1. Introduction
Pachychoroid spectrum diseases [
1] (PSD) include a variety of clinical findings such as central serous chorioretinopathy (CSC) with serous retinal detachment (SRD) [
2,
3] of the sensory retina, choroidal vascular hyperpermeability [
4], late filling of dye into the choroid on indocyanine green angiography (ICGA) in choroid [
4], pachychoroid [
3], pachyveins [
5], thinning (attenuation) of the choriocapillaris layer, anastomosis in vortex veins [
4,
6], thickened sclera [
7], loculation of fluid in suprachoroid [
8,
9], and pigment epitheliopathy [
10], all of which can result in not only CSC but also pachychoroid neovasculopathy (PNV) [
11] and polypoidal choroidal vasculopathy (PCV) [
12], similar in appearance to age-related macular degeneration (AMD).
Some theories as to the pathogenesis of these entities have been proposed. Kishi et al. [
4] found filling delay areas in the choriocapillaris and dilation of the emissary vortex vein on ICGA and suggested that the blood flow into the choriocapillaris is delayed as a result of congestion of the dominant vortex veins. Imanaga et al. [
7] found sclera thickening in CSC and postulated that the scleral thickening may choke the emissary vortex veins, eliciting the emissary vortex vein congestion. However, this vortex vein congestion theory cannot consistently explain all the above-mentioned characteristic findings. Although this theory may suggest that pachyveins result from blood congestion caused by choking the vortex veins, it is still questionable whether longstanding congestion in choriocapillaris, venules, and vortex veins elicit vascular endothelial growth factor (VEGF)-production which may finally cause PNV and PCV. Dropout of choriocapillaris is unlikely to occur by compression of a pachyvein, because capillary pressure is higher than venous pressure. On the other hand, there will be another possibility that pigment epitheliopathy as a primary lesion may alter VEGF-production, followed by choroidal vascular hyperpermeability and incidence of CSC, PNV, and PCV. This hypothesis needs to explain that alteration of retinal pigment epithelium and choriocapillaris can elicit other characteristic findings such as pachychoroid and pachyveins.
Since most of these findings are related to the blood flow in the choroid, there is a possibility that a hydrodynamic analysis may provide clues as to the possible common pathogenesis to the entities we name PSD.
We attempted to analyze and interpret these findings based on the physics theorems of Equation of Continuity and Bernoulli’s Principle of fluid mechanics [
13].
2. Methods
We applied the two following representative theorems of fluid dynamics in physics to the above clinical findings and phenomena.
Equation of Continuity [
13]: Q = A · V
Q: (blood) flow volume, A: sectional area of vessel, V: (blood) flow velocity.
This equation is based on the principle of “Conservation of mass”. Thus, for a fluid through a pipe at all the cross-section, the quantity of fluid per second is constant. As the equation shows, a decrease in the flow volume occurs simultaneously with a decrease in the flow velocity and/or sectional area, and vice versa.
- 2.
Bernoulli’s Principle [
13]: 1/2 V
2 + P/ρ = Constant
V: (blood) flow velocity, P: static (blood) pressure, ρ: (blood) fluid density
This equation relates velocity, static pressure, and elevation changes of a fluid in motion. The equation can be obtained by integrating Euler’s equation along the streamline for a constant fluid.
Since gravitational g and elevation z for the choroid are a small part of papillo-macular region and always same for a patient during the examination, they can be regarded as constant. Hence, the equation can be formed as
As the equation shows, a decrease in the velocity of a fluid occurs simultaneously with an increase in static pressure, and vice versa.
These theorems can be applied to non-viscous, noncompressible fluids [
13]. The viscosity of a fluid can be expressed as the coefficient of viscosity [
14]: water 1 cp (centi poise), blood plasma 1.2–1.3 cp, blood 3.5–5.0 cp, olive oil 80 cp [
15]. Since blood is similar in its consistency to water, it can be regarded as non-viscous. Noncompressibility is defined as the ratio of the speed of a flow to the speed of sound and expressed in Mach number [
13,
16]. Accordingly, when the speed is less than Mach 0.3, the fluid is noncompressible [
16]. Blood flow can be considered to meet this definition (arterial velocity: 1.9–19.0 cm/s, venous velocity: 1.5–7.1 cm/s in the index finger [
17]).
3. Results
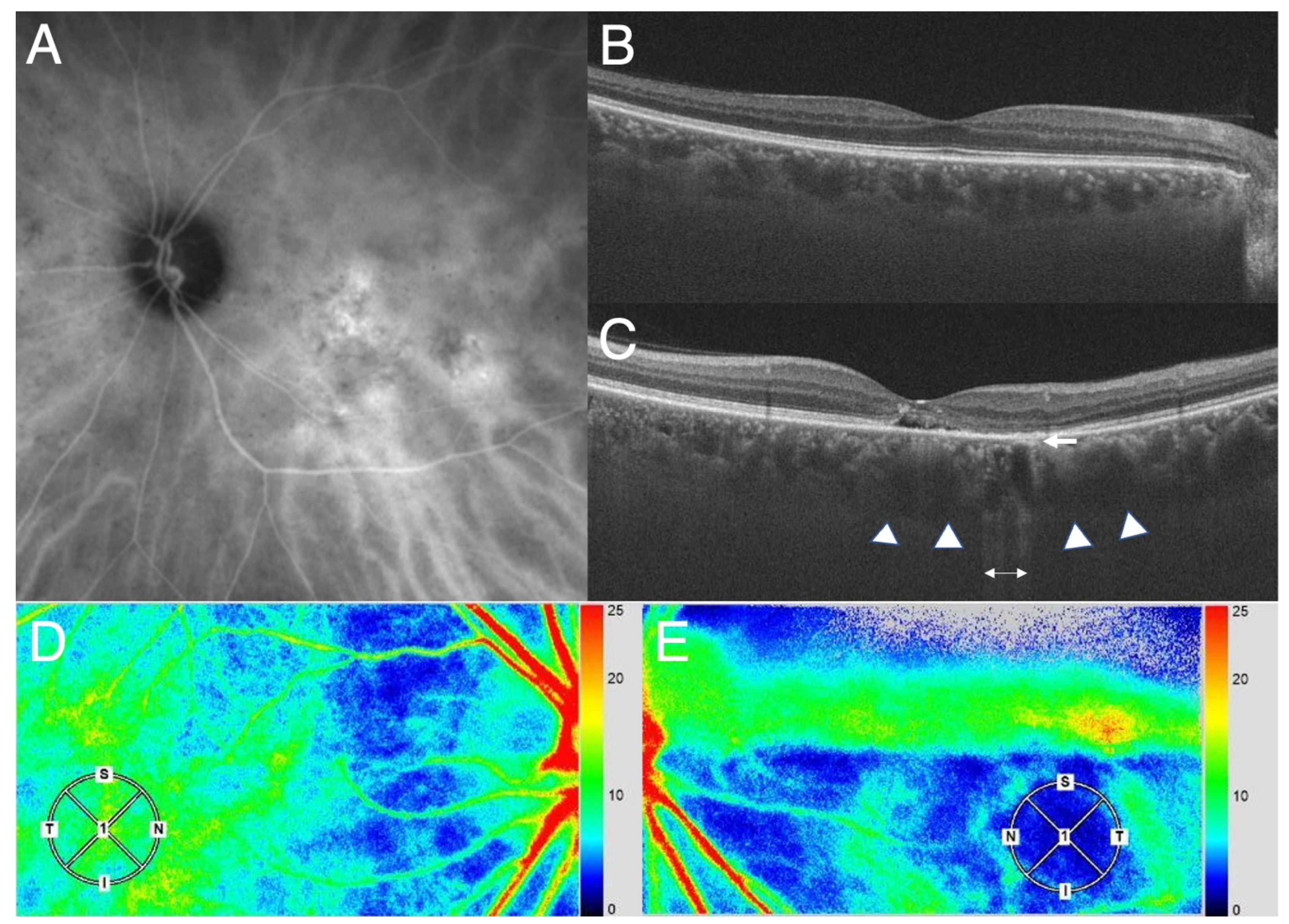
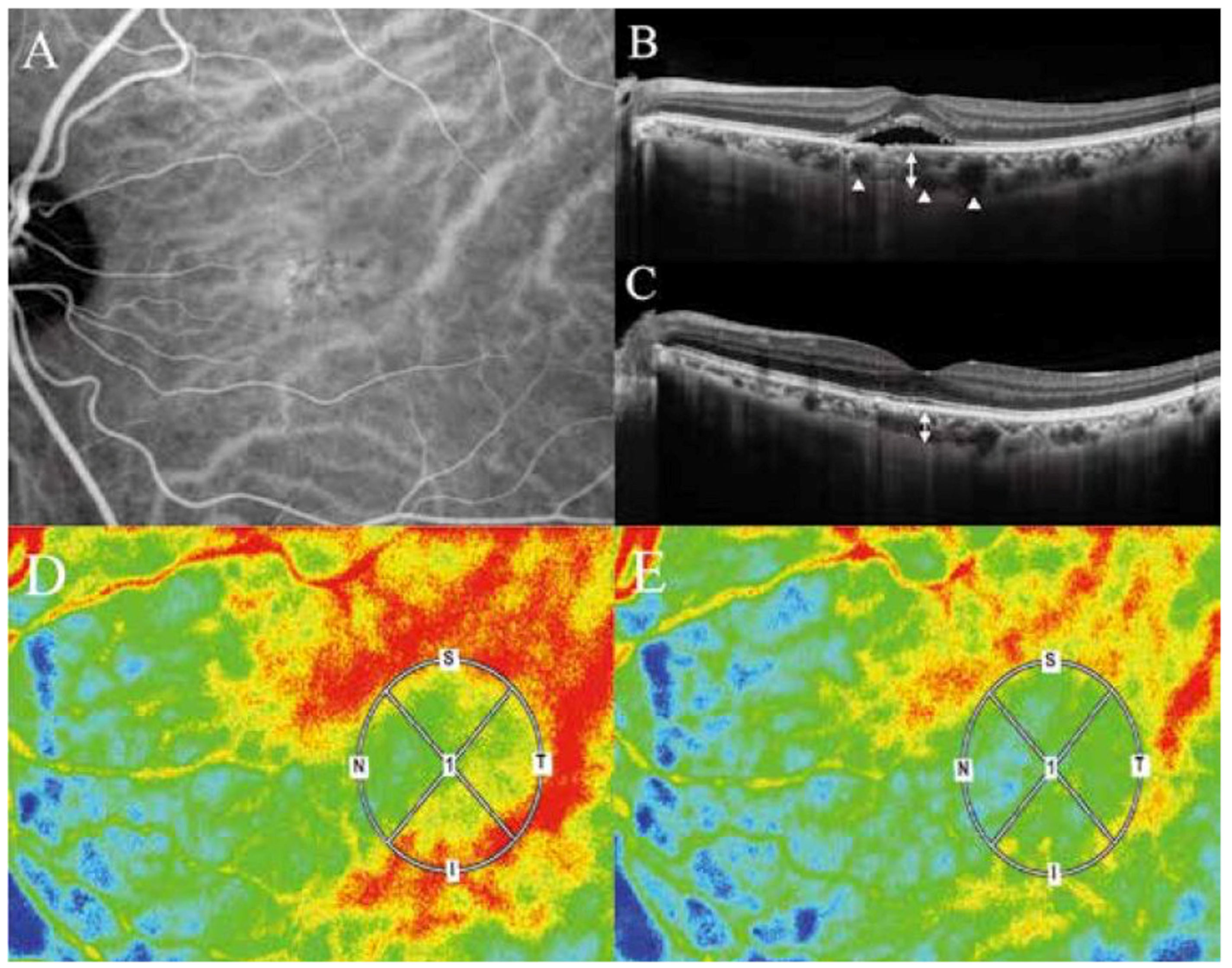
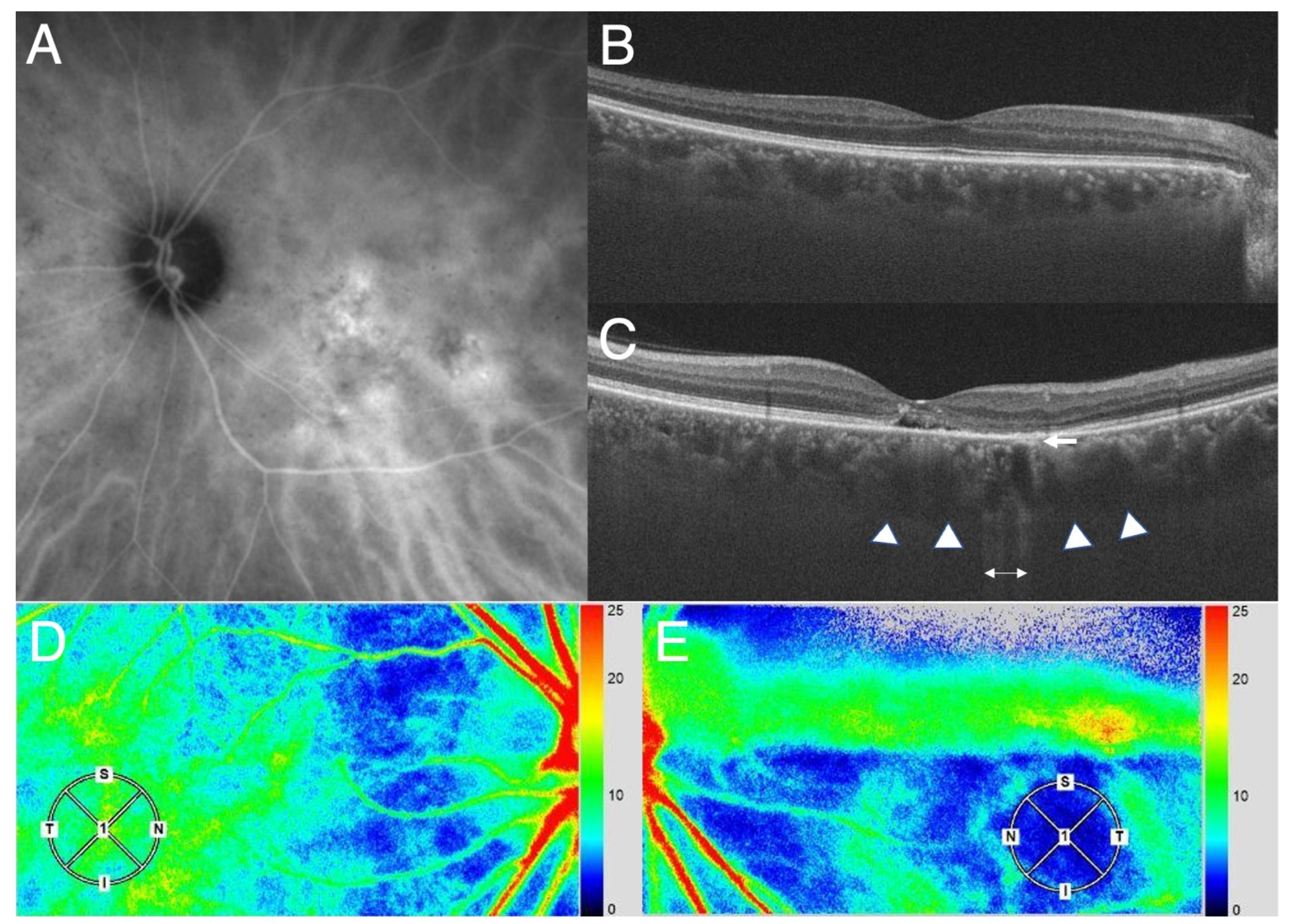
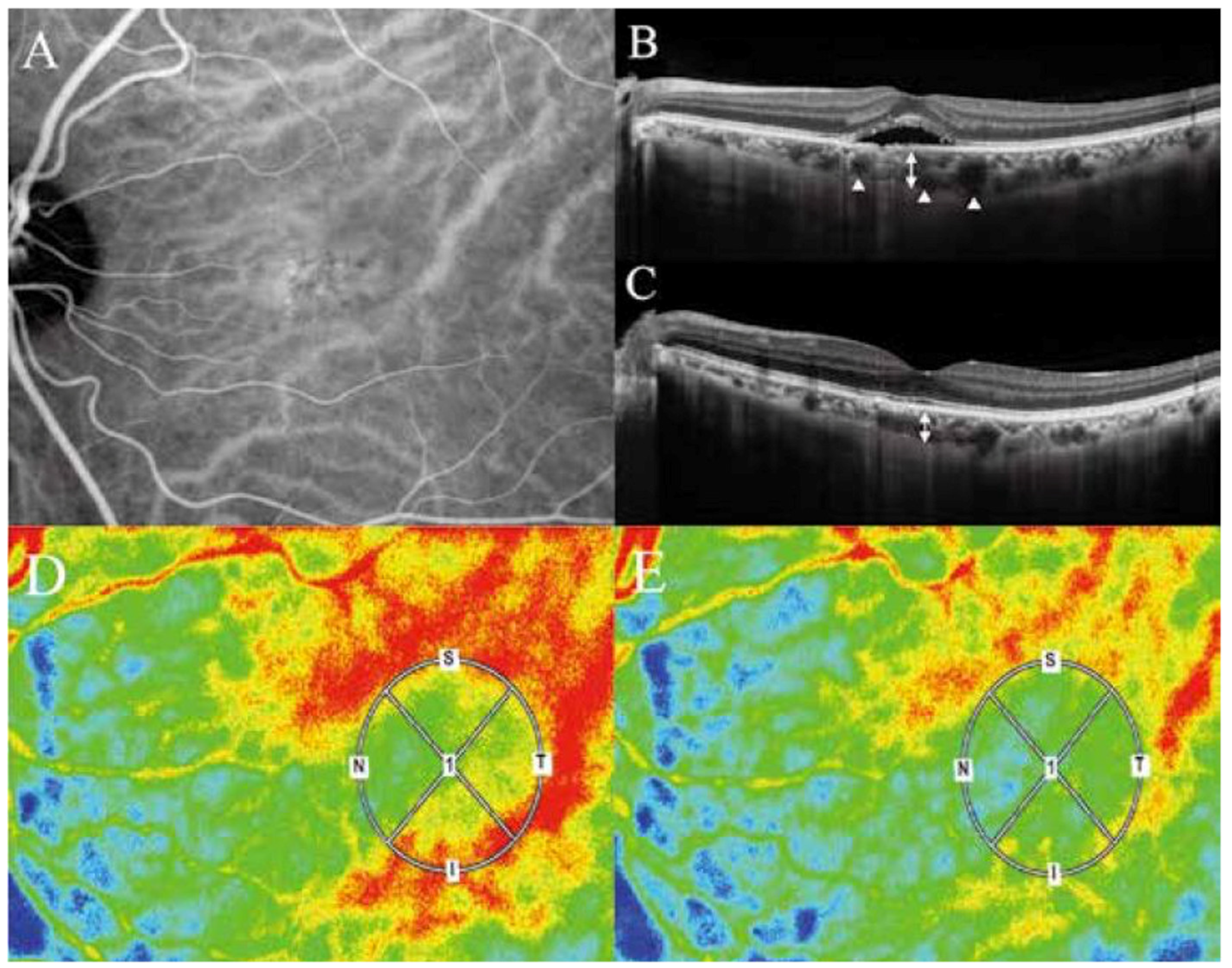
Applying the variety of clinical presentations of PSD to these physics equations, it is important to first recognize that the hyperpermeability [
4] of the choriocapillaris will elicit blood plasma exudation into the interstitial space surrounding the choriocapillaris forming pachychoroid driven by oncotic pressure of exudates including albumin and fibrinogen. The concomitant increase of hydrostatic pressure in the interstitial space of the choroid, when accompanied by the disruption of blood retinal barrier in the retinal pigment epithelium, will lead to exudation and/or transudation into the sensory retina, forming SRD. This may result in a decrease in blood flow volume (Q) in the choriocapillaris, since the exudate -in contrast to the transudate- will not be totally absorbed into the choriocapillaris at the arteriole side. A decrease in (Q) simultaneously elicits a decrease in the blood flow velocity (V), according to the Equation of Continuity. This decrease in the blood flow velocity is clinically observable as filling delay into choriocapillaris on ICGA [
4] and on laser speckle flowgraphy (LSFG) (
Figure 1 and
Figure 2).
When a decrease in the blood flow velocity (V) exists, Bernoulli’s Principle dictates that an increase in the static blood pressure (P) will simultaneously occur in the venules. Furthermore, since the blood density ρ may increase due to the exudation, its reciprocal, the blood pressure P will become much greater to keep the Bernoulli’s equation constant. With the decelerated velocity of the blood flow, the elicited higher blood pressure may expand Sattler and Haller vessels, forming pachyveins.
4. Discussion
Applying these two physics theorems of fluid mechanics to the large variety of clinical findings in the PSD entities, one must consider mathematical-physical equations and relate them to the hyperpermeability of the choriocapillaris and disruption of the blood retinal barrier of the pigment epithelium with CSC. The two theorems lead to the conclusion that pachyveins may be the result of a blood pressure increase occurring simultaneously in the wake of a decrease in the blood flow velocity in the choriocapillaris and choroidal venules. Therefore, hyperpermeability of the choriocapillaris including pigment epitheliopathy may be considered as the primary lesion of PSD [
20,
21,
22]. Lipid accumulation in Bruch’s membrane initiates at 30 years of age, thereafter, decreasing the hydraulic conductivity of Bruch’s membrane with aging [
20,
21]. Schmidt-Erfurth et al. [
22] showed that lipid accumulation in Bruch’s membrane enhanced expression of VEGF under the retinal pigment epithelium in low density lipoprotein receptor knockout mice, an experimental model of lipid accumulation in aging eyes. We speculate that lipid accumulation may be associated with upregulation of VEGF secreted from the retinal pigment epithelium and focal pigment epitheliopathy may affect amount and dynamics of VEGF accumulated between the retinal pigment epithelium and Bruch’s membrane, resulting in both attenuation and hyperpermeability of the choriocapillaris. In truth, CSC generally develops over 30 years of age. Moreover, retinal pigment alteration seems to be necessary for PSD, while either pachychoroid or pachyveins is not always present in all cases of PSD. Thus, the pachychoroid including pachyveins alone is not the primary lesion rather the secondary accompanying phenomenon in these disorders.
The effect of the vortex vein compression and its consequence by the thickened sclera [
7,
8,
9] can be explained using the principles discussed here. The compression of the vortex vein delays the blood flow velocity (V). According to the Bernoulli’s Principle, the resulting delayed blood flow will elicit simultaneously a blood pressure (P) rise which can expand Sattler and Haller vessels. However, whether the compression of the vortex veins as the primary cause can elicit pigment epitheliopathy followed by VEGF-production, PNV, and PCV is unanswered. The thickened sclera and loculation of fluid in suprachoroid are explainable by diffusion of oncotic pressure-driven exudates such as albumin in the interstitial space of the choroid, because even molecules as large as antibodies can pass through the sclera [
23].
All of above considerations emphasize the important role of the blood pressure in pachyveins and pachychoroid formation which, to date, has received scant attention. When, in the future, the means to ascertain the blood pressure in the Haller layer becomes available, the above theoretical considerations can be corroborated. We are now developing a method to measure the blood pressure of choroid using LSFG.
The arising important issue will be what then and where the primary lesion of PSD is. The choking of vortex veins eliciting congestion in the choroidal circulation [
7] could be a prime consideration. The congestion by the thickened sclera alone may be able to initially raise the blood pressure in the choriocapillaris and Haller layer. When this raised pressure exceeds the so-called plasma-osmotic pressure in the choriocapillaris, the transudate around the choriocapillaris can no longer be absorbed into the capillaries, resulting in a condition of chronic edema. However, whether this condition can be the cause of pigment epitheliopathy, hyperpermeability of choriocapillaris and choroidal neovascularization, resulting in the exudation into the interstitial space is still unanswered.
On the other hand, even in eyes without the primary vortex vein congestion by the thickened sclera, when the blood plasma components exit the choriocapillaris due to its increased permeability, the blood flow slows down, and the blood pressure, simultaneously, rises hydrodynamically in accord with Bernoulli’s Principle resulting in an expansion of Haller veins, as shown in this study. Thus, the blood pressure rises and congestion in the choroidal circulation can occur as a secondary result of the hyperpermeability of the choriocapillaris and the disruption of the blood retinal barrier. The primary lesion then would be the pigment epithelium, Bruch’s membrane and/or choriocapillaris [
18]. In this case, the thickened sclera would then be considered as secondary lesions. It could be caused by an imbibition of the edema and/or interstitial exudates into the corresponding sclera region.
Finally, the limitation of our study is that the above results and discussions are based merely on the theoretical considerations. In the future studies, we will measure the difference in the blood flow speed in the choroid of the macula region, as shown in the
Figure 1 and
Figure 2, using LSFG in a cohort of the patients with PSD. The blood pressure will be measured using LSFG as well. These may help corroborate the theory.
5. Conclusions
According to Bernoulli’s Principle of fluid mechanics, a decrease in the velocity of blood flow in the choriocapillaris in CSC and PSD occurs simultaneously in an increase in the blood pressure of the vortex veins, which may expand the venules. Pachyveins can be the result of a blood pressure increase occurring simultaneously in the wake of a decrease in the blood flow velocity in the choriocapillaris, suggesting that pigment epitheliopathy including hyperpermeability of the choriocapillaris may be the primary causative lesion of pachychoroid-spectrum diseases.
Author Contributions
Conceptualization, O.N. and T.Y. All authors have read and agreed to the published version of the manuscript.
Funding
Tsutomu Yasukawa was supported by Grant-in-Aid for Scientific Research (B) 22H03243 from the Japan Society for the Promotion of Science.
Institutional Review Board Statement
This study did not require ethical approval.
Informed Consent Statement
Informed consent was obtained from the patienrt involved in the study.
Data Availability Statement
The study did not report any data.
Conflicts of Interest
Tsutomu Yasukawa: Novartis Pharma (F, R), Santen Pharmaceutical (R), Bayer (R). Okihiro Nishi has no financial disclosures. The authors attest that they meet the current ICMJE criteria for authorship.
References
- Cheung, C.M.G.; Lee, W.K.; Koizumi, H.; Dansingani, K.; Lai, T.Y.Y.; Freund, K.B. Pachychoroid Diseases. Eye 2019, 33, 14–33. [Google Scholar] [CrossRef]
- Prünte, C.; Flammer, J. Choroidal Capillary and Venous Congestion in Central Serous Chorioretinopathy. Am. J. Ophthalmol. 1996, 121, 26–34. [Google Scholar] [CrossRef]
- Imamura, Y.; Fujiwara, T.; Margolis, R.; Spaide, R.F. Enhanced depth imaging optical coherence tomography of the choroid in central serous chorioretinopathy. Retina 2009, 29, 1469–1473. [Google Scholar] [CrossRef]
- Kishi, S.; Matsumoto, H.; Sonoda, S.; Hiroe, T.; Sakamoto, T.; Akiyama, H. Geographic filling delay of the choriocapillaris in the region of dilated asymmetric vortex veins in central serous chorioretinopathy. PLoS ONE 2018, 13, e0206646. [Google Scholar] [CrossRef]
- Kim, S.; Chung, Y.; Kim, J.; Lee, K. Choroidal thickness in patients with central serous chorioretinopathy: Assessment of haller’s and sattler’s layers. Acta Ophthalmol. 2015, 93, 1652–1657. [Google Scholar] [CrossRef]
- Matsumoto, H.; Hoshino, J.; Mukai, R.; Nakamura, K.; Kikuchi, Y.; Kishi, S.; Akiyama, H. Vortex Vein Anastomosis at the Watershed in Pachychoroid Spectrum Diseases. Ophthalmol. Retin. 2020, 4, 938–945. [Google Scholar] [CrossRef]
- Imanaga, N.; Terao, N.; Nakamine, S.; Tamashiro, T.; Wakugawa, S.; Sawaguchi, K.; Koizumi, H. Scleral thickness in central cerous chorioretinopathy. Ophthalmol. Retin. 2021, 5, 285–291. [Google Scholar] [CrossRef]
- Spaide, R.F.; Ryan, E.H., Jr. Loculation of fluid in the posterior choroid in eyes with central serous chorioretinopathy. Am. J. Ophthalmol. 2015, 160, 1211–1216. [Google Scholar] [CrossRef]
- Imanaga, N.; Terao, N.; Sawaguchi, S.; Tamashiro, T.; Wakugawa, S.; Yamauchi, Y.; Koizumi, H. Clinical Factors Related to Loculation of Fluid in Central Serous Chorioretinopathy. Am. J. Ophthalmol. 2021, 235, 197–203. [Google Scholar] [CrossRef]
- Warrow, D.J.; Hoang, Q.V.; Freund, K.B. Pachychoroid pigment epitheliopathy. Retina 2013, 33, 1659–1672. [Google Scholar] [CrossRef] [PubMed]
- Pang, C.E.; Freund, K.B. Pachychoroid neovasculopathy. Retina 2015, 35, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.K.; Baek, J.; Dansingani, K.K.; Lee, J.H.; Freund, K.B. Choroidal morphology in eyes with polypoidal choroidal vasculopathy and normal or subnormal subfoveal choroidal thickness. Retina 2016, 36, S73–S82. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, S. Fluid of kinetics: Continuity equation, Fluid dynamics: Bernoulli’s equation. In Textbook of Fluid Mechanics; CBS Publ & Dist Pvt Ltd.: Delhi, India, 2017; Volume 48, p. 104. [Google Scholar]
- Nader, E.; Skinner, S.; Romana, M.; Fort, R.; Lemonne, N.; Guillot, N.; Gauthier, A.; Antoine-Jonville, S.; Renoux, C.; Hardy-Dessources, M.-D.; et al. Blood Rheology: Key Parameters, Impact on Blood Flow, Role in Sickle Cell Disease and Effects of Exercise. Front. Physiol. 2019, 10, 1329. [Google Scholar] [CrossRef] [PubMed]
- Nierat, T.H.; Musameh, M.; Abdel-Raziq, I.R. Temperature-dependence of olive oil viscosity. Mater. Sci. 2014, 11, 233–238. [Google Scholar]
- Matsuo, K. Compressible Fluid Dynamics: Theory and Analysis in Internal Flow; Ohmsha: Tokyo, Japan, 2020; p. 33. ISBN 978-4-274-06969-7. [Google Scholar]
- Klarhöfer, M.; Csapo, B.; Balassy, C.; Szeles, J.; Moser, E. High-resolution blood flow velocity measurements in the human finger. Magn. Reson. Med. 2001, 45, 716–719. [Google Scholar] [CrossRef] [PubMed]
- Saito, W.; Hashimoto, Y.; Hirooka, K.; Ishida, S. Changes in choroidal blood flow velocity in patients diagnosed with central serous chorioretinopathy during follow-up for pachychoroid pigment epitheliopathy. Am. J. Ophthalmol. Case Rep. 2020, 18, 100651. [Google Scholar] [CrossRef]
- Saito, W.; Hashimoto, Y.; Hirooka, K.; Ishida, S. Choroidal thickness changes in a patient diagnosed with central serous chorioretinopathy during follow-up for pachychoroid pigment epitheliopathy. Retin. Cases Brief Rep. 2021, 15, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.J.; Hussain, A.A.; Marshall, J. Age-related variation in the hydraulic conductivity of Bruch’s membrane. Investig. Ophthalmol. Vis. Sci. 1995, 36, 1290–1297. [Google Scholar]
- Huang, J.-D.; Curcio, C.A.; Johnson, M. Morphometric Analysis of Lipoprotein-like Particle Accumulation in Aging Human Macular Bruch’s Membrane. Investig. Opthalmol. Vis. Sci. 2008, 49, 2721–2727. [Google Scholar] [CrossRef]
- Schmidt-Erfurth, U.; Rudolf, M.; Funk, M.; Hofmann-Rummelt, C.; Franz-Haas, N.-S.; Aherrahrou, Z.; Schlo¨tzer-Schrehardt, U. Ultrastructural Changes in a Murine Model of Graded Bruch Membrane Lipoidal Degeneration and Corresponding VEGF164Detection. Investig. Opthalmol. Vis. Sci. 2008, 49, 390–398. [Google Scholar] [CrossRef] [Green Version]
- Ambati, J.; Gragoudas, E.S.; Miller, J.W.; You, T.T.; Miyamoto, K.; Delori, F.C.; Adamis, A.P. Transscleral delivery of bioactive protein to the choroid and retina. Investig. Ophthalmol. Vis. Sci. 2000, 41, 1186–1191. [Google Scholar]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



{kind=link}
{kind=link}