
Practical Considerations for the Use of Cannabis in Cancer Pain Management—What a Medical Oncologist Should Know

 , , ,
, , ,
Abstract
:1. Introduction
2. Overview on Cancer Pain Management, and Related Issues
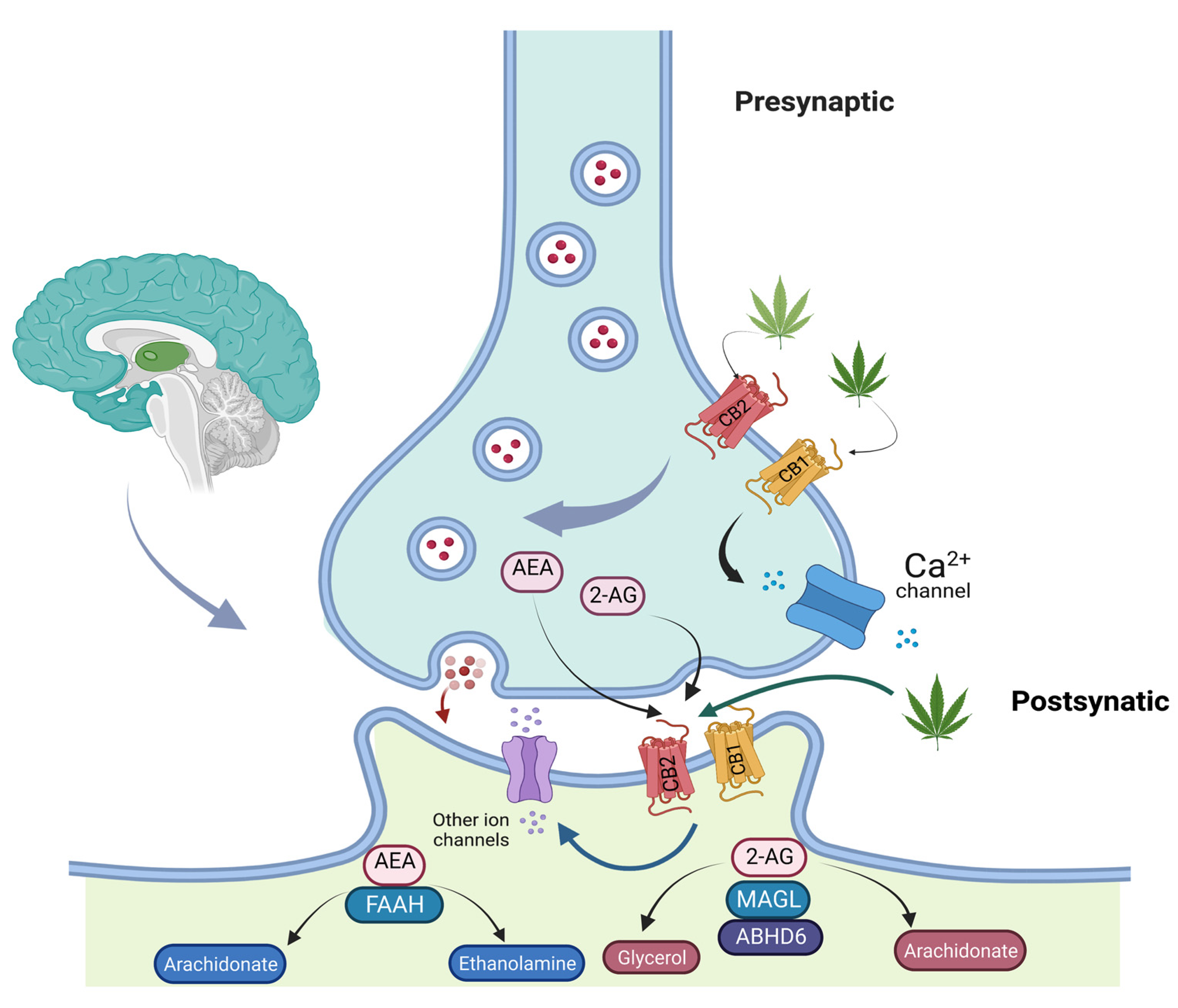
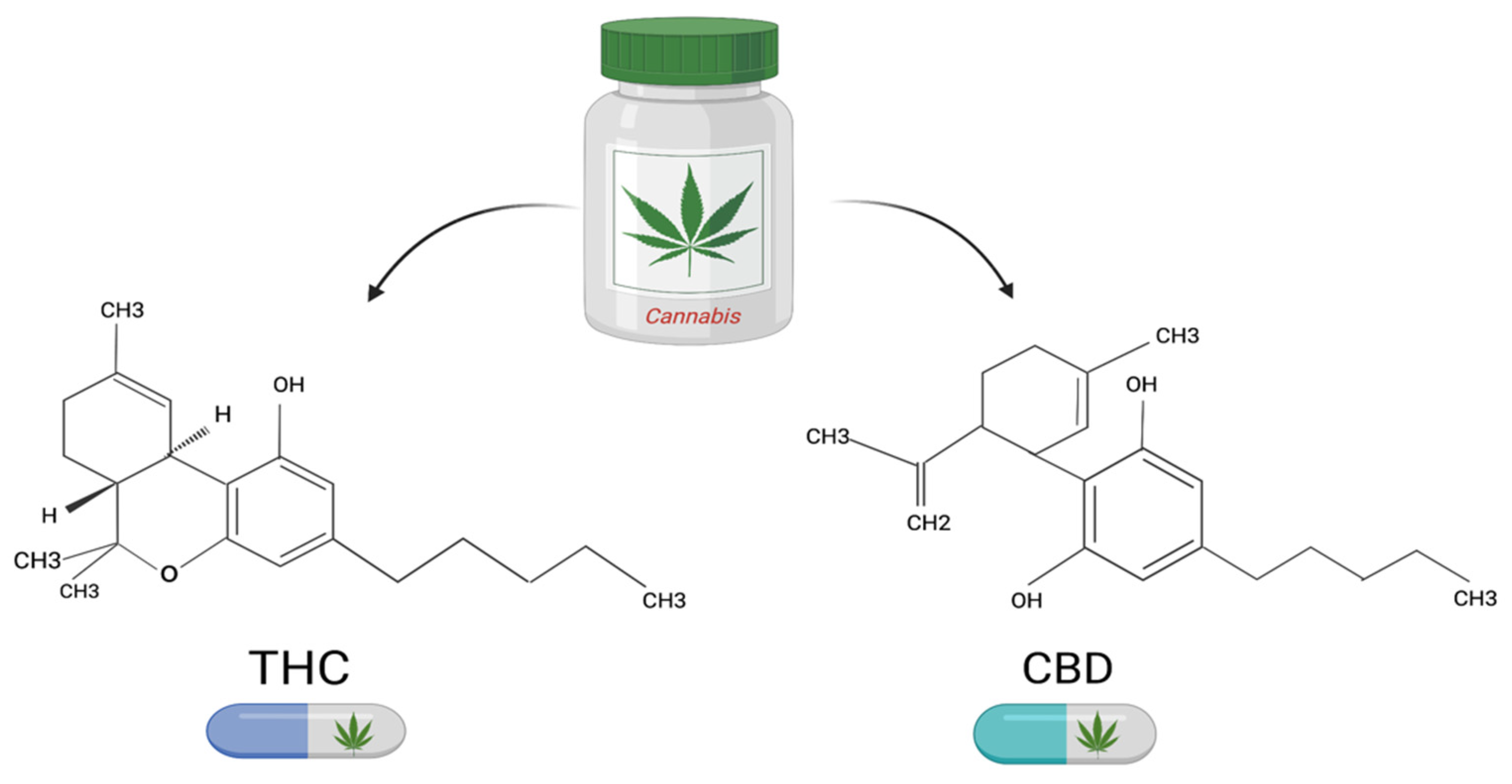
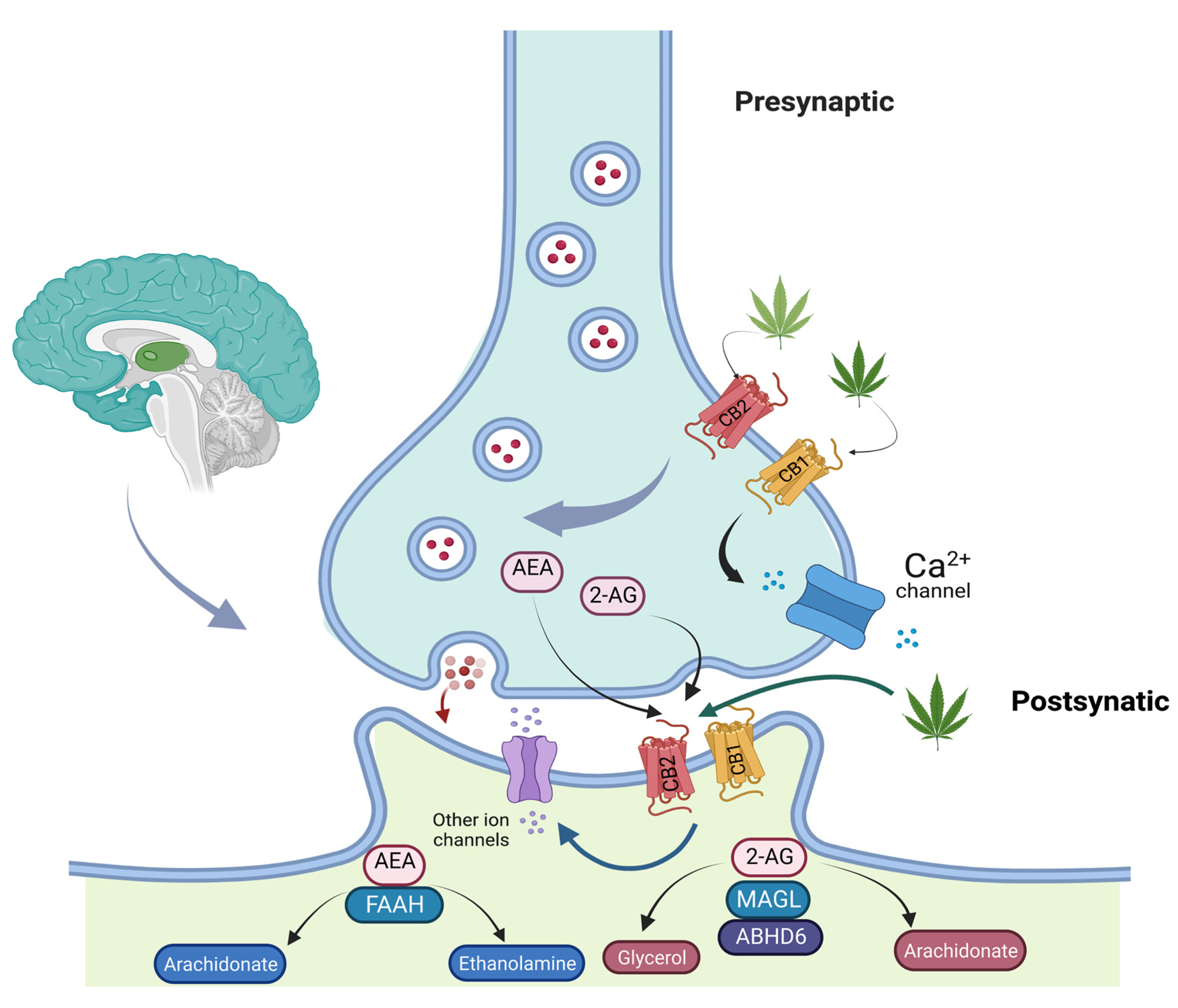
3. Cannabis and Its Mechanisms of Action
4. Cannabis-Based Medicines
4.1. Preclinical Evidence
4.2. Clinical Evidence
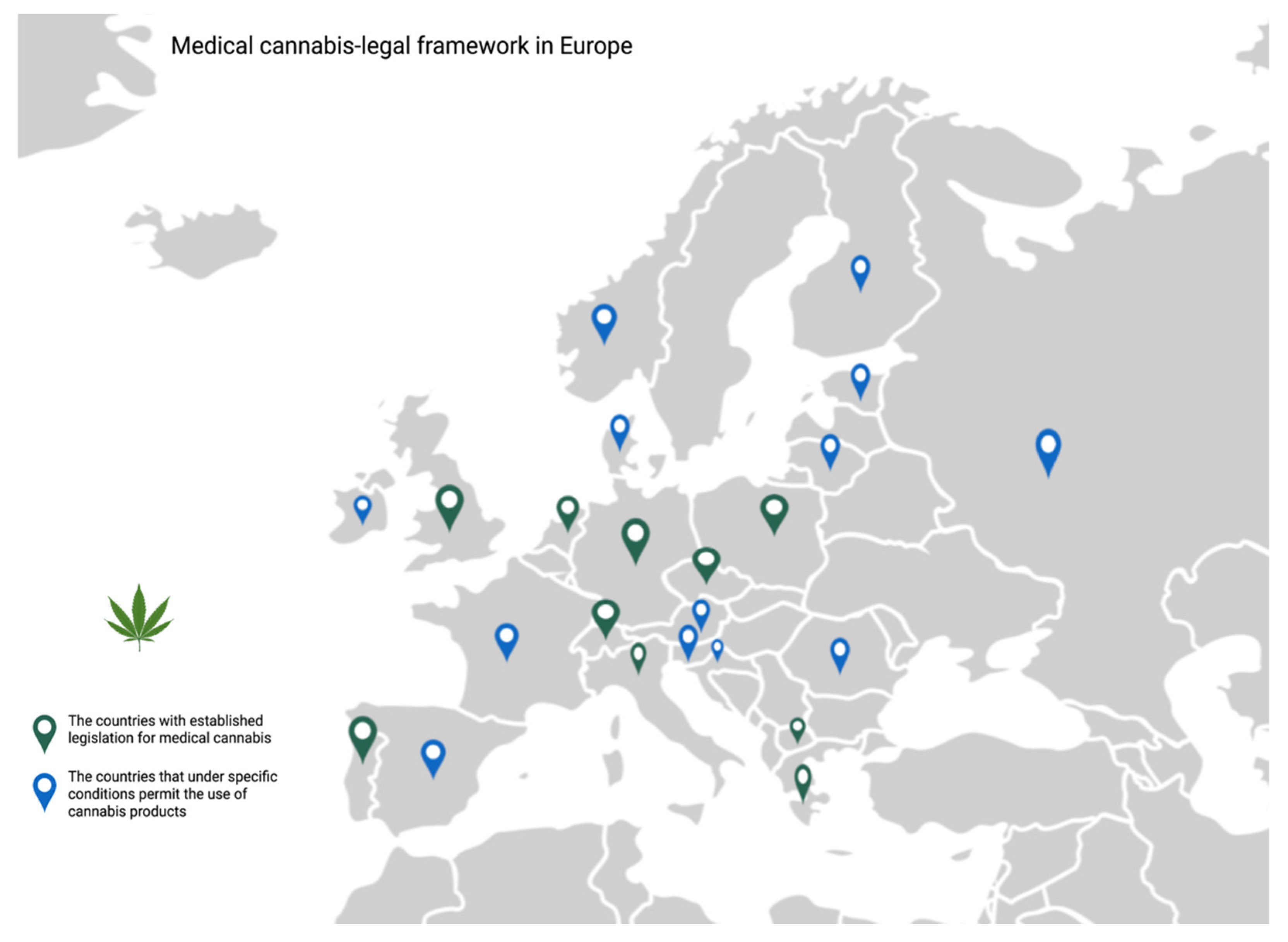
5. Existing Concerns and Legal Considerations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haroutounian, S.; Ratz, Y.; Ginosar, Y.; Furmanov, K.; Saifi, F.; Meidan, R.; Davidson, E. The Effect of Medicinal Cannabis on Pain and Quality-of-Life Outcomes in Chronic Pain. Clin. J. Pain 2016, 32, 1036–1043. [Google Scholar] [CrossRef] [PubMed]
- Prommer, E.E. Pharmacological Management of Cancer-Related Pain. Cancer Control 2015, 22, 412–425. [Google Scholar] [CrossRef] [PubMed]
- Candido, K.D.; Kusper, T.M.; Knezevic, N.N. New Cancer Pain Treatment Options. Curr. Pain Headache Rep. 2017, 21, 12. [Google Scholar] [CrossRef] [PubMed]
- Bruera, E. Parenteral Opioid Shortage—Treating Pain during the Opioid-Overdose Epidemic. N. Engl. J. Med. 2018, 379, 601–603. [Google Scholar] [CrossRef]
- Kwon, J.H. Overcoming Barriers in Cancer Pain Management. J. Clin. Oncol. 2014, 32, 1727–1733. [Google Scholar] [CrossRef]
- Häuser, W.; Welsch, P.; Klose, P.; Radbruch, L.; Fitzcharles, M.-A. Efficacy, tolerability and safety of cannabis-based medicines for cancer pain. Schmerz 2019, 33, 424–436. [Google Scholar] [CrossRef]
- Chayasirisobhon, S. Mechanisms of Action and Pharmacokinetics of Cannabis. Perm. J. 2020, 25, 1–4. [Google Scholar] [CrossRef]
- Martín-Sánchez, E.; Furukawa, T.A.; Taylor, J.; Martin, J.L.R. Systematic Review and Meta-analysis of Cannabis Treatment for Chronic Pain. Pain Med. 2009, 10, 1353–1368. [Google Scholar] [CrossRef] [PubMed]
- Nugent, S.M.; Morasco, B.J.; O’Neil, M.E.; Freeman, M.; Low, A.; Kondo, K.; Elven, C.; Zakher, B.; Motu’apuaka, M.; Paynter, R.; et al. The Effects of Cannabis Among Adults with Chronic Pain and an Overview of General Harms. Ann. Intern. Med. 2017, 167, 319–331. [Google Scholar] [CrossRef]
- van den Beuken-van Everdingen, M.H.J.; Hochstenbach, L.M.J.; Joosten, E.A.J.; Tjan-Heijnen, V.C.G.; Janssen, D.J.A. Update on Prevalence of Pain in Patients with Cancer: Systematic Review and Meta-Analysis. J. Pain Symptom Manag. 2016, 51, 1070–1090.e9. [Google Scholar] [CrossRef] [Green Version]
- Russo, M.M.; Sundaramurthi, T. An Overview of Cancer Pain: Epidemiology and Pathophysiology. Semin. Oncol. Nurs. 2019, 35, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Leppert, W.; Zajączkowska, R.; Wordliczek, J.; Dobrogowski, J.; Woroń, J.; Krzakowski, M. Pathophysiology and clinical characteristics of pain in most common locations in cancer patients. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2016, 67, 787–799. [Google Scholar]
- Wordliczek, J.; Zajaczkowska, R. Mechanisms in Cancer Pain. In Cancer Pain; Hanna, M., Zylicz, Z., Eds.; Springer: London, UK, 2013; pp. 47–70. ISBN 978-0-85729-230-8. [Google Scholar]
- Yoon, S.Y.; Oh, J. Neuropathic cancer pain: Prevalence, pathophysiology, and management. Korean J. Intern. Med. 2018, 33, 1058–1069. [Google Scholar] [CrossRef] [PubMed]
- Fink, R.M.; Gallagher, E. Cancer Pain Assessment and Measurement. Semin. Oncol. Nurs. 2019, 35, 229–234. [Google Scholar] [CrossRef]
- World Health Organization. Cancer Pain Relief; World Health Organization: Geneva, Switzerland, 1986.
- Smith, T.J.; Saiki, C.B. Cancer Pain Management. Mayo Clin. Proc. 2015, 90, 1428–1439. [Google Scholar] [CrossRef]
- Roberto, A.; Greco, M.T.; Uggeri, S.; Cavuto, S.; Deandrea, S.; Corli, O.; Apolone, G. Living systematic review to assess the analgesic undertreatment in cancer patients. Pain Pract. 2022, 22, 487–496. [Google Scholar] [CrossRef]
- Stanic, J.; Perrenoud, B.; Rochat, E.; Ballabeni, P.; Jaques, C.; Schaer-Chaudhry, A.-C.; Zumstein-Shaha, M. Experiences of newly diagnosed cancer patients in confronting the finitudes of life: A qualitative systematic review protocol. JBI Evid. Synth. 2018, 16, 2288–2294. [Google Scholar] [CrossRef]
- Clark, J.; Gnanapragasam, S.; Greenley, S.; Pearce, J.; Johnson, M. Perceptions and experiences of laws and regulations governing access to opioids in South, Southeast, East and Central Asia: A systematic review, critical interpretative synthesis and development of a conceptual framework. Palliat. Med. 2021, 35, 59–75. [Google Scholar] [CrossRef]
- Stein, K.D.; Alcaraz, K.I.; Kamson, C.; Fallon, E.A.; Smith, T.G. Sociodemographic inequalities in barriers to cancer pain management: A report from the American Cancer Society’s Study of Cancer Survivors-II (SCS-II). Psycho-Oncol. 2016, 25, 1212–1221. [Google Scholar] [CrossRef]
- Paice, J.A. Cancer pain management and the opioid crisis in America: How to preserve hard-earned gains in improving the quality of cancer pain management. Cancer 2018, 124, 2491–2497. [Google Scholar] [CrossRef]
- Patton, T.; Revill, P.; Sculpher, M.; Borquez, A. Using Economic Evaluation to Inform Responses to the Opioid Epidemic in the United States: Challenges and Suggestions for Future Research. Subst. Use Misuse 2022, 57, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Fredheim, O.M.S.; Brelin, S.; Hjermstad, M.J.; Loge, J.H.; Aass, N.; Johannesen, T.B.; Skurtveit, S. Prescriptions of analgesics during complete disease trajectories in patients who are diagnosed with and die from cancer within the five-year period 2005–2009. Eur. J. Pain Lond. Engl. 2017, 21, 530–540. [Google Scholar] [CrossRef]
- Ziegler, L.; Mulvey, M.; Blenkinsopp, A.; Petty, D.; Bennett, M.I. Opioid prescribing for patients with cancer in the last year of life: A longitudinal population cohort study. Pain 2016, 157, 2445–2451. [Google Scholar] [CrossRef] [PubMed]
- George, B.; Minello, C.; Allano, G.; Maindet, C.; Burnod, A.; Lemaire, A. Opioids in cancer-related pain: Current situation and outlook. Supportive Care Cancer 2019, 27, 3105–3118. [Google Scholar] [CrossRef]
- Wall, T.; Sherwin, A.; Ma, D.; Buggy, D.J. Influence of perioperative anaesthetic and analgesic interventions on oncological outcomes: A narrative review. Br. J. Anaesth. 2019, 123, 135–150. [Google Scholar] [CrossRef] [PubMed]
- Sekandarzad, M.W.; Doornebal, C.; Hollmann, M.W. Opiophobia in Cancer Biology-Justified?—The Role of Perioperative Use of Opioids in Cancer Recurrence. Curr. Pharm. Des. 2019, 25, 3020–3027. [Google Scholar] [CrossRef] [PubMed]
- Bar-Sela, G.; Cohen, I.; Campisi-Pinto, S.; Lewitus, G.M.; Oz-Ari, L.; Jehassi, A.; Peer, A.; Turgeman, I.; Vernicova, O.; Berman, P.; et al. Cannabis Consumption Used by Cancer Patients during Immunotherapy Correlates with Poor Clinical Outcome. Cancers 2020, 12, 2447. [Google Scholar] [CrossRef]
- Blake, A.; Wan, B.A.; Malek, L.; DeAngelis, C.; Diaz, P.; Lao, N.; Chow, E.; O’Hearn, S. A selective review of medical cannabis in cancer pain management. Ann. Palliat. Med. 2017, 6, S215–S222. [Google Scholar] [CrossRef]
- Andre, C.M.; Hausman, J.-F.; Guerriero, G. Cannabis sativa: The Plant of the Thousand and One Molecules. Front. Plant Sci. 2016, 7, 19. [Google Scholar] [CrossRef]
- Hill, K.P.; Palastro, M.D.; Johnson, B.; Ditre, J.W. Cannabis and Pain: A Clinical Review. Cannabis Cannabinoid Res. 2017, 2, 96–104. [Google Scholar] [CrossRef]
- Mechoulam, R.; Parker, L.A. The Endocannabinoid System and the Brain. Annu. Rev. Psychol. 2013, 64, 21–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Battista, N.; Di Tommaso, M.; Bari, M.; Maccarrone, M. The endocannabinoid system: An overview. Front. Behav. Neurosci. 2012, 6, 9. [Google Scholar] [CrossRef] [PubMed]
- Ueda, N.; Tsuboi, K.; Uyama, T.; Ohnishi, T. Biosynthesis and degradation of the endocannabinoid 2-arachidonoylglycerol. BioFactors Oxf. Engl. 2011, 37, 1–7. [Google Scholar] [CrossRef]
- Wang, J.; Ueda, N. Biology of endocannabinoid synthesis system. Prostaglandins Other Lipid Mediat. 2009, 89, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Ligresti, A.; Petrosino, S.; Di Marzo, V. From endocannabinoid profiling to ‘endocannabinoid therapeutics. Curr. Opin. Chem. Biol. 2009, 13, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Zou, S.; Kumar, U. Cannabinoid Receptors and the Endocannabinoid System: Signaling and Function in the Central Nervous System. Int. J. Mol. Sci. 2018, 19, 833. [Google Scholar] [CrossRef]
- Mackie, K. Distribution of Cannabinoid Receptors in the Central and Peripheral Nervous System. In Cannabinoids; Pertwee, R.G., Ed.; Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2005; pp. 299–325. [Google Scholar]
- Ye, L.; Cao, Z.; Wang, W.; Zhou, N. New Insights in Cannabinoid Receptor Structure and Signaling. Curr. Mol. Pharmacol. 2019, 12, 239–248. [Google Scholar] [CrossRef]
- Lauckner, J.E.; Jensen, J.B.; Chen, H.-Y.; Lu, H.-C.; Hille, B.; Mackie, K. GPR55 is a cannabinoid receptor that increases intracellular calcium and inhibits M current. Proc. Natl. Acad. Sci. USA 2008, 105, 2699–2704. [Google Scholar] [CrossRef]
- Bian, Y.; He, X.; Jing, Y.; Wang, L.; Wang, J.; Xie, X.-Q. Computational systems pharmacology analysis of cannabidiol: A combination of chemogenomics-knowledgebase network analysis and integrated in silico modeling and simulation. Acta Pharmacol. Sin. 2019, 40, 374–386. [Google Scholar] [CrossRef]
- Da Fonseca Pacheco, D.; Klein, A.; De Castro Perez, A.; Da Fonseca Pacheco, C.M.; De Francischi, J.N.; Duarte, I.D.G. The μ-opioid receptor agonist morphine, but not agonists at δ- or κ-opioid receptors, induces peripheral antinociception mediated by cannabinoid receptors. Br. J. Pharmacol. 2008, 154, 1143–1149. [Google Scholar] [CrossRef]
- Watkins, A.R. Cannabinoid interactions with ion channels and receptors. Channels 2019, 13, 162–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, J.M.; Huang, S.M. Cannabinoid analgesia. Pharmacol. Ther. 2002, 95, 127–135. [Google Scholar] [CrossRef]
- Zogopoulos, P.; Vasileiou, I.; Patsouris, E.; Theocharis, S.E. The role of endocannabinoids in pain modulation. Fundam. Clin. Pharmacol. 2013, 27, 64–80. [Google Scholar] [CrossRef] [PubMed]
- Potenzieri, C.; Brink, T.S.; Pacharinsak, C.; Simone, D.A. Cannabinoid Modulation of Cutaneous Aδ Nociceptors During Inflammation. J. Neurophysiol. 2008, 100, 2794–2806. Available online: https://journals.physiology.org/doi/full/10.1152/jn.90809.2008 (accessed on 17 August 2022). [CrossRef] [PubMed]
- Uhelski, M.L.; Cain, D.M.; Harding-Rose, C.; Simone, D.A. The non-selective cannabinoid receptor agonist WIN 55,212-2 attenuates responses of C-fiber nociceptors in a murine model of cancer pain. Neuroscience 2013, 247, 84–94. [Google Scholar] [CrossRef]
- Tijani, A.O.; Thakur, D.; Mishra, D.; Frempong, D.; Chukwunyere, U.I.; Puri, A. Delivering therapeutic cannabinoids via skin: Current state and future perspectives. J. Control. Release 2021, 334, 427–451. [Google Scholar] [CrossRef]
- Bloomfield, M.A.P.; Ashok, A.H.; Volkow, N.D.; Howes, O.D. The effects of Δ9-tetrahydrocannabinol on the dopamine system. Nature 2016, 539, 369–377. [Google Scholar] [CrossRef]
- Amin, M.R.; Ali, D.W. Pharmacology of Medical Cannabis. In Recent Advances in Cannabinoid Physiology and Pathology; Bukiya, A.N., Ed.; Advances in Experimental Medicine and Biology; Springer International Publishing: Cham, Germany, 2019; pp. 151–165. [Google Scholar]
- Rock, E.M.; Parker, L.A. Constituents of Cannabis Sativa. In Cannabinoids and Neuropsychiatric Disorders; Murillo-Rodriguez, E., Pandi-Perumal, S.R., Monti, J.M., Eds.; Advances in Experimental Medicine and Biology; Springer International Publishing: Cham, Germany, 2021; pp. 1–13. ISBN 978-3-030-57369-0. [Google Scholar]
- Boggs, D.L.; Nguyen, J.D.; Morgenson, D.; Taffe, M.A.; Ranganathan, M. Clinical and Preclinical Evidence for Functional Interactions of Cannabidiol and Δ9-Tetrahydrocannabinol. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2018, 43, 142–154. [Google Scholar] [CrossRef]
- Ożarowski, M.; Karpiński, T.M.; Zielińska, A.; Souto, E.B.; Wielgus, K. Cannabidiol in Neurological and Neoplastic Diseases: Latest Developments on the Molecular Mechanism of Action. Int. J. Mol. Sci. 2021, 22, 4294. [Google Scholar] [CrossRef]
- Mlost, J.; Bryk, M.; Starowicz, K. Cannabidiol for Pain Treatment: Focus on Pharmacology and Mechanism of Action. Int. J. Mol. Sci. 2020, 21, 8870. [Google Scholar] [CrossRef]
- Lucas, C.J.; Galettis, P.; Schneider, J. The pharmacokinetics and the pharmacodynamics of cannabinoids. Br. J. Clin. Pharmacol. 2018, 84, 2477–2482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reuter, S.E.; Martin, J.H. Pharmacokinetics of Cannabis in Cancer Cachexia-Anorexia Syndrome. Clin. Pharmacokinet. 2016, 55, 807–812. [Google Scholar] [CrossRef]
- Biehl, J.R.; Burnham, E.L. Cannabis Smoking in 2015: A Concern for Lung Health? Chest 2015, 148, 596–606. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Murthy, P.; Bharath, M.M.S. Chemistry, Metabolism, and Toxicology of Cannabis: Clinical Implications. Iran. J. Psychiatry 2012, 7, 149–156. [Google Scholar] [PubMed]
- Flachenecker, P.; Henze, T.; Zettl, U.K. Nabiximols (THC/CBD Oromucosal Spray, Sativex®) in Clinical Practice—Results of a Multicenter, Non-Interventional Study (MOVE 2) in Patients with Multiple Sclerosis Spasticity. Eur. Neurol. 2014, 71, 271–279. [Google Scholar] [CrossRef]
- Abu-Sawwa, R.; Scutt, B.; Park, Y. Emerging Use of Epidiolex (Cannabidiol) in Epilepsy. J. Pediatr. Pharmacol. Ther. 2020, 25, 485–499. [Google Scholar] [CrossRef]
- Badowski, M.E.; Yanful, P.K. Dronabinol oral solution in the management of anorexia and weight loss in AIDS and cancer. Ther. Clin. Risk Manag. 2018, 14, 643–651. [Google Scholar] [CrossRef]
- Savage, S.R.; Romero-Sandoval, A.; Schatman, M.; Wallace, M.; Fanciullo, G.; McCarberg, B.; Ware, M. Cannabis in Pain Treatment: Clinical and Research Considerations. J. Pain 2016, 17, 654–668. [Google Scholar] [CrossRef]
- Chung, M.; Kim, H.K.; Abdi, S. Update on cannabis and cannabinoids for cancer pain. Curr. Opin. Anesthesiol. 2020, 33, 825–831. [Google Scholar] [CrossRef]
- Dhopeshwarkar, A.; Mackie, K. CB2 Cannabinoid Receptors as a Therapeutic Target—What Does the Future Hold? Mol. Pharmacol. 2014, 86, 430–437. [Google Scholar] [CrossRef]
- Woodhams, S.G.; Chapman, V.; Finn, D.P.; Hohmann, A.G.; Neugebauer, V. The cannabinoid system and pain. Neuropharmacology 2017, 124, 105–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soliman, N.; Haroutounian, S.; Hohmann, A.G.; Krane, E.; Liao, J.; Macleod, M.; Segelcke, D.; Sena, C.; Thomas, J.; Vollert, J.; et al. Systematic review and meta-analysis of cannabinoids, cannabis-based medicines, and endocannabinoid system modulators tested for antinociceptive effects in animal models of injury-related or pathological persistent pain. Pain 2021, 162, S26–S44. [Google Scholar] [CrossRef] [PubMed]
- Bennett, M.I.; Rayment, C.; Hjermstad, M.; Aass, N.; Caraceni, A.; Kaasa, S. Prevalence and aetiology of neuropathic pain in cancer patients: A systematic review. Pain 2012, 153, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Massey, R.L.; Kim, H.K.; Abdi, S. Brief review: Chemotherapy-induced painful peripheral neuropathy (CIPPN): Current status and future directions. Can. J. Anesth. Can. Anesth. 2014, 61, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Burgos, E.; Gómez-Nicola, D.; Pascual, D.; Martín, M.I.; Nieto-Sampedro, M.; Goicoechea, C. Cannabinoid agonist WIN 55,212-2 prevents the development of paclitaxel-induced peripheral neuropathy in rats. Possible involvement of spinal glial cells. Eur. J. Pharmacol. 2012, 682, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Rahn, E.J.; Deng, L.; Thakur, G.A.; Vemuri, K.; Zvonok, A.M.; Lai, Y.Y.; Makriyannis, A.; Hohmann, A.G. Prophylactic cannabinoid administration blocks the development of paclitaxel-induced neuropathic nociception during analgesic treatment and following cessation of drug delivery. Mol. Pain 2014, 10, 27. [Google Scholar] [CrossRef]
- Wu, J.; Hocevar, M.; Bie, B.; Foss, J.F.; Naguib, M. Cannabinoid Type 2 Receptor System Modulates Paclitaxel-Induced Microglial Dysregulation and Central Sensitization in Rats. J. Pain 2019, 20, 501–514. [Google Scholar] [CrossRef]
- King, K.M.; Myers, A.M.; Soroka-Monzo, A.J.; Tuma, R.F.; Tallarida, R.J.; Walker, E.A.; Ward, S.J. Single and combined effects of Δ9 -tetrahydrocannabinol and cannabidiol in a mouse model of chemotherapy-induced neuropathic pain. Br. J. Pharmacol. 2017, 174, 2832–2841. [Google Scholar] [CrossRef]
- Rahn, E.J.; Makriyannis, A.; Hohmann, A.G. Activation of cannabinoid CB1 and CB2 receptors suppresses neuropathic nociception evoked by the chemotherapeutic agent vincristine in rats. Br. J. Pharmacol. 2007, 152, 765–777. [Google Scholar] [CrossRef]
- Deng, L.; Guindon, J.; Vemuri, V.K.; Thakur, G.A.; White, F.A.; Makriyannis, A.; Hohmann, A.G. The maintenance of cisplatin- and paclitaxel-induced mechanical and cold allodynia is suppressed by cannabinoid CB2 receptor activation and independent of CXCR4 signaling in models of chemotherapy-induced peripheral neuropathy. Mol. Pain 2012, 8, 71. [Google Scholar] [CrossRef]
- Harris, H.M.; Sufka, K.J.; Gul, W.; ElSohly, M.A. Effects of Delta-9-Tetrahydrocannabinol and Cannabidiol on Cisplatin-Induced Neuropathy in Mice. Planta Med. 2016, 82, 1169–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mecs, L.; Tuboly, G.; Toth, K.; Nagy, E.; Nyari, T.; Benedek, G.; Horvath, G. Peripheral antinociceptive effect of 2-arachidonoyl-glycerol and its interaction with endomorphin-1 in arthritic rat ankle joints. Clin. Exp. Pharmacol. Physiol. 2010, 37, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, A.K.; Neufeld, M.; Jesus, C.H.A.; Cunha, J.M. Peripheral antinociceptive effect of anandamide and drugs that affect the endocannabinoid system on the formalin test in normal and streptozotocin-diabetic rats. Neuropharmacology 2012, 63, 1286–1297. [Google Scholar] [CrossRef] [PubMed]
- Karbarz, M.J.; Luo, L.; Chang, L.; Tham, C.-S.; Palmer, J.A.; Wilson, S.J.; Wennerholm, M.L.; Brown, S.M.; Scott, B.P.; Apodaca, R.L.; et al. Biochemical and Biological Properties of 4-(3-phenyl-[1,2,4] thiadiazol-5-yl)-piperazine-1-carboxylic acid phenylamide, a Mechanism-Based Inhibitor of Fatty Acid Amide Hydrolase. Anesth. Analg. 2009, 108, 316–329. [Google Scholar] [CrossRef]
- Cravatt, B.F.; Demarest, K.; Patricelli, M.P.; Bracey, M.H.; Giang, D.K.; Martin, B.R.; Lichtman, A.H. Supersensitivity to anandamide and enhanced endogenous cannabinoid signaling in mice lacking fatty acid amide hydrolase. Proc. Natl. Acad. Sci. USA 2001, 98, 9371–9376. Available online: https://www.pnas.org/doi/abs/10.1073/pnas.161191698 (accessed on 1 August 2022). [CrossRef] [PubMed]
- Kamimura, R.; Hossain, M.Z.; Unno, S.; Ando, H.; Masuda, Y.; Takahashi, K.; Otake, M.; Saito, I.; Kitagawa, J. Inhibition of 2-arachydonoylgycerol degradation attenuates orofacial neuropathic pain in trigeminal nerve-injured mice. J. Oral Sci. 2018, 60, 37–44. [Google Scholar] [CrossRef]
- Desroches, J.; Guindon, J.; Lambert, C.; Beaulieu, P. Modulation of the anti-nociceptive effects of 2-arachidonoyl glycerol by peripherally administered FAAH and MGL inhibitors in a neuropathic pain model. Br. J. Pharmacol. 2008, 155, 913–924. [Google Scholar] [CrossRef]
- Khasabova, I.A.; Chandiramani, A.; Harding-Rose, C.; Simone, D.A.; Seybold, V.S. Increasing 2-arachidonoyl glycerol signaling in the periphery attenuates mechanical hyperalgesia in a model of bone cancer pain. Pharmacol. Res. 2011, 64, 60–67. [Google Scholar] [CrossRef]
- Noyes, R.; Brunk, S.F.; Baram, D.A.; Canter, A. Analgesic effect of delta-9-tetrahydrocannabinol. J. Clin. Pharmacol. 1975, 15, 139–143. [Google Scholar] [CrossRef]
- Noyes, R., Jr.; Brunk, S.F.; Avery, D.H.; Canter, A. The analgesic properties of delta-9-tetrahydrocannabinol and codeine. Clin. Pharmacol. Ther. 1975, 18, 84–89. [Google Scholar] [CrossRef]
- Johnson, J.R.; Lossignol, D.; Burnell-Nugent, M.; Fallon, M.T. An Open-Label Extension Study to Investigate the Long-Term Safety and Tolerability of THC/CBD Oromucosal Spray and Oromucosal THC Spray in Patients With Terminal Cancer-Related Pain Refractory to Strong Opioid Analgesics. J. Pain Symptom Manag. 2013, 46, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Lichtman, A.H.; Lux, E.A.; McQuade, R.; Rossetti, S.; Sanchez, R.; Sun, W.; Wright, S.; Kornyeyeva, E.; Fallon, M.T. Results of a Double-Blind, Randomized, Placebo-Controlled Study of Nabiximols Oromucosal Spray as an Adjunctive Therapy in Advanced Cancer Patients with Chronic Uncontrolled Pain. J. Pain Symptom Manag. 2018, 55, 179–188.e1. [Google Scholar] [CrossRef] [PubMed]
- Bar-Lev Schleider, L.; Mechoulam, R.; Lederman, V.; Hilou, M.; Lencovsky, O.; Betzalel, O.; Shbiro, L.; Novack, V. Prospective analysis of safety and efficacy of medical cannabis in large unselected population of patients with cancer. Eur. J. Intern. Med. 2018, 49, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Hong, P.J.; May, C.; Rehman, Y.; Oparin, Y.; Hong, C.J.; Hong, B.Y.; AminiLari, M.; Gallo, L.; Kaushal, A.; et al. Medical cannabis or cannabinoids for chronic non-cancer and cancer related pain: A systematic review and meta-analysis of randomised clinical trials. BMJ 2021, 374, n1034. [Google Scholar] [CrossRef]
- Lynch, M.E.; Cesar-Rittenberg, P.; Hohmann, A.G. A Double-Blind, Placebo-Controlled, Crossover Pilot Trial With Extension Using an Oral Mucosal Cannabinoid Extract for Treatment of Chemotherapy-Induced Neuropathic Pain. J. Pain Symptom Manag. 2014, 47, 166–173. [Google Scholar] [CrossRef]
- Wang, T.; Collet, J.-P.; Shapiro, S.; Ware, M.A. Adverse effects of medical cannabinoids: A systematic review. CMAJ 2008, 178, 1669–1678. [Google Scholar] [CrossRef]
- Machado Bergamaschi, M.; Helena Costa Queiroz, R.; Waldo Zuardi, A.; Alexandre, S.; Crippa, J. Safety and Side Effects of Cannabidiol, a Cannabis sativa Constituent. Curr. Drug Saf. 2011, 6, 237–249. [Google Scholar] [CrossRef]
- Campeny, E.; López-Pelayo, H.; Nutt, D.; Blithikioti, C.; Oliveras, C.; Nuño, L.; Maldonado, R.; Florez, G.; Arias, F.; Fernández-Artamendi, S.; et al. The blind men and the elephant: Systematic review of systematic reviews of cannabis use related health harms. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2020, 33, 1–35. [Google Scholar] [CrossRef]
- Volkow, N.D.; Baler, R.D.; Compton, W.M.; Weiss, S.R.B. Adverse Health Effects of Marijuana Use. N. Engl. J. Med. 2014, 370, 2219–2227. [Google Scholar] [CrossRef]
- Freeman, T.P.; Hindocha, C.; Green, S.F.; Bloomfield, M.A.P. Medicinal use of cannabis based products and cannabinoids. BMJ 2019, 365, l1141. [Google Scholar] [CrossRef]
- Powell, D.; Pacula, R.L.; Jacobson, M. Do medical marijuana laws reduce addictions and deaths related to pain killers? J. Health Econ. 2018, 58, 29–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayor, S. WHO proposes rescheduling cannabis to allow medical applications. BMJ 2019, 364, l574. [Google Scholar] [CrossRef] [PubMed]
- Maharajan, M.K.; Yong, Y.J.; Yip, H.Y.; Woon, S.S.; Yeap, K.M.; Yap, K.Y.; Yip, S.C.; Yap, K.X. Medical cannabis for chronic pain: Can it make a difference in pain management? J. Anesth. 2020, 34, 95–103. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Study Name | Phase | Status | Condition | Treatment | Primary Endpoint |
|---|---|---|---|---|---|
| NCT04808531 | Phase 3 | Not yet recruiting | Cancer-related pain | NanaBisTM Oxycodone Placebo Spray Placebo Tablet | Significant changes in responders with NanaBis™ spray over placebo Comparable efficacy in proportion of responders from NanaBis™ spray to the proportion of responders to Oxycodone |
| NCT04875286 | N/A | Recruiting | Cancer-associated pain | Electronic health record review Questionnaire administration | Proportion of patients who prefer opioids + THC-marijuana and/or opioids with CBD to opioids alone for cancer pain relief |
| NCT03948074 | Phase 2 | Recruiting | Pain, nausea, anxiety, and sleep disturbance related to cancer | Cannabis | Average Patients’ Global Impression of Change (PGIC) for overall cancer-related symptoms |
| NCT04042545 | Phase 2 | Recruiting | Cancer pain QoL | Cannabis Placebo | Uncontrolled cancer pain measured using a patient’s self-administered questionnaire. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gorzo, A.; Havași, A.; Spînu, Ș.; Oprea, A.; Burz, C.; Sur, D. Practical Considerations for the Use of Cannabis in Cancer Pain Management—What a Medical Oncologist Should Know. J. Clin. Med. 2022, 11, 5036. https://doi.org/10.3390/jcm11175036
Gorzo A, Havași A, Spînu Ș, Oprea A, Burz C, Sur D. Practical Considerations for the Use of Cannabis in Cancer Pain Management—What a Medical Oncologist Should Know. Journal of Clinical Medicine. 2022; 11(17):5036. https://doi.org/10.3390/jcm11175036
Chicago/Turabian StyleGorzo, Alecsandra, Andrei Havași, Ștefan Spînu, Adela Oprea, Claudia Burz, and Daniel Sur. 2022. "Practical Considerations for the Use of Cannabis in Cancer Pain Management—What a Medical Oncologist Should Know" Journal of Clinical Medicine 11, no. 17: 5036. https://doi.org/10.3390/jcm11175036
APA StyleGorzo, A., Havași, A., Spînu, Ș., Oprea, A., Burz, C., & Sur, D. (2022). Practical Considerations for the Use of Cannabis in Cancer Pain Management—What a Medical Oncologist Should Know. Journal of Clinical Medicine, 11(17), 5036. https://doi.org/10.3390/jcm11175036