
Predictive Markers of Crohn’s Disease in Small Bowel Capsule Endoscopy: A Retrospective Study of Small Bowel Capsule Endoscopy

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. SBCE Procedure
2.3. Data Collection
2.4. Statistical Methods
3. Results
3.1. Patient Characteristics
3.2. Prior Lower Endoscopy
3.3. Capsule Retention
3.4. Prior Imaging
3.5. Laboratory Findings
3.6. Multivariate Analysis
3.7. CECDAI-Score
3.8. Follow-Up
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- de Ridder, L.; Mensink, P.B.; Lequin, M.H.; Aktas, H.; de Krijger, R.R.; van der Woude, C.J.; Escher, J.C. Single-balloon enteroscopy, magnetic resonance enterography, and abdominal US useful for evaluation of small-bowel disease in children with (suspected) Crohn’s disease. Gastrointest. Endosc. 2012, 75, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Aaltonen, G.; Keränen, I.; Carpelan-Holmström, M.; Savolainen, R.; Lindén, R.; Lepistö, A. Intra-Abdominal Adhesions Make the Interpretation of Magnetic Resonance Enterography in Crohn’s Disease More Difficult. Dig. Surg. 2017, 34, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Kaushal, P.; Somwaru, A.S.; Charabaty, A.; Levy, A.D. MR Enterography of Inflammatory Bowel Disease with Endoscopic Correlation. RadioGraphics 2017, 37, 116–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costamagna, G.; Shah, S.K.; Riccioni, M.E.; Foschia, F.; Mutignani, M.; Perri, V.; Vecchioli, A.; Brizi, M.G.; Picciocchi, A.; Marano, P. A prospective trial comparing small bowel radiographs and video capsule endoscopy for suspected small bowel disease. Gastroenterology 2002, 123, 999–1005. [Google Scholar] [CrossRef]
- Papanikolaou, N.; Prassopoulos, P.; Eracleous, E.; Maris, T.; Gogas, C.; Gourtsoyiannis, N. Contrast-Enhanced Magnetic Resonance Cholangiography Versus Heavily T2-Weighted Magnetic Resonance Cholangiography. Investig. Radiol. 2001, 36, 682–686. [Google Scholar] [CrossRef]
- Kovanlikaya, A.; Watson, E.; Hayward, J.; Beneck, D.; Sockolow, R.; Solomon, A.; Christos, P.; Brill, P.W. Magnetic resonance enterography and wireless capsule endoscopy in the evaluation of patients with inflammatory bowel disease. Clin. Imaging 2013, 37, 77–82. [Google Scholar] [CrossRef] [Green Version]
- González-Suárez, B.; Rodriguez, S.; Ricart, E.; Ordás, I.; Rimola, J.; Díaz-González, Á.; Romero, C.; de Miguel, C.R.; Jáuregui, A.; Araujo, I.K.; et al. Comparison of Capsule Endoscopy and Magnetic Resonance Enterography for the Assessment of Small Bowel Lesions in Crohn’s Disease. Inflamm. Bowel Dis. 2018, 24, 775–780. [Google Scholar] [CrossRef]
- Gomollón, F.; Dignass, A.; Annese, V.; Tilg, H.; Van Assche, G.; Lindsay, J.O.; Peyrin-Biroulet, L.; Cullen, G.J.; Daperno, M.; Kucharzik, T.; et al. 3rd European Evidence-based Consensus on the Diagnosis and Management of Crohn’s Disease 2016: Part 1: Diagnosis and Medical Management. J. Crohn’s Colitis 2017, 11, 3–25. [Google Scholar] [CrossRef] [Green Version]
- Dionisio, P.M.; Gurudu, S.R.; Leighton, J.A.; Leontiadis, G.I.; Fleischer, D.E.; Hara, A.K.; Heigh, R.I.; Shiff, A.D.; Sharma, V.K. Capsule endoscopy has a significantly higher diagnostic yield in patients with suspected and established small-bowel Crohn’s disease: A meta-analysis. Am. J. Gastroenterol. 2010, 105, 1240–1248. [Google Scholar] [CrossRef]
- Kopylov, U.; Yung, D.E.; Engel, T.; Vijayan, S.; Har-Noy, O.; Katz, L.; Oliva, S.; Avni, T.; Battat, R.; Eliakim, R.; et al. Diagnostic yield of capsule endoscopy versus magnetic resonance enterography and small bowel contrast ultrasound in the evaluation of small bowel Crohn’s disease: Systematic review and meta-analysis. Dig. Liver Dis. 2017, 49, 854–863. [Google Scholar] [CrossRef] [Green Version]
- Liao, Z.; Gao, R.; Xu, C.; Li, Z.-S. Indications and detection, completion, and retention rates of small-bowel capsule endoscopy: A systematic review. Gastrointest. Endosc. 2010, 71, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Hosoe, N.; Takabayashi, K.; Ogata, H.; Kanai, T. Capsule endoscopy for small-intestinal disorders: Current status. Dig. Endosc. 2019, 31, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Vernia, F.; Di Ruscio, M.; Stefanelli, G.; Viscido, A.; Frieri, G.; Latella, G. Is fecal calprotectin an accurate marker in the management of Crohn’s disease? J. Gastroenterol. Hepatol. 2020, 35, 390–400. [Google Scholar] [CrossRef]
- Sipponen, T.; Haapamäki, J.; Savilahti, E.; Alfthan, H.; Hämäläinen, E.; Rautiainen, H.; Koskenpato, J.; Nuutinen, H.; Färkkilä, M. Fecal calprotectin and S100A12 have low utility in prediction of small bowel Crohn’s disease detected by wireless capsule endoscopy. Scand J. Gastroenterol. 2012, 47, 778–784. [Google Scholar] [CrossRef]
- Kopylov, U.; Yung, D.E.; Engel, T.; Avni, T.; Battat, R.; Ben-Horin, S.; Plevris, J.N.; Eliakim, R.; Koulaouzidis, A. Fecal calprotectin for the prediction of small-bowel Crohn’s disease by capsule endoscopy: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2016, 28, 1137–1144. [Google Scholar] [CrossRef] [PubMed]
- Koulaouzidis, A.; Sipponen, T.; Nemeth, A.; Makins, R.; Kopylov, U.; Nadler, M.; Giannakou, A.; Yung, D.E.; Johansson, G.W.; Bartzis, L.; et al. Association Between Fecal Calprotectin Levels and Small-bowel Inflammation Score in Capsule Endoscopy: A Multicenter Retrospective Study. Am. J. Dig. Dis. 2016, 61, 2033–2040. [Google Scholar] [CrossRef]
- Niv, Y.; Ilani, S.; Levi, Z.; Hershkowitz, M.; Niv, E.; Fireman, Z.; O’Donnel, S.; O’Morain, C.; Eliakim, R.; Scapa, E.; et al. Validation of the Capsule Endoscopy Crohn’s Disease Activity Index (CECDAI or Niv score): A multicenter prospective study. Endoscopy 2012, 44, 21–26. [Google Scholar] [CrossRef]
- Gal, E.; Geller, A.; Fraser, G.; Levi, Z.; Niv, Y. Assessment and Validation of the New Capsule Endoscopy Crohn’s Disease Activity Index (CECDAI). Am. J. Dig. Dis. 2008, 53, 1933–1937. [Google Scholar] [CrossRef]
- Rosa, B.; Pinho, R.; de Ferro, S.M.; Almeida, N.; Cotter, J.; Saraiva, M.M. Endoscopic Scores for Evaluation of Crohn’s Disease Activity at Small Bowel Capsule Endoscopy: General Principles and Current Applications. GE Port J. Gastroenterol. 2016, 23, 36–41. [Google Scholar] [CrossRef] [Green Version]
- Koulaouzidis, A.; Douglas, S.; Plevris, J.N. Lewis Score Correlates More Closely with Fecal Calprotectin Than Capsule Endoscopy Crohn’s Disease Activity Index. Am. J. Dig. Dis. 2012, 57, 987–993. [Google Scholar] [CrossRef]
- Valenzuela, J.E.; López, A.P.; Fernández, V.P.; Parras, F.A.D.L.; Álvarez, F.C. Fecal calprotectin and C-reactive protein are associated with positive findings in capsule endoscopy in suspected small bowel Crohn?s disease. Rev. Esp. Enferm. Dig. 2016, 108, 394–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bar-Gil Shitrit, A.; Koslowsky, B.; Livovsky, D.M.; Shitrit, D.; Paz, K.; Adar, T.; Adler, S.N.; Goldin, E. A prospective study of fecal calprotectin and lactoferrin as predictors of small bowel Crohn’s disease in patients undergoing capsule endoscopy. Scand. J. Gastroenterol. 2017, 52, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Rustgi, S.D.; Kayal, M.; Shah, S.C. Sex-based differences in inflammatory bowel diseases: A review. Ther. Adv. Gastroenterol. 2020, 13, 1756284820915043. [Google Scholar] [CrossRef] [PubMed]
- Omori, T.; Matsumoto, T.; Hara, T.; Kambayashi, H.; Murasugi, S.; Ito, A.; Yonezawa, M.; Nakamura, S.; Tokushige, K. A Novel Capsule Endoscopic Score for Crohn’s Disease. Crohn’s Colitis 360 2020, 2, otaa040. [Google Scholar] [CrossRef]
- Pasha, S.F.; Pennazio, M.; Rondonotti, E.; Wolf, D.; Buras, M.; Albert, J.G.; Cohen, S.A.; Cotter, J.; D’Haens, G.; Eliakim, R.; et al. Capsule Retention in Crohn’s Disease: A Meta-analysis. Inflamm. Bowel Dis. 2020, 26, 33–42. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Patients (N = 374) | CD Group (N = 110) | Non-CD Group (N = 264) | p-Value | |
|---|---|---|---|---|
| Characteristic | No. (%) | No. (%) | No. (%) | |
| Age | ||||
| Mean (Y) | 40.78 | 40.47 | 40.91 | 0.69 |
| 95% CI (Y) | 39.07–42.49 | 37.15–43.79 | 38.91–42.92 | |
| STD (Y) | 16.83 | |||
| Median [Q1:Q3] (Y) | 37.28 [27.06:53.41] | 36.12 [26.37:52.45] | 38.05 [27.41:53.86] | |
| Age (min-max) (Y) | 3.92–87.34 | 10.85–79.47 | 3.92–87.34 | |
| Gender | ||||
| Male | 158/374 (42.2) | 54/110 (49.1) | 104/264 (39.4) | 0.086 |
| Female | 216/374 (57.8) | 56/110 (50.1) | 160/264 (60.1) | 0.086 |
| NSAID | ||||
| NSAID use | 81/313 (22.5) | 22/109 (20.18) | 59/251 (23.51) | 0.58 |
| Smoking status | ||||
| Smokers | 71/313 (22.68) | 21/102 (20.59) | 50/211 (23.7) | 0.39 |
| Ex-smokers | 38/313 (12.14) | 16/102 (15.69) | 22/211 (10.43) | |
| Never smoked | 204/313 (65.18) | 65/102 (63.73) | 139/211 (65.88) |
| All Patients (N = 374) | CD Group (N = 110) | Non-CD Group (N = 264) | |
|---|---|---|---|
| Finding | No. (%) | No. (%) | No. (%) |
| Colonoscopy | |||
| Data available | 366/374 (97.86) | 109/110 (99.09) | 257/264 (97.34) |
| Ileum intubated | 342/366 (93.4) | 104/109 (95.41) | 238/257 (92.61) |
| Ileitis | 131/342 (38.3) | 73/104 (70.91) | 58/238 (24.37) |
| Normal pathology in ileal biopsy | 223/321 (69.5) | 49/102 (48.04) | 174/219 (79.45) |
| Nonspecific inflammation in ileal biopsy | 94/321 (29.3) | 50/102 (49.02) | 44/219 (20.09) |
| Granulomas in ileal biopsy | 4/321 (1.2) | 3/102 (2.94) | 1/219 (0.46) |
| Imaging | |||
| Imaging of small bowel performed | 281/374 (75.1) | 89/110 (80.91) | 192/264 (72.73) |
| Magnetic resonance enterography | 224/374 (59.9) | 76/110 (69.09) | 148/264 (56.06) |
| Computed tomography | 57/374 (15.2) | 13/110 (11.82) | 44/264 (16.67) |
| Normal findings | 180/281 (64.1) | 41/89 (46.07) | 139/192 (72.4) |
| Suspected inflammation | 66/281 (23.5) | 26/89 (29.21) | 40/192 (20.83) |
| Active inflammation | 35/281 (12.5) | 22/89 (24.72) | 13/192 (6.77) |
| Capsule retention | |||
| Capsule retention rate | 6/374 (1.6) | 3/110 (2.73) | 3/264 (1.14) |
| All Patients (N = 374) | CD Group (N = 110) | Non-CD Group (N = 264) | p-Value | |
|---|---|---|---|---|
| Laboratory Finding | No. (%) | No. (%) | No. (%) | |
| C-reactive protein | ||||
| Data available | 263/374 (70.6) | 77/110 (70.0) | 186/264 (70.5) | |
| Mean (mg/L) [95%Cl] | 8.11 [5.9–10.3] | 10.08 [5.4–14.7] | 7.29 [4.9–9.7] | 0.24 |
| STD | 17.84 | |||
| Median [Q1:Q3] | 2 [1:8] | 3 [1:9] | 2 [1:8] | |
| [Min–max] | [1–131] | [1–131] | [1–122] | |
| Hemoglobin | ||||
| Data available | 365/374 (97.6) | 109/110 (99.0) | 256/264 (97.0) | |
| Mean (g/L) [95%Cl] | 138.3 [136.8–139.9] | 138.32 [135.5–141.1] | 138.3 [136.4–140.2] | 0.59 |
| STD | 15.18 | |||
| Median [Q1:Q3] | 139 [130:149] | 138 [127:149] | 139 [131:148] | |
| [Min–max] | [87–183] | [103–183] | [87–177] | |
| Erythrocyte sedimentation rate | ||||
| Data available | 121/374 (32.4) | 43/110 (39.1) | 78/264 (29.5) | |
| Mean (mm/h) [95%Cl] | 11.23 [9.14–13.33] | 13.67 [10.05–17.30] | 9.88 [7.31–12.45] | 0.022 |
| STD | 11.63 | |||
| Median [Q1:Q3] | 7 [2.00:14] | 9 [5:20] | 6 [2:12] | |
| [Min–max] | [1–54] | [2–48] | [1–54] | |
| Serum albumin | ||||
| Data available | 162/374 (43.3) | 72/110 (65.5) | 140/264 (53.0) | |
| Mean (g/L) [95%Cl] | 38.21 [37.68–38.74] | 37.58 [36.62–38.54] | 38.35 [37.89–39.17] | 0.025 |
| STD | 3.93 | |||
| Median [Q1:Q3] | 38.75 [36.35:40.40] | 38.1 [35.6:40.1] | 39.4 [37.2:40.6] | |
| [Min–max] | [12–46.8] | [18.7–46.8] | [15–45.3] | |
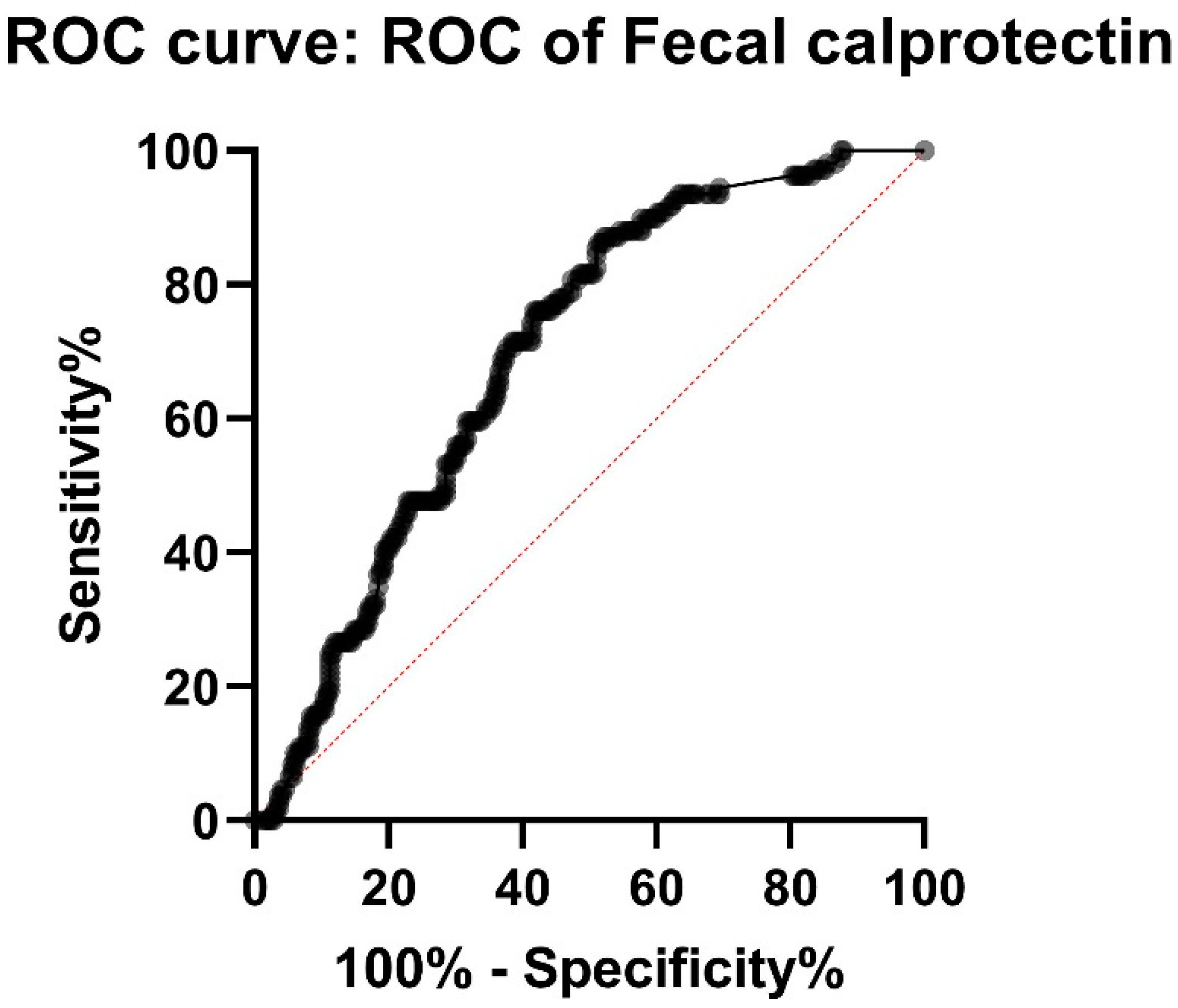
| Fecal calprotectin | ||||
| Data available | 358/374 (95.7) | 109 (99.1) | 249/264 (94.3) | |
| Mean (ug/g) [95%Cl] | 506.34 [415.38–597.30] | 625.85 [496.61:755.30] | 453.98 [336.15–571.81] | <0.001 |
| STD | 875.1 | |||
| Median [Q1:Q3] | 207 [57:527] | 354 [195:802] | 132 [50:413] | |
| [Min–max] | [20–6000] | [22–3165] | [20–6000] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mattila, J.; Stenholm, T.; Löyttyniemi, E.; Koffert, J. Predictive Markers of Crohn’s Disease in Small Bowel Capsule Endoscopy: A Retrospective Study of Small Bowel Capsule Endoscopy. J. Clin. Med. 2022, 11, 4635. https://doi.org/10.3390/jcm11154635
Mattila J, Stenholm T, Löyttyniemi E, Koffert J. Predictive Markers of Crohn’s Disease in Small Bowel Capsule Endoscopy: A Retrospective Study of Small Bowel Capsule Endoscopy. Journal of Clinical Medicine. 2022; 11(15):4635. https://doi.org/10.3390/jcm11154635
Chicago/Turabian StyleMattila, Juho, Teppo Stenholm, Eliisa Löyttyniemi, and Jukka Koffert. 2022. "Predictive Markers of Crohn’s Disease in Small Bowel Capsule Endoscopy: A Retrospective Study of Small Bowel Capsule Endoscopy" Journal of Clinical Medicine 11, no. 15: 4635. https://doi.org/10.3390/jcm11154635
APA StyleMattila, J., Stenholm, T., Löyttyniemi, E., & Koffert, J. (2022). Predictive Markers of Crohn’s Disease in Small Bowel Capsule Endoscopy: A Retrospective Study of Small Bowel Capsule Endoscopy. Journal of Clinical Medicine, 11(15), 4635. https://doi.org/10.3390/jcm11154635