
Single Lead Epidural Spinal Cord Stimulation Targeted Trunk Control and Standing in Complete Paraplegia


Abstract
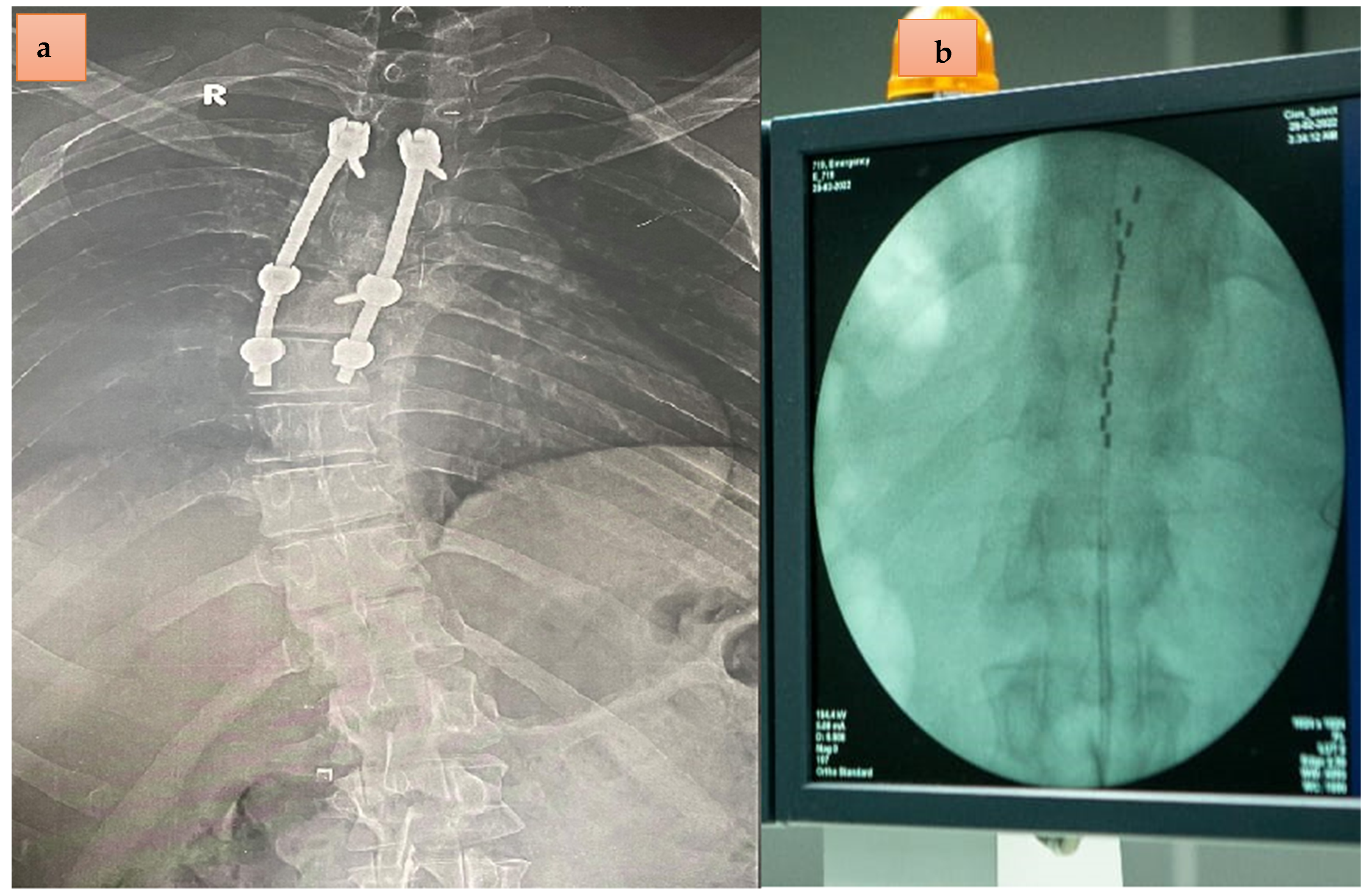
:1. Case Report
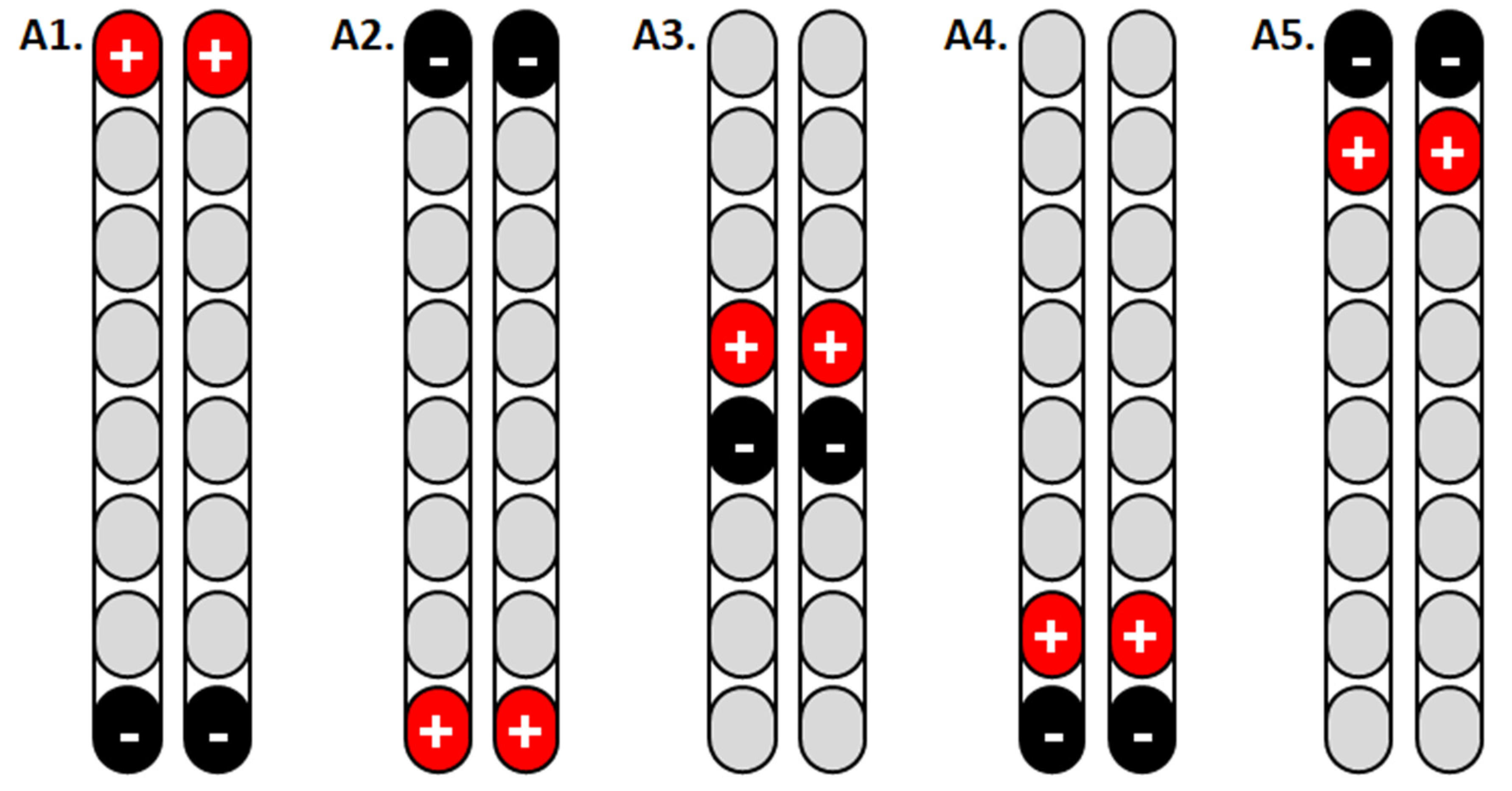
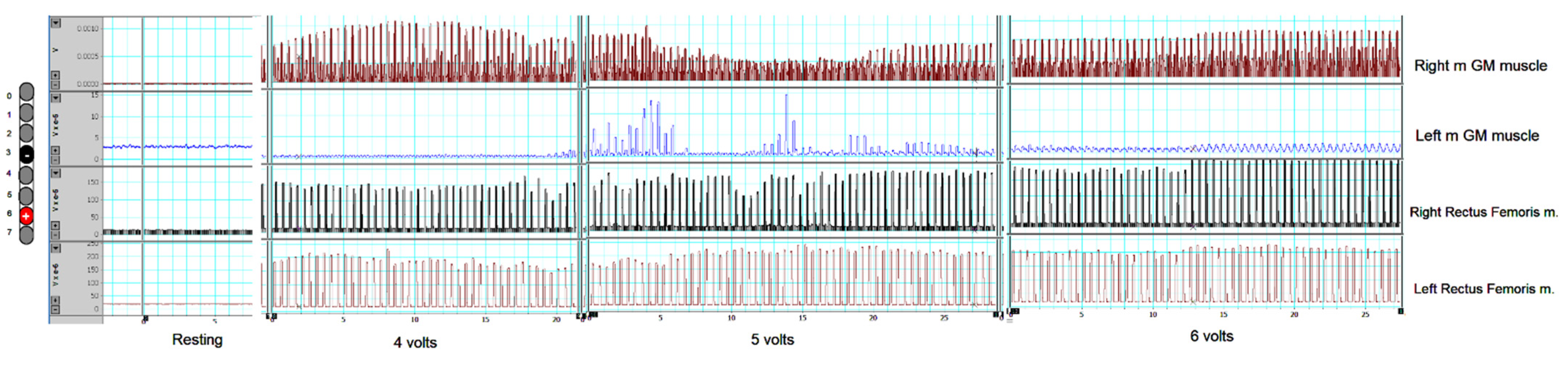
2. Targeted Stimulation to Achieve Standing
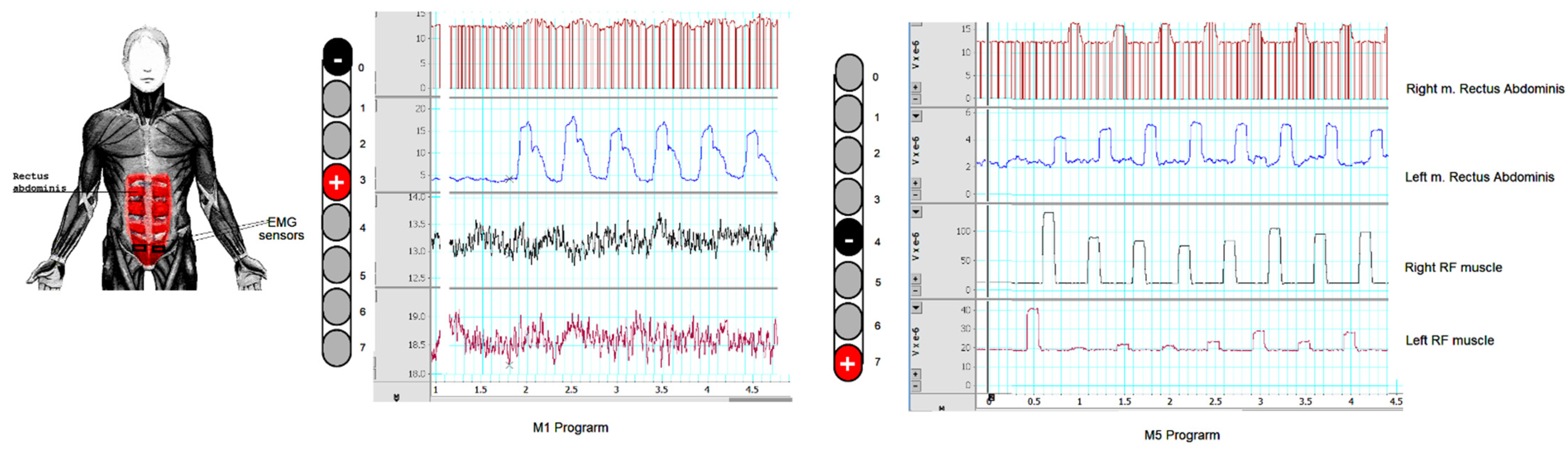
3. Targeted Stimulation to Achieve Trunk Control
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cameron, T. Safety and efficacy of spinal cord stimulation for the treatment of chronic pain: A 20-year literature review. J. Neurosurg. Spine 2004, 100, 254–267. [Google Scholar] [CrossRef] [PubMed]
- Frey, M.E.; Manchikanti, L.; Benyamin, R.M.; Schultz, D.M.; Smith, H.S.; Cohen, S.P. Spinal cord stimulation for patients with failed back surgery syndrome: A systematic review. Pain Physician 2009, 12, 379. [Google Scholar] [CrossRef] [PubMed]
- Harkema, S.; Gerasimenko, Y.; Hodes, J.; Burdick, J.; Angeli, C.; Chen, Y.; Ferreira, C.; Willhite, A.; Rejc, E.; Grossman, R.G. Effect of epidural stimulation of the lumbosacral spinal cord on voluntary movement, standing, and assisted stepping after motor complete paraplegia: A case study. Lancet 2011, 377, 1938–1947. [Google Scholar] [CrossRef]
- Angeli, C.A.; Boakye, M.; Morton, R.A.; Vogt, J.; Benton, K.; Chen, Y.; Ferreira, C.K.; Harkema, S.J. Recovery of over-ground walking after chronic motor complete spinal cord injury. N. Engl. J. Med. 2018, 379, 1244–1250. [Google Scholar] [CrossRef]
- Wagner, F.B.; Mignardot, J.-B.; Le Goff-Mignardot, C.G.; Demesmaeker, R.; Komi, S.; Capogrosso, M.; Rowald, A.; Seáñez, I.; Caban, M.; Pirondini, E. Targeted neurotechnology restores walking in humans with spinal cord injury. Nature 2018, 563, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Gorgey, A.S.; Gill, S.; Holman, M.E.; Davis, J.C.; Atri, R.; Bai, O.; Goetz, L.; Lester, D.L.; Trainer, R.; Lavis, T.D. The feasibility of using exoskeletal-assisted walking with epidural stimulation: A case report study. Ann. Clin. Transl. Neurol. 2020, 7, 259–265. [Google Scholar] [CrossRef]
- Gorgey, A.S.; Sutor, T.W.; Goldsmith, J.A.; Ennasr, A.N.; Lavis, T.D.; Cifu, D.X.; Trainer, R. Epidural stimulation with locomotor training ameliorates unstable blood pressure after tetraplegia. A case report. Ann. Clin. Transl. Neurol. 2022, 9, 232–238. [Google Scholar] [CrossRef]
- Basques, B.A.; Varthi, A.G.; Golinvaux, N.S.; Bohl, D.D.; Grauer, J.N. Patient characteristics associated with increased postoperative length of stay and readmission after elective laminectomy for lumbar spinal stenosis. Spine 2014, 39, 833. [Google Scholar] [CrossRef]
- Osman, N.S.; Cheung, Z.B.; Hussain, A.K.; Phan, K.; Arvind, V.; Vig, K.S.; Vargas, L.; Kim, J.S.; Cho, S.K.-W. Outcomes and complications following laminectomy alone for thoracic myelopathy due to ossified ligamentum flavum. Spine 2018, 43, E842. [Google Scholar] [CrossRef]
- Hofstoetter, U.S.; Perret, I.; Bayart, A.; Lackner, P.; Binder, H.; Freundl, B.; Minassian, K. Spinal motor mapping by epidural stimulation of lumbosacral posterior roots in humans. Iscience 2021, 24, 101930. [Google Scholar] [CrossRef]
- Barolat, G.; Myklebust, J.B.; Wenninger, W. Effects of spinal cord stimulation on spasticity and spasms secondary to myelopathy. Stereotact. Funct. Neurosurg. 1988, 51, 29–44. [Google Scholar] [CrossRef] [PubMed]
- Minassian, K.; Jilge, B.; Rattay, F.; Pinter, M.; Binder, H.; Gerstenbrand, F.; Dimitrijevic, M.R. Stepping-like movements in humans with complete spinal cord injury induced by epidural stimulation of the lumbar cord: Electromyographic study of compound muscle action potentials. Spinal Cord 2004, 42, 401–416. [Google Scholar] [CrossRef] [PubMed]
- Benavides, F.D.; Jo, H.J.; Lundell, H.; Edgerton, V.R.; Gerasimenko, Y.; Perez, M.A. Cortical and subcortical effects of transcutaneous spinal cord stimulation in humans with tetraplegia. J. Neurosci. 2020, 40, 2633–2643. [Google Scholar] [CrossRef] [PubMed]
- Hachmann, J.T.; Yousak, A.; Wallner, J.J.; Gad, P.N.; Edgerton, V.R.; Gorgey, A.S. Epidural spinal cord stimulation as an intervention for motor recovery after motor complete spinal cord injury. J. Neurophysiol. 2021, 126, 1843–1859. [Google Scholar] [CrossRef]
- Gupta, M.; Abd-Elsayed, A.; Hughes, M.; Rotte, A. A retrospective review of lead migration rate in patients permanently implanted with percutaneous leads and a 10 kHz SCS device. Pain Res. Manag. 2021, 2021, 6639801. [Google Scholar] [CrossRef]
- Sayenko, D.G.; Angeli, C.; Harkema, S.J.; Edgerton, V.R.; Gerasimenko, Y.P. Neuromodulation of evoked muscle potentials induced by epidural spinal-cord stimulation in paralyzed individuals. J. Neurophysiol. 2014, 111, 1088–1099. [Google Scholar] [CrossRef]
- Gill, M.; Linde, M.; Fautsch, K.; Hale, R.; Lopez, C.; Veith, D.; Calvert, J.; Beck, L.; Garlanger, K.; Edgerton, R.; et al. Epidural Electrical Stimulation of the Lumbosacral Spinal Cord Improves Trunk Stability During Seated Reaching in Two Humans With Severe Thoracic Spinal Cord Injury. Front. Syst. Neurosci. 2020, 14, 79. [Google Scholar] [CrossRef]
- Minassian, K.; Hofstoetter, U.S. Spinal cord stimulation and augmentative control strategies for leg movement after spinal paralysis in humans. CNS Neurosci. Ther. 2016, 22, 262–270. [Google Scholar] [CrossRef]
- Rejc, E.; Angeli, C.; Harkema, S. Effects of lumbosacral spinal cord epidural stimulation for standing after chronic complete paralysis in humans. PLoS ONE 2015, 10, e0133998. [Google Scholar]
- Calvert, J.S.; Gill, M.L.; Linde, M.B.; Veith, D.D.; Thoreson, A.R.; Lopez, C.; Lee, K.H.; Gerasimenko, Y.P.; Edgerton, V.R.; Lavrov, I.A. Voluntary modulation of evoked responses generated by epidural and transcutaneous spinal stimulation in humans with spinal cord injury. J. Clin. Med. 2021, 10, 4898. [Google Scholar] [CrossRef]
- Mendez, A.; Islam, R.; Latypov, T.; Basa, P.; Joseph, O.J.; Knudsen, B.; Siddiqui, A.M.; Summer, P.; Staehnke, L.J.; Grahn, P.J. Segment-specific orientation of the dorsal and ventral roots for precise therapeutic targeting of human spinal cord. Mayo Clin. Proc. 2021, 96, 1426–1437. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.P.; Brownstone, R.M. Mechanisms of spinal cord stimulation for the treatment of pain: Still in the dark after 50 years. Eur. J. Pain 2019, 23, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Dombovy-Johnson, M.L.; D’Souza, R.S.; Ha, C.T.; Hagedorn, J.M. Incidence and risk factors for spinal cord stimulator lead migration with or without loss of efficacy: A retrospective review of 91 consecutive thoracic lead implants. Neuromodulation Technol. Neural Interface 2022, 25, 731–737. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Day 1 (2 Hz and 150 µs) | Day 2 (20–30 Hz and 210 µs) | |||||||
|---|---|---|---|---|---|---|---|---|
| Amplitude (Volts) | 2.5 | 5 | 7.5 | 10 | 2.5 | 5 | 7.5 | 10 |
| A1 | No response | Extension with internal rotation (visible contraction) | No response | Left leg flexion was imitated at 3.5 v | ||||
| A2 | No response | Extension with internal rotation (visible contraction) | Strong bilateral extension | No response | Visible left hip flexion | Participant was capable of enabling left hip flexion at 6.5–7.0 volts | ||
| A3 | No response | Emphasis on the right extension | Strong emphasis on the right extension | No response | Bilateral leg extension (potential standing program) | Bilateral leg extension with right side emphasis | Bilateral oscillations of both lower extremities | |
| A4 | Right gastrocnemius muscle (visible ankle movement in plantarflexion) | Bilateral emphasis on gastrocnemius and knee extensors | Strong emphasis on gastrocnemius and knee extensors | No response | Visible left hip flexion at 4 volts Bilateral hip flexions at 4.5 volts/ | |||
| A5 | No response | No response | No response | Left side knee extensors and gluteus maximums muscle | Program was excluded based on the results of day 1 | |||
| Amplitude (Volts) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Program | Cathode | Anode | Muscles | 1 | 2 | 3 | 4 | 5 | 6 | 7 | Abdominal Muscle Stimulation (Y/N) |
| M1 | 0 | 3 | Left RF on | x | x x | x x | Y | ||||
| Right RF on | |||||||||||
| Left GM on | |||||||||||
| Right GM on | |||||||||||
| M2 | 1 | 4 | Left RF on | x | x x | N | |||||
| Right RF on | |||||||||||
| Left GM on | |||||||||||
| Right GM on | |||||||||||
| M3 | 2 | 5 | Left RF on | x x | x x | N | |||||
| Right RF on | |||||||||||
| Left GM on | |||||||||||
| Right GM on | |||||||||||
| M4 | 3 | 6 | Left RF on | x x | x x | N | |||||
| Right RF on | |||||||||||
| Left GM on | |||||||||||
| Right GM on | |||||||||||
| M5 | 4 | 7 | Left RF on | x x | x x x x | x x x x | x x x x | Y | |||
| Right RF on | |||||||||||
| Left GM on | |||||||||||
| Right GM on | |||||||||||
| M6 | 3 | 0 | Left RF on | x | x x | x x | N | ||||
| Right RF on | |||||||||||
| Left GM on | |||||||||||
| Right GM on | |||||||||||
| M7 | 4 | 3 | Left RF on | x | x x | N | |||||
| Right RF on | |||||||||||
| Left GM on | |||||||||||
| Right GM on | |||||||||||
| M8 | 5 | 2 | Left RF on | x | x x | N | |||||
| Right RF on | |||||||||||
| Left GM on | |||||||||||
| Right GM on | |||||||||||
| M9 | 6 | 3 | Left RF on | x x | x x | N | |||||
| Right RF on | |||||||||||
| Left GM on | |||||||||||
| Right GM on | |||||||||||
| M10 | 7 | 4 | Left RF on | x x | x x x x | x x x x | N | ||||
| Right RF on | |||||||||||
| Left GM on | |||||||||||
| Right GM on | |||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gorgey, A.S.; Gouda, J.J. Single Lead Epidural Spinal Cord Stimulation Targeted Trunk Control and Standing in Complete Paraplegia. J. Clin. Med. 2022, 11, 5120. https://doi.org/10.3390/jcm11175120
Gorgey AS, Gouda JJ. Single Lead Epidural Spinal Cord Stimulation Targeted Trunk Control and Standing in Complete Paraplegia. Journal of Clinical Medicine. 2022; 11(17):5120. https://doi.org/10.3390/jcm11175120
Chicago/Turabian StyleGorgey, Ashraf S., and Jan J. Gouda. 2022. "Single Lead Epidural Spinal Cord Stimulation Targeted Trunk Control and Standing in Complete Paraplegia" Journal of Clinical Medicine 11, no. 17: 5120. https://doi.org/10.3390/jcm11175120
APA StyleGorgey, A. S., & Gouda, J. J. (2022). Single Lead Epidural Spinal Cord Stimulation Targeted Trunk Control and Standing in Complete Paraplegia. Journal of Clinical Medicine, 11(17), 5120. https://doi.org/10.3390/jcm11175120