
Clinical and Epidemiological Characteristics of Bloodstream Infections in Head and Neck Cancer Patients: A Decadal Observational Study

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Definitions and Outcomes
2.3. Method for Collecting Blood Cultures
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gudiol, C.; Aguado, J.M.; Carratalà, J. Bloodstream infections in patients with solid tumors. Virulence 2016, 7, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global Cancer Statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, Y.; Cho, H.; Yamamoto, M.; Nakahara, S.; Yamamoto, Y.; Inohara, H. Incidence and predictors of febrile neutropenia during chemotherapy in patients with head and neck cancer. Support. Care Cancer 2013, 21, 2861–2868. [Google Scholar] [CrossRef] [PubMed]
- Trotti, A.; Bellm, L.A.; Epstein, J.B.; Frame, D.; Fuchs, H.J.; Gwede, C.K.; Komaroff, E.; Nalysnyk, L.; Zilberberg, M.D. Mucositis incidence, severity and associated outcomes in patients with head and neck cancer receiving radiotherapy with or without chemotherapy: A systematic literature review. Radiother. Oncol. 2003, 66, 253–262. [Google Scholar] [CrossRef]
- Anatoliotaki, M.; Valatas, V.; Mantadakis, E.; Apostolakou, H.; Mavroudis, D.; Georgoulias, V.; Rolston, K.V.; Kontoyiannis, D.P.; Galanakis, E.; Samonis, G. Bloodstream infections in patients with solid tumors: Associated factors, microbial spectrum and outcome. Infection 2004, 32, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Wisplinghoff, H.; Seifert, H.; Wenzel, R.P.; Edmond, M.B. Current trends in the epidemiology of nosocomial bloodstream infections in patients with hematological malignancies and solid neoplasms in hospitals in the United States. Clin. Infect. Dis. 2003, 36, 1103–1110. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.K.; Lyman, J.A. Updated review of blood culture contamination. Clin. Microbiol. Rev. 2006, 19, 788–802. [Google Scholar] [CrossRef]
- Mermel, L.A.; Allon, M.; Bouza, E.; Craven, D.E.; Flynn, P.; O’Grady, N.P.; Raad, I.I.; Rijnders, B.J.; Sherertz, R.J.; Warren, D.K. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2009, 49, 1–45. [Google Scholar] [CrossRef]
- Common Terminology Criteria for Adverse Events (CTCAE); Version 5; United States Department of Health and Human Services: Washington, DC, USA; National Institutes of Health—National Cancer Institute: Bethesda, MD, USA, 2017.
- Marschall, J.; Agniel, D.; Fraser, V.J.; Doherty, J.; Warren, D.K. Gram-negative bacteraemia in non-ICU patients: Factors associated with inadequate antibiotic therapy and impact on outcomes. J. Antimicrob. Chemother. 2008, 61, 1376–1383. [Google Scholar] [CrossRef]
- Vallés, J.; León, C.; Spanish Collaborative Group for Infections in Intensive Care Units of Sociedad Espanola de Medicina Intensiva y Unidades Coronarias (SEMIUC). Nosocomial bacteremia in critically ill patients: A multicenter study evaluating epidemiology and prognosis. Clin. Infect. Dis. 1997, 24, 387–395. [Google Scholar] [CrossRef][Green Version]
- Fritz, A.; Percy, C.; Jack, A.; Shanmugaratnam, K.; Sobin, L.; Parkin, D.; Whelan, S. (Eds.) International Classification of Diseases for Oncology (ICD-O), 3rd ed.; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Fritz, A.; Percy, C.; Jack, A.; Shanmugaratnam, K.; Sobin, L.; Parkin, D.; Whelan, S. (Eds.) International Classification of Diseases for Oncology (ICD-O), 1st Rev., 3rd ed.; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Fritz, A.; Percy, C.; Jack, A.; Shanmugaratnam, K.; Sobin, L.; Parkin, D.; Whelan, S. (Eds.) International Classification of Diseases for Oncology (ICD-O), 2nd Rev., 3rd ed.; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Greene, F.L.; Page, D.L.; Fleming, I.D. TNM Classification of Malignant Tumors, 6th ed.; Springer: New York, NY, USA, 2002. [Google Scholar]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumors, 7th ed.; Wiley-Blackwell: Oxford, UK, 2010. [Google Scholar]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumors, 8th ed.; Wiley-Blackwell: Oxford, UK, 2017. [Google Scholar]
- Marin, M.; Gudiol, C.; Ardanuy, C.; Garcia-Vidal, C.; Calvo, M.; Arnan, M.; Carratalà, J. Bloodstream infections in neutropenic patients with cancer: Differences between patients with haematological malignancies and solid tumours. J. Infect. 2014, 69, 417–423. [Google Scholar] [CrossRef]
- Samonis, G.; Vardakas, K.Z.; Maraki, S.; Tansarli, G.S.; Dimopoulou, D.; Kofteridis, D.P.; Andrianaki, A.M.; Falagas, M.E. A prospective study of characteristics and outcomes of bacteremia in patients with solid organ or hematologic malignancies. Support. Care Cancer 2013, 21, 2521–2526. [Google Scholar] [CrossRef] [PubMed]
- Jensen, K.H.; Vogelius, I.; Moser, C.E.; Andersen, E.; Eriksen, J.G.; Johansen, J.; Farhadi, M.; Andersen, M.; Overgaard, J.; Friborg, J. Bloodstream infections in head and neck cancer patients after curative-intent radiotherapy: A population-based study from the Danish Head and Neck Cancer Group database. Br. J. Cancer 2021, 125, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Escande, M.C.; Herbrecht, R. Prospective study of bacteraemia in cancer patients. results of a French multicentre study. Support. Care Cancer 1998, 6, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Cometta, A.; Calandra, T.; Gaya, H.; Zinner, S.H.; de Bock, R.; Del Favero, A.; Bucaneve, G.; Crokaert, F.; Kern, W.V.; Klastersky, J.; et al. Monotherapy with meropenem versus combination therapy with ceftazidime plus amikacin as empiric therapy for fever in granulocytopenic patients with cancer. The International Antimicrobial Therapy Cooperative Group of the European Organization for Research and Treatment of Cancer and the Gruppo Italiano Malattie Ematologiche Maligne dell’adulto Infection Program. Antimicrob. Agents Chemother. 1996, 40, 1108–1115. [Google Scholar] [CrossRef] [PubMed]
- Bochud, P.; Cometta, A.; Francioli, P. Virulent infections caused by alpha-haemolytic streptococci in cancer patients and their management. Curr. Opin. Infect. Dis. 1997, 10, 422–430. [Google Scholar] [CrossRef]
- Wisplinghoff, H.; Bischoff, T.; Tallent, S.M.; Seifert, H.; Wenzel, R.P.; Edmond, M.B. Nosocomial bloodstream infections in US hospitals: Analysis of 24,179 cases from a prospective nationwide surveillance study. Clin. Infect. Dis. 2004, 39, 309–317. [Google Scholar] [CrossRef]
- Yamada, K.; Kuwabara, G.; Imoto, W.; Yamairi, K.; Shibata, W.; Oshima, K.; Yoshii, N.; Nakaie, K.; Niki, M.; Okada, Y.; et al. Blood culture reports by infectious disease physicians can improve prognosis of bacteremia, including weekend-onset cases. Int. J. Infect. Dis. 2020, 100, 174–179. [Google Scholar] [CrossRef]
- Raad, I.; Hachem, R.; Hanna, H.; Bahna, P.; Chatzinikolaou, I.; Fang, X.; Jiang, Y.; Chemaly, R.F.; Rolston, K. Sources and outcome of bloodstream infections in cancer patients: The role of central venous catheters. Eur. J. Clin. Microbiol. Infect. Dis. 2007, 26, 549–556. [Google Scholar] [CrossRef]
- Akahane, A.; Sone, M.; Ehara, S.; Kato, K.; Tanaka, R.; Nakasato, T. Subclavian vein versus arm vein for totally implantable central venous port for patients with head and neck cancer: A retrospective comparative analysis. Cardiovasc. Interv. Radiol. 2011, 34, 1222–1229. [Google Scholar] [CrossRef]
- Bell, T.; O’Grady, N.P. Prevention of central line-associated bloodstream infections. Infect. Dis. Clin. N. Am. 2017, 31, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Bekçibaşi, M.; Dayan, S.; Aslan, E.; Kortak, M.Z.; Hoşoğlu, S. Risk factors for central venous catheter-related bloodstream infections. Infez. Med. 2019, 27, 258–265. [Google Scholar] [PubMed]
- O’Grady, N.P.; Alexander, M.; Burns, L.A.; Dellinger, E.P.; Garland, J.; Heard, S.O.; Lipsett, P.A.; Masur, H.; Mermel, L.A.; Pearson, M.L.; et al. Guidelines for the prevention of intravascular catheter-related infections. Clin. Infect. Dis. 2011, 52, e162–e193. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, A.Q.; Cao, L.; Xia, H.T.; Ma, J.J. Taurolidine lock solutions for the prevention of catheter-related bloodstream infections: A systematic review and meta-analysis of randomized controlled trials. PLoS ONE 2013, 8, e79417. [Google Scholar] [CrossRef]
- Bookstaver, P.B.; Gerrald, K.R.; Moran, R.R. Clinical outcomes of antimicrobial lock solutions used in a treatment modality: A retrospective case series analysis. Clin. Pharmacol. 2010, 2, 123–130. [Google Scholar] [CrossRef]
- Noelting, J.; Jurewitsch, B.; Allard, J.P. Non-antibiotic antimicrobial catheter lock solutions in patients on home parenteral nutrition. Nutrients 2018, 10, 1165. [Google Scholar] [CrossRef]
- Lee, Y.M.; Moon, C.; Kim, Y.J.; Lee, H.J.; Lee, M.S.; Park, K.H. Clinical impact of delayed catheter removal for patients with central-venous-catheter-related gram-negative bacteraemia. J. Hosp. Infect. 2018, 99, 106–113. [Google Scholar] [CrossRef]
- Annunziato, G. Strategies to overcome antimicrobial resistance (AMR) making use of non-essential target inhibitors: A review. Int. J. Mol. Sci. 2019, 20, 5844. [Google Scholar] [CrossRef]
- Jung, S.J.; Kim, D.Y.; Joo, S.Y. Rick factors associated with aspiration in patients with head and neck cancer. Ann. Rehabil. Med. 2011, 35, 781–790. [Google Scholar] [CrossRef]
- Pezdirec, M.; Strojan, P.; Boltezar, I.H. Swallowing disorders after treatment for head and neck cancer. Radiol. Oncol. 2019, 53, 225–230. [Google Scholar] [CrossRef]
- Van der Molen, L.; van Rossum, M.A.; Burkhead, L.M.; Smeele, L.E.; Hilgers, F.J. Functional outcomes and rehabilitation strategies in patients treated with chemoradiotherapy for advanced head and neck cancer: A systematic review. Eur. Arch. Otorhinolaryngol. 2009, 266, 889–900. [Google Scholar] [CrossRef] [PubMed]
- Manikantan, K.; Khode, S.; Sayed, S.I.; Roe, J.; Nutting, C.M.; Rhys-Evans, P.; Harrington, K.J.; Kazi, R. Dysphagia in head and neck cancer. Cancer Treat. Rev. 2009, 35, 724–732. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Non-BSI Group (n = 221) | BSI Group (n = 67) | p-Value | |
|---|---|---|---|
| Demographic | |||
| Sex (male, %) | 174 (78.7%) | 50 (74.6%) | 0.504 |
| Age, years, median (IQR) | 69 (64–75) | 71.0 (64.5–76) | 0.367 |
| Comorbidities | |||
| Diabetes mellitus | 48 (21.7%) | 14 (20.0%) | 1.000 |
| Dementia | 2 (0.9%) | 0 (0%) | 1.000 |
| Cerebrovascular disease | 17 (7.7%) | 7 (10.4%) | 0.457 |
| Respiratory disease | 37 (16.7%) | 18 (26.9%) | 0.076 |
| Digestive disease | 74 (33.5%) | 28 (41.8%) | 0.244 |
| Kidney and urological disease | 34 (15.4%) | 11 (16.4%) | 0.849 |
| Brain and nervous system disease | 4 (1.8%) | 0 (0%) | 0.576 |
| Social history | |||
| Chronic drinker | 127 (57.5%) (n = 220) | 31 (46.3%) | 0.123 |
| Smoking | 82 (37.1%) (n = 220) | 25 (37.3%) | 1.000 |
| Vital signs | |||
| Body weight, kg, median (IQR) | 50.3 (43.9–56.1) (n = 220) | 48.7 (43.4–53.9) | 0.385 |
| Body temperature, °C, median (IQR) | 38.2 (37.5–38.8) (n = 219) | 39.1 (38.4–39.6) | <0.001 * |
| Laboratory markers | |||
| WBC count, /μL, median (IQR) | 8868.4 (3600–11,900) | 7500 (2950–10,700) | 0.478 |
| Neutrophil count, /μL, median (IQR) | 8000.4 (2862.5–10,447.5) (n = 214) | 6470 (2815–9245) | 0.836 |
| C-reactive protein, mg/dL, median (IQR) | 9.3 (3.7–12) | 10.0 (4.0–18.1) | 0.036 * |
| Neutropenia | 11 (5.0%) | 5 (7.5%) | 0.541 |
| Mortality | |||
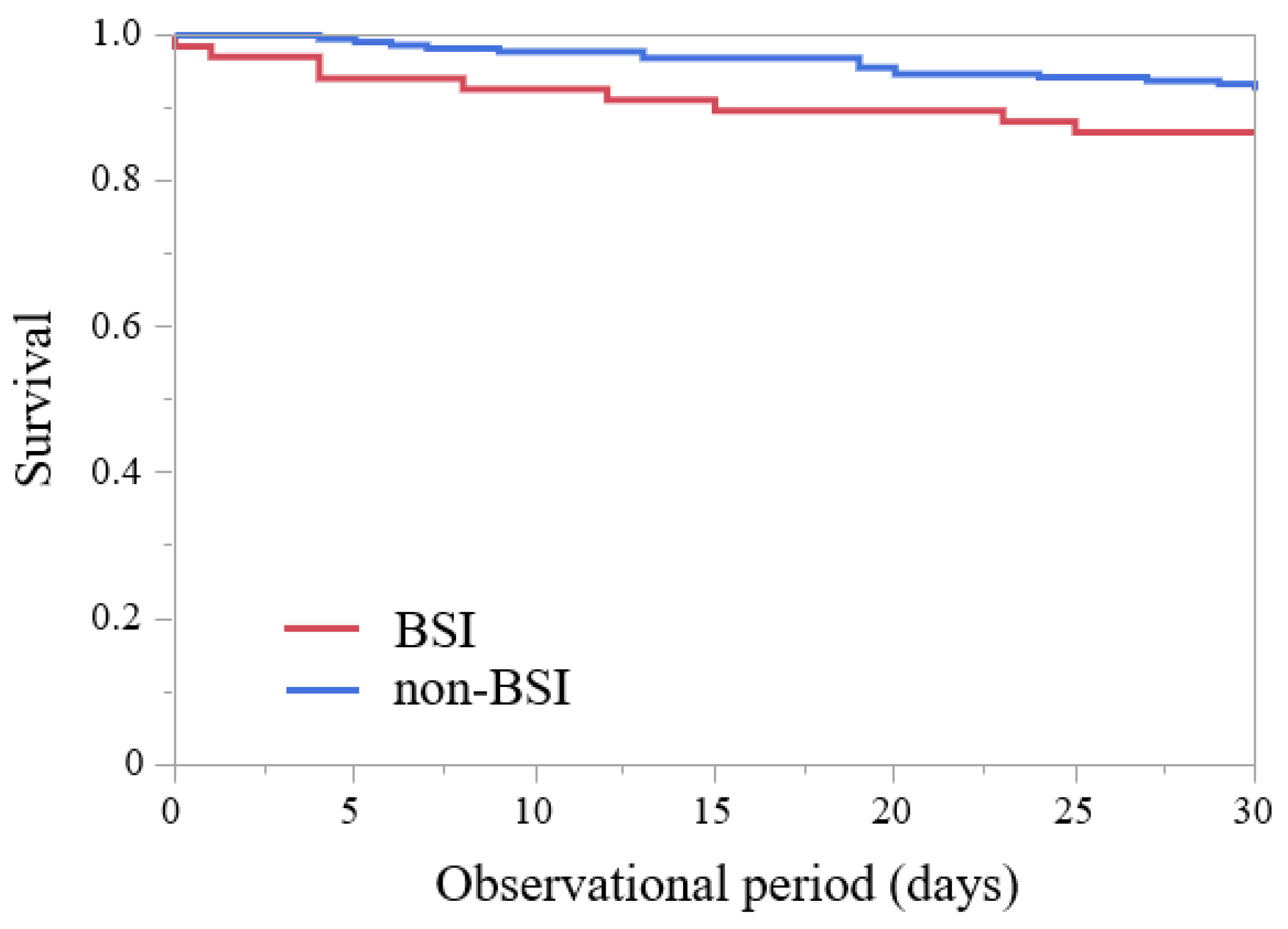
| 30-day mortality | 4 (1.8%) | 7 (10.4%) | 0.004 * |
| Duration of hospital stay, days, median (IQR) | 87.0 (56.5–112.8) (n = 218) | 86.0 (44–113) | 0.590 |
| Use of antibiotics (appropriate) | 54 (80.6%) | ||
| Ratio of infectious disease departments participating in treatment | 43 (64.2%) | ||
| Sets of blood cultures | |||
| One set | 24 (10.9%) | 12 (17.9%) | 0.141 |
| Two sets | 195 (88.2%) | 55 (82.1%) | 0.217 |
| Four sets | 2 (0.9%) | 0 (0%) | 1.000 |
| Monomicrobial/Polymicrobial | |||
| Monomicrobial | 12 (92.3%) | 53 (79.1%) | |
| Polymicrobial | 1 (7.7%) | 14 (20.9%) | |
| Site of infection | |||
| Catheter-related infection | 15 (6.8%) | 26 (38.8%) | <0.001 * |
| Respiratory tract infection | 50 (22.6%) | 13 (19.4%) | 0.618 |
| Catheter-associated urinary tract infection | 6 (2.7%) | 4 (6.0%) | 0.136 |
| Gastrointestinal infection | 3 (1.4%) | 3 (4.5%) | 0.141 |
| Pyogenic spondylitis | 1 (0.5%) | 3 (4.5%) | 0.040 * |
| Thrombophlebitis | 0 (0%) | 3 (4.5%) | 0.012 * |
| IE | 2 (0.9%) | 1 (1.5%) | 0.550 |
| Mucositis | 13 (5.9%) | 0 (0%) | 0.044 * |
| SSI | 4 (1.8%) | 0 (0%) | 0.576 |
| Tumor-infection | 3 (1.4%) | 0 (0%) | 1.000 |
| Cervical abscess | 2 (0.9%) | 0 (0%) | 1.000 |
| Contamination | 13 (5.9%) | ||
| Others | 12 (5.4%) | 4 (6.0%) | 0.770 |
| Unknown | 97 (43.9%) | 19 (28.4%) | 0.033 * |
| CVC/CV port | |||
| CVC presence | 28 (12.7%) | 23 (34.3%) | <0.001 * |
| CV port presence | 4 (1.8%) | 7 (10.4%) | 0.004 * |
| CVC duration before BSIs occurred, days, median (IQR) | 21 (12.8–41.3) | 20 (11–35) | 0.705 |
| CV port duration before BSIs occurred, days, median (IQR) | 87 (28.5–204.3) | 24 (20–153) | 0.412 |
| CVC removal | 17 (60.8%) | 18 (78.3%) | 0.034 * |
| CV port removal | 4 (100%) | 5 (71.4%) | <0.001 * |
| Tumor site | |||
| Oral cavity | 70 (31.7%) | 18 (26.9%) | 0.545 |
| Oropharynx | 47 (21.3%) | 11 (16.4%) | 0.487 |
| Hypopharynx | 49 (22.2%) | 18 (26.9%) | 0.415 |
| Larynx | 23 (10.4%) | 10 (14.9%) | 0.380 |
| Carcinoma of maxilla | 13 (5.9%) | 4 (6.0%) | 1.000 |
| Others | 19 (8.6%) | 6 (9.0%) | 1.000 |
| Cancer stage | 37 (16.7%) | 12 (17.9%) | 0.853 |
| Early stage (Stage I–II) | 167 (75.6%) | 51 (76.1%) | 1.000 |
| Locally advanced (Stage III–IV) | 17 (7.7%) | 4 (6.0%) | 1.000 |
| Recurrence or metastatic disease | 140 (63.3%) | 39 (58.2%) | 0.474 |
| Treatment | |||
| Surgical treatment | 39 (17.6%) | 16 (23.9%) | 0.288 |
| Chemotherapy | |||
| FP | 0 (0%) | 1 (1.5%) | 0.233 |
| TPF | 17 (7.7%) | 5 (7.5%) | 1.000 |
| Adriamycin | 1 (0.5%) | 1 (1.5%) | 0.412 |
| Other regimens | 2 (0.9%) | 1 (1.5%) | 0.550 |
| Radiotherapy | 26 (11.8%) | 9 (13.4%) | 0.675 |
| Chemoradiotherapy | |||
| CDDP-RT | 57 (25.8%) | 6 (9.0%) | 0.004 * |
| FP-RT | 7 (3.2%) | 1 (1.5%) | 0.686 |
| TPF-RT | 4 (1.8%) | 2 (3.0%) | 0.626 |
| DC-RT | 2 (0.9%) | 2 (3.0%) | 0.232 |
| Biotherapy | |||
| Cmab | 2 (0.9%) | 0 (0%) | 1.000 |
| Cmab-FP | 9 (4.1%) | 6 (9.0%) | 0.124 |
| Cmab-RT | 6 (2.7%) | 3 (4.5%) | 0.439 |
| Nivolumab | 2 (0.9%) | 1 (1.5%) | 0.550 |
| Treatment interval/Palliative care | 47 (21.3%) | 13 (19.4%) | 0.864 |
| Variable | Adjusted OR (95% CI) | p-Value |
|---|---|---|
| Sex | 1.580 (0.759–3.288) | 0.221 |
| Age | 1.025 (0.992–1.059) | 0.137 |
| Respiratory disease | 1.787 (0.860–3.717) | 0.120 |
| Body temperature, °C | 2.563 (1.829–3.593) | <0.001 * |
| C-reactive protein, mg/dL | 1.047 (1.009–1.085) | 0.013 * |
| CDDP-RT | 0.336 (0.129–0.870) | 0.025 * |
| Variable | Adjusted OR (95% CI) | p-Value |
|---|---|---|
| Sex | 3.619 (0.594–22.036) | 0.163 |
| Age | 0.959 (0.869–1.059) | 0.411 |
| Respiratory disease | 3.026 (0.486–18.828) | 0.235 |
| Body temperature, ℃ | 0.858 (0.310–2.375) | 0.768 |
| C-reactive protein, mg/dL | 1.058 (0.967–1.159) | 0.220 |
| CDDP-RT | 2.695 (0.185–39.271) | 0.468 |
| Causative Organisms | Number | Frequency |
|---|---|---|
| Gram-positive coccus | ||
| Staphylococcus aureus (MRSA) | 18 | 26.9% |
| Staphylococcus epidermidis | 12 | 17.9% |
| Staphylococcus aureus (MSSA) | 4 | 4.8% |
| Enterococcus faecalis | 2 | 6.0% |
| Staphylococcus capitis | 3 | 4.5% |
| Others | 6 | 9.0% |
| Gram-positive bacilli | ||
| Bacillus cereus | 3 | 4.5% |
| Bacillus spp. | 1 | 1.5% |
| Gram-negative bacilli | ||
| Pseudomonas aeruginosa | 7 | 10.4% |
| Enterobacter aerogenes | 6 | 9.0% |
| Klebsiella pneumoniae | 4 | 4.8% |
| Klebsiella oxytoca | 3 | 4.5% |
| Citrobacter koseri | 2 | 6.0% |
| Enterobacter cloacae | 2 | 6.0% |
| Others | 4 | 4.8% |
| Fungi | ||
| Candida albicans | 3 | 4.5% |
| Candida parapsilosis | 3 | 4.5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitaya, S.; Kakuta, R.; Kanamori, H.; Ohkoshi, A.; Ishii, R.; Nomura, K.; Tokuda, K.; Katori, Y. Clinical and Epidemiological Characteristics of Bloodstream Infections in Head and Neck Cancer Patients: A Decadal Observational Study. J. Clin. Med. 2022, 11, 4820. https://doi.org/10.3390/jcm11164820
Kitaya S, Kakuta R, Kanamori H, Ohkoshi A, Ishii R, Nomura K, Tokuda K, Katori Y. Clinical and Epidemiological Characteristics of Bloodstream Infections in Head and Neck Cancer Patients: A Decadal Observational Study. Journal of Clinical Medicine. 2022; 11(16):4820. https://doi.org/10.3390/jcm11164820
Chicago/Turabian StyleKitaya, Shiori, Risako Kakuta, Hajime Kanamori, Akira Ohkoshi, Ryo Ishii, Kazuhiro Nomura, Koichi Tokuda, and Yukio Katori. 2022. "Clinical and Epidemiological Characteristics of Bloodstream Infections in Head and Neck Cancer Patients: A Decadal Observational Study" Journal of Clinical Medicine 11, no. 16: 4820. https://doi.org/10.3390/jcm11164820
APA StyleKitaya, S., Kakuta, R., Kanamori, H., Ohkoshi, A., Ishii, R., Nomura, K., Tokuda, K., & Katori, Y. (2022). Clinical and Epidemiological Characteristics of Bloodstream Infections in Head and Neck Cancer Patients: A Decadal Observational Study. Journal of Clinical Medicine, 11(16), 4820. https://doi.org/10.3390/jcm11164820