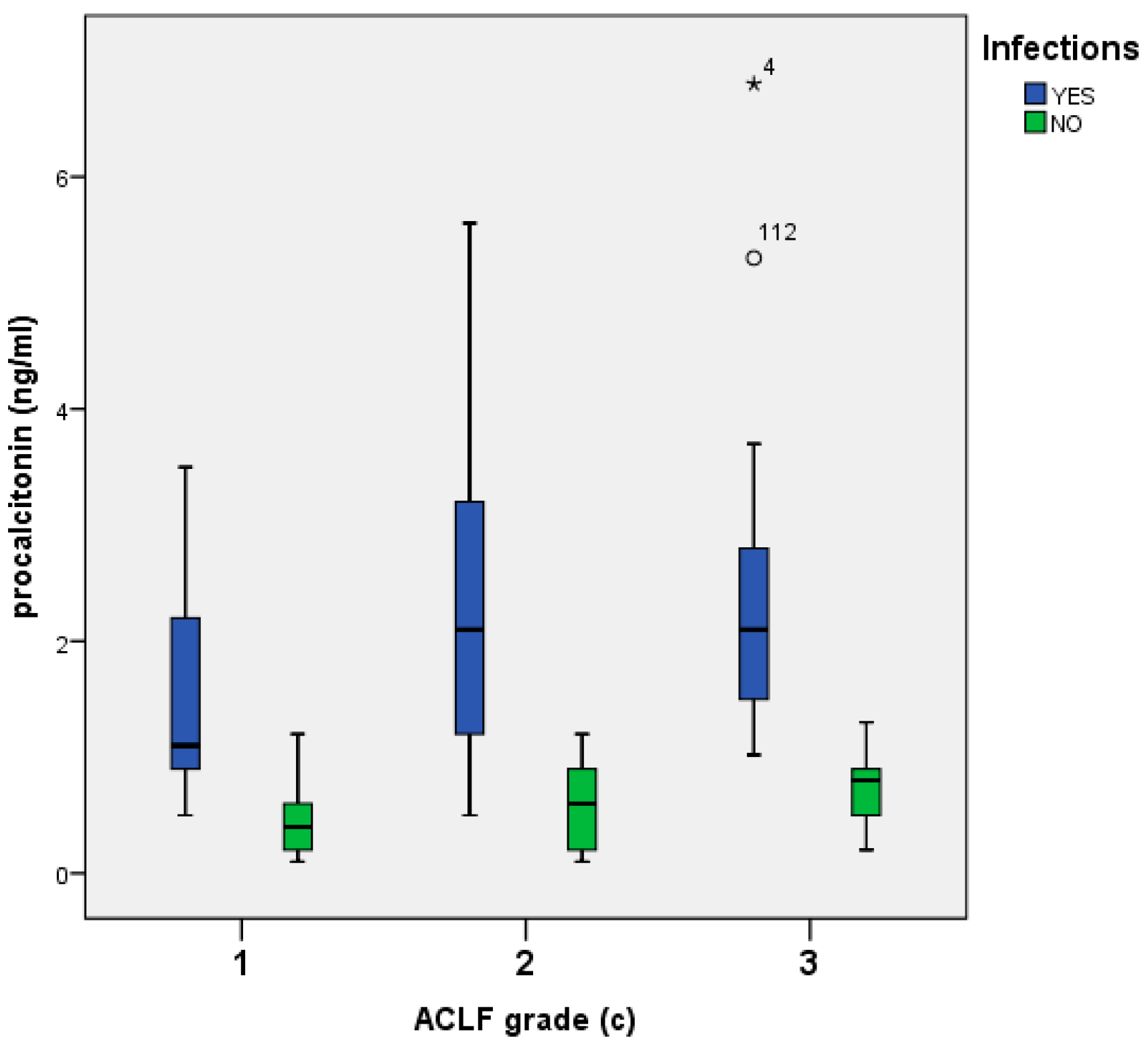
3.3. Presepsin, PCT, and CRP Infectious Complications
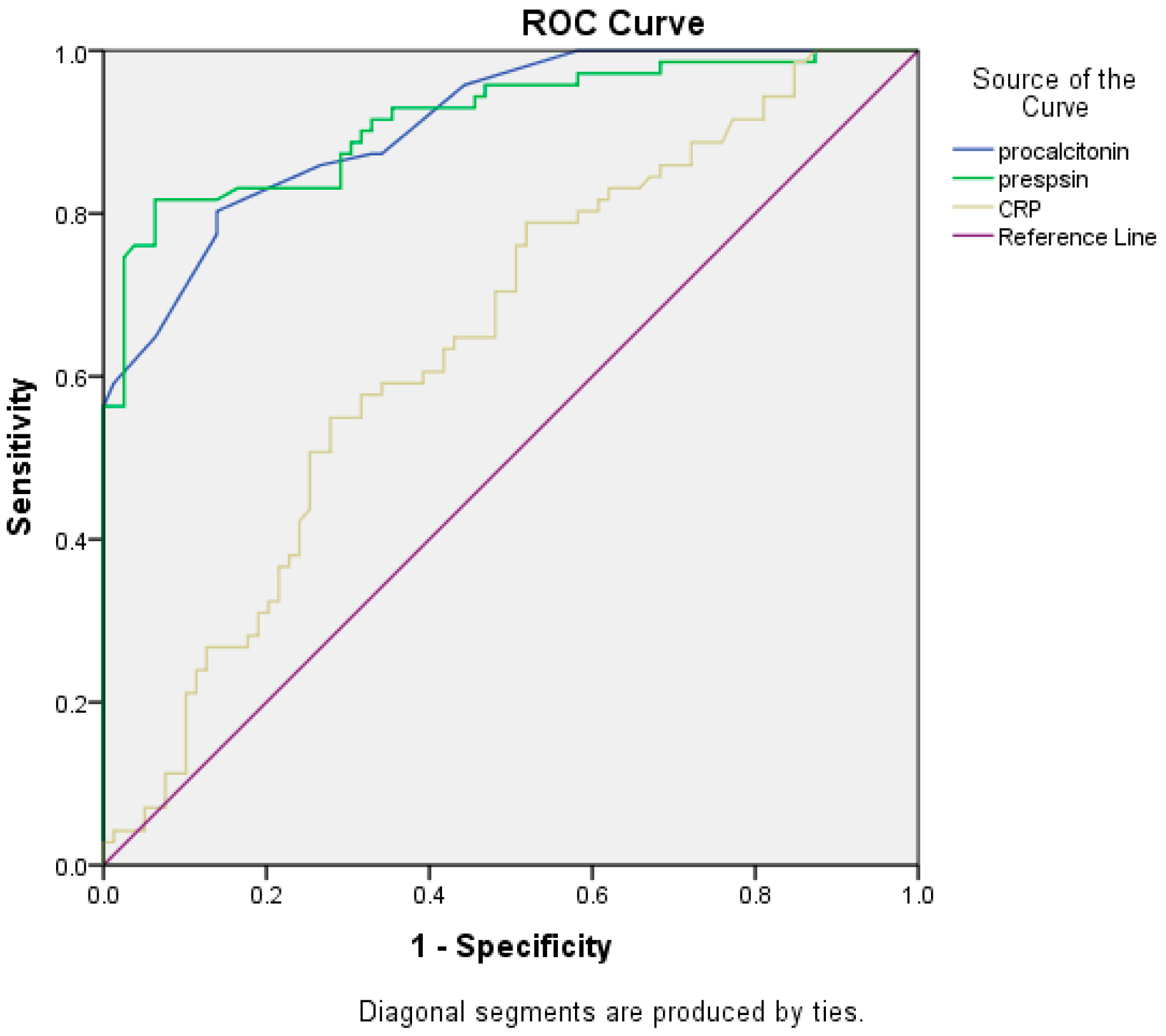
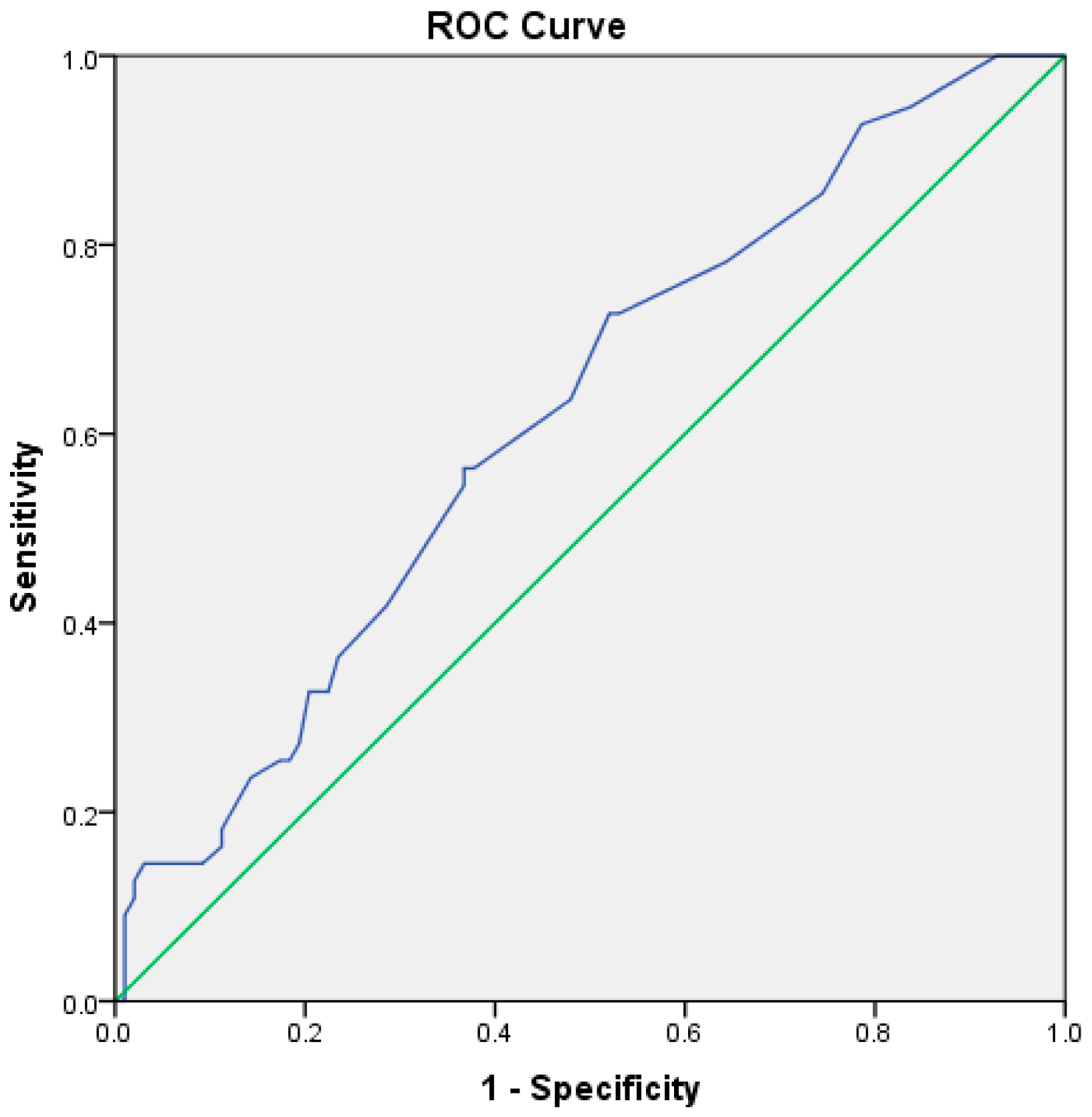
3.4. Biomarkers Accuracy for Infection Diagnosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arroyo, V.; Moreau, R.; Jalan, R. Acute-on-Chronic Liver Failure. N. Engl. J. Med. 2020, 382, 2137–2145. [Google Scholar] [CrossRef] [PubMed]
- Moreau, R.; Jalan, R.; Gines, P.; Pavesi, M.; Angeli, P.; Cordoba, J.; Durand, F.; Gustot, T.; Saliba, F.; Domenicali, M.; et al. Acute-on-Chronic Liver Failure Is a Distinct Syndrome That Develops in Patients with Acute Decompensation of Cirrhosis. Gastroenterology 2013, 144, 1426–1437.e9. [Google Scholar] [CrossRef] [PubMed]
- Piano, S.; Singh, V.; Caraceni, P.; Maiwall, R.; Alessandria, C.; Fernandez, J.; Soares, E.C.; Kim, D.J.; Kim, S.E.; Marino, M.; et al. Epidemiology and Effects of Bacterial Infections in Patients with Cirrhosis Worldwide. Gastroenterology 2019, 156, 1368–1380.e10. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Roberts, D.; Wood, K.E.; Light, B.; Parrillo, J.E.; Sharma, S.; Suppes, R.; Feinstein, D.; Zanotti, S.; Taiberg, L.; et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 2006, 34, 1589–1596. [Google Scholar] [CrossRef]
- Arvaniti, V.; D’Amico, G.; Fede, G.; Manousou, P.; Tsochatzis, E.; Pleguezuelo, M.; Burroughs, A.K. Infections in Patients with Cirrhosis Increase Mortality Four-Fold and Should Be Used in Determining Prognosis. Gastroenterology 2010, 139, 1246–1256.e5. [Google Scholar] [CrossRef]
- Piotrowski, D.; Boroń-Kaczmarska, A. Bacterial infections and hepatic encephalopathy in liver cirrhosis–prophylaxis and treatment. Adv. Med. Sci. 2017, 62, 345–356. [Google Scholar] [CrossRef]
- Villanueva, C.; Albillos, A.; Genescà, J.; Garcia-Pagan, J.C.; Brujats, A.; Calleja, J.L.; Aracil, C.; Bañares, R.; Morillas, R.M.; Poca, M.; et al. Bacterial infections adversely influence the risk of decompensation and survival in compensated cirrhosis. J. Hepatol. 2021, 75, 589–599. [Google Scholar] [CrossRef]
- Piano, S.; Bartoletti, M.; Tonon, M.; Baldassarre, M.; Chies, G.; Romano, A.; Viale, P.; Vettore, E.; Domenicali, M.; Stanco, M.; et al. Assessment of Sepsis-3 criteria and quick SOFA in patients with cirrhosis and bacterial infections. Gut 2018, 67, 1892–1899. [Google Scholar] [CrossRef]
- Fischer, P.; Grigoras, C.; Bugariu, A.; Nicoara-Farcau, O.; Stefanescu, H.; Benea, A.; Hadade, A.; Margarit, S.; Sparchez, Z.; Tantau, M.; et al. Are presepsin and resistin better markers for bacterial infection in patients with decompensated liver cirrhosis? Dig. Liver Dis. 2019, 51, 1685–1691. [Google Scholar] [CrossRef]
- Elefsiniotis, I. Presepsin levels in cirrhotic patients with bacterial infections and/or portal hypertension-related bleeding, presenting with or without acute kidney injury. Ann. Gastroenterol. 2018, 31, 604–612. [Google Scholar] [CrossRef]
- Ferrarese, A.; Frigo, A.C.; Mion, M.M.; Plebani, M.; Russo, F.P.; Germani, G.; Gambato, M.; Cillo, U.; Cattelan, A.; Burra, P.; et al. Diagnostic and prognostic role of presepsin in patients with cirrhosis and bacterial infection. Clin. Chem. Lab. Med. 2021, 59, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.H.; Wang, F.L.; Wu, M.S.; Jiang, B.Y.; Kao, W.L.; Chao, H.Y.; Wu, J.-Y.; Lee, C.-C. Serum procalcitonin and C-reactive protein levels as markers of bacterial infection in patients with liver cirrhosis: A systematic review and meta-analysis. Diagn. Microbiol. Infect. Dis. 2014, 80, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Shozushima, T.; Takahashi, G.; Matsumoto, N.; Kojika, M.; Endo, S.; Okamura, Y. Usefulness of presepsin (sCD14-ST) measurements as a marker for the diagnosis and severity of sepsis that satisfied diagnostic criteria of systemic inflammatory response syndrome. J. Infect. Chemother. 2011, 17, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Velissaris, D.; Zareifopoulos, N.; Karamouzos, V.; Karanikolas, E.; Pierrakos, C.; Koniari, I.; Karanikolas, M. Presepsin as a Diagnostic and Prognostic Biomarker in Sepsis. Cureus 2021, 13, e15019. [Google Scholar] [CrossRef]
- Yang, H.S.; Hur, M.; Yi, A.; Kim, H.; Lee, S.; Kim, S.N. Prognostic value of presepsin in adult patients with sepsis: Systematic review and meta-analysis. PLoS ONE 2018, 13, e0191486. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, D.; Liu, Y.N.; Wang, R.; Xie, L.X. The accuracy of presepsin (sCD14-ST) for the diagnosis of sepsis in adults: A meta-analysis. Crit. Care 2015, 19, 323. [Google Scholar] [CrossRef]
- Bota, D.P.; Van Nuffelen, M.; Zakariah, A.N.; Vincent, J.L. Serum levels of C-reactive protein and procalcitonin in critically ill patients with cirrhosis of the liver. J. Lab. Clin. Med. 2005, 146, 347–351. [Google Scholar] [CrossRef]
- Kan, W.C.; Huang, Y.T.; Wu, V.C.; Shiao, C.C. Predictive Ability of Procalcitonin for Acute Kidney Injury: A Narrative Review Focusing on the Interference of Infection. Int. J. Mol. Sci. 2021, 22, 6903. [Google Scholar] [CrossRef]
- Villarreal, E.; Vacacela, K.; Gordon, M.; Calabuig, C.; Alonso, R.; Ruiz, J.; Kot, P.; Babiloni, D.; Ramírez, P. Usefulness of procalcitonin for diagnosing infection in critically ill patients with liver cirrhosis. Med. Intensiva Engl. 2016, 40, 84–89. [Google Scholar] [CrossRef]
- Sato, S.; Sato, S.; Tsuzura, H.; Ikeda, Y.; Hayashida, S.; Takahashi, S.; Amano, N.; Murata, A.; Shimada, Y.; Iijima, K.; et al. Elevated serum procalcitonin levels and their association with the prognosis of patients with liver cirrhosis. Eur. J. Gastroenterol. Hepatol. 2020, 32, 1222–1228. [Google Scholar] [CrossRef]
- Zhang, Z.; Ma, K.; Yang, Z.; Cheng, Q.; Hu, X.; Liu, M.; Liu, Y.; Liu, T.; Zhang, M.; Luo, X.; et al. Development and Validation of a Clinical Predictive Model for Bacterial Infection in Hepatitis B Virus Related Acute-On-Chronic Liver Failure. Infect Dis. Ther. 2021, 10, 1347–1361. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Ze-Bing, H.; Li, H.; Zheng, X.; Chen, J.J.; Wang, X.B.; Qian, Z.; Liu, X.; Fan, X.; Hu, X.; et al. Early Diagnostic Biomarkers of Sepsis for Patients with Acute-on-Chronic Liver Failure: A Multicenter Study. Infect. Dis. Ther. 2021, 10, 281–290. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef]
- Novelli, S.; Morabito, V.; Ruberto, F.; Bini, F.; Marinozzi, F.; Pugliese, F.; Berloco, P.; Pretagostini, R. Diagnostic Value of Presepsin for Bacterial Infection in Cirrhosis: A Pilot Study. Transplant. Proc. 2020, 52, 1593–1600. [Google Scholar] [CrossRef]
- Khedher, S.; Fouthaili, N.; Maoui, A.; Lahiani, S.; Salem, M.; Bouzid, K. The Diagnostic and Prognostic Values of C-Reactive Protein and Procalcitonin during Bacterial Infections in Decompensated Cirrhosis. Gastroenterol. Res. Pract. 2018, 2018, 5915947. [Google Scholar] [CrossRef] [PubMed]
- Zaccherini, G.; Weiss, E.; Moreau, R. Acute-on-chronic liver failure: Definitions, pathophysiology and principles of treatment. JHEP Rep. 2021, 3, 100176. [Google Scholar] [CrossRef] [PubMed]
- Fukui, H. Leaky Gut and Gut-Liver Axis in Liver Cirrhosis: Clinical Studies Update. Gut Liver 2021, 15, 666–676. [Google Scholar] [CrossRef]
- Papp, M.; Tornai, T.; Vitalis, Z.; Tornai, I.; Tornai, D.; Dinya, T.; Sumegi, A.; Antal-Szalmas, P. Presepsin teardown—Pitfalls of biomarkers in the diagnosis and prognosis of bacterial infection in cirrhosis. World J. Gastroenterol. 2016, 22, 9172. [Google Scholar] [CrossRef]
- Ulla, M.; Pizzolato, E.; Lucchiari, M.; Loiacono, M.; Soardo, F.; Forno, D.; Morello, F.; Lupia, E.; Moiraghi, C.; Mengozzi, G.; et al. Diagnostic and prognostic value of presepsin in the management of sepsis in the emergency department: A multicenter prospective study. Crit. Care 2013, 17, R168. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | All Patients n = 153 | With Bacterial Infections n = 71 | Without Bacterial Infections n = 82 | p |
|---|---|---|---|---|
| Age, years, median, (IQR) | 60 (16) | 60 (20) | 59.5 (15) | 0.418 |
| Male sex, n (%) | 100 (65.4) | 45 (63.3) | 55 (67.1) | 0.632 |
| Comorbidities, n, (%) | 111 (72.5) | 51 (71.8) | 60 (73.1) | 0.853 |
| Cirrhosis alcoholic etiology, n, (%) | 134 (87.6) | 62 (87.3) | 72 (87.8) | 0.928 |
| Acute alcoholic hepatitis, n, (%) | 30 (19.6) | 14 (19.7) | 16 (19.5) | 0.974 |
| ACLF grade 1/2/3, n, (%) | 72/39/42 (47.1/25.5/27.4) | 33/17/21 (46.4/23.9/29.7) | 39/22/21 (47.5/26.8/25.7) | 0.839 |
| Child–Pugh class B/C, n, (%) | 30/123 (19.6/80.4) | 11/60 (15.4/84.5) | 19/63 (23.1/76.9) | 0.233 |
| Child–Pugh score median, (IQR) | 12 (3) | 12 (3) | 11 (2) | 0.007 |
| MELD score, median, (IQR) | 26 (13) | 28 (11) | 26 (17) | 0.002 |
| Variceal bleeding, n, (%) | 31 (20.3) | 11 (15.4) | 20 (24.4) | 0.172 |
| Ascites grade 1/2/3, n, (%) | 11/58/84 (7.2/37.9/54.9) | 5/28/38 (7.04/39.4/53.56) | 6/30/46 (7.3/36.6/56.) | 0.936 |
| CLIF ACLF score, median, (IQR) | 55.2 ± 10.3 | 57.5 (13) | 57 (14) | 0.049 |
| qSOFA score, median, IQR | 1 (1) | 2 (2) | 1 (0) | <0.001 |
| Total bilirubin, mg/dL, median, (IQR) | 8.9 (9.6) | 8.7 (13.1) | 7.8 (5.08) | 0.347 |
| Lactate median, (IQR) | 28 (18) | 31.8 (15.6) | 26.7 (26) | 0.919 |
| Creatinine mg/dL, median, (IQR) | 2.23 (1.17) | 2.23 (1.19) | 2.09 (2.34) | 0.723 |
| INR, median, (IQR) | 2.5 (0.88) | 2.6 (0.76) | 2.5 (0.23) | 0.700 |
| CRP, mg/dL, median (IQR) | 4.07 (5.7) | 5.65 (6.99) | 3.36 (4.80) | 0.023 |
| Presepsin, pg/mL, median (IQR) | 2038 (5314.5) | 6530 (6385) | 1045 (1715) | <0.001 |
| Procalcitonin, ng/mL, median (IQR) | 0.9 (1) | 1.5 (1.5) | 0.7 (0.75) | <0.001 |
| NSBB n, (%) | 60 (39.2) | 27 (38.0) | 33 (40.2) | 0.780 |
| PPI n, (%) | 25 (16.3) | 10 (14.1) | 15 (18.3) | 0.483 |
| Rifaximin n, (%) | 61 (39.9) | 29 (40.8) | 32 (39.02) | 0.819 |
| Hospitalization days, median (IQR) | 15 (12) | 15 (13) | 15 (11) | 0.544 |
| In hospital mortality n, (%) | 55 (35.9) | 27 (38.0) | 28 (34.1) | 0.618 |
| Parameter | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| OR | CI 95% | p-Value | OR | CI 95% | p-Value | |
| Male gender | 0.94 | 0.749–1.193 | 0.758 | 0.75 | 0.278–2.050 | 0.581 |
| Presepsin ≥ 2300 pg/mL | 2.88 | 1.917–4.350 | <0.001 | 3.65 | 1.394–9.588 | 0.008 |
| CRP ≥ 5.3 mg/dL | 1.64 | 1.129–2.405 | 0.013 | 2.07 | 0.789–5437 | 0.139 |
| PCT ≥0.9 ng/mL | 5.98 | 3.412–10.491 | <0.001 | 8.79 | 6.168–25.736 | <0.001 |
| Acute alcoholic hepatitis | 1.01 | 0.531–1.922 | 0.974 | 0.518 | 0.149–1.800 | 0.301 |
| MELD ≥ 18 | 1.20 | 1.064–1.374 | 0.008 | 7.37 | 1.416–18.430 | 0.018 |
| Child–Pugh class C | 1.10 | 0.942–1.284 | 0.323 | 1.03 | 0.313–3.404 | 0.958 |
| Previous NSBBs treatment | 0.94 | 0.635–1.406 | 0.779 | 1.04 | 0.326–3.304 | 0.949 |
| Previous rifaximin treatment | 1.04 | 0.709–1.545 | 0.819 | 1.86 | 0.608–5.693 | 0.949 |
| Previous PPIs treatment | 0.77 | 0.369–1.605 | 0.481 | 1.27 | 0.417–3.928 | 0.667 |
| Parameter | B | Wald | RR | 95% CI | p-Value |
|---|---|---|---|---|---|
| PCT ≥ 0.9 ng/mL | 0.608 | 3.570 | 1.83 | 0.978–3.453 | 0.059 |
| Presepsin ≥ 2300 pg/mL | 0.116 | 0.137 | 1.12 | 0.607–2.07 | 0.711 |
| CRP ≥ 5.3 mg/dL | 0.269 | 0.885 | 1.30 | 0.747–2.289 | 0.347 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Igna, R.; Gîrleanu, I.; Cojocariu, C.; Huiban, L.; Muzîca, C.; Sîngeap, A.-M.; Sfarti, C.; Chiriac, S.; Petrea, O.C.; Zenovia, S.; et al. The Role of Presepsin and Procalcitonin in Early Diagnosis of Bacterial Infections in Cirrhotic Patients with Acute-on-Chronic Liver Failure. J. Clin. Med. 2022, 11, 5410. https://doi.org/10.3390/jcm11185410
Igna R, Gîrleanu I, Cojocariu C, Huiban L, Muzîca C, Sîngeap A-M, Sfarti C, Chiriac S, Petrea OC, Zenovia S, et al. The Role of Presepsin and Procalcitonin in Early Diagnosis of Bacterial Infections in Cirrhotic Patients with Acute-on-Chronic Liver Failure. Journal of Clinical Medicine. 2022; 11(18):5410. https://doi.org/10.3390/jcm11185410
Chicago/Turabian StyleIgna, Razvan, Irina Gîrleanu, Camelia Cojocariu, Laura Huiban, Cristina Muzîca, Ana-Maria Sîngeap, Cătălin Sfarti, Stefan Chiriac, Oana Cristina Petrea, Sebastian Zenovia, and et al. 2022. "The Role of Presepsin and Procalcitonin in Early Diagnosis of Bacterial Infections in Cirrhotic Patients with Acute-on-Chronic Liver Failure" Journal of Clinical Medicine 11, no. 18: 5410. https://doi.org/10.3390/jcm11185410
APA StyleIgna, R., Gîrleanu, I., Cojocariu, C., Huiban, L., Muzîca, C., Sîngeap, A.-M., Sfarti, C., Chiriac, S., Petrea, O. C., Zenovia, S., Nastasa, R., Cuciureanu, T., Stafie, R., Stratina, E., Rotaru, A., Stanciu, C., Blaj, M., & Trifan, A. (2022). The Role of Presepsin and Procalcitonin in Early Diagnosis of Bacterial Infections in Cirrhotic Patients with Acute-on-Chronic Liver Failure. Journal of Clinical Medicine, 11(18), 5410. https://doi.org/10.3390/jcm11185410