
Dermoscopic Features of Different Forms of Cutaneous Mastocytosis: A Systematic Review

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
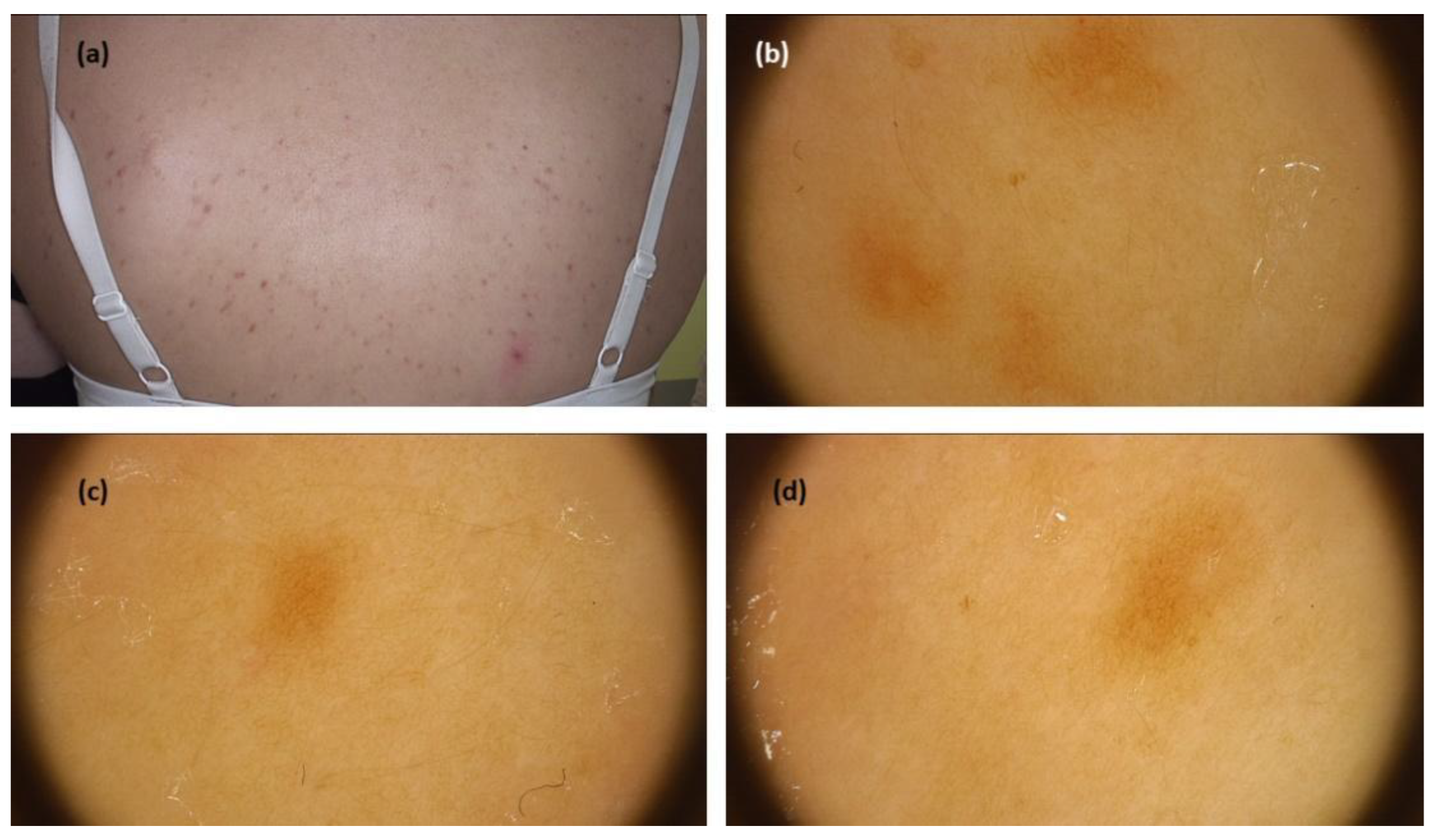
3.1. Maculopapular Cutaneous Mastocytosis (UP Clinical Subtype)
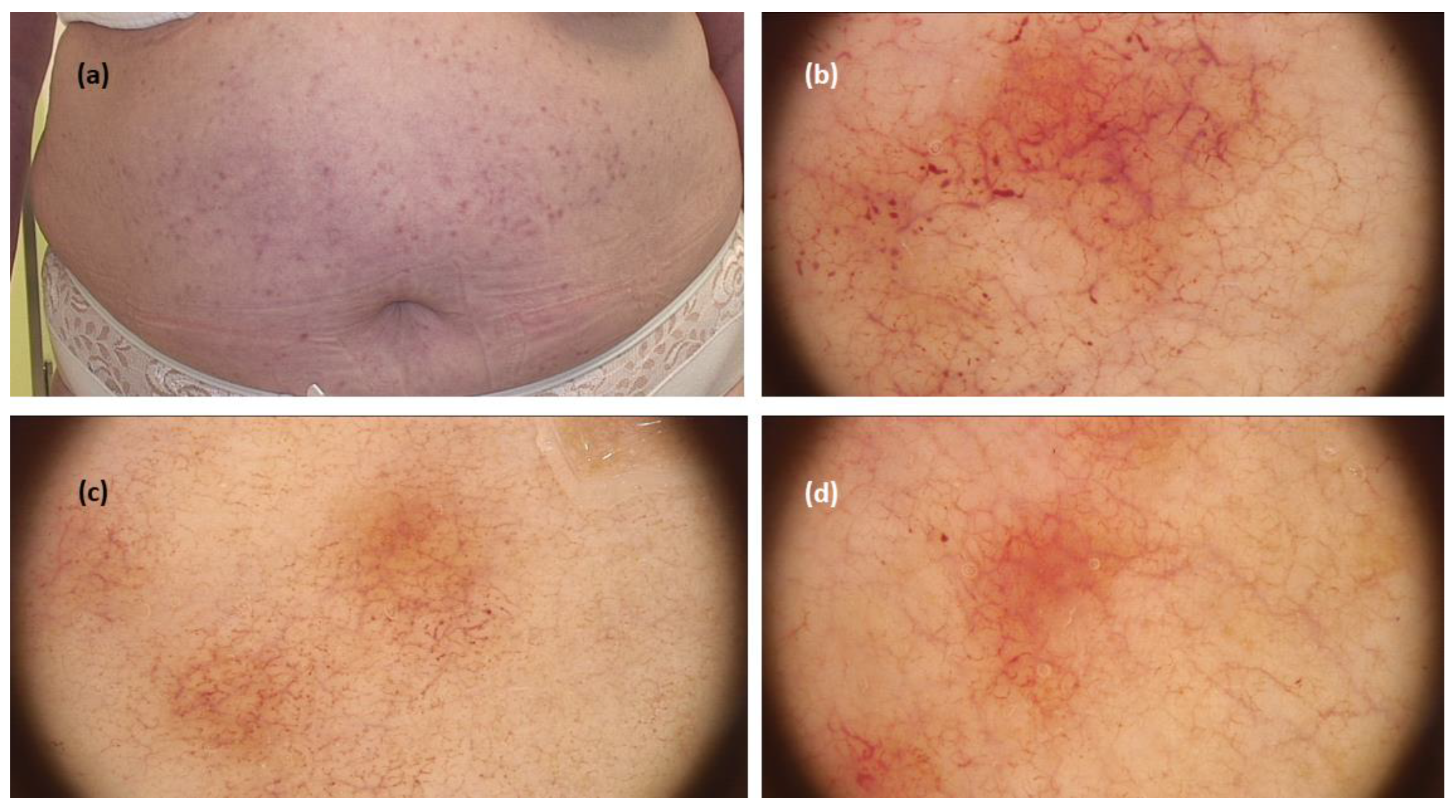
3.2. Maculopapular Cutaneous Mastocytosis (TMEP Clinical Subtype)
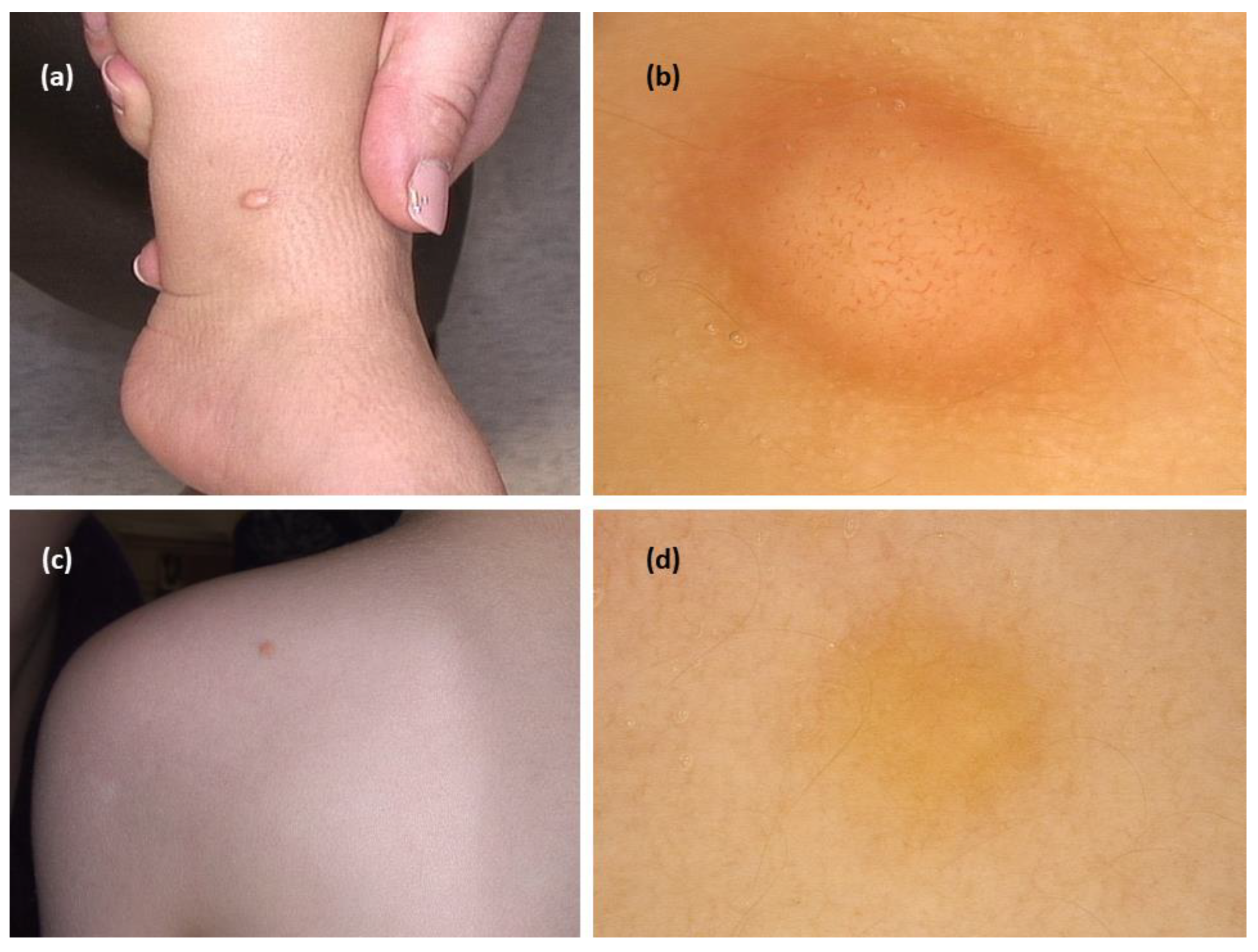
3.3. Mastocytoma
3.4. Other Clinical Forms of CM
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Valent, P.; Akin, C.; Gleixner, K.V.; Sperr, W.R.; Reiter, A.; Arock, M.; Triggiani, M. Multidisciplinary challenges in mastocytosis and how to address with personalized medicine approaches. Int. J. Mol. Sci. 2019, 20, 2976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartmann, K.; Escribano, L.; Grattan, C.; Brockow, K.; Carter, M.C.; Alvarez-Twose, I.; Matito, A.; Broesby-Olsen, S.; Siebenhaar, F.; Lange, M.; et al. Cutaneous manifestations in patients with mastocytosis: Consensus report of the European Competence Network on Mastocytosis; the American Academy of Allergy, Asthma &; Immunology; and the European Academy of Allergology and Clinical Immunology. J. Allergy Clin. Immunol. 2015, 137, 35–45. [Google Scholar] [PubMed]
- Brockow, K. Epidemiology, prognosis, and risk factors in mastocytosis. Immunol. Allergy Clin. N. Am. 2014, 34, 283–295. [Google Scholar] [CrossRef] [PubMed]
- Lange, M.; Hartmann, K.; Carter, M.; Siebenhaar, F.; Alvarez-Twose, I.; Torrado, I.; Brockow, K.; Renke, J.; Irga-Jaworska, N.; Plata-Nazar, K.; et al. Molecular Background, Clinical Features and Management of Pediatric Mastocytosis: Status 2021. Int. J. Mol. Sci. 2021, 22, 2586. [Google Scholar] [CrossRef] [PubMed]
- Valent, P.; Akin, C.; Metcalfe, D.D. Mastocytosis: 2016 updated WHO classification and novel emerging treatment concepts. Blood 2017, 129, 1420–1427. [Google Scholar] [CrossRef]
- Li, Q.; Zeng, K.; Peng, X.; Wang, F. Dermoscopic findings of pseudoxanthomatous mastocytosis localised on vulva. An. Bras. de Dermatol. 2018, 93, 940–941. [Google Scholar] [CrossRef]
- Salah, L.; Ljungberg, O.; Svensson, Å.; Rubin, A. Pseudoangiomatous Xanthelasmoid Mastocytosis—A New Histopathological Entity. J. Eur. Acad. Dermatol. Venereol. 2016, 31, e261–e263. [Google Scholar] [CrossRef]
- Sammut, J.; Mercieca, L.; Boffa, M.M.; Pisani, D.; Betts, A.; Boffa, M.J. Palmoplantar maculopapular cutaneous mastocytosis. Int. J. Dermatol. 2019, 58, E79–E80. [Google Scholar] [CrossRef]
- Vano-Galvan, S.; Alvarez-Twose, I.; De las Heras, E.; Morgado, J.M.; Matito, A.; Sánchez-Muñoz, L.; Plana, M.N.; Jaén, P.; Orfao, A.; Escribano, L. Dermoscopic features of skin lesions in patients with mastocytosis. Arch Dermatol. 2011, 147, 932–940. [Google Scholar] [CrossRef] [Green Version]
- Akay, B.N.; Kittler, H.; Sanlı, H.; Harmankaya, K.; Anadolu, R. Dermatoscopic findings of cutaneous mastocytosis. Dermatology 2008, 218, 226–230. [Google Scholar] [CrossRef]
- Kumar, S.; Jakhar, D.; Misri, R. Dermoscopy of Telangiectasia Macularis Eruptiva Perstans. Indian Dermatol. Online J. 2020, 11, 131–132. [Google Scholar] [PubMed]
- Unterstell, N.; Lavorato, F.G.; Nery, N.S.; Mann, D.; Alves, M.D.F.S.G.; Barcaui, C.B. Dermatoscopic findings in telangiectasia macularis eruptiva perstans. An. Bras. de Dermatol. 2013, 88, 643–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brockow, K.; Ring, J.; Alvarez-Twose, I.; Orfao, A.; Escribano, L. Extensive blistering is a predictor for severe complications in children with mastocytosis. Allergy 2012, 67, 1323–1324. [Google Scholar] [CrossRef] [PubMed]
- Salas-Alanis, J.C.; Rosales-Mendoza, C.E.; Ocampo-Candiani, J. Bullous mastocytosis mimicking congenital epidermolysis bullosa. Case Rep. Dermatol. 2014, 6, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Lange, M.; Niedoszytko, M.; Nedoszytko, B.; Łata, J.; Trzeciak, M.; Biernat, W. Diffuse cutaneus mastocytosis: Analysis of 10 cases and a brief review of the literature. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 1565–1571. [Google Scholar] [PubMed]
- Errichetti, E. Dermoscopy in Monitoring and Predicting Therapeutic Response in General Dermatology (Non-Tumoral Dermatoses): An Up-To-Date Overview. Dermatol. Ther. 2020, 10, 1199–1214. [Google Scholar] [CrossRef] [PubMed]
- Oxford Centre for Evidence-Based Medicine. The Oxford 2011 Levels of Evidence. Available online: http://www.cebm.net/index.aspx?o=5653 (accessed on 3 June 2022).
- Errichetti, E.; Zalaudek, I.; Kittler, H.; Apalla, Z.; Argenziano, G.; Bakos, R.; Blum, A.; Braun, R.; Ioannides, D.; Lacarrubba, F.; et al. Standardization of dermoscopic terminology and basic dermoscopic parameters to evaluate in general dermatology (non-neoplastic dermatoses): An expert consensus on behalf of the International Dermoscopy Society. Br. J. Dermatol. 2019, 182, 454–467. [Google Scholar] [CrossRef]
- Gutiérrez-González, E.; Ginarte, M.; Toribio, J. Letter: Cutaneous mastocytosis with systemic involvement mimicking clinical and dermatoscopically multiple melanocytic nevi. Dermatol. Online J. 2011, 17, 15. [Google Scholar] [CrossRef]
- Miller, M.D.B.; Nery, N.S.; Gripp, A.C.; Maceira, J.P.; Nascimento, G.M.D. Dermatoscopic findings of urticaria pigmentosa. An. Bras. Dermatol. 2013, 88, 986–988. [Google Scholar] [CrossRef] [Green Version]
- Nirmal, B.; Krishnaram, A.S.; Muthu, Y.; Rajagopal, P. Dermatoscopy of Urticaria Pigmentosa with and without Darier’s Sign in Skin of Colour. Indian Dermatol. Online J. 2019, 10, 577–579. [Google Scholar] [CrossRef]
- Chauhan, P.; Bhardway, N.; Shirazi, N. Dermoscopy of Urticaria Pigmentosa. Indian Dermatol. Online J. 2020, 11, 475–476. [Google Scholar] [CrossRef] [PubMed]
- Amorim, R.O.; Enokihara, M.M.S.S.; Ogawa, M.M.; Batista, M.D. Multiple lesions with pigmented network on dermoscopy on a 1-year-old boy. Int. J. Dermatol. 2021, 60, e364–e365. [Google Scholar] [CrossRef] [PubMed]
- Adya, K.A.; Inamadar, A.C.; Palit, A. Dermoscopy of Cutaneous Mastocytoma. Indian Dermatol. Online J. 2018, 9, 218–219. [Google Scholar] [PubMed]
- Gündüz, Ö.; Yildirim, D.; Erdoğan, F.G.; Kaya, B.; Doğan, H. Solitary Bullous Mastocytoma with Dermoscopic Features in a Neonate. Dermatol. Pract. Concept. 2019, 9, 302–303. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Kansal, N.K.; Anuragi, R.P. Cutaneous mastocytosis: Clinical, dermoscopic and pathological features. BMJ Case Rep. 2020, 13, e24016. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S.; Neema, S.; Sinha, P.; Sandhu, S.; Kashif, A.W.; Radhakrishnan, S. Dermoscopic Demonstration of Darier Sign. Dermatol. Pract. Concept. 2021, 11, e2021114. [Google Scholar] [CrossRef]
- Grattan, C.E.H.; Radia, D.H. Mastocytosis. In Rook’s Textbook of Dermatology, 9th ed.; Griffiths, C.E.M., Barker, J., Bleiker, T., Chalmers, R., Creamer, D., Eds.; Wiley-Blackwell: Oxford, UK, 2016; Volume 46, pp. 1–10. [Google Scholar]
- Bañuls, J.; Arribas, P.; Berbegal, L.; DeLeón, F.J.; Francés, L.; Zaballos, P. Yellow and orange in cutaneous lesions: Clinical and dermoscopic data. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 2317–2325. [Google Scholar] [CrossRef]
- Vázquez-López, F.; Fueyo, A.; Sánchez-Martín, J.; Pérez-Oliva, N. Dermoscopy for the Screening of Common Urticaria and Urticaria Vasculitis. Arch. Dermatol. 2008, 144, 568. [Google Scholar] [CrossRef]
- Suh, K.; Kang, D.; Lee, K.; Han, S.; Park, J.; Kim, S.; Jang, M. Evolution of urticarial vasculitis: A clinical, dermoscopic and histopathological study. J. Eur. Acad. Dermatol. Venereol. 2013, 28, 674–675. [Google Scholar] [CrossRef]
- Peruilh-Bagolini, L.; Silva-Astorga, M.; Martín, M.J.H.S.; Manoli, M.-S.; Papageorgiou, C.; Apalla, Z.; Lallas, A. Dermoscopy of Juvenile Xanthogranuloma. Dermatology 2020, 237, 946–951. [Google Scholar] [CrossRef]
- Di Brizzi, E.V.; Moscarella, E.; Scharf, C.; Argenziano, G.; Piccolo, V. Dermoscopy of juvenile xanthogranuloma: A retrospective descriptive study on 35 paediatric patients. J. Eur. Acad Dermatol. Venereol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Palmer, A.; Bowling, J. Dermoscopic appearance of juvenile xanthogranuloma. Dermatology 2007, 215, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Zalaudek, I.; Argenziano, G.; Di Stefani, A.; Ferrara, G.; Marghoob, A.A.; Hofmann-Wellenhof, R.; Soyer, H.P.; Braun, R.; Kerl, H. Dermoscopy in general dermatology. Dermatology 2006, 212, 7–18. [Google Scholar] [CrossRef]
- Errichetti, E.; Stinco, G. Dermatoscopy in general dermatology: A practical overview. Dermatol. Ther. 2016, 6, 471–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosseila, M.; Sonthalia, S.; Agrawal, M.; Bhatia, J.; Zeeshan, M.; Elsamanoudy, S.; Tiwary, P.; Bhat, Y.J.; Jha, A. Entodermoscopy update: A contemporary review on dermoscopy of cutaneous infections and infestations. Indian Dermatol. Online J. 2021, 12, 220–236. [Google Scholar]
- Chauhan, P.; Jindal, R.; Errichetti, E. Dermoscopy of skin parasitoses, bites and stings: A systematic review of the literature. J. Eur. Acad. Dermatol. Venereol. 2022. [Google Scholar] [CrossRef]
- Brazel, M.; Desai, A.; Are, A.; Motaparthi, K. Staphylococcal Scalded Skin Syndrome and Bullous Impetigo. Medicina 2021, 57, 1157. [Google Scholar] [CrossRef]
- Guida, S.; Longhitano, S.; Ardigò, M.; Pampena, R.; Bs, S.C.; Bigi, L.; Mandel, V.D.; Msc, C.V.; Manfredini, M.; Pezzini, C.; et al. Dermoscopy, confocal microscopy and optical coherence tomography features of main inflammatory and autoimmune skin diseases: A systematic review. Australas. J. Dermatol. 2021, 63, 15–26. [Google Scholar] [CrossRef]
- Narkhede, N.D.; Nikham, B.; Jamale, V.; Hussain, A.; Kale, M. Evaluation of Dermoscopic Patterns of Vesiculobullous Disorders. Indian J. Dermatol. 2021, 66, 445. [Google Scholar]
- Errichetti, E.; Stinco, G. Dermatoscopy in life-threatening and severe acute rashes. Clin. Dermatol. 2019, 38, 113–121. [Google Scholar] [CrossRef]
- Miyashita, K.; Ogawa, K.; Iioka, H.; Miyagawa, F.; Okazaki, A.; Kobayashi, N.; Asada, H. Adult case of staphylococcalscalded skin syndrome differentiated from toxic epidermal necrolysis withthe aid of dermatoscopy. J. Dermatol. 2016, 43, 842–843. [Google Scholar] [CrossRef] [PubMed]
- Amatya, B. Evaluation of Dermoscopic Features in Facial Melanosis with Wood Lamp Examination. Dermatol. Pract. Concept. 2022, 12, e2022030. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Manifestation of CM | First Author, Journal, Year | Dermoscopic Features per Diagnosis (Number/%) | Corresponding Terminology Based on International Dermoscopy Society Consensus Document | Dermoscopic-Histopathological Correlation Discussed in the Article | Type of Dermoscope/Magnification | Polarisation/Immersion | Study Design | Number of Cases of Specific Mastocytosis Subtype | Level of Evidence | Aspects Important for Clinical Practice |
|---|---|---|---|---|---|---|---|---|---|---|
| Maculopapular CM (MPCM) urticaria pigmentosa clinical subtype | Akay, Dermatology, 2008 [10] | brown reticular lines | brown lines arranged in a network-like structure | basal hyperpigmentation and increase in mast cells in the dermis | DermLite II Pro HR 3Gen/NR | NR/NR | case series | 3 | V | brown reticular lines seen on dermoscopy may be present also in melanocytic lesion, dermatofibroma, solar lentigo, ink-spot lentigo, seborrheic keratosis, accessory nipple |
| Vano-Galvan, Arch Dermatol, 2011 [9] | light-brown blot (43/90;47.8%); pigment network (36/90; 40.0%); vascular pattern (11/90; 12.2%) | brown structureless areas; brown lines arranged in a network-like structure; linear vessels arranged in a reticular pattern; dotted vessels | hyperpigmentation of basal layer (mild and homogenous); mast cells in the dermis; hyperpigmentation of the basal layer (marked on the rete ridges); mast cells in the dermis; blood vessel dilatation | DermLite 3Gen/×10 | NR/NR | case series | 90 | V | vascular pattern was an independent predictive factor for the need for daily anti-mediator therapy | |
| Gutiérrez-González, Dermatol Online J, 2011 [19] | brown reticular lines | brown lines arranged in a network-like structure | increase in melanocytes and melanin deposits in the basal layer, mast cells in the dermis | NR/NR | NR/NR | case report | 1 | V | papules dermoscopically mimicked melanocytic nevi | |
| Miller, An Bras Dermatol, 2013 [20] | pigment network, light-brownish blot | brown lines arranged in a network-like structure, brown structureless areas | basal cell layer hyperpigmentation, mast cells and lymphocytes in dermis | NR/×10 | NR/NR | case report | 1 | V | ||
| Nirmal, Indian Dermatol Online J, 2019 [21] | brown reticular lines | brown lines arranged in a network-like structure | basal cell layer hyperpigmentation; mast cells in dermis | DermLite DL3,3Gen/×10 | polarised/NR | case series | 2 | V | brownish lines seen on dermoscopy were darker in case of mastocytosis with positive Darier sign | |
| Chauhan, Indian Dermatol Online J, 2020 [22] | brown reticular lines, reddish background | brown lines arranged in a network-like structure - | basal cell layer hyperpigmentation, mild epidermal spongiosis, increase in mast cells and lymphocytes in dermis | DermLite II hybrid m; 3Gen/×10 | polarised/NR | case report | 1 | V | reddish background was suggested by the authors as a feature helpful in differentiation between mastocytosis and melanocytic nevi | |
| Amorim, Int J Dermatol, 2021 [23] | reticular lines (pigmented network) | brown lines arranged in a network-like structure | mastocytes on superficial dermis | NR/NR | NR/NR | case report | 1 | V | ||
| MPCM telangiectasia macularis eruptiva perstans clinical subtype | Akay, Dermatology, 2008 [10] | thin reticular telangiectasias (3/3); erythematous background (2/3); brown reticular lines (1/3) | linear vessels arranged in a reticular pattern - brown lines arranged in a network-like structure | dilated dermal vessels; mast cells in superficial dermis; NR | DermLite II Pro HR 3Gen/NR | NR/NR | case series | 3 | V | reticular vascular pattern may be helpful in differentiation between TMEP and other eruptions |
| Vano-Galvan, Arch Dermatol, 2011 [9] | reticular vascular pattern (7/7; 100%) | linear vessels arranged in a reticular pattern | dilation of the blood vessels | DermLite 3Gen/×10 | NR/NR | case series | 7 | V | ||
| Unterstell, An Bras Dermatol, 2013 [12] | thin and tortuous linear vessels, mild erythema, fine pigment network | linear-curved vessels - brown lines arranged in a network-like structure | dilatation and vascular proliferation associated with the presence of mast cells in the dermis, NR | NR/NR | NR/NR | case report | 1 | V | ||
| Kumar, Indian Dermatol Online J, 2019 [11] | reticular vascular pattern of linear and branching vessels, brownish background | linear vessels and linear vessels with branches in a reticular distribution, brown structureless areas | dilated superficial capillaries surrounded by mast cells in the papillary dermis; NR | Dino Lite AM413ZT Digital Microscope/×50 | polarised/NR | case report | 1 | V | at higher magnification (200×), branching vessels encircled the eccrine glands (visible as white dots) | |
| MPCM telangiectasia macularis eruptiva perstans clinical subtype—limited to acral areas | Sammut, Int J Dermatol, 2019 [8] | reticular vascular pattern | linear vessels arranged in a reticular pattern | prominent ectatic blood vessels in the upper and mid dermis | NR/NR | NR/NR | case report | 1 | V | |
| Mastocytoma | Vano-Galvan, Arch Dermatol, 2011 [9] | yellow-orange blot (11/11; 100%) | yellow-orange structureless areas | dense infiltration of mast cells along the papillary and reticular dermis | DermLite 3Gen/×10 | NR/NR | case series | 11 | V | in differential diagnosis of lesions presenting with yellow-orange structureless pattern on dermoscopy consider: juvenile/adult xanthogranuloma, sebaceous hyperplasia, reticulohistiocytoma, xanthomatous dermatofibroma |
| Adya, Indian Dermatol Online J, 2018 [24] | central white structureless area, yellow background, peripheral brown reticular lines | central white structureless area, diffuse yellow structureless area, brown lines arranged in a network-like structure | accumulation of serosanguineous fluid produced due to excoriation of the epidermis in the centre of the lesion, diffuse mononuclear cell infiltrate involving the dermis extending into and expanding the dermal papillae, increased melanisation of the basal layer | DermLite DL3/×10 | polarised/NR | case report | 1 | V | dermoscopy is helpful in differentiation with juvenile xanthogranuloma | |
| Gündüz, Dermatol Pract Concept, 2019 [25] | central vascular structures * peripheral yellow structureless area | - peripheral yellow structureless area | central vascular structure might reflect the detachment of epidermis due to the bullous reaction, dense mast cell infiltration in dermis | NR/×10 | NR/NR | case report | 1 | V | ||
| Kumar, BMJ Case Reports, 2020 [26] | central whitish area, reticulate light brown rim, yellowish background | central white structureless area, brown lines arranged in a network-like structure, diffuse yellow structureless area | NR, basal layer melanisation, diffuse infiltration of the superficial epidermis by mastocytes | NR/NR | NR/NR | case report | 1 | V | ||
| Mukherje, Dermatol Pract Concept, 2021 [27] | pigment network, yellow background | brown lines arranged in a network-like structure, diffuse yellow structureless area | basal layer hyperpigmentation, mast cells in dermis | DermLite DL4/×10 | polarised/NR | case report | 1 | V | provocation of Darier sign on dermoscopy shows decrease in yellow colour and pigment network intensity with appearance of peripheral erythema | |
| Other clinical forms Plaque-type mastocytosis | Vano-Galvan, Arch Dermatol, 2011 [9] | light-brown blot (5/8; 62.5%); pigment network (3/18; 37.5%) | brown structureless areas; brown lines arranged in a network-like structure | hyperpigmentation of basal layer (mild and homogenous), mast cells in the dermis; hyperpigmentation of the basal layer (marked on the rete ridges), mast cells in the dermis | DermLite 3Gen/×10 | NR/NR | case series | 8 | V | |
| Other clinical forms Nodular mastocytosis | Vano-Galvan, Arch Dermatol, 2011 [9] | light-brown blot (3/11; 27.3%); pigment network (5/11; 45.5%); yellow-orange blot (6/11; 54.6%) | brown structureless areas; brown lines arranged in a network-like structure; yellow-orange structureless areas | hyperpigmentation of basal layer (mild and homogenous), mast cells in the dermis; hyperpigmentation of the basal layer (marked on the rete ridges), mast cells in the dermis; dense infiltration of mast cells along the papillary and reticular dermis | DermLite 3Gen/×10 | NR/NR | case series | 11 | V | |
| Other clinical forms Pseudoangiomatous xanthelasmoid mastocytosis | Salah, J Eur Acad Dermatol, 2016 [7] | brown reticular pattern, yellow blots | brown lines arranged in a network-like structure. yellow structureless areas | patchy basal hyperpigmentation, mast cells in dermis | NR/NR | NR/NR | case report | 1 | V | main clinical differential diagnoses: xanthoma, vascular tumour/malformation, xanthogranuloma |
| Other clinical forms Pseudoxanthomatous localised mastocytosis | Li, An Bras Dermatol, 2018 [6] | pigmented stripes radiating from hair follicles, pink background, linear branched vessels, reticular vessels | specific clue, - linear vessels with branches, linear vessels arranged in a reticular pattern | hyperpigmentation of keratinocytes in the basal layer, dense infiltration of mast cells, NR, NR | NR/NR | NR/NR | case report | 1 | V | vulva may be predilection site for localised cases; clinical differential diagnoses include pseudoxanthoma elasticum, juvenile xanthogranuloma, xanthoma; pigmented lines arranged radially around hair follicles may be a specific feature |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sławińska, M.; Kaszuba, A.; Lange, M.; Nowicki, R.J.; Sobjanek, M.; Errichetti, E. Dermoscopic Features of Different Forms of Cutaneous Mastocytosis: A Systematic Review. J. Clin. Med. 2022, 11, 4649. https://doi.org/10.3390/jcm11164649
Sławińska M, Kaszuba A, Lange M, Nowicki RJ, Sobjanek M, Errichetti E. Dermoscopic Features of Different Forms of Cutaneous Mastocytosis: A Systematic Review. Journal of Clinical Medicine. 2022; 11(16):4649. https://doi.org/10.3390/jcm11164649
Chicago/Turabian StyleSławińska, Martyna, Agnieszka Kaszuba, Magdalena Lange, Roman J. Nowicki, Michał Sobjanek, and Enzo Errichetti. 2022. "Dermoscopic Features of Different Forms of Cutaneous Mastocytosis: A Systematic Review" Journal of Clinical Medicine 11, no. 16: 4649. https://doi.org/10.3390/jcm11164649
APA StyleSławińska, M., Kaszuba, A., Lange, M., Nowicki, R. J., Sobjanek, M., & Errichetti, E. (2022). Dermoscopic Features of Different Forms of Cutaneous Mastocytosis: A Systematic Review. Journal of Clinical Medicine, 11(16), 4649. https://doi.org/10.3390/jcm11164649