
Advances in the Non-Operative Management of Multidirectional Instability of the Glenohumeral Joint
Abstract
1. Introduction
2. Aetiology
2.1. Passive Factors
2.2. Scapula
2.3. Altered Muscle Control
2.4. Altered Proprioception and Central Function
3. Classification
4. Clinical Presentation
4.1. History
4.2. Physical Examination
- A positive test for at least one direction (anterior and/or posterior), for at least two of three following tests:
4.3. Assessing Motor Control Deficits and the Effect of Correction
- The therapist choosing an objective test while noting the patient’s faulty scapular and/or humeral head biomechanics during that test in association with symptoms;
- Applying manual correction of the scapula, humeral head and possibly a combination of both to correct the faulty mechanics while reassessing the test, noting any improvements in range of motion, pain, subluxations/dislocations and/or strength on reassessment.
5. Treatment
6. The WIP1 Updates
6.1. Assessment of Manual Correction
6.2. Treatment
6.3. Return to Sport and Detecting Change with Treatment
6.4. Dosage, Timelines and Discharge
6.5. Associated Factors That Alter the Focus of Rehabilitation
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ruiz Ibán, M.A.; Díaz Heredia, J.; García Navlet, M.; Serrano, F.; Santos Oliete, M. Multidirectional Shoulder Instability: Treatment. Open Orthop. J. 2017, 11, 812–825. [Google Scholar] [CrossRef] [PubMed]
- Johansson, K. Multidirectional instability of the glenohumeral joint: An unstable classification resulting in uncertain evidence-based practice. Br. J. Sports Med. 2016, 50, 1105. [Google Scholar] [CrossRef] [PubMed]
- Ren, H.; Bicknell, R.T. From the unstable painful shoulder to multidirectional instability in the young athlete. Clin. Sports Med. 2013, 32, 815–823. [Google Scholar] [CrossRef] [PubMed]
- Misamore, G.W.; Sallay, P.I.; Didelot, W. A longitudinal study of patients with multidirectional instability of the shoulder with seven- to ten-year follow-up. J. Shoulder Elbow Surg. 2005, 14, 466–470. [Google Scholar] [CrossRef]
- Watson, L.; Warby, S.A.; Balster, S.; Lenssen, R.; Pizzari, T. The treatment of multidirectional instability with an exercise program: Part 1. Shoulder Elb. 2016, 8, 271–278. [Google Scholar] [CrossRef]
- Watson, L.; Warby, S.A.; Balster, S.; Lenssen, R.; Pizzari, T. The treatment of multidirectional instability with an exercise program: Part 2. Shoulder Elb. 2017, 9, 46–53. [Google Scholar] [CrossRef]
- Ganderton, C.L.; Tirosh, O.; Munro, D.; Mayer, D.; Ross, L.; Balster, S.; Watson, L.; Warby, S. Rehabilitation for atraumatic shoulder instability in circus arts performers: Delivery via telehealth. J. Shoulder Elbow Surg. 2022, 31, e246–e257. [Google Scholar] [CrossRef]
- Watson, L.; Balster, S.; Lenssen, R.; Hoy, G.; Pizzari, T. The effects of a conservative rehabilitation program for multidirectional instability of the shoulder. J. Shoulder Elbow Surg. 2018, 27, 104–111. [Google Scholar] [CrossRef]
- Ganderton, C.L.; Tirosh, O.; Munro, D.; Meyer, D.; Lenssen, R.; Balster, S.; Watson, L.; Warby, S. Comparison of two exercise rehabilitation programs for multidirectional instability of the glenohumeral joint: A randomised controlled trial. Am. J. Sports Med. 2017, 31, e246–e257. [Google Scholar] [CrossRef]
- Warby, S.A.; Watson, L.; Ford, J.J.; Hahne, A.J.; Pizzari, T. Multidirectional instability of the glenohumeral joint: Etiology, classification, assessment, and management. J. Hand Ther. 2017, 30, 175–181. [Google Scholar] [CrossRef]
- Lim, C.-O.; Park, K.-J.; Cho, B.-K.; Kim, Y.-M.; Chun, K.-A. A new screening method for multidirectional shoulder instability on magnetic resonance arthrography: Labro-capsular distance. Skeletal Radiol. 2016, 45, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Merolla, G.; Cerciello, S.; Chillemi, C.; Paladini, P.; De Santis, E.; Porcellini, G. Multidirectional instability of the shoulder: Biomechanics, clinical presentation, and treatment strategies. Eur. J. Orthop. Surg. Traumatol. 2015, 25, 975–985. [Google Scholar] [CrossRef] [PubMed]
- Ayekoloye, C.; Nwangwu, O. Multidirectional instability of the shoulder (MDI)—Focus on non-operative management. Eur. J. Physiother 2019, 21, 197–203. [Google Scholar] [CrossRef]
- Hsu, Y.C.; Pan, R.Y.; Shih, Y.Y.; Lee, M.S.; Huang, G.S. Superior-capsular elongation and its significance in atraumatic posteroinferior multidirectional shoulder instability in magnetic resonance arthrography. Acta Radiol. 2010, 51, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Kim, N.R.; Moon, S.G.; Ko, S.M.; Park, J.Y. Multidirectional instability of the shoulder: Rotator interval dimension and capsular laxity evaluation using MR arthrography. Skeletal Radiol. 2013, 42, 231–238. [Google Scholar] [CrossRef]
- Finnoff, J.T.; Doucette, S.; Hicken, G. Glenohumeral instability and dislocation. Phys. Med. Rehabil. Clin. N. Am. 2004, 15, 575–605. [Google Scholar] [CrossRef]
- Byström, M.G.; Rasmussen-Barr, V.; Grooten, W.J.A. Motor Control Exercises Reduces Pain and Disability in Chronic and Recurrent Low Back Pain: A Meta-Analysis. Spine 2013, 38, E350–E358. [Google Scholar] [CrossRef] [PubMed]
- Rodeo, S.A.; Suzuki, K.; Yamauchi, M.; Bhargava, M.; Warren, R.F. Analysis of collagen and elastic fibers in shoulder capsule in patients with shoulder instability. Am. J. Sports Med. 1998, 26, 634–643. [Google Scholar] [CrossRef]
- Saccomanno, M.F.; Fodale, M.; Capasso, L.; Cazzato, G.; Milano, G. Generalized joint laxity and multidirectional instability of the shoulder. Joints 2013, 1, 171–179. [Google Scholar] [CrossRef]
- Navlet, M.G.; Asenjo-Gismero, C.V. Multidirectional Instability: Natural History and Evaluation. Open Orthop. J. 2017, 11, 861–874. [Google Scholar] [CrossRef][Green Version]
- McFarland, E.G.; Campbell, G.; McDowell, J. Posterior Shoulder Laxity in Asymptomatic Athletes. Am. J. Sports Med. 1996, 24, 468–471. [Google Scholar] [CrossRef] [PubMed]
- Castori, M.; Tinkle, B.; Levy, H.; Grahame, R.; Malfait, F.; Hakim, A. A framework for the classification of joint hypermobility and related conditions. Am. J. Med. Genet. C Semin. Med. Genet. 2017, 175, 148–157. [Google Scholar] [CrossRef]
- Brown, G.; Tan, J.; Kirkley, A. The lax shoulder in females: Issues, answers, but many more questions. Clin. Orthop. Relat. Res. 2000, 372, 110–122. [Google Scholar] [CrossRef]
- VandenBerghe, G.; Hoenecke, H.; Fronek, J. Glenohumeral joint instability: The orthopedic approach. Semin. Musculoskelet. Radiol. 2009, 43, 259–264. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Guerrero, P.; Busconi, B.; Deangelis, N.; Powers, G. Congenital instability of the shoulder joint: Assessment and treatment options. J. Orthop. Sports Phys. Ther. 2009, 39, 124–134. [Google Scholar] [CrossRef][Green Version]
- Edelson, J.G. Localized glenoid hypoplasia. An anatomic variation of possible clinical significance. Clin. Orthop. Relat. Res. 1995, 321, 189–195. [Google Scholar]
- Kim, S.H.; Noh, K.C.; Park, J.S.; Ryu, B.D.; Irvin, O. Loss of chondrolabral containment of the glenohumeral joint in atraumatic posteroinferior multidirectional instability. J. Bone Joint Surg. 2005, 87, 92–98. [Google Scholar] [CrossRef]
- Spanhove, V.; Van Daele, M.; Van den Abeele, A.; Rombaut, L.; Castelein, B.; Calders, P.; Malfait, F.; Cools, A.; De Wandele, I. Muscle activity and scapular kinematics in individuals with multidirectional shoulder instability: A systematic review. Ann. Phys. Rehabil. Med. 2021, 64, 101457. [Google Scholar] [CrossRef]
- Ogston, J.B.; Ludewig, P.M. Differences in 3-dimensional shoulder kinematics between persons with multidirectional instability and asymptomatic controls. Am. J. Sports Med. 2007, 35, 1361–1370. [Google Scholar] [CrossRef]
- Johnson, N.; Pizzari, T.; Watson, L.; Wickham, J.; Balster, S. Functional improvements and electromyographic (EMG) changes in multidirectional instability of the shoulder after conservative rehabilitation. J. Sci. Med. Sport 2010, 13, e33–e34. [Google Scholar] [CrossRef]
- Kikuchi, K.; Itoi, E.; Yamamoto, N.; Seki, N.; Abe, H.; Minagawa, H.; Shimada, Y. Scapular inclination and glenohumeral joint stability: A cadaveric study. J. Orthop. Sci. 2008, 13, 72–77. [Google Scholar] [CrossRef]
- Bahu, M.J.; Trentacosta, N.; Vorys, G.C.; Covey, A.S.; Ahmad, C.S. Multidirectional instability: Evaluation and treatment options. Clin. Sports Med. 2008, 27, 671–689. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, J. Glenohumeral movements of the involuntary inferior and multidirectional instability. Clin. Orthop. Relat. Res. 1989, 238, 107–111. [Google Scholar] [CrossRef]
- Itoi, E.; Motzkin, N.E.; Morrey, B.F.; An, K.N. Scapular inclination and inferior stability of the shoulder. J. Shoulder Elbow Surg. 1992, 1, 131–139. [Google Scholar] [CrossRef]
- Illyés, Á.; Kiss, R.M. Kinematic and muscle activity characteristics of multidirectional shoulder joint instability during elevation. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 673–685. [Google Scholar] [CrossRef]
- Green, R.A.; Taylor, N.F.; Watson, L.; Ardern, C. Altered scapula position in elite young cricketers with shoulder problems. J. Sci. Med. Sport 2013, 16, 22–27. [Google Scholar] [CrossRef]
- Morris, A.D.; Kemp, G.J.; Frostick, S.P. Shoulder electromyography in multidirectional instability. J. Shoulder Elbow Surg. 2004, 13, 24–29. [Google Scholar] [CrossRef]
- Rio, E.; Kidgell, D.; Moseley, G.L.; Gaida, J.; Docking, S.; Purdam, C.; Cook, J. Tendon neuroplastic training: Changing the way we think about tendon rehabilitation: A narrative review. Br. J. Sports Med. 2016, 50, 209. [Google Scholar] [CrossRef]
- Madeleine, P.; Leclerc, F.; Arendt-Nielsen, L.; Ravier, P.; Farina, D. Experimental muscle pain changes the spatial distribution of upper trapezius muscle activity during sustained contraction. Clin. Neurophysiol. 2006, 117, 2436–2445. [Google Scholar] [CrossRef]
- Barden, J.; Balyk, R.; Raso, V.; Moreau, M.; Bagnall, K. Dynamic upper limb proprioception in multidirectional shoulder instability. Clin. Orthop. Relat. Res. 2004, 420, 181–189. [Google Scholar] [CrossRef]
- Jari, R.; Boyd, K.T.; Neumann, L.; Wallace, W.A. Shoulder Proprioception in Multidirectional Instability before and after Thermocapsular Shrinkage. Orthop. Proc. 2002, 84-B, 197. [Google Scholar] [CrossRef]
- Kirkley, A.; Adlington, J.; Edmonds, G.; Griffin, S. Proprioception in Multidirectional Instability. In Proceedings of the ORS/AAOS Combined Session Shoulder Instability-47th Annual Meeting, Orthopaedic Research Society, San Francisco, CA, USA, 25–28 February 2001. [Google Scholar]
- Barden, J.M.; Balyk, R.; Raso, V.J.; Moreau, M.; Bagnall, K. Atypical shoulder muscle activation in multidirectional instability. Clin. Neurophysiol. 2005, 116, 1846–1857. [Google Scholar] [CrossRef] [PubMed]
- Lephart, S.M.; Jari, R. The role of proprioception in shoulder instability. Oper. Tech. Sports Med. 2002, 10, 2–4. [Google Scholar] [CrossRef]
- Kiss, R.M.; Illyés, Á.; Kiss, J. Physiotherapy vs. capsular shift and physiotherapy in multidirectional shoulder joint instability. J. Electromyogr. Kinesiol. 2010, 20, 489–501. [Google Scholar] [CrossRef] [PubMed]
- McFarland, E.G.; Kim, T.K.; Park, H.B.; Neira, C.A.; Gutierrez, M.I. The Effect of Variation in Definition on the Diagnosis of Multidirectional Instability of the Shoulder. J. Bone Joint Surg. Am. 2003, 85, 2138–2144. [Google Scholar] [CrossRef]
- Lewis, A.; Kitamura, T.; Bayley, J. The classification of shoulder instability: New light through old windows! Curr. Orthop. 2004, 18, 97–108. [Google Scholar] [CrossRef]
- Sadi, J.; Torchia, E.; Faber, K.J.; MacDermid, J.; Lalonde, C.; Watson, L.; Weber, M.; Wu, N. Posterior Shoulder Instability Classification, Assessment, and Management: An International Delphi Study. J. Orthop. Sports Phys. Ther. 2020, 50, 373–380. [Google Scholar] [CrossRef]
- Rockwood, C. Subluxation of the shoulder: The classification diagnosis, and treatment. Orthop Trans. 1979, 4, 306. Available online: http://www.worldcat.org/title/orthopaedic-transactions/oclc/3486915 (accessed on 23 April 2022).
- Warby, S.A.; Pizzari, T.; Ford, J.J.; Hahne, A.J.; Watson, L. The effect of exercise-based management for multidirectional instability of the glenohumeral joint: A systematic review. J. Shoulder Elbow Surg. 2014, 23, 128–142. [Google Scholar] [CrossRef]
- Warby, S.A.; Pizzari, T.; Ford, J.J.; Hahne, A.J.; Watson, L. Exercise-based management versus surgery for multidirectional instability of the glenohumeral joint: A systematic review. Br. J. Sports Med. 2016, 50, 1115–1123. [Google Scholar] [CrossRef]
- Kłaptocz, P.; Solecki, W.; Grzegorzewski, A.; Błasiak, A.; Brzóska, R. Effectiveness of conservative treatment of multidirectional instability of the shoulder joint. Literature review and meta-analysis. Pol. Przegl. Chir. 2021, 94, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Best, M.J.; Tanaka, M.J. Multidirectional Instability of the Shoulder: Treatment Options and Considerations. Sports Med. Arthrosc. Rev. 2018, 26, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Uribe, J.; Zvijac, J.; Zikria, B.; Botto-van Bemden, A. Multidirectional Instability of the Shoulder. In The Athlete’s Shoulder, 2nd ed.; Wilk, K.E., Reinold, M.M., Andrews, J.R., Eds.; Churchill Livingstone: Philadelphia, PA, USA, 2009; pp. 229–238. [Google Scholar]
- Panayiotou Charalambous, C. Multidirectional Glenohumeral Instability. In The Shoulder Made Easy; Panayiotou Charalambous, C., Ed.; Springer International Publishing: Switzerland, UK, 2019; pp. 467–477. [Google Scholar]
- Galvin, J.W.; Ernat, J.J.; Waterman, B.R.; Stadecker, M.J.; Parada, S.A. The Epidemiology and Natural History of Anterior Shoulder Instability. Curr. Rev. Musculoskelet. Med. 2017, 10, 411–424. [Google Scholar] [CrossRef]
- Paxton, E.S.; Dodson, C.C.; Lazarus, M.D. Shoulder Instability in Older Patients. Orthop. Clin. North Am. 2014, 45, 377–385. [Google Scholar] [CrossRef]
- Hegedus, E.J.; Michener, L.A.; Seitz, A.L. Three Key Findings When Diagnosing Shoulder Multidirectional Instability: Patient Report of Instability, Hypermobility, and Specific Shoulder Tests. J. Orthop. Sports Phys. Ther. 2020, 50, 52–54. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, J.E. A new classification system for shoulder instability. Br. J. Sports Med. 2010, 44, 341–346. [Google Scholar] [CrossRef]
- McIntyre, K.; Bélanger, A.; Dhir, J.; Somerville, L.; Watson, L.; Willis, M.; Sadi, J. Evidence-based conservative rehabilitation for posterior glenohumeral instability: A systematic review. Phys. Ther. Sport 2016, 22, 94–100. [Google Scholar] [CrossRef]
- Beasley, L.; Faryniarz, D.A.; Hannafin, J.A. Multidirectional instability of the shoulder in the female athlete. Clin. Sports Med. 2000, 19, 331–349. [Google Scholar] [CrossRef]
- De Martino, I.; Rodeo, S.A. The Swimmer’s Shoulder: Multi-directional Instability. Curr. Rev. Musculoskelet. Med. 2018, 11, 167–171. [Google Scholar] [CrossRef]
- Van Blarcum, G.S.; Svoboda, S.J. Glenohumeral Instability Related to Special Conditions: SLAP Tears, Pan-labral Tears, and Multidirectional Instability. Sports Med. Arthrosc. Rev. 2017, 25, e12–e17. [Google Scholar] [CrossRef]
- Bao, M.H.; DeAngelis, J.P.; Wu, J.S. Imaging of traumatic shoulder injuries—Understanding the surgeon’s perspective. Eur. J. Radiol. Open. 2022, 9, 100411. [Google Scholar] [CrossRef] [PubMed]
- Vahlensieck, M. MRI of the shoulder. Eur. Radiol. 2000, 10, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Omoumi, P. Advanced Imaging of Glenohumeral Instability: It May Be Less Complicated than It Seems. J. Belg. Soc. Radiol. 2016, 100, 97. [Google Scholar] [CrossRef]
- Altchek, D.W.; Warren, R.F.; Skyhar, M.J.; Ortiz, G. T-plasty modification of the Bankart procedure for multidirectional instability of the anterior and inferior types. J. Bone Joint Surg. 1991, 73, 105–112. Available online: http://jbjs.org/content/73/1/105.abstract (accessed on 23 January 2022). [CrossRef] [PubMed]
- Staker, J.L.; Braman, J.P.; Ludewig, P.M. Kinematics and biomechanical validity of shoulder joint laxity tests as diagnostic criteria in multidirectional instability. Braz. J. Phys. Ther. 2021, 25, 883–890. [Google Scholar] [CrossRef]
- Bahk, M.; Keyurapan, E.; Tasaki, A.; Sauers, E.L.; McFarland, E.G. Laxity testing of the shoulder: A review. Am. J. Sports Med. 2007, 35, 131–144. [Google Scholar] [CrossRef]
- Levy, A.S.; Lintner, S.; Kenter, K.; Speer, K.P. Intra- and interobserver reproducibility of the shoulder laxity examination. Am. J. Sports Med. 1999, 27, 460–463. [Google Scholar] [CrossRef]
- Jia, X.; Petersen, S.; Khosravi, A.; Venkat, A.; Vinodhkumar, P.; Edward, M.G. Examination of the shoulder: The past, the present, and the future. J. Bone Joint Surg. Am. 2009, 91, 10–18. [Google Scholar] [CrossRef]
- Warby, S.A.; Ford, J.J.; Hahne, A.J.; Watson, L.; Balster, S.; Lenssen, R.; Pizzari, T. The effect of exercise based management on multidirectional instability of the glenohumeral joint: A pilot randomised controlled trial protocol. BMJ Open 2016, 6, e013083. [Google Scholar] [CrossRef]
- Kibler, W.B.; Sciascia, A. The role of the scapula in preventing and treating shoulder instability. Knee Surg. Sports Traumatol. Arthrosc. 2015, 24, 390–397. [Google Scholar] [CrossRef]
- Lewis, J.S.; McCreesh, K.; Barratt, E.; Hegedus, E.J.; Sim, J. Inter-rater reliability of the Shoulder Symptom Modification Procedure in people with shoulder pain. BMJ Open Sport Exerc. Med. 2016, 2, e000181. [Google Scholar] [CrossRef] [PubMed]
- Lo, I.K.Y.; Nonweiler, B.; Woolfrey, M.; Litchfield, R.; Kirkley, A. An Evaluation of the Apprehension, Relocation, and Surprise Tests for Anterior Shoulder Instability. Am. J. Sports Med. 2004, 32, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Farber, A.J.; Castillo, R.; Clough, M.; Bahk, M.; McFarland, E.G. Clinical Assessment of Three Common Tests for Traumatic Anterior Shoulder Instability. J. Bone Joint Surg. 2006, 88, 1467–1474. [Google Scholar] [CrossRef] [PubMed]
- Brzóska, R.; Milano, G.; Randelli, P.S.; Kovačič, L. 360° Around Shoulder Instability, 1st ed.; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Cools, A.M.J.; Struyf, F.; De Mey, K.; Maenhout, A.; Castelein, B.; Cagnie, B. Rehabilitation of scapular dyskinesis: From the office worker to the elite overhead athlete. Br. J. Sports Med. 2014, 48, 692–697. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Goldberg, J.; Herald, J.; Critchley, I.; Barmare, A. Effects of surgical management on multidirectional instability of the shoulder: A meta-analysis. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 630–639. [Google Scholar] [CrossRef]
- Witney-Lagen, C.F.; Hassan, A.M.; Doodson, A.B.; Venkateswaran, B.F. Arthroscopic plication for multidirectional instability: 50 patients with a minimum of 2 years of follow-up. J. Shoulder Elbow Surg. 2017, 26, e29–e36. [Google Scholar] [CrossRef]
- Ma, H.L.; Huang, H.K.; Chiang, E.R.; Wang, S.T.; Hung, S.C.; Liu, C.L. Arthroscopic Pancapsular Plication for Multidirectional Shoulder Instability in Overhead Athletes. Orthopedics 2012, 35, e497–e502. [Google Scholar] [CrossRef]
- Griffin, J.; Jaggi, A.; Daniell, H.; Chester, R. A systematic review to compare physiotherapy treatment programmes for atraumatic shoulder instability. Shoulder Elb. 2022, 17585732221080730. [Google Scholar] [CrossRef]
- Bateman, M.; Smith, B.E.; Osborne, S.E.; Wilkes, S.R. Physiotherapy treatment for atraumatic recurrent shoulder instability: Early results of a specific exercise protocol using pathology-specific outcome measures. Shoulder Elb. 2015, 7, 282–288. [Google Scholar] [CrossRef]
- Burkhead, W.Z.; Rockwood, C.A. Treatment of instability of the shoulder with an exercise program. J. Bone Joint Surg. 1992, 74A, 890–896. Available online: http://jbjs.org (accessed on 5 December 2021). [CrossRef]
- Remple, M.S.; Bruneau, R.M.; VandenBerg, P.M.; Goertzen, C.; Kleim, J. A Sensitivity of cortical movement representations to motor experience: Evidence that skill learning but not strength training induces cortical reorganization. Behav. Brain Res. 2001, 123, 133–141. [Google Scholar] [CrossRef]
- Leung, M.; Rantalainen, T.; Teo, W.P.; Kidgell, D. Motor cortex excitability is not differentially modulated following skill and strength training. Neuroscience 2015, 305, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.L.; Marstrand, P.C.D.; Nielsen, J.B. Motor skill training and strength training are associated with different plastic changes in the central nervous system. J. Appl. Physiol. 2005, 99, 1558–1568. [Google Scholar] [CrossRef] [PubMed]
- Warby, S.; Ganderton, C.; Watson, L.; Balster, S.; Kerr, B.; Lawrence, S.; Pizzari, T.; Takla, A.; Rotstein, A.; Hughes, M.; et al. The Effect of a Rehabilitation Program on Patients with Multidirectional Instability of the Glenohumeral Joint: A Functional MRI Study. Available online: https://anzctr.org.au/Trial/Registration/TrialReview.aspx?id=365110&isReview=true (accessed on 10 July 2022).
- Willmore, E.G.; Smith, M.J. Scapular dyskinesia: Evolution towards a systems-based approach. Shoulder Elb. 2016, 8, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Pizzari, T.; Wickham, J.; Balster, S.; Ganderton, C.; Watson, L. Modifying a shrug exercise can facilitate the upward rotator muscles of the scapula. Clin Biomech. 2014, 29, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.; Pizzari, T.; Balster, S. Thoracic outlet syndrome part 1: Clinical manifestations, differentiation and treatment pathways. Man. Ther. 2009, 14, 586–595. [Google Scholar] [CrossRef]
- Boudreau, S.A.; Farina, D.; Falla, D. The role of motor learning and neuroplasticity in designing rehabilitation approaches for musculoskeletal pain disorders. Man. Ther. 2010, 15, 410–414. [Google Scholar] [CrossRef]
- Illyés, Á.; Kiss, J.; Kiss, R.M. Electromyographic analysis during pull, forward punch, elevation and overhead throw after conservative treatment or capsular shift at patient with multidirectional shoulder joint instability. J. Electromyogr. Kinesiol. 2009, 19, 438–447. [Google Scholar] [CrossRef]
- Reinold, M.M.; Wilk, K.E.; Fleisig, G.S.; Zheng, N.; Barrentine, S.W.; Chmielewski, T.; Cody, R.C.; Jameson, G.G.; Andrews, J.R. Electromyographic Analysis of the Rotator Cuff and Deltoid Musculature During Common Shoulder External Rotation Exercises. J. Orthop. Sports Phys. Ther. 2004, 34, 385–394. [Google Scholar] [CrossRef]
- Spanhove, V.; De Wandele, I.; Kjær, B.H.; Malfait, F.; Vanderstukken, F.; Cools, A. The effect of five isometric exercises on glenohumeral translations in healthy subjects and patients with the hypermobility type of the ehlers-danlos syndrome (heds) or hypermobility spectrum disorder (hsd) with multidirectional shoulder instability: An observational study. Physiotherapy 2020, 107, 11–18. [Google Scholar] [CrossRef]
- Kronberg, M.; Nemeth, G.; Brostrom, L.-A. Muscle Activity and Coordination in the Normal Shoulder: An Electromyographic Study. Clin. Orthop. Relat. Res. 1990, 257, 76–85. [Google Scholar] [CrossRef]
- Kadaba, M.P.; Cole, A.; Wootten, M.E.; McCann, P.; Reid, M.; Mulford, G.; April, E.; Bigliani, L. Intramuscular wire electromyography of the subscapularis. J. Orthop. Res 1992, 10, 394–397. [Google Scholar] [CrossRef] [PubMed]
- Ovesen, J.; Nielsen, S. Stability of the shoulder joint: Cadaver study of stabilizing structures. Acta Orthop. Scand. 1985, 56, 149–151. [Google Scholar] [CrossRef] [PubMed]
- Pizzari, T.; Ganderton, C.; Watson, L.; Balster, S. A novel exercise for retraining the rotator cuff muscles of the shoulder. J. Sci. Med. Sport 2013, 16 (Suppl. 1), e7. [Google Scholar] [CrossRef]
- Jaggi, A.; Lambert, S. Rehabilitation for shoulder instability. Br. J. Sports Med. 2010, 44, 333–340. [Google Scholar] [CrossRef]
- Decker, M.J.; Hintermeister, R.A.; Faber, K.J.; Hawkins, R.J. Serratus anterior muscle activity during selected rehabilitation exercises. Am. J. Sports Med. 1999, 27, 784–791. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=med4&AN=10569366 (accessed on 4 February 2022). [CrossRef]
- Kido, T.; Itoi, E.; Lee, S.B.; Neale, P.G.; An, K.N. Dynamic stabilizing function of the deltoid muscle in shoulders with anterior instability. Am. J. Sports Med. 2003, 31, 399–403. Available online: https://journals-sagepub-com.ez.library.latrobe.edu.au/doi/pdf/10.1177/03635465030310031201 (accessed on 23 November 2021). [CrossRef]
- Cools, A.M.; Borms, D.; Castelein, B.; Vanderstukken, F.; Johansson, F.R. Evidence-based rehabilitation of athletes with glenohumeral instability. Knee Surg. Sports Traumatol. Arthrosc. 2015, 24, 382–389. [Google Scholar] [CrossRef]
- Sciascia, A.; Thigpen, C.; Namdari, S.; Baldwin, K. Kinetic Chain Abnormalities in the Athletic Shoulder. Sports Med. Arthrosc. 2012, 20, 16–21. [Google Scholar] [CrossRef]
- Burkhart, S.S.; Morgan, C.D.; Ben Kibler, W. The disabled throwing shoulder: Spectrum of pathology part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy 2003, 19, 641–661. [Google Scholar] [CrossRef]
- Drummond Junior, M.; Popchak, A.; Wilson, K.; Kane, G.; Lin, A. Criteria-based return-to-sport testing is associated with lower recurrence rates following arthroscopic Bankart repair. J. Shoulder Elbow Surg. 2021, 30, S14–S20. [Google Scholar] [CrossRef] [PubMed]
- Ganderton, C.; Kerr, B.; King, M.; Lenssen, R.; Warby, S.; Munro, D.; Watson, L.; Balster, S.; Han, J.; Tirosh, O. Intra-Rater and Inter-Rater Reliability of Hand-Held Dynamometry for Shoulder Strength Assessment in Circus Arts Students. Med. Probl. Perform. Art. 2021, 36, 88–102. [Google Scholar] [CrossRef]
- Plancher, K.D.; Lipnick, S.L. Analysis of Evidence-Based Medicine for Shoulder Instability. Arthrosc. J. Arthrosc. Relat. Surg. 2009, 25, 897–908. [Google Scholar] [CrossRef]
- Ratamess, N.A.; Alvar, B.A.; Kibler, W.B.; Kraemer, W.J.; Triplett, N.T. Progression models in resistance training for healthy adults. Am. Coll. Sports Med. 2002, 34, 364–380. [Google Scholar]
- Gaskill, T.R.; Taylor, D.C.; Millett, P.J. Management of multidirectional instability of the shoulder. J. Am. Acad. Orthop. Surg. 2011, 19, 758–767. Available online: http://journals.lww.com/jaaos/pages/default.aspx (accessed on 10 April 2022). [CrossRef]
- Howard, A.; Powell, J.L.; Gibson, J.; Hawkes, D.; Kemp, G.J.; Frostick, S.P. A functional Magnetic Resonance Imaging study of patients with Polar Type II/III complex shoulder instability. Sci. Rep. 2019, 9, 6271. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.; Pizzari, T.; Balster, S. Thoracic outlet syndrome part 2: Conservative management of thoracic outlet. Man. Ther. 2010, 15, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Lebus, G.F.; Raynor, M.B.; Nwosu, S.K.; Wagstrom, E.; Jani, S.S.; Carey, J.L.; Hettrich, C.M.; Cox, C.L.; Kuhn, J.E.; MOON Shoulder Group. Predictors for Surgery in Shoulder Instability: A Retrospective Cohort Study Using the FEDS System. Orthop. J. Sports Med. 2015, 3, 2325967115607434. [Google Scholar] [CrossRef]
- Breckenridge, J.D.; McAuley, J.H.; Moseley, G.L.; Ginn, K.A. Is implicit motor imagery altered in people with shoulder pain? The shoulder left/right judgement task. Musculoskelet. Sci. Pract. 2020, 48, 102159. [Google Scholar] [CrossRef]
- Hemington, K.S.; Wu, Q.; Kucyi, A.; Inman, R.D.; Davis, K.D. Abnormal cross-network functional connectivity in chronic pain and its association with clinical symptoms. Brain Struct. Funct. 2016, 221, 4203–4219. [Google Scholar] [CrossRef]
- Moseley, G.L.; Flor, H. Targeting Cortical Representations in the Treatment of Chronic Pain: A Review. Neurorehabil. Neural Repair 2012, 26, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Moseley, L.G. Graded motor imagery for pathologic pain: A randomized controlled trial. Neurology 2006, 67, 2129–2134. [Google Scholar] [CrossRef] [PubMed]
- Yap, B.W.D.; Lim, E.C.W. The Effects of Motor Imagery on Pain and Range of Motion in Musculoskeletal Disorders: A Systematic Review Using Meta-Analysis. Clin. J. Pain 2019, 35, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Neuro Orthopaedic Institute (NOI) Australasia. Graded Motor Imagery. Available online: http://www.gradedmotorimagery.com (accessed on 9 July 2022).
- Araya-Quintanilla, F.; Gutiérrez-Espinoza, H.; Jesús Muñoz-Yanez, M.; Rubio-Oyarzún, D.; Cavero-Redondo, I.; Martínez-Vizcaino, V.; Álvarez-Bueno, C. The Short-term Effect of Graded Motor Imagery on the Affective Components of Pain in Subjects with Chronic Shoulder Pain Syndrome: Open-Label Single-Arm Prospective Study. Pain Med. 2020, 21, 2496–2501. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Associated Factor | Clinical Presentation | Key Modifications/Explanation and Examples |
|---|---|---|
| MDI with connective tissue disorders | Examples: Hypermobility syndrome Marfan’s syndrome Ehlers–Danlos syndrome May have concurrent musculoskeletal disorders (e.g., craniocervical instability, cervical spine weakness, patella-femoral joint pain) May have concurrent systematic disorders (e.g., heart murmur, poor gastro-intestinal mobility, valvular heart disease) | Key modifications: Rehabilitation loads, exercise drills and rates of progression need to be modified due to fragility of tissues. Explanation and Examples: Exercise loads may need to be applied and progressed with TheraBandTM instead of weights for a long period. If weights prescribed, may need to limit to a maximum amount (e.g., 2–3 kg for bent over row, 2–3 kg supine flexion drills, 1–2 kg overhead press). Drills rarely performed to the very end ranges of motion. Entry into the rehabilitation program is typically lower (e.g., supine or side lie scapular drills instead of standing). Progression through the program is slower. Focus on 1 to 3 motor control drills with light load for several weeks before progression. May need to be counselled on realistic expectations of their shoulders and bodies regarding activities (e.g., contact and throwing sports unlikely and/or high risk). |
| MDI with severe motor patterning and unamenable to correction | Patient does not respond to scapular correction (at least initially) Typically, a long history of symptoms May have psychosocial involvement Manual correction typically met with severe and involuntary muscle guarding which may appear as glenohumeral capsular stiffness. Note: True glenohumeral joint stiffness is unlikely in the absence of trauma and in the typical MDI age range [24,113]. Possible central involvement [111]. Patients may have poor laterality (left and right recognition) [114]. When asked to perform imagery of simple shoulder motion (e.g., flexion, abduction, ER) patients may report ‘gaps’ in imaged motion (e.g., missing pieces of flexion range), or an increase in pain during attempted imagery [115,116]. | Key modifications: Can still respond well to the rehabilitation program; however, commence the program at a lower level and progress at a much slower rate. Brain training with graded motor imagery (GMI) may be required in a small sub- group of patients. Explanation and Examples: Scapular drills may need to be performed in side-lying, supine or isometrically prior to performing the drill isotonically. Fewer repetitions of the exercise may be required initially. Once patients can progress scapular drills to standing, then they can usually progress along the standard WIP1 guidelines. Once these patients have regained a sense of normal scapular motor patterning, it is not uncommon for them to become correctable. A small sub-group of patients may be unable to perform the simplest of scapular drills (e.g., supine) and may require brain training with GMI prior to performing active motor drills. GMI has good evidence for efficacy in musculoskeletal disorders [117,118]. Normalise left and right recognition if abnormal [114,117,119]. Imagery training such as mental rehearsal of a correct scapular motor pattern (often facilitated by watching a video of “normal” scapula motion), simple shoulder range of motion, or shoulder-based activities of daily living (e.g., washing hair, reaching up into a cupboard, getting dressed) within pain limits [117,119]. Mirror therapy is rarely required in this context though may be implemented if deemed necessary [117,119,120]. |
| MDI with a history of microtrauma or trauma | History of significant trauma (e.g., fall and contact with an external object and conscious awareness of the onset of pain and/or subluxation/dislocation). Or Microtrauma (gradual or acute overload of muscular, e.g., increase in volume of tennis with a heavier than usual racquet). More likely to have 2 (anterior and/or posterior) rather than 3 directions of instability Increased likelihood of structural lesions | Key modifications: Microtraumatic MDI: If 6 months of evidence-based rehabilitation fails, surgery may be considered. MDI with trauma: rehabilitation to normalise poor motor patters. Early surgical referral warranted in cases of significant traumatic structural lesions. Explanation and Examples Clinician should determine if the patient is amenable to scapular +/− humeral head correction. Correctable = rehabilitation should be commenced to correct any movement errors. If the patient continues to improve over 12 to 24 weeks, then rehabilitation is continued. Non-correctable +/− aberrant motor patterns= commence rehabilitation to determine if the patient’s assessment asterisk/s improve over several weeks and to normalise faulty motor control. If improved over 12 to 24 weeks, then rehabilitation is continued. If not showing any improvement over 2 to 3 weeks of rehabilitation\high quality imaging should be sought. If significant structural lesion present and not responding to conservative rehabilitation, then surgery to restore the soft tissue structures may be indicated [13,51]. Post-surgery, the focus of rehabilitation is still on establishing good scapular and humeral head control, initially at rest and then through movement [5,6,8,9]. Passive stretching of the glenohumeral joint is usually avoided, as most MDI patients will regain their range with gentle active motion. Post-surgical rehabilitation typically has a longer time frame (9 to 12 months) compared to other post-surgical rehabilitation programs for other types of shoulder instability. |
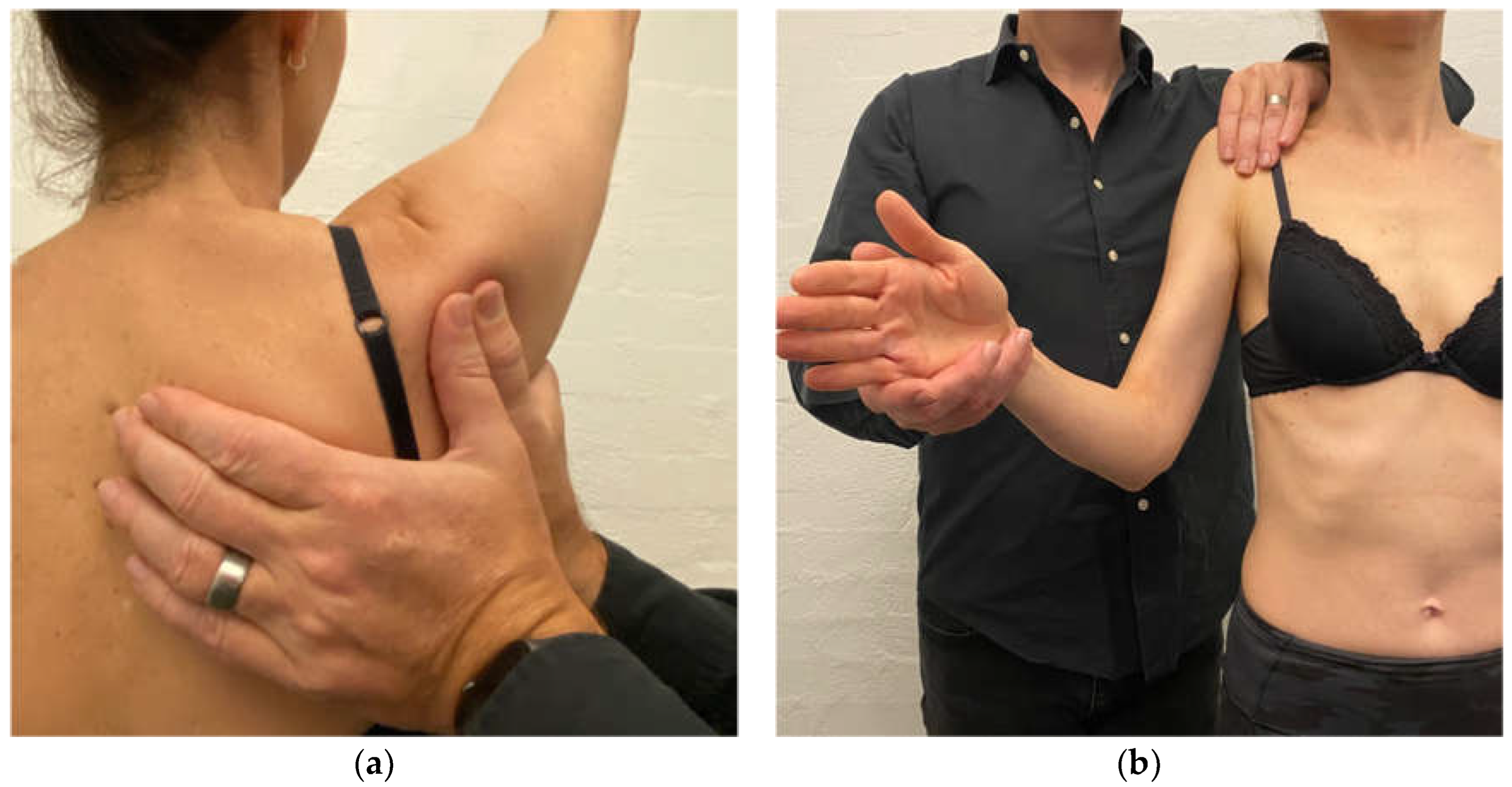
| MDI with neck dysfunction | MDI patient with concurrent cervical spine pain and/or weakness and/or postural thoracic outlet syndrome (TOS). Typically due to traction of cervical structures and the brachial plexus from a depressed and downwardly rotated scapula [32,91,112] and/or primary cervical spine weakness. Deep cervical flexors (DCF) are weak on pressure biofeedback assessment and/or lack smooth motor control of the neck flexion. Scapular corrective techniques and reassessment of cervical range of motion can assist in determining if the scapula position is a significant driver of neck and/or TOS symptoms. | Key modifications: Normalise cervical spine strength prior to commencing standing scapula drills. Explanation and Examples: Treatment involves offloading the cervical structures with scapular taping and bracing and addressing ergonomics (e.g., arm rest at the desk to prevent excessive cervical traction). DCF activity and strength needs to be normalised as a precursor to prescribing standing scapula drills as performing upward rotation, elevation drills on a weak and painful neck are likely to exacerbate neck symptoms. Drills are then progressed from supine (Figure 12a) to standing against a wall (Figure 12b). Once the patient can perform DCF drills in standing then they are usually ready to add in a standing scapular drill to their DCF drill. Cervical extension drills are also added. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watson, L.; Pizzari, T.; Balster, S.; Lenssen, R.; Warby, S.A. Advances in the Non-Operative Management of Multidirectional Instability of the Glenohumeral Joint. J. Clin. Med. 2022, 11, 5140. https://doi.org/10.3390/jcm11175140
Watson L, Pizzari T, Balster S, Lenssen R, Warby SA. Advances in the Non-Operative Management of Multidirectional Instability of the Glenohumeral Joint. Journal of Clinical Medicine. 2022; 11(17):5140. https://doi.org/10.3390/jcm11175140
Chicago/Turabian StyleWatson, Lyn, Tania Pizzari, Simon Balster, Ross Lenssen, and Sarah Ann Warby. 2022. "Advances in the Non-Operative Management of Multidirectional Instability of the Glenohumeral Joint" Journal of Clinical Medicine 11, no. 17: 5140. https://doi.org/10.3390/jcm11175140
APA StyleWatson, L., Pizzari, T., Balster, S., Lenssen, R., & Warby, S. A. (2022). Advances in the Non-Operative Management of Multidirectional Instability of the Glenohumeral Joint. Journal of Clinical Medicine, 11(17), 5140. https://doi.org/10.3390/jcm11175140