
Efficacy and Safety of JAK Inhibitors for Rheumatoid Arthritis: A Meta-Analysis


Abstract
:1. Introduction
2. Methods
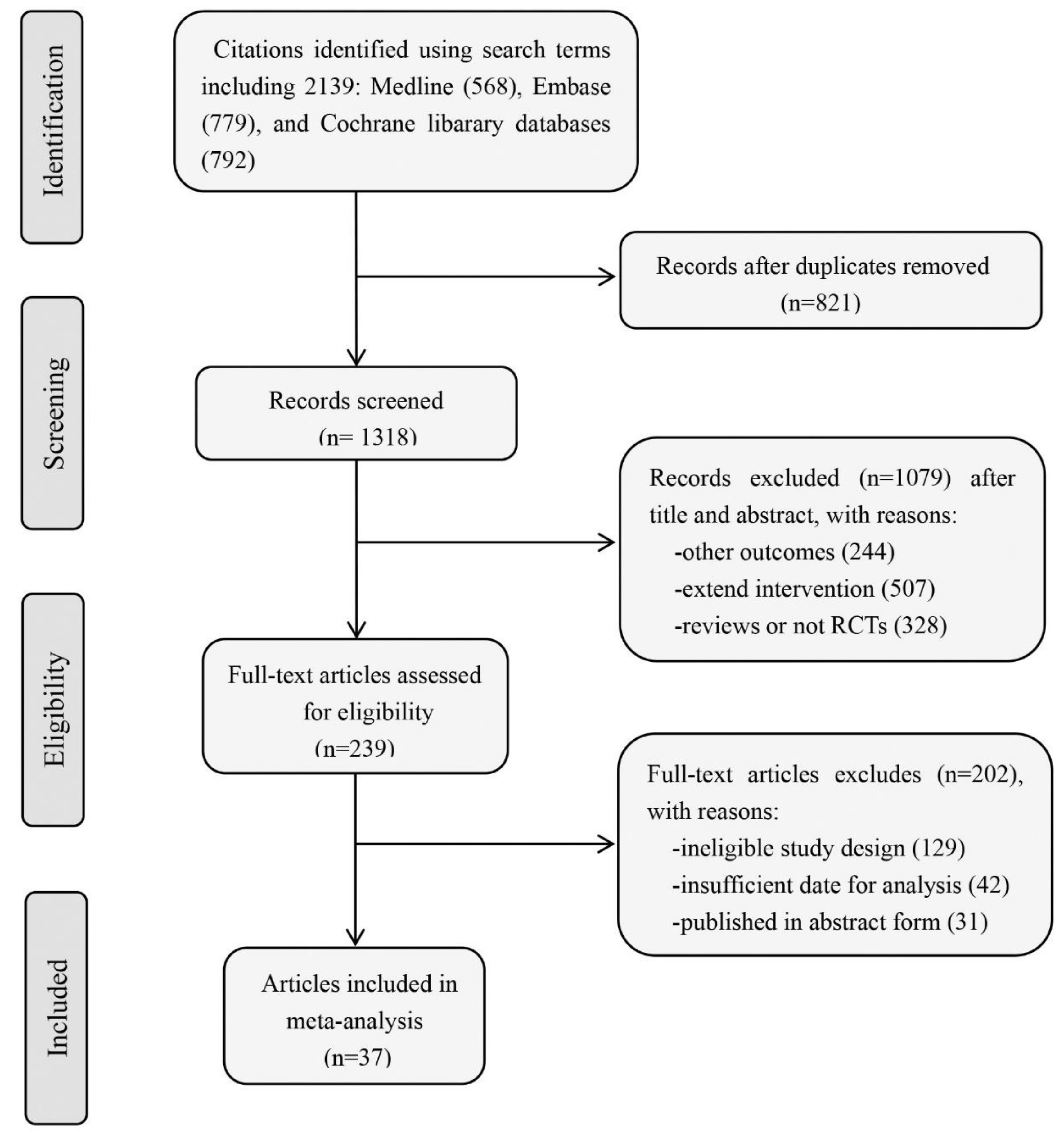
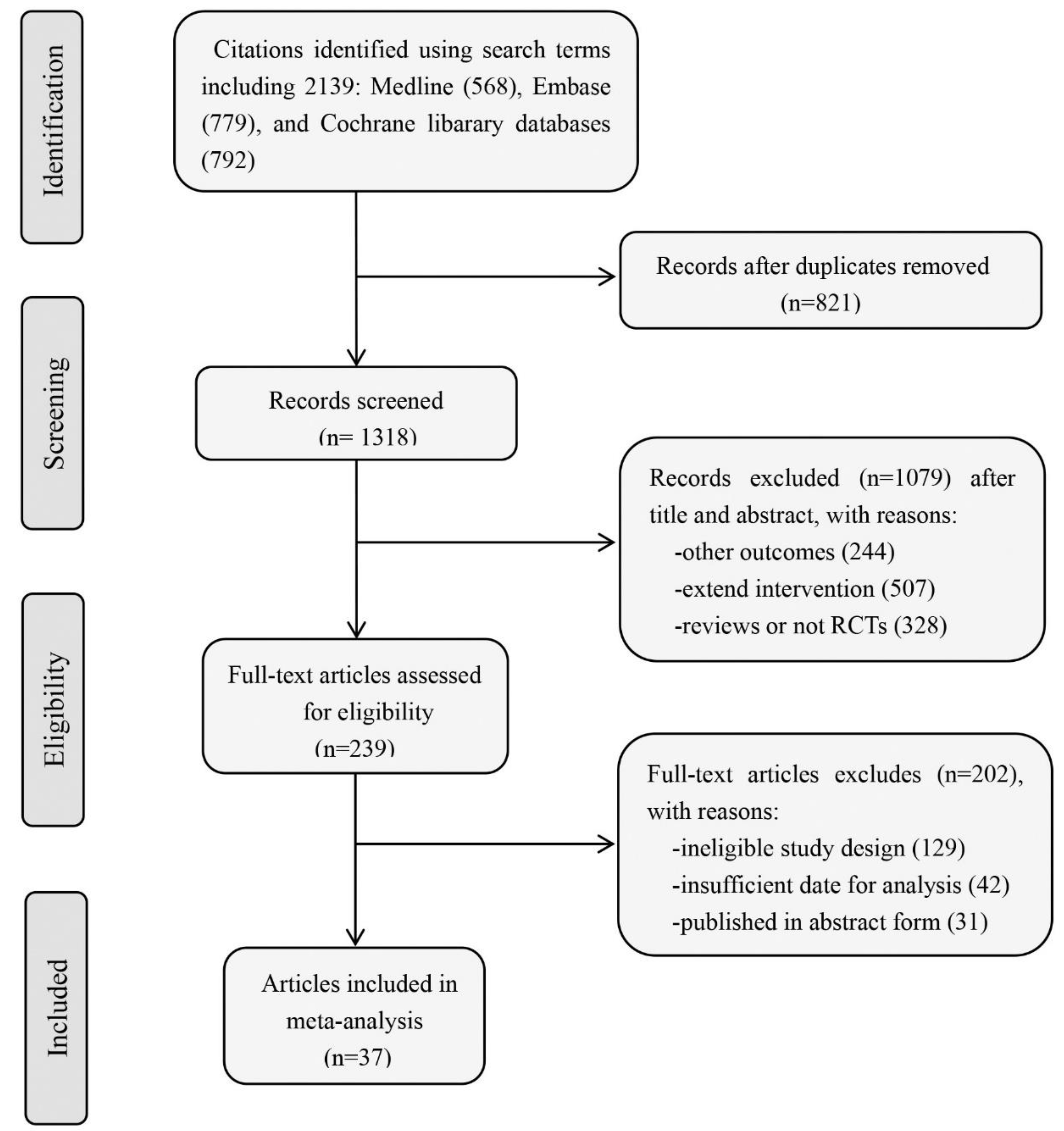
2.1. Literature Searches and Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Outcome Measures
2.4. Statistical Analyses
3. Results
3.1. Study Characteristics
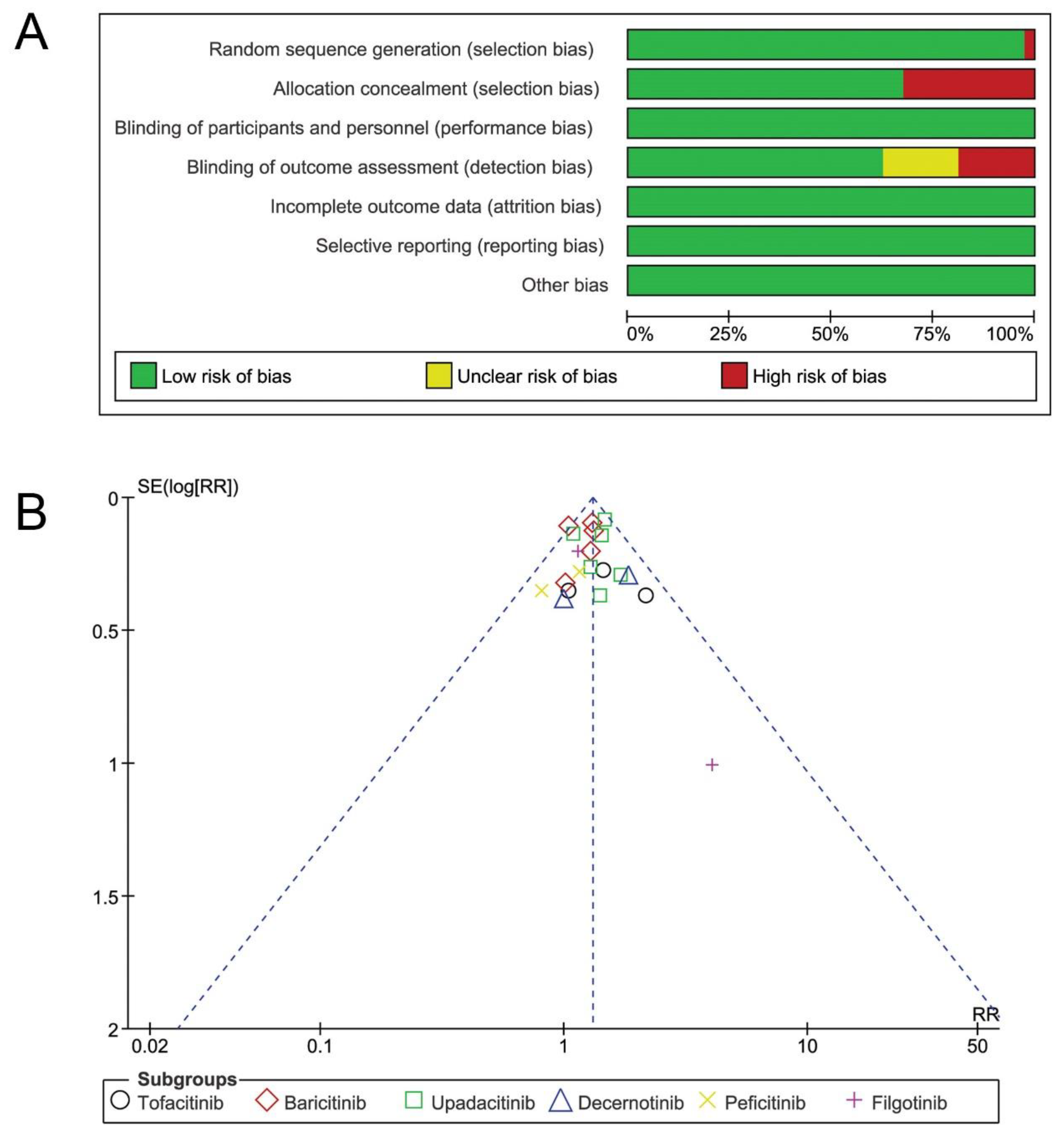
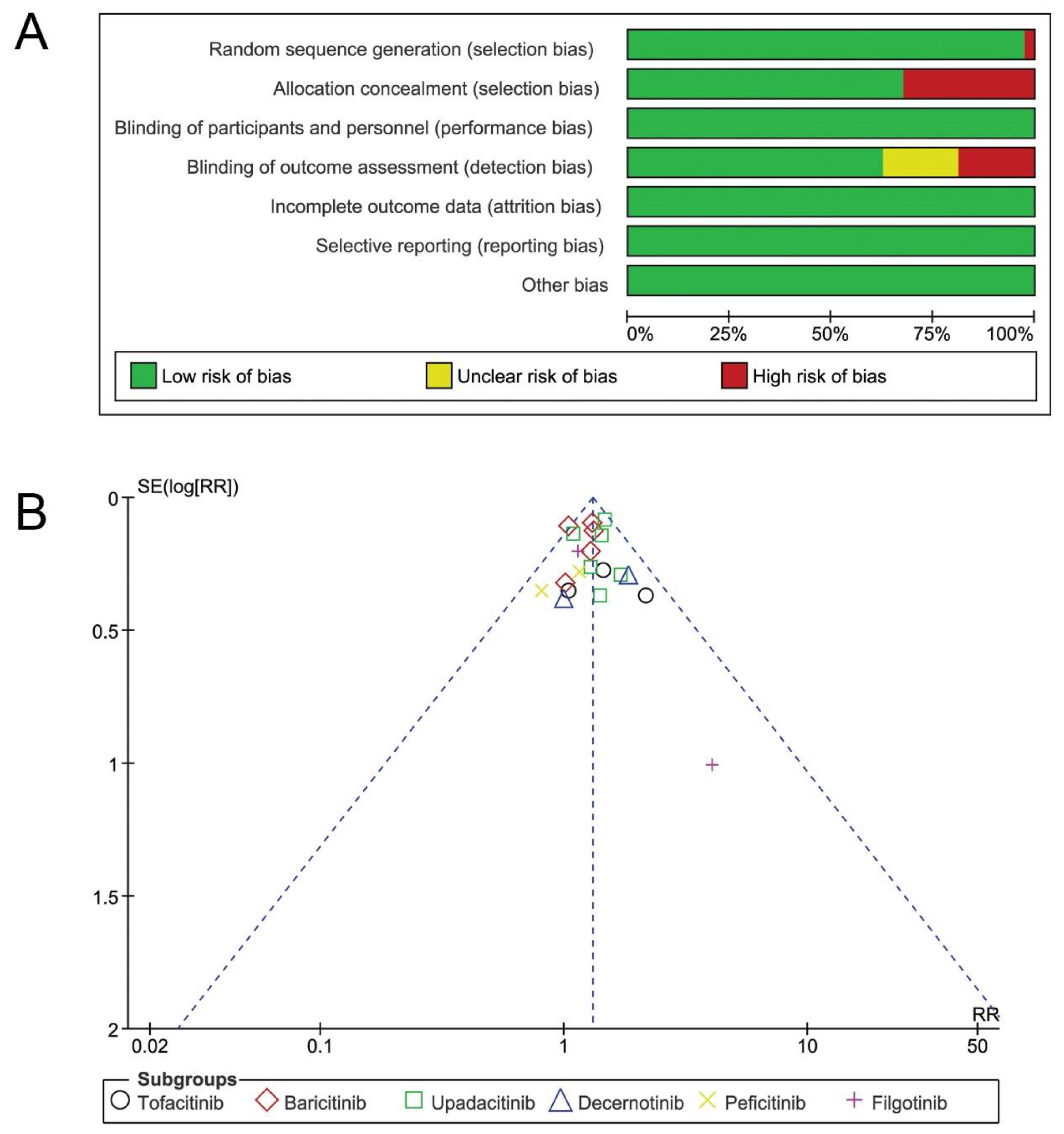
3.2. Risk of Bias Assessment
3.3. Efficacy
3.3.1. ACR20, ACR50, and ACR70
3.3.2. HAQ-ID
3.4. Safety
3.4.1. AEs and SAEs
3.4.2. Infections and Serious Infections
3.4.3. HZ
3.4.4. Upper Respiratory Tract Infections
3.4.5. Thromboembolic Events
3.4.6. MACE
3.4.7. Neoplasm
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| RA | Rheumatoid arthritis |
| csDMARDs | Conventional disease-modifying-drugs |
| MTX | Methotrexate |
| DAS28-4[ESR] | 28-joint disease activity score using erythrocyte sedimentation rate |
| JAK | Janus kinases |
| STAT | Signal transduction and activator of transcription |
| JAKinibs | JAK inhibitors |
| ACR 20 | American College of Rheumatology 20% |
| HAQ-DI | Health Assessment Questionnaire—Disability Index |
| AE | Adverse events |
| SAE | Serious adverse events |
| HZ | Herpes zoster |
| MD | Mean differences |
| RR | Risk ratio |
| CI | Confidence intervals |
References
- Taylor, P.C. Clinical efficacy of launched JAK inhibitors in rheumatoid arthritis. Rheumatology 2019, 58, i17–i26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smolen, J.S.; Aletaha, D.; McInnes, I.B. Rheumatoid arthritis. Lancet. 2016, 388, 2023–2038. [Google Scholar] [CrossRef]
- Sparks, J.A. Rheumatoid Arthritis. Ann. Intern. Med. 2019, 170, ITC1–ITC16. [Google Scholar] [CrossRef] [PubMed]
- Burmester, G.R.; Pope, J.E. Novel treatment strategies in rheumatoid arthritis. Lancet 2017, 389, 2338–2348. [Google Scholar] [CrossRef]
- Semerano, L.; Decker, P.; Clavel, G.; Boissier, M.C. Developments with investigational Janus kinase inhibitors for rheumatoid arthritis. Expert Opin. Investig. Drugs 2016, 25, 1355–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarzi-Puttini, P.; Ceribelli, A.; Marotto, D.; Batticciotto, A.; Atzeni, F. Systemic rheumatic diseases: From biological agents to small molecules. Autoimmun. Rev. 2019, 18, 583–592. [Google Scholar] [CrossRef]
- Banerjee, S.; Biehl, A.; Gadina, M.; Hasni, S.; Schwartz, D.M. JAK-STAT Signaling as a Target for Inflammatory and Autoimmune Diseases: Current and Future Prospects. Drugs 2017, 77, 521–546. [Google Scholar] [CrossRef]
- Villarino, A.V.; Kanno, Y.; O’Shea, J.J. Mechanisms and consequences of Jak-STAT signaling in the immune system. Nat. Immunol. 2017, 18, 374–384. [Google Scholar] [CrossRef]
- Malemud, C.J. The role of the JAK/STAT signal pathway in rheumatoid arthritis. Ther. Adv. Musculoskelet. Dis. 2018, 10, 117–127. [Google Scholar] [CrossRef]
- Fragoulis, G.E.; McInnes, I.B.; Siebert, S. JAK-inhibitors. New players in the field of immune-mediated diseases, beyond rheumatoid arthritis. Rheumatology 2019, 58, i43–i54. [Google Scholar] [CrossRef] [Green Version]
- Choy, E.H. Clinical significance of Janus Kinase inhibitor selectivity. Rheumatology 2019, 58, 953–962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mogul, A.; Corsi, K.; McAuliffe, L. Baricitinib: The Second FDA-Approved JAK Inhibitor for the Treatment of Rheumatoid Arthritis. Ann. Pharmacother. 2019, 53, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Duggan, S.; Keam, S.J. Upadacitinib: First Approval. Drugs 2019, 79, 1819–1828. [Google Scholar] [CrossRef] [PubMed]
- Kawalec, P.; Mikrut, A.; Wisniewska, N.; Pilc, A. The effectiveness of tofacitinib, a novel Janus kinase inhibitor, in the treatment of rheumatoid arthritis: A systematic review and meta-analysis. Clin Rheumatol. 2013, 32, 1415–1424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Huedo-Medina, T.B.; Sanchez-Meca, J.; Marin-Martinez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol. Methods. 2006, 11, 193–206. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.; Sutton, A.J.; Ioannidis, J.P.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [Green Version]
- Kremer, J.M.; Bloom, B.J.; Breedveld, F.C.; Coombs, J.H.; Fletcher, M.P.; Gruben, D.; Krishnaswami, S.; Burgos-Vargas, R.; Wilkinson, B.; Schmid, C.H.; et al. The safety and efficacy of a JAK inhibitor in patients with active rheumatoid arthritis: Results of a double-blind, placebo-controlled phase IIa trial of three dosage levels of CP-690,550 versus placebo. Arthritis. Rheum. 2009, 60, 1895–1905. [Google Scholar] [CrossRef]
- Tanaka, Y.; Suzuki, M.; Nakamura, H.; Toyoizumi, S.; Zwillich, S.H.; Tofacitinib Study, I. Phase II study of tofacitinib (CP-690,550) combined with methotrexate in patients with rheumatoid arthritis and an inadequate response to methotrexate. Arthritis. Care Res. 2011, 63, 1150–1158. [Google Scholar] [CrossRef]
- Van Vollenhoven, R.F.; Fleischmann, R.; Cohen, S.; Lee, E.B.; Garcia Meijide, J.A.; Wagner, S.; Forejtova, S.; Zwillich, S.H.; Gruben, D.; Koncz, T.; et al. Tofacitinib or adalimumab versus placebo in rheumatoid arthritis. N. Engl. J. Med. 2012, 367, 508–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleischmann, R.; Cutolo, M.; Genovese, M.C.; Lee, E.B.; Kanik, K.S.; Sadis, S.; Connell, C.A.; Gruben, D.; Krishnaswami, S.; Wallenstein, G.; et al. Phase IIb dose-ranging study of the oral JAK inhibitor tofacitinib (CP-690,550) or adalimumab monotherapy versus placebo in patients with active rheumatoid arthritis with an inadequate response to disease-modifying antirheumatic drugs. Arthritis Rheum. 2012, 64, 617–629. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, R.; Kremer, J.; Cush, J.; Schulze-Koops, H.; Connell, C.A.; Bradley, J.D.; Gruben, D.; Wallenstein, G.V.; Zwillich, S.H.; Kanik, K.S. Placebo-controlled trial of tofacitinib monotherapy in rheumatoid arthritis. N. Engl. J. Med. 2012, 367, 495–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kremer, J.M.; Cohen, S.; Wilkinson, B.E.; Connell, C.A.; French, J.L.; Gomez-Reino, J.; Gruben, D.; Kanik, K.S.; Krishnaswami, S.; Pascual-Ramos, V.; et al. A phase IIb dose-ranging study of the oral JAK inhibitor tofacitinib (CP-690,550) versus placebo in combination with background methotrexate in patients with active rheumatoid arthritis and an inadequate response to methotrexate alone. Arthritis Rheum. 2012, 64, 970–981. [Google Scholar] [CrossRef] [Green Version]
- Burmester, G.R.; Blanco, R.; Charles-Schoeman, C.; Wollenhaupt, J.; Zerbini, C.; Benda, B.; Gruben, D.; Wallenstein, G.; Krishnaswami, S.; Zwillich, S.H.; et al. Tofacitinib (CP-690,550) in combination with methotrexate in patients with active rheumatoid arthritis with an inadequate response to tumour necrosis factor inhibitors: A randomised phase 3 trial. Lancet 2013, 381, 451–460. [Google Scholar] [CrossRef]
- Kremer, J.; Li, Z.G.; Hall, S.; Fleischmann, R.; Genovese, M.; Martin-Mola, E.; Isaacs, J.D.; Gruben, D.; Wallenstein, G.; Krishnaswami, S.; et al. Tofacitinib in combination with nonbiologic disease-modifying antirheumatic drugs in patients with active rheumatoid arthritis: A randomized trial. Ann. Intern. Med. 2013, 159, 253–261. [Google Scholar] [CrossRef] [Green Version]
- Van der Heijde, D.; Tanaka, Y.; Fleischmann, R.; Keystone, E.; Kremer, J.; Zerbini, C.; Cardiel, M.H.; Cohen, S.; Nash, P.; Song, Y.W.; et al. Tofacitinib (CP-690,550) in patients with rheumatoid arthritis receiving methotrexate: Twelve-month data from a twenty-four-month phase III randomized radiographic study. Arthritis Rheum. 2013, 65, 559–570. [Google Scholar] [CrossRef]
- Boyle, D.L.; Soma, K.; Hodge, J.; Kavanaugh, A.; Mandel, D.; Mease, P.; Shurmur, R.; Cohen, S.; Singhal, A.K.; Wei, N.; et al. The JAK inhibitor tofacitinib suppresses synovial JAK1-STAT signalling in rheumatoid arthritis. Ann. Rheum. Dis. 2015, 74, 1311–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, Y.; Takeuchi, T.; Yamanaka, H.; Nakamura, H.; Toyoizumi, S.; Zwillich, S. Efficacy and safety of tofacitinib as monotherapy in Japanese patients with active rheumatoid arthritis: A 12-week, randomized, phase 2 study. Mod. Rheumatol. 2015, 25, 514–521. [Google Scholar] [CrossRef] [Green Version]
- Kremer, J.M.; Kivitz, A.J.; Simon-Campos, J.A.; Nasonov, E.L.; Tony, H.P.; Lee, S.K.; Vlahos, B.; Hammond, C.; Bukowski, J.; Li, H.; et al. Evaluation of the effect of tofacitinib on measured glomerular filtration rate in patients with active rheumatoid arthritis: Results from a randomised controlled trial. Arthritis Res. Ther. 2015, 17, 95. [Google Scholar] [CrossRef] [Green Version]
- Keystone, E.C.; Taylor, P.C.; Drescher, E.; Schlichting, D.E.; Beattie, S.D.; Berclaz, P.Y.; Lee, C.H.; Fidelus-Gort, R.K.; Luchi, M.; Rooney, T.P.; et al. Safety and efficacy of baricitinib at 24 weeks in patients with rheumatoid arthritis who have had an inadequate response to methotrexate. Ann. Rheum. Dis. 2015, 74, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Emoto, K.; Cai, Z.; Aoki, T.; Schlichting, D.; Rooney, T.; Macias, W. Efficacy and Safety of Baricitinib in Japanese Patients with Active Rheumatoid Arthritis Receiving Background Methotrexate Therapy: A 12-week, Double-blind, Randomized Placebo-controlled Study. J. Rheumatol. 2016, 43, 504–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genovese, M.C.; Kremer, J.; Zamani, O.; Ludivico, C.; Krogulec, M.; Xie, L.; Beattie, S.D.; Koch, A.E.; Cardillo, T.E.; Rooney, T.P.; et al. Baricitinib in Patients with Refractory Rheumatoid Arthritis. N. Engl. J. Med. 2016, 374, 1243–1252. [Google Scholar] [CrossRef]
- Taylor, P.C.; Keystone, E.C.; van der Heijde, D.; Weinblatt, M.E.; Del Carmen Morales, L.; Reyes Gonzaga, J.; Yakushin, S.; Ishii, T.; Emoto, K.; Beattie, S.; et al. Baricitinib versus Placebo or Adalimumab in Rheumatoid Arthritis. N. Engl. J. Med. 2017, 376, 652–662. [Google Scholar] [CrossRef] [PubMed]
- Dougados, M.; van der Heijde, D.; Chen, Y.C.; Greenwald, M.; Drescher, E.; Liu, J.; Beattie, S.; Witt, S.; de la Torre, I.; Gaich, C.; et al. Baricitinib in patients with inadequate response or intolerance to conventional synthetic DMARDs: Results from the RA-BUILD study. Ann. Rheum. Dis. 2017, 76, 88–95. [Google Scholar] [CrossRef]
- Li, Z.; Hu, J.; Bao, C.; Li, X.; Li, X.; Xu, J.; Spindler, A.J.; Zhang, X.; Xu, J.; He, D.; et al. Baricitinib in patients with rheumatoid arthritis with inadequate response to methotrexate: Results from a phase 3 study. Clin. Exp. Rheumatol. 2020, 38, 732–741. [Google Scholar]
- Kremer, J.M.; Emery, P.; Camp, H.S.; Friedman, A.; Wang, L.; Othman, A.A.; Khan, N.; Pangan, A.L.; Jungerwirth, S.; Keystone, E.C.; et al. A Phase IIb Study of ABT-494, a Selective JAK-1 Inhibitor, in Patients With Rheumatoid Arthritis and an Inadequate Response to Anti-Tumor Necrosis Factor Therapy. Arthritis Rheumatol. 2016, 68, 2867–2877. [Google Scholar] [CrossRef]
- Genovese, M.C.; Smolen, J.S.; Weinblatt, M.E.; Burmester, G.R.; Meerwein, S.; Camp, H.S.; Wang, L.; Othman, A.A.; Khan, N.; Pangan, A.L.; et al. Efficacy and Safety of ABT-494, a Selective JAK-1 Inhibitor, in a Phase IIb Study in Patients With Rheumatoid Arthritis and an Inadequate Response to Methotrexate. Arthritis Rheumatol. 2016, 68, 2857–2866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burmester, G.R.; Kremer, J.M.; Van den Bosch, F.; Kivitz, A.; Bessette, L.; Li, Y.; Zhou, Y.; Othman, A.A.; Pangan, A.L.; Camp, H.S. Safety and efficacy of upadacitinib in patients with rheumatoid arthritis and inadequate response to conventional synthetic disease-modifying anti-rheumatic drugs (SELECT-NEXT): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2018, 391, 2503–2512. [Google Scholar] [CrossRef]
- Genovese, M.C.; Fleischmann, R.; Combe, B.; Hall, S.; Rubbert-Roth, A.; Zhang, Y.; Zhou, Y.; Mohamed, M.F.; Meerwein, S.; Pangan, A.L. Safety and efficacy of upadacitinib in patients with active rheumatoid arthritis refractory to biologic disease-modifying anti-rheumatic drugs (SELECT-BEYOND): A double-blind, randomised controlled phase 3 trial. Lancet 2018, 391, 2513–2524. [Google Scholar] [CrossRef]
- Fleischmann, R.; Pangan, A.L.; Song, I.H.; Mysler, E.; Bessette, L.; Peterfy, C.; Durez, P.; Ostor, A.J.; Li, Y.; Zhou, Y.; et al. Upadacitinib Versus Placebo or Adalimumab in Patients with Rheumatoid Arthritis and an Inadequate Response to Methotrexate: Results of a Phase III, Double-Blind, Randomized Controlled Trial. Arthritis Rheumatol. 2019, 71, 1788–1800. [Google Scholar] [CrossRef] [PubMed]
- Kameda, H.; Takeuchi, T.; Yamaoka, K.; Oribe, M.; Kawano, M.; Zhou, Y.; Othman, A.A.; Pangan, A.L.; Kitamura, S.; Meerwein, S.; et al. Efficacy and safety of upadacitinib in Japanese patients with rheumatoid arthritis (SELECT-SUNRISE): A placebo-controlled phase IIb/III study. Rheumatology 2020, 59, 3303–3313. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, R.M.; Damjanov, N.S.; Kivitz, A.J.; Legedza, A.; Hoock, T.; Kinnman, N. A randomized, double-blind, placebo-controlled, twelve-week, dose-ranging study of decernotinib, an oral selective JAK-3 inhibitor, as monotherapy in patients with active rheumatoid arthritis. Arthritis Rheumatol. 2015, 67, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Genovese, M.C.; Yang, F.; Ostergaard, M.; Kinnman, N. Efficacy of VX-509 (decernotinib) in combination with a disease-modifying antirheumatic drug in patients with rheumatoid arthritis: Clinical and MRI findings. Ann. Rheum. Dis. 2016, 75, 1979–1983. [Google Scholar] [CrossRef] [PubMed]
- Genovese, M.C.; van Vollenhoven, R.F.; Pacheco-Tena, C.; Zhang, Y.; Kinnman, N. VX-509 (Decernotinib), an Oral Selective JAK-3 Inhibitor, in Combination With Methotrexate in Patients With Rheumatoid Arthritis. Arthritis Rheumatol. 2016, 68, 46–55. [Google Scholar] [CrossRef]
- Takeuchi, T.; Tanaka, Y.; Iwasaki, M.; Ishikura, H.; Saeki, S.; Kaneko, Y. Efficacy and safety of the oral Janus kinase inhibitor peficitinib (ASP015K) monotherapy in patients with moderate to severe rheumatoid arthritis in Japan: A 12-week, randomised, double-blind, placebo-controlled phase IIb study. Ann. Rheum. Dis. 2016, 75, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Genovese, M.C.; Greenwald, M.; Codding, C.; Zubrzycka-Sienkiewicz, A.; Kivitz, A.J.; Wang, A.; Shay, K.; Wang, X.; Garg, J.P.; Cardiel, M.H. Peficitinib, a JAK Inhibitor, in Combination With Limited Conventional Synthetic Disease-Modifying Antirheumatic Drugs in the Treatment of Moderate-to-Severe Rheumatoid Arthritis. Arthritis Rheumatol. 2017, 69, 932–942. [Google Scholar] [CrossRef]
- Kivitz, A.J.; Gutierrez-Urena, S.R.; Poiley, J.; Genovese, M.C.; Kristy, R.; Shay, K.; Wang, X.; Garg, J.P.; Zubrzycka-Sienkiewicz, A. Peficitinib, a JAK Inhibitor, in the Treatment of Moderate-to-Severe Rheumatoid Arthritis in Patients with an Inadequate Response to Methotrexate. Arthritis Rheumatol. 2017, 69, 709–719. [Google Scholar] [CrossRef] [Green Version]
- Takeuchi, T.; Tanaka, Y.; Tanaka, S.; Kawakami, A.; Iwasaki, M.; Katayama, K.; Rokuda, M.; Izutsu, H.; Ushijima, S.; Kaneko, Y.; et al. Efficacy and safety of peficitinib (ASP015K) in patients with rheumatoid arthritis and an inadequate response to methotrexate: Results of a phase III randomised, double-blind, placebo-controlled trial (RAJ4) in Japan. Ann. Rheum. Dis. 2019, 78, 1305–1319. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, Y.; Takeuchi, T.; Tanaka, S.; Kawakami, A.; Iwasaki, M.; Song, Y.W.; Chen, Y.H.; Wei, J.C.C.; Lee, S.H.; Rokuda, M.; et al. Efficacy and safety of peficitinib (ASP015K) in patients with rheumatoid arthritis and an inadequate response to conventional DMARDs: A randomised, double-blind, placebo-controlled phase III trial (RAJ3). Ann. Rheum. Dis. 2019, 78, 1320–1332. [Google Scholar] [CrossRef] [Green Version]
- Kavanaugh, A.; Kremer, J.; Ponce, L.; Cseuz, R.; Reshetko, O.V.; Stanislavchuk, M.; Greenwald, M.; Van der Aa, A.; Vanhoutte, F.; Tasset, C.; et al. Filgotinib (GLPG0634/GS-6034), an oral selective JAK1 inhibitor, is effective as monotherapy in patients with active rheumatoid arthritis: Results from a randomised, dose-finding study (DARWIN 2). Ann. Rheum. Dis. 2017, 76, 1009–1019. [Google Scholar] [CrossRef] [PubMed]
- Westhovens, R.; Taylor, P.C.; Alten, R.; Pavlova, D.; Enriquez-Sosa, F.; Mazur, M.; Greenwald, M.; Van der Aa, A.; Vanhoutte, F.; Tasset, C.; et al. Filgotinib (GLPG0634/GS-6034), an oral JAK1 selective inhibitor, is effective in combination with methotrexate (MTX) in patients with active rheumatoid arthritis and insufficient response to MTX: Results from a randomised, dose-finding study (DARWIN 1). Ann. Rheum. Dis. 2017, 76, 998–1008. [Google Scholar] [CrossRef] [Green Version]
- Vanhoutte, F.; Mazur, M.; Voloshyn, O.; Stanislavchuk, M.; Van der Aa, A.; Namour, F.; Galien, R.; Meuleners, L.; van‘t Klooster, G. Efficacy, Safety, Pharmacokinetics, and Pharmacodynamics of Filgotinib, a Selective JAK-1 Inhibitor, After Short-Term Treatment of Rheumatoid Arthritis: Results of Two Randomized Phase IIa Trials. Arthritis Rheumatol. 2017, 69, 1949–1959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genovese, M.C.; Kalunian, K.; Gottenberg, J.E.; Mozaffarian, N.; Bartok, B.; Matzkies, F.; Gao, J.; Guo, Y.; Tasset, C.; Sundy, J.S.; et al. Effect of Filgotinib vs Placebo on Clinical Response in Patients with Moderate to Severe Rheumatoid Arthritis Refractory to Disease-Modifying Antirheumatic Drug Therapy: The FINCH 2 Randomized Clinical Trial. JAMA 2019, 322, 315–325. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.M.; Kanno, Y.; Villarino, A.; Ward, M.; Gadina, M.; O’Shea, J.J. JAK inhibition as a therapeutic strategy for immune and inflammatory diseases. Nat. Rev. Drug Discov. 2017, 16, 843–862. [Google Scholar] [CrossRef] [PubMed]
- Traynor, K. FDA approves tofacitinib for rheumatoid arthritis. Am. J. Health Syst. Pharm. 2012, 69, 2120. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. Full Prescribing Information for XELJANZ (tofacitinib). May 2018. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/203214s018lbl.pdf (accessed on 25 May 2021).
- U.S. Food and Drug Administration. Full Prescribing Information for OLUMIANT (baricitinib). May 2018. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/207924s000lbl.pdf (accessed on 25 May 2021).
- Administration UFaD. Full Prescribing Information for RINVOQ™ (upadacitinib) 2019. August 2019. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/211675s000lbl.pdf (accessed on 25 May 2021).
- Bechman, K.; Subesinghe, S.; Norton, S.; Atzeni, F.; Galli, M.; Cope, A.P.; Winthrop, K.L.; Galloway, J.B. A systematic review and meta-analysis of infection risk with small molecule JAK inhibitors in rheumatoid arthritis. Rheumatology 2019, 58, 1755–1766. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.C.; Lee, Y.H. Comparison of the efficacy and safety of tofacitinib and baricitinib in patients with active rheumatoid arthritis: A Bayesian network meta-analysis of randomized controlled trials. Z. Rheumatol. 2019, 78, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Kosinski, M.; Zhao, S.Z.; Dedhiya, S.; Osterhaus, J.T.; Ware, J.E., Jr. Determining minimally important changes in generic and disease-specific health-related quality of life questionnaires in clinical trials of rheumatoid arthritis. Arthritis Rheum. 2000, 43, 1478–1487. [Google Scholar] [CrossRef]
- Wells, G.A.; Tugwell, P.; Kraag, G.R.; Baker, P.R.; Groh, J.; Redelmeier, D.A. Minimum important difference between patients with rheumatoid arthritis: The patient’s perspective. J. Rheumatol. 1993, 20, 557–560. [Google Scholar] [PubMed]
- Kunwar, S.; Collins, C.E.; Constantinescu, F. Baricitinib, a Janus kinase inhibitor, in the treatment of rheumatoid arthritis: A systematic literature review and meta-analysis of randomized controlled trials. Clin. Rheumatol. 2018, 37, 2611–2620. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Sun, L.; Wang, S.; Davis, J.M., III; Matteson, E.L.; Murad, M.H.; Luo, F.; Vassallo, R. Efficacy and Safety of Tofacitinib, Baricitinib, and Upadacitinib for Rheumatoid Arthritis: A Systematic Review and Meta-Analysis. Mayo. Clin. Proc. 2020, 95, 1404–1419. [Google Scholar] [CrossRef] [PubMed]
- Desai, R.J.; Pawar, A.; Weinblatt, M.E.; Kim, S.C. Comparative Risk of Venous Thromboembolism in Rheumatoid Arthritis Patients Receiving Tofacitinib Versus Those Receiving Tumor Necrosis Factor Inhibitors: An Observational Cohort Study. Arthritis Rheumatol. 2019, 71, 892–900. [Google Scholar] [CrossRef] [PubMed]
- Mease, P.; Charles-Schoeman, C.; Cohen, S.; Fallon, L.; Woolcott, J.; Yun, H.; Kremer, J.; Greenberg, J.; Malley, W.; Onofrei, A.; et al. Incidence of venous and arterial thromboembolic events reported in the tofacitinib rheumatoid arthritis, psoriasis and psoriatic arthritis development programmes and from real-world data. Ann. Rheum. Dis. 2020, 79, 1400–1413. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S.; Landewe, R.B.M.; Bijlsma, J.W.J.; Burmester, G.R.; Dougados, M.; Kerschbaumer, A.; McInnes, I.B.; Sepriano, A.; van Vollenhoven, R.F.; de Wit, M.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann. Rheum. Dis. 2020, 79, 685–699. [Google Scholar] [CrossRef] [Green Version]
- Yates, M.; Mootoo, A.; Adas, M.; Bechman, K.; Rampes, S.; Patel, V.; Qureshi, S.; Cope, A.P.; Norton, S.; Galloway, J.B. Venous Thromboembolism Risk With JAK Inhibitors: A Meta-Analysis. Arthritis Rheumatol. 2021, 73, 779–788. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Author (Year) | Region | Trial Identifier | Follow-Up | No. of Patients | Dose |
|---|---|---|---|---|---|
| Tofacitinib | |||||
| Kremer 2009 [19] | Worldwide | NCT00147498 | 6 weeks | 264 | 5, 15, 30 mg twice daily |
| Tanaka 2011 [20] | Japan | NCT00603512 | 12 weeks | 140 | 1, 3, 5, 10, 15 mg twice daily |
| Vollenhoven 2012 [21] | America and Europe | NCT00853385 | 24 weeks | 513 | 5, 10 mg twice daily |
| Fleischmann 2012a [22] | Worldwide | NCT00550446 | 24 weeks | 274 | 1, 3, 5, 10, 15 mg twice daily |
| Fleischmann 2012 b [23] | Worldwide | NCT00814307 | 24 weeks | 611 | 5, 10 mg twice daily |
| Kremer 2012 [24] | America and Europe | NCT00413660 | 12 weeks | 507 | 1, 3, 5, 10, 15 mg twice daily, 20 mg/day |
| Burmester 2013 [25] | America and Europe | NCT00960440 | 12 weeks | 399 | 5, 10 mg twice daily |
| Kremer 2013 [26] | Worldwide | NCT00856544 | 24 weeks | 792 | 5, 10 mg twice daily |
| Heijde 2013 [27] | Worldwide | NCT00847613 | 24 weeks | 797 | 5, 10 mg twice daily |
| Boyle 2015 [28] | Worldwide | NCT00976599 | 4 weeks | 29 | 10 mg twice daily |
| Tanaka 2015 [29] | Japan | NCT00687193 | 12 weeks | 317 | 1, 3, 5, 10, 15 mg twice daily, 20 mg/day |
| Kremer 2015 [30] | Worldwide | NCT01484561 | 6 weeks | 148 | 10 mg twice daily |
| Baricitinib | |||||
| Keystone 2015 [31] | Worldwide | NCT01185353 | 12 weeks | 301 | 1, 2, 4, 8 mg once daily |
| Tanaka 2016 [32] | Japan | NCT01469013 | 12 weeks | 145 | 1, 2, 4, 8 mg once daily |
| Genovese 2016 [33] | Worldwide | NCT01721044 | 24 weeks | 527 | 2, 4 mg once daily |
| Taylor 2017 [34] | Worldwide | NCT01710358 | 24 weeks | 1307 | 4 mg once daily |
| Dougados 2017 [35] | Worldwide | NCT01721057 | 24 weeks | 684 | 2, 4 mg once daily |
| Li 2020 [36] | China, Brazil, Argentina | NCT02265705 | 12 weeks | 290 | 4 mg once daily |
| Upadacitinib | |||||
| Kremer 2016 [37] | Worldwide | NCT01960855 | 12 weeks | 276 | 3, 6, 12, 18 mg twice daily |
| Genovese 2016 [38] | Worldwide | NCT02066389 | 12 weeks | 299 | 3, 6, 12, 18 mg twice daily, 24 mg once daily |
| Burmester 2018 [39] | Worldwide | NCT02675426 | 12 weeks | 661 | 15, 30 mg once daily |
| Genovese 2018 [40] | Worldwide | NCT02706847 | 24 weeks | 499 | 15, 30 mg once daily |
| Fleischmann 2019 [41] | Worldwide | NCT02629159 | 12 weeks | 1304 | 15 mg once daily |
| Kameda 2020 [42] | Japan | NCT02720523 | 12 weeks | 148 | 15, 30 mg once daily |
| Decernotinib | |||||
| Fleischmann 2015 [43] | Worldwide | NCT01052194 | 12 weeks | 204 | 25, 50, 100, 150 mg twice daily |
| Genovese 2016a [44] | Worldwide | NCT01754935 | 12 weeks | 43 | 100, 200, 300 mg once daily |
| Genovese 2016b [45] | Worldwide | NCT2011-004419-22 | 24 weeks | 358 | 100, 150, 200 mg once daily, 100 mg twice daily |
| Peficitinib | |||||
| Takeuchi 2016 [46] | Japan | NCT01649999 | 12 weeks | 281 | 25, 50, 100, 150 mg once daily |
| Genovese 2017 [47] | Worldwide | NCT01565655 | 12 weeks | 289 | 25, 50, 100, 150 mg once daily |
| Kivitz 2017 [48] | Worldwide | NCT01554696 | 12 weeks | 378 | 25, 50, 100, 150 mg once daily |
| Takeuchi 2019 [49] | Japan | NCT02305849 | 12 weeks | 519 | 100, 150 mg once daily |
| Tanaka 2019 [50] | Japan, Korea, Taiwan | NCT02308163 | 12 weeks | 307 | 100, 150 mg once daily |
| Filgotinib | |||||
| Kavanaugh 2017 [51] | Worldwide | NCT01894516 | 24 weeks | 283 | 50, 100, 200 mg once daily |
| Westhovens 2017 [52] | Worldwide | NCT01888874 | 24 weeks | 594 | 50, 100, 200 mg once daily and twice daily |
| Vanhoutte 2017 1 [53] | Republic of Moldova | NCT01384422 | 4 weeks | 36 | 100 mg twice daily or 200 once daily |
| Vanhoutte 2017 2 [53] | Worldwide | NCT01668641 | 4 weeks | 91 | 30, 75, 150, 300 mg once daily |
| Genovese 2019 [54] | Worldwide | NCT02873936 | 24 weeks | 449 | 100, 200 mg once daily |
| Outcomes | Studies (n) | RR | Lower 95% CI | Upper 95% CI | I2 | Outcomes | Studies (n) | RR | Lower 95% CI | Upper 95% CI | I2 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| ACR-20 | Infections | ||||||||||
| All RCTs | 36 | 2.03 | 1.85 | 2.23 | 65% | All RCTs | 21 | 1.29 | 1.19 | 1.39 | 0% |
| Tofacitinib | 11 | 2.21 | 1.86 | 2.63 | 52% | Tofacitinib | 3 | 1.30 | 1.00 | 1.94 | 0% |
| Baricitinib | 6 | 1.95 | 1.57 | 2.42 | 78% | Baricitinib | 5 | 1.22 | 1.09 | 1.37 | 0% |
| Upadacitinib | 6 | 1.99 | 1.68 | 2.36 | 64% | Upadacitinib | 6 | 1.38 | 1.22 | 1.56 | 0% |
| Decernotinib | 3 | 2.61 | 1.70 | 4.01 | 31% | Decernotinib | 2 | 1.43 | 0.80 | 2.58 | 37% |
| Peficitinib | 5 | 2.01 | 1.32 | 3.05 | 84% | Peficitinib | 2 | 1.01 | 0.66 | 1.56 | 0% |
| Filgotinib | 5 | 1.80 | 1.43 | 2.27 | 46% | Filgotinib | 2 | 1.50 | 0.53 | 4.20 | 37% |
| ACR-50 | ACR-70 | ||||||||||
| All RCTs | 35 | 3.12 | 2.48 | 3.93 | 84% | All RCTs | 33 | 3.87 | 3.02 | 4.97 | 56% |
| Tofacitinib | 11 | 3.43 | 2.30 | 5.12 | 78% | Tofacitinib | 11 | 4.15 | 2.21 | 7.80 | 74% |
| Baricitinib | 6 | 2.73 | 2.03 | 3.66 | 64% | Baricitinib | 6 | 3.81 | 2.97 | 4.89 | 0% |
| Upadacitinib | 6 | 2.25 | 1.12 | 4.52 | 96% | Upadacitinib | 6 | 4.53 | 3.53 | 5.83 | 0% |
| Decernotinib | 3 | 4.72 | 2.48 | 8.96 | 0% | Decernotinib | 3 | 4.06 | 1.50 | 10.98 | 0% |
| Peficitinib | 5 | 2.84 | 1.42 | 5.70 | 82% | Peficitinib | 5 | 3.64 | 1.32 | 10.05 | 73% |
| Filgotinib | 4 | 5.56 | 2.79 | 11.06 | 11% | Filgotinib | 2 | 3.41 | 0.94 | 12.40 | 45% |
| HAQ-DI | Serious infections | ||||||||||
| All RCTs | 20 | −0.31 | −0.34 | −0.28 | 0% | All RCTs | 29 | 1.30 | 0.92 | 1.86 | 0% |
| Tofacitinib | 7 | −0.34 | −0.39 | −0.28 | 0% | Tofacitinib | 8 | 1.35 | 0.72 | 2.55 | 0% |
| Baricitinib | 2 | −0.24 | −0.33 | −0.15 | 0% | Baricitinib | 6 | 0.91 | 0.48 | 1.71 | 0% |
| Upadacitinib | 5 | −0.31 | −0.36 | −0.26 | 0% | Upadacitinib | 6 | 1.92 | 0.83 | 4.47 | 4% |
| Decernotinib | 2 | −0.24 | −0.48 | −0.01 | 72% | Decernotinib | 2 | 2.58 | 0.49 | 13.63 | 0% |
| Peficitinib | 1 | −0.22 | −0.42 | −0.02 | - | Peficitinib | 4 | 2.63 | 0.59 | 11.73 | 0% |
| Filgotinib | 3 | −0.33 | −0.44 | −0.22 | 44% | Filgotinib | 3 | 0.67 | 0.18 | 2.44 | 0% |
| Adverse events | Herpes zoster | ||||||||||
| All RCTs | 34 | 1.10 | 1.05 | 1.14 | 25% | All RCTs | 25 | 1.59 | 1.09 | 2.32 | 0% |
| Tofacitinib | 11 | 1.06 | 0.98 | 1.15 | 29% | Tofacitinib | 4 | 1.28 | 0.72 | 2.29 | 0% |
| Baricitinib | 5 | 1.10 | 1.01 | 1.21 | 48% | Baricitinib | 6 | 3.15 | 1.19 | 8.33 | 0% |
| Upadacitinib | 6 | 1.19 | 1.11 | 1.28 | 7% | Upadacitinib | 6 | 1.25 | 0.56 | 2.81 | 0% |
| Decernotinib | 3 | 1.32 | 0.97 | 1.78 | 40% | Decernotinib | 1 | 1.79 | 0.09 | 34.04 | - |
| Peficitinib | 5 | 1.04 | 0.94 | 1.16 | 0% | Peficitinib | 5 | 2.13 | 0.51 | 8.92 | 37% |
| Filgotinib | 5 | 0.96 | 0.84 | 1.10 | 0% | Filgotinib | 3 | 0.97 | 0.21 | 4.51 | 0% |
| Serious adverse events | Upper respiratory infection | ||||||||||
| All RCTs | 34 | 0.94 | 0.77 | 1.15 | 0% | All RCTs | 15 | 1.26 | 0.97 | 1.63 | 0% |
| Tofacitinib | 11 | 0.74 | 0.47 | 1.18 | 20% | Tofacitinib | 8 | 1.20 | 0.69 | 2.10 | 33% |
| Baricitinib | 6 | 0.92 | 0.65 | 1.31 | 0% | Baricitinib | 2 | 1.22 | 0.78 | 1.89 | 0% |
| Upadacitinib | 6 | 1.72 | 0.92 | 3.25 | 18% | Upadacitinib | 1 | 1.34 | 0.63 | 2.83 | - |
| Decernotinib | 3 | 1.47 | 0.58 | 3.71 | 0% | Decernotinib | 1 | 1.24 | 0.28 | 5.52 | - |
| Peficitinib | 5 | 0.95 | 0.46 | 1.96 | 0% | Peficitinib | 2 | 1.60 | 0.69 | 3.67 | 0% |
| Filgotinib | 3 | 0.70 | 0.24 | 2.07 | 46% | Filgotinib | 1 | 0.89 | 0.30 | 2.60 | - |
| Thromboembolic events | MACE | ||||||||||
| All RCTs | 13 | 1.04 | 0.38 | 2.84 | 0% | All RCTs | 16 | 1.02 | 0.45 | 2.34 | 0% |
| Tofacitinib | 2 | 0.19 | 0.01 | 2.91 | 35% | Tofacitinib | 3 | 2.43 | 0.31 | 19.07 | 0% |
| Baricitinib | 2 | 2.38 | 0.27 | 20.84 | 0% | Baricitinib | 5 | 0.59 | 0.10 | 3.40 | 21% |
| Upadacitinib | 5 | 1.65 | 0.33 | 8.35 | 0% | Upadacitinib | 5 | 1.17 | 0.32 | 4.22 | 0% |
| Decernotinib | 1 | 0.77 | 0.03 | 18.52 | - | Decernotinib | 2 | 0.76 | 0.08 | 7.22 | 0% |
| Peficitinib * | 2 | - | - | - | - | Peficitinib * | 1 | - | - | - | - |
| Filgotinib | 1 | 1.49 | 0.06 | 36.24 | - | Filgotinib | 0 | - | - | - | - |
| Neoplasms | |||||||||||
| All RCTs | 19 | 1.70 | 0.74 | 3.89 | 0% | ||||||
| Tofacitinib | 1 | 9.50 | 0.56 | 162.20 | - | ||||||
| Baricitinib | 5 | 1.03 | 0.26 | 4.10 | 0% | ||||||
| Upadacitinib | 6 | 1.50 | 0.40 | 5.54 | 0% | ||||||
| Decernotinib | 5 | 2.92 | 0.35 | 24.20 | 0% | ||||||
| Peficitinib | - | - | - | - | - | ||||||
| Filgotinib * | 2 | - | - | - | - |
| Variables | No. of Studies | No. of Patients | Effect | NNT/NNH | Quality of the Evidence (GRADE) | Quality Domains and Assessments | Importance | ||
|---|---|---|---|---|---|---|---|---|---|
| JAKinibs Group | Placebo Group | Relative (95% CI) | Absolute (95% CI) | ||||||
| ACR20 | 36 | 6191/10,361 (59.8%) | 1251/4255 (29.4%) | RR 2.03 (1.85 to 2.23) | 303 more per 1000 (from 250 more to 362 more) | 4 | ⨁⨁⨁◯ MODERATE | Risk of bias: not serious Inconsistency: not serious Indirectness: not serious Imprecision: not serious Other: publication bias strongly suspected a | Critical |
| ACR50 | 35 | 3800/10,061 (37.8%) | 551/4107 (13.4%) | RR 3.10 (2.63 to 3.66) | 282 more per 1000 (from 219 more to 357 more) | 5 | ⨁⨁⨁◯ MODERATE | Risk of bias: not serious Inconsistency: not serious Indirectness: not serious Imprecision: not serious Other: publication bias strongly suspected a | Important |
| ACR70 | 33 | 1946/9963 (19.5%) | 212/4078 (5.2%) | RR 3.87 (3.02 to 4.97) | 149 more per 1000 (from 105 more to 206 more) | 7 | ⨁⨁⨁◯ MODERATE | Risk of bias: not serious Inconsistency: not serious Indirectness: not serious Imprecision: not serious Other: publication bias strongly suspected a | Important |
| Adverse events | 34 | 5735/10,181 (56.3%) | 2162/4079 (53.0%) | RR 1.10 (1.05 to 1.14) | 53 more per 1000 (from 27 more to 74 more) | 30 | ⨁⨁⨁⨁ HIGH | Risk of bias: not serious Inconsistency: not serious Indirecteness: not serious Imprecision: not serious Other: none | Critical |
| Serious adverse events | 34 | 321/9898 (3.2%) | 136/4181 (3.3%) | RR 0.94 (0.77 to 1.15) | 2 fewer per 1000 (from 7 fewer to 5 more) | 1000 | ⨁⨁⨁◯ MODERATE | Risk of bias: not serious Inconsistency: seriousIndirectness: not serious Imprecision: not serious Other: publication bias strongly suspected a | Important |
| Infection | 21 | 1696/6292 (27.0%) | 695/2948 (23.6%) | RR 1.29 (1.19 to 1.39) | 68 more per 1000 (from 45 more to 92 more) | 30 | ⨁⨁⨁⨁ HIGH | Risk of bias: not serious Inconsistency: not serious Indirectness: not serious Imprecision: not serious Other: none | Important |
| Serious infection | 29 | 155/9043 (1.7%) | 37/3879 (1.0%) | RR 1.30 (0.92 to 1.86) | 3 more per 1000 (from 1 fewer to 8 more) | 143 | ⨁⨁⨁⨁ HIGH | Risk of bias: not serious Inconsistency: serious Indirectness: not serious Imprecision: not serious Other: none | Important |
| Herpes zoster | 25 | 160/7700 (2.1%) | 28/3533 (0.8%) | RR 1.59 (1.09 to 2.32) | 5 more per 1000 (from 1 more to 10 more) | 77 | ⨁⨁⨁⨁ HIGH | Risk of bias: not serious Inconsistency: serious b Indirectness: not serious Imprecision: serious Other: none | Important |
| Upper respiratory infection | 15 | 315/5491 (5.7%) | 74/1733 (4.3%) | RR 1.26 (0.97 to 1.63) | 11 more per 1000 (from 1 more to 27 more) | 72 | ⨁⨁⨁◯ MODERATE | Risk of bias: not serious Inconsistency: not serious Indirectness: not serious Imprecision: not serious Other: publication bias strongly suspected a | Not important |
| Thromboembolic events | 13 | 12/4455 (0.3%) | 3/2241 (0.1%) | RR 1.04 (0.38 to 2.84) | 0 fewer per 1000 (from 1 fewer to 2 more) | 500 | ⨁⨁◯◯ LOW | Risk of bias: not serious Inconsistency: not serious Indirectness: not serious Imprecision: serious b: Other: publication bias strongly suspected a | Important |
| MACE | 16 | 20/5704 (0.4%) | 5/2735 (0.2%) | RR 1.02 (0.45 to 2.34) | 0 fewer per 1000 (from 1 fewer to 2 more) | 500 | ⨁⨁◯◯ LOW | Risk of bias: serious Inconsistency: not serious Indirectness: not serious Imprecision: serious b: Other: publication bias strongly suspected a | Not IMPORTANT |
| Neoplasms | 19 | 27/5885 (0.5%) | 4/3051 (0.1%) | RR 1.70 (0.74 to 3.89) | 1 fewer per 1000 (from 0 fewer to 4 more) | 250 | ⨁⨁◯◯ LOW | Risk of bias: serious Inconsistency: not serious Indirectness: not serious Imprecision: serious b: Other: publication bias strongly suspected a | Not IMPORTANT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, F.; Tang, X.; Zhu, M.; Mao, H.; Wan, H.; Luo, F. Efficacy and Safety of JAK Inhibitors for Rheumatoid Arthritis: A Meta-Analysis. J. Clin. Med. 2022, 11, 4459. https://doi.org/10.3390/jcm11154459
Wang F, Tang X, Zhu M, Mao H, Wan H, Luo F. Efficacy and Safety of JAK Inhibitors for Rheumatoid Arthritis: A Meta-Analysis. Journal of Clinical Medicine. 2022; 11(15):4459. https://doi.org/10.3390/jcm11154459
Chicago/Turabian StyleWang, Faping, Xiaoju Tang, Min Zhu, Hui Mao, Huajing Wan, and Fengming Luo. 2022. "Efficacy and Safety of JAK Inhibitors for Rheumatoid Arthritis: A Meta-Analysis" Journal of Clinical Medicine 11, no. 15: 4459. https://doi.org/10.3390/jcm11154459
APA StyleWang, F., Tang, X., Zhu, M., Mao, H., Wan, H., & Luo, F. (2022). Efficacy and Safety of JAK Inhibitors for Rheumatoid Arthritis: A Meta-Analysis. Journal of Clinical Medicine, 11(15), 4459. https://doi.org/10.3390/jcm11154459