
Impact of Catheter Ablation on Brain Microstructure and Blood Flow Alterations for Cognitive Improvements in Patients with Atrial Fibrillation: A Pilot Longitudinal Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection and Protocol
2.3. Interventional Procedures for AF Ablation
2.4. Cognitive–Psychological Tests
2.5. Echocardiography
2.6. Brain Image Acquisition
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Longitudinal Changes in Cognitive Function after a 6-Month AF Ablation Therapy
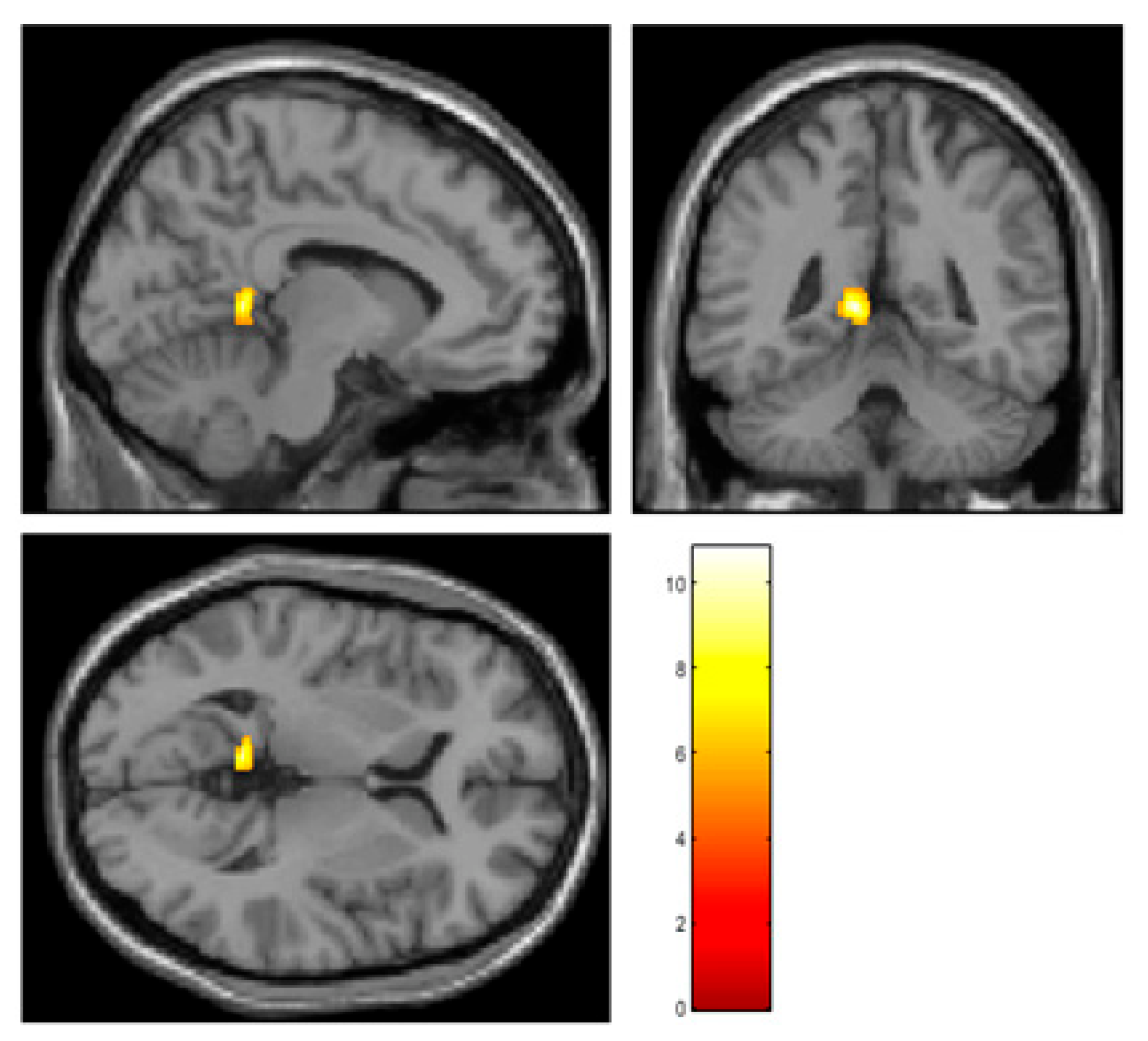
3.3. Changes in Brain Perfusion after a 6-Month AF Ablation Therapy
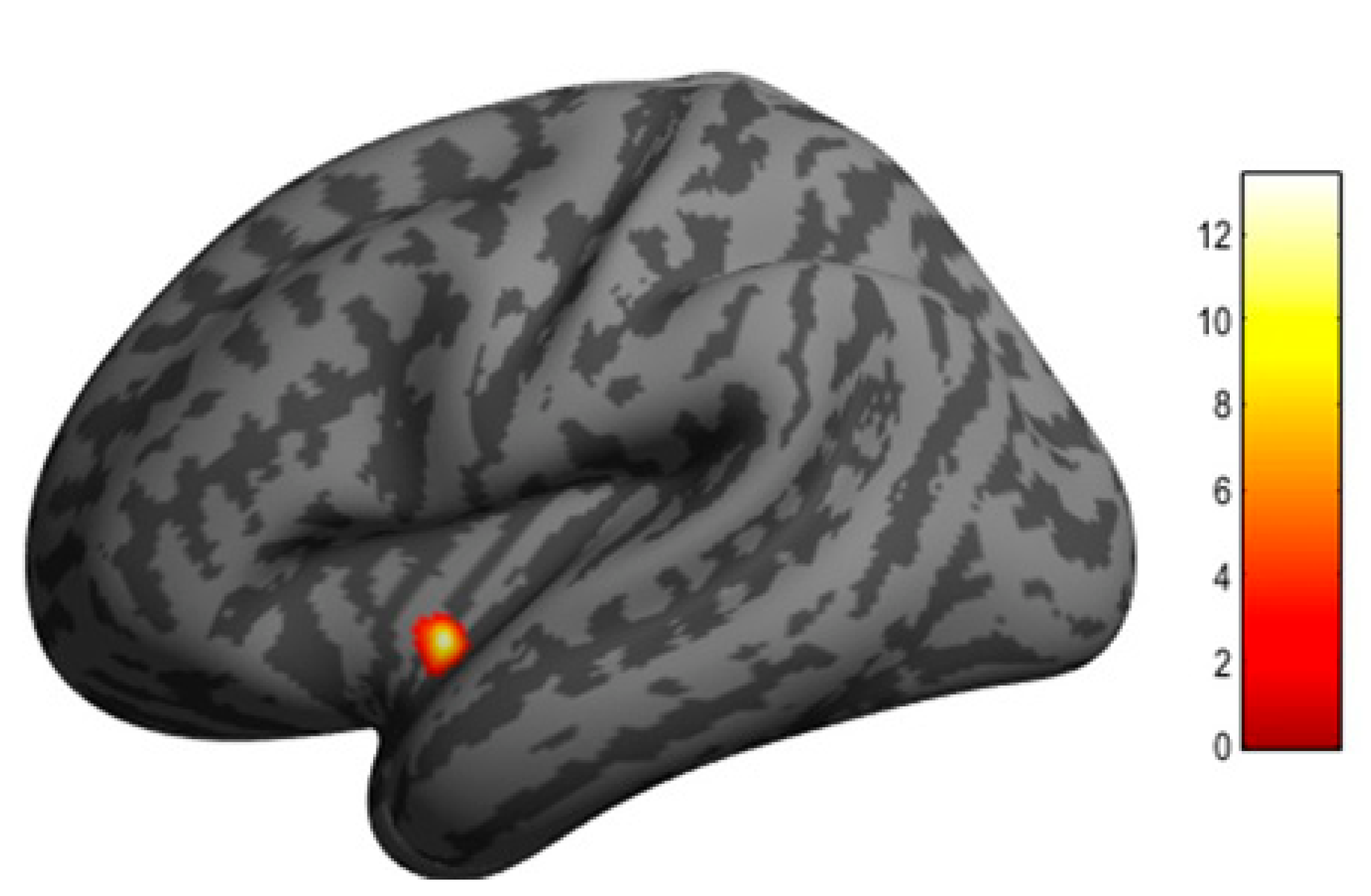
3.4. Microanatomical Changes in Cortical Thickness after a 6-Month AF Ablation Therapy
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miyasaka, Y.; Barnes, M.E.; Gersh, B.J.; Cha, S.S.; Bailey, K.R.; Abhayaratna, W.P.; Seward, J.B.; Tsang, T.S. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006, 114, 119–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Bruijn, R.F.; Heeringa, J.; Wolters, F.J.; Franco, O.H.; Stricker, B.H.; Hofman, A.; Koudstaal, P.J.; Ikram, M.A. Association between atrial fibrillation and dementia in the general population. JAMA Neurol. 2015, 72, 1288–1294. [Google Scholar] [CrossRef]
- Ott, A.; Breteler, M.M.; de Bruyne, M.C.; van Harskamp, F.; Grobbee, D.E.; Hofman, A. Atrial fibrillation and dementia in a population-based study. The Rotterdam Study. Stroke 1997, 28, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Jin, M.N.; Kim, T.H.; Kang, K.W.; Yu, H.T.; Uhm, J.S.; Joung, B.; Lee, M.H.; Kim, E.; Pak, H.N. Atrial fibrillation catheter ablation improves 1-year follow-up cognitive function, especially in patients with impaired cognitive function. Circ. Arrhythm. Electrophysiol. 2019, 12, e007197. [Google Scholar] [CrossRef]
- Stefansdottir, H.; Arnar, D.O.; Aspelund, T.; Sigurdsson, S.; Jonsdottir, M.K.; Hjaltason, H.; Launer, L.J.; Gudnason, V. Atrial fibrillation is associated with reduced brain volume and cognitive function independent of cerebral infarcts. Stroke 2013, 44, 1020–1025. [Google Scholar] [CrossRef] [Green Version]
- Gardarsdottir, M.; Sigurdsson, S.; Aspelund, T.; Rokita, H.; Launer, L.J.; Gudnason, V.; Arnar, D.O. Atrial fibrillation is associated with decreased total cerebral blood flow and brain perfusion. Europace 2018, 20, 1252–1258. [Google Scholar] [CrossRef] [PubMed]
- Kato, N.; Muraga, K.; Hirata, Y.; Shindo, A.; Matsuura, K.; Ii, Y.; Shiga, M.; Tabei, K.I.; Satoh, M.; Fujita, S.; et al. Brain magnetic resonance imaging and cognitive alterations after ablation in patients with atrial fibrillation. Sci. Rep. 2021, 11, 18995. [Google Scholar] [CrossRef] [PubMed]
- Bunch, T.J.; Crandall, B.G.; Weiss, J.P.; May, H.T.; Bair, T.L.; Osborn, J.S.; Anderson, J.L.; Muhlestein, J.B.; Horne, B.D.; Lappe, D.L.; et al. Patients treated with catheter ablation for atrial fibrillation have long-term rates of death, stroke, and dementia similar to patients without atrial fibrillation. J. Cardiovasc. Electrophysiol. 2011, 22, 839–845. [Google Scholar] [CrossRef]
- Petersen, E.T.; Lim, T.; Golay, X. Model-free arterial spin labeling quantification approach for perfusion MRI. Magn. Reson. Med. 2006, 55, 219–232. [Google Scholar] [CrossRef]
- Tatewaki, Y.; Higano, S.; Taki, Y.; Thyreau, B.; Murata, T.; Mugikura, S.; Ito, D.; Takase, K.; Takahashi, S. Regional reliability of quantitative signal targeting with alternating radiofrequency (STAR) labeling of arterial regions (QUASAR). J. Neuroimaging 2014, 24, 554–561. [Google Scholar] [CrossRef]
- Tatewaki, Y.; Mutoh, T.; Sato, H.; Enoki, R.; Kobayashi, A.; Muranaka, M.; Yamamoto, S.; Yagi, T.; Taki, Y. Catheter ablation improves QUASAR-arterial spin labeling based regional brain perfusion in the posterior cingulate cortex and auditory-verbal memory function in elderly patients with atrial fibrillation. Circulation 2020, 142 (Suppl. 3), A13806. [Google Scholar] [CrossRef]
- Kochhäuser, S.; Lohmann, H.H.; Ritter, M.A.; Leitz, P.; Güner, F.; Zellerhoff, S.; Korsukewitz, C.; Dechering, D.G.; Banken, J.; Peters, N.M.; et al. Neuropsychological impact of cerebral microemboli in ablation of atrial fibrillation. Clin. Res. Cardiol. 2015, 104, 234–240. [Google Scholar] [CrossRef]
- Vann, S.D.; Aggleton, J.P.; Maguire, E.A. What does the retrosplenial cortex do? Nat. Rev. Neurosci. 2009, 10, 792–802. [Google Scholar] [CrossRef] [PubMed]
- Aldrugh, S.; Sardana, M.; Henninger, N.; Saczynski, J.S.; McManus, D.D. Atrial fibrillation, cognition and dementia: A review. J. Cardiovasc. Electrophysiol. 2017, 28, 958–965. [Google Scholar] [CrossRef]
- Efimova, I.; Efimova, N.; Chernov, V.; Popov, S.; Lishmanov, Y. Ablation and pacing: Improving brain perfusion and cognitive function in patients with atrial fibrillation and uncontrolled ventricular rates. Pacing Clin. Electrophysiol. 2012, 35, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Nuzzi, R.; Dallorto, L.; Rolle, T. Changes of visual pathway and brain connectivity in glaucoma: A systematic review. Front. Neurosci. 2018, 12, 363. [Google Scholar] [CrossRef] [PubMed]
- Chouchou, F.; Mauguière, F.; Vallayer, O.; Catenoix, H.; Isnard, J.; Montavont, A.; Jung, J.; Pichot, V.; Rheims, S.; Mazzola, L. How the insula speaks to the heart: Cardiac responses to insular stimulation in humans. Hum. Brain Mapp. 2019, 40, 2611–2622. [Google Scholar] [CrossRef]
- Cechetto, D.F. Cortical control of the autonomic nervous system. Exp. Physiol. 2014, 99, 326–331. [Google Scholar] [CrossRef]
- Zhou, J.; Scherlag, B.J.; Edwards, J.; Jackman, W.M.; Lazzara, R.; Po, S.S. Gradients of atrial refractoriness and inducibility of atrial fibrillation due to stimulation of ganglionated plexi. J. Cardiovasc. Electrophysiol. 2007, 18, 83–90. [Google Scholar] [CrossRef]
- Chen, P.S.; Chen, L.S.; Fishbein, M.C.; Lin, S.F.; Nattel, S. Role of the autonomic nervous system in atrial fibrillation: Pathophysiology and therapy. Circ. Res. 2014, 114, 1500–1515. [Google Scholar] [CrossRef] [Green Version]
- ter Laan, M.; van Dijk, J.M.; Elting, J.W.; Staal, M.J.; Absalom, A.R. Sympathetic regulation of cerebral blood flow in humans: A review. Br. J. Anaesth. 2013, 111, 361–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imberti, F.J.; Ding, Y.W.; Kotalczyk, A.; Zhang, J.; Boriani, G.; Lip, G.; Andrade, J.; Gupta, D. Catheter ablation as first-line treatment for paroxysmal atrial fibrillation: A systematic review and meta-analysis. Heart 2021, 107, 1630–1636. [Google Scholar] [CrossRef] [PubMed]
- Ashburner, J.; Friston, K.J. Unified segmentation. Neuroimage 2005, 26, 839–851. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, H.; Tomita, H.; Taki, Y.; Kikuchi, Y.; Ono, C.; Yu, Z.; Sekiguchi, A.; Nouchi, R.; Kotozaki, Y.; Nakagawa, S.; et al. The VEGF gene polymorphism impacts brain volume and arterial blood volume. Hum. Brain Mapp. 2017, 38, 3516–3526. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Baseline | After AF Ablation | p Value | |
|---|---|---|---|
| Gender (M/F) | 2/6 | - | |
| Age (years) | 63.4 ± 7.3 (49–72) | - | |
| Heart rate (bpm) | 82.6 ± 29.3 (53–136) | 72.3 ± 15.5 (59–88) | 0.264 |
| LAD (mm) | 41.4 ± 6.6 (33.1–53.6) | 40.3 ± 6.7 (42.9–53.0) | 0.183 |
| LVDd (mm) | 46.7 ± 4.4 (40.7–52.6) | 45.8 ± 4.5 (41.4–47.5) | 0.116 |
| LVDs (mm) | 30.9 ± 4.0 (25.8–36.5) | 30.1 ± 3.6 (25.6–36.5) | 0.169 |
| EF (%) | 62.9 ± 6.0 (52.1–68.4) | 63.2 ± 4.9 (52.6–68.8) | 0.435 |
| LA volume (mL) | 75.8 ± 16.5 (50.7–99.0) | 74.6 ± 25.3 (55.8–124.0) | 0.405 |
| LA volume index (mL/m2) | 45.1 ± 8.0 (32.5–54.3) | 43.5 ± 11.3 (29.5–63.9) | 0.277 |
| CO (L/min) | 4.5 ± 0.8 (3.2–5.6) | 4.3 ± 0.9 (3.1–5.7) | 0.603 |
| CI (L/min/m2) | 2.7 ± 0.6 (1.7–3.3) | 2.6 ± 0.4 (1.9–3.0) | 0.720 |
| Serum BNP level (pg/mL) | 83.2 ± 71.9 (26.1–229.3) | 37.1 ± 29.0 (7.5–92.1) | 0.034 * |
| Objectives | NC Group | p Value (NC vs. Baseline) | AF Group | p Value (Pre vs. Post) | ||
|---|---|---|---|---|---|---|
| Pre | Post | |||||
| Gender (M/F) | 2/5 | 0.876 | 2/6 | |||
| Age | 63.0 ± 6.9 | 0.921 | 63.4 ± 7.3 | |||
| MMSE | Total cognitive function | 29.6 ± 0.5 | 0.015 * | 27.6 ± 1.7 | 28.9 ± 1.5 | 0.023 * |
| WAIS digit symbol | Executive function | 12.7 ± 1.0 | 0.157 | 11.3 ± 3.3 | 11.9 ± 4.0 | 0.008 * |
| WAIS digit span | Working Memory | 9.6 ± 0.7 | 0.666 | 10.0 ± 2.3 | 10.4 ± 3.5 | 0.267 |
| TMT-A (s) | Executive function | 66.6 ± 7.8 | 0.205 | 80.9 ± 25.9 | 73.7 ± 16.4 | 0.099 |
| TMT-B (s) | Executive function | 87.2 ± 16.5 | 0.393 | 106.5 ± 43.6 | 103.7 ± 33.0 | 0.148 |
| RAVLT | Verbal memory | |||||
| Recognition | 14.4 ± 1.0 | 0.032 | 11.1 ± 3.5 | 13.4 ± 1.3 | 0.078 | |
| Total recall | Immediate memory | 48.5 ± 3.0 | 0.066 | 39.3 ± 14.1 | 44.6 ± 15.2 | 0.023 * |
| Learning | 7.0 ± 0.6 | 1.000 | 7.0 ± 2.3 | 4.4 ± 2.0 | 0.954 | |
| Forgetting | Delayed recall | 2.5 ± 0.6 | 0.500 | 1.9 ± 2.3 | 1.4 ± 2.8 | 0.427 |
| CES-D | Depressive state | 6.8 ± 3.6 | 0.084 | 15.9 ± 10.8 | 13.5 ± 6.2 | 0.287 |
| STAI | Anxiety state | |||||
| Y1 | 32.6 ± 3.2 | 0.003 * | 48.5 ± 9.4 | 38.5 ± 8.8 | 0.004 * | |
| Y2 | 33.0 ± 4.4 | 0.008 * | 51.8 ± 12.8 | 47.8 ± 10.7 | 0.128 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tatewaki, Y.; Mutoh, T.; Sato, H.; Kobayashi, A.; Totsune, T.; Thyreau, B.; Sekiguchi, A.; Nakase, T.; Yagi, T.; Taki, Y. Impact of Catheter Ablation on Brain Microstructure and Blood Flow Alterations for Cognitive Improvements in Patients with Atrial Fibrillation: A Pilot Longitudinal Study. J. Clin. Med. 2022, 11, 4346. https://doi.org/10.3390/jcm11154346
Tatewaki Y, Mutoh T, Sato H, Kobayashi A, Totsune T, Thyreau B, Sekiguchi A, Nakase T, Yagi T, Taki Y. Impact of Catheter Ablation on Brain Microstructure and Blood Flow Alterations for Cognitive Improvements in Patients with Atrial Fibrillation: A Pilot Longitudinal Study. Journal of Clinical Medicine. 2022; 11(15):4346. https://doi.org/10.3390/jcm11154346
Chicago/Turabian StyleTatewaki, Yasuko, Tatsushi Mutoh, Hirokazu Sato, Akiko Kobayashi, Tomoko Totsune, Benjamin Thyreau, Atsushi Sekiguchi, Taizen Nakase, Tetsuo Yagi, and Yasuyuki Taki. 2022. "Impact of Catheter Ablation on Brain Microstructure and Blood Flow Alterations for Cognitive Improvements in Patients with Atrial Fibrillation: A Pilot Longitudinal Study" Journal of Clinical Medicine 11, no. 15: 4346. https://doi.org/10.3390/jcm11154346
APA StyleTatewaki, Y., Mutoh, T., Sato, H., Kobayashi, A., Totsune, T., Thyreau, B., Sekiguchi, A., Nakase, T., Yagi, T., & Taki, Y. (2022). Impact of Catheter Ablation on Brain Microstructure and Blood Flow Alterations for Cognitive Improvements in Patients with Atrial Fibrillation: A Pilot Longitudinal Study. Journal of Clinical Medicine, 11(15), 4346. https://doi.org/10.3390/jcm11154346