
Prediction of Tinnitus Perception Based on Daily Life MHealth Data Using Country Origin and Season




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- RQ1: Can momentary tinnitus (Question 1 of the daily EMA questionnaire; yes/no answer options) of TYT users be predicted (binary classifier trained) based on the following features: country, season, age, and sex from the baseline questionnaires as well as the following items of the daily EMA questionnaire: mood, arousal, stress, concentration, and the worst symptom perception. Note that, except for the prediction targets, the features used have been used in other analyses and have proven prediction power on this data set. To be more precise, we excluded features of TYT that are highly correlated with the target, such as tinnitus loudness, tinnitus stress, and momentary tinnitus. However, we included features that are known to be correlated with tinnitus, such as sex and age [16].
- RQ2: Can the reported tinnitus loudness of TYT users (Question 2 of the daily EMA questionnaire; slider question) be predicted (regressor be trained) based on the same features such as those used in RQ1?
- RQ3: Based on inferential statistics, are we able to reveal further country- and season-specific differences for the reported momentary tinnitus based on the daily EMA questionnaires of TYT users?
- RQ: Are there country-specific differences in momentary tinnitus?
- RQ: Are there season-specific differences in momentary tinnitus?
- RQ: In light of a combination of country- and season-specific differences, the question arises whether momentary tinnitus varies within the year and across countries.
- RQ: Another question is whether country- and season-specific differences in the reported worst symptom can be identified.
2. Materials and Methods
- I am feeling depressed because of the tinnitus.
- I find it harder to relax because of the tinnitus.
- I have strong worries because of the tinnitus.
- Because of the tinnitus it is difficult to follow a conversation, a piece of music or a film.
- Because of the tinnitus it is hard for me to get to sleep.
- Because of the tinnitus it is difficult to concentrate.
- Because of the tinnitus I am more irritable with my family, friends and colleagues.
- Because of the tinnitus I am more sensitive to environmental noises.
- I don’t have any of these symptoms.
2.1. Data Preprocessing
2.2. Gradient Boosting Machines for Classification and Regression
2.3. Features for RQ1 and RQ2
3. Results
3.1. RQ1: Is the Momentary Tinnitus of TYT Users Predictable Using the Features Country, Season, Age, Sex, and from the Daily EMA Questionnaire, Mood, Arousal, Stress, Concentration, and Worst Symptom Perception?
3.2. RQ2: Is the Reported Loudness of TYT Users Predictable Using the Same Features as in RQ1?
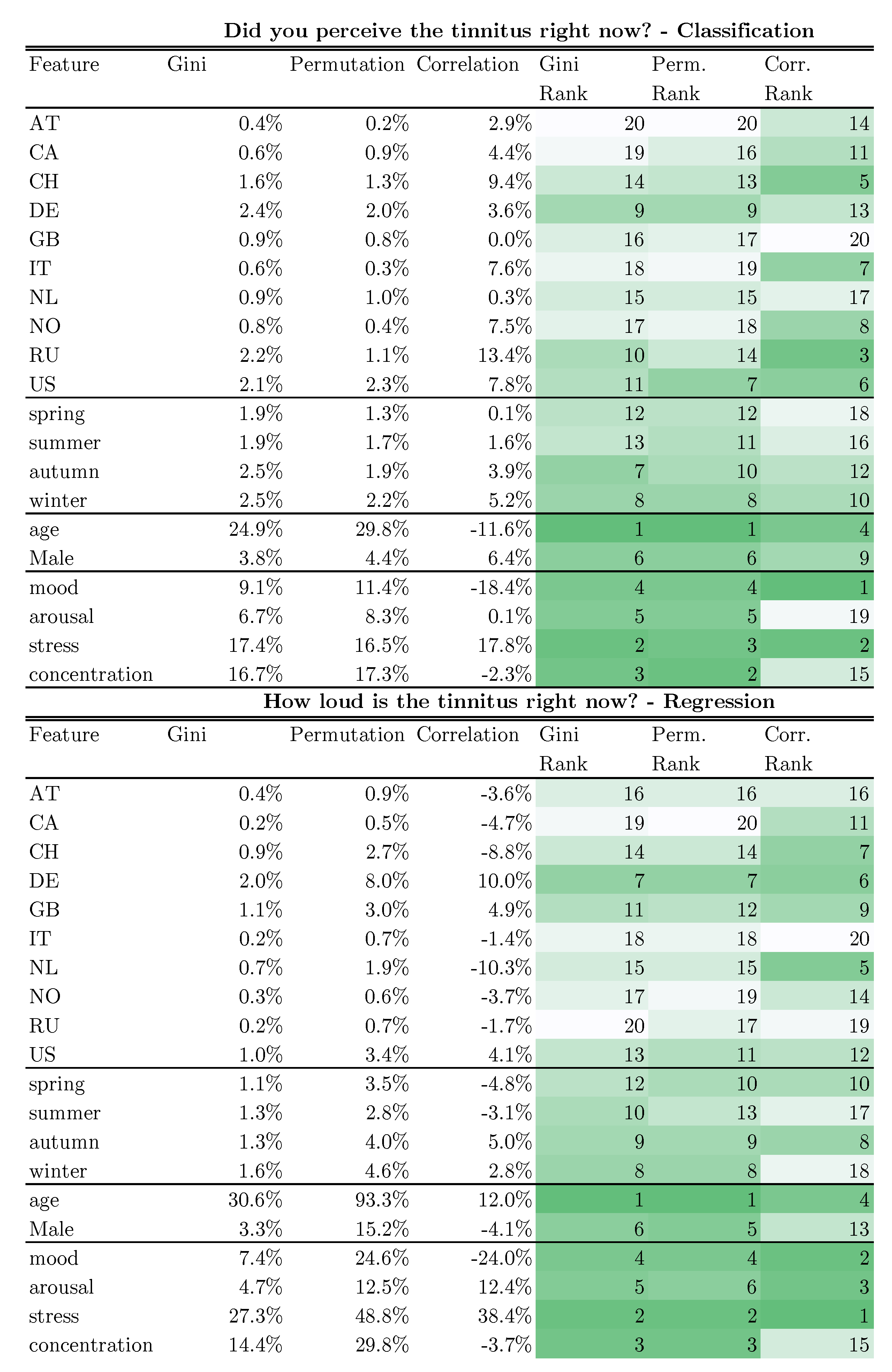
Feature Importance
3.3. RQ3: Are We Able to Reveal Country- and Season-Specific Differences for the Reported Momentary Tinnitus Based on the Daily Questionnaire of TYT Users?
- RQ: Are there country-specific differences for the momentary tinnitus?
- RQ: Are there season-specific differences for momentary tinnitus?
- RQ: In the Light of a Combination of Country- and Season-Specific Differences, does Momentary Tinnitus Vary within the Year and Across Countries?
- RQ: Can Country- and Season-Specific Differences in the Reported Worst Symptom be Identified?
4. Discussion
- For RQ1, we found that we can predict momentary tinnitus with an F1-score of 93.79% on the assessment level.
- For RQ2, we found that the tinnitus loudness can be regressed with a mean absolute error rate of 7.9%-points on a scale from 0 to 100%.
- For RQ (country specific differences for the momentary tinnitus), we found that most countries report momentary tinnitus differently.
- For RQ, we found season-specific differences in momentary tinnitus. If the data are not grouped by country, momentary tinnitus is most likely to occur in the summer. This is in contrast to the results of [7], where Tinnitus was most likely in summer. When we group our data by country, an ambiguous picture emerges between countries as to the most likely season for tinnitus.
- For RQ, we found that the momentary tinnitus does vary within the year and within countries. We found that this momentary tinnitus variance within one country is different from one country to another, i.e., if we compare Great Britain to the US.
- For RQ, we examined whether the distribution of the worst symptom changes between years or whether it is significantly different between countries. Our analysis showed that neither varied significantly, although the numbers suggest small differences.
- In our TYT data set, the country of users or the season in which an assessment was provided revealed a small prediction power for momentary tinnitus. The prediction power is better than guessing, and the statistical analyses showed differences between countries and seasons as well as within countries. This indicates that country- and season-specific differences should be considered when explaining inter- and intra-individual variance in tinnitus fluctuations.
- Self-reported mHealth data, which are collected globally with a longitudinal design, can contribute to the understanding of the biological mechanisms underlying tinnitus.
4.1. Performance Depends on Which Level We Split: Assessment Level vs. User Level
4.2. Feature Importance
4.3. The Temperature Dataset
4.4. Worst Season for Tinnitus
4.5. Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schlee, W.; Neff, P.; Simoes, J.; Langguth, B.; Schoisswohl, S.; Steinberger, H.; Norman, M.; Spiliopoulou, M.; Schobel, J.; Hannemann, R.; et al. Smartphone-guided educational counseling and self-help for chronic tinnitus. J. Clin. Med. 2022, 11, 1825. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, D.; Schlee, W.; Vanneste, S.; Londero, A.; Weisz, N.; Kleinjung, T.; Shekhawat, G.S.; Elgoyhen, A.B.; Song, J.J.; Andersson, G.; et al. Tinnitus and tinnitus disorder: Theoretical and operational definitions (an international multidisciplinary proposal). Prog. Brain Res. 2021, 260, 1–25. [Google Scholar] [PubMed]
- Langguth, B.; Kreuzer, P.M.; Kleinjung, T.; De Ridder, D. Tinnitus: Causes and clinical management. Lancet Neurol. 2013, 12, 920–930. [Google Scholar] [CrossRef]
- Izuhara, K.; Wada, K.; Nakamura, K.; Tamai, Y.; Tsuji, M.; Ito, Y.; Nagata, C. Association between tinnitus and sleep disorders in the general Japanese population. Ann. Otol. Rhinol. Laryngol. 2013, 122, 701–706. [Google Scholar] [CrossRef] [PubMed]
- McKenna, L.; Hallam, R.S.; Hinchcliffef, R. The prevalence of psychological disturbance in neuro-otology outpatients. Clin. Otolaryngol. Allied Sci. 1991, 16, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Mehdi, M.; Dode, A.; Pryss, R.; Schlee, W.; Reichert, M.; Hauck, F.J. Contemporary and Systematic Review of Smartphone Apps for Tinnitus Management and Treatment. Brain Sci. 2020, 10, 867. [Google Scholar] [CrossRef]
- Plante, D.T.; Ingram, D.G. Seasonal trends in tinnitus symptomatology: Evidence from Internet search engine query data. Eur. Arch.-Oto-Rhino-Laryngol. 2015, 272, 2807–2813. [Google Scholar] [CrossRef]
- Yang, A.C.; Huang, N.E.; Peng, C.K.; Tsai, S.J. Do seasons have an influence on the incidence of depression? The use of an internet search engine query data as a proxy of human affect. PLoS ONE 2010, 5, e13728. [Google Scholar] [CrossRef] [Green Version]
- Hilger, J.A. Autonomic dysfunction in the inner ear. Laryngoscope 1949, 59, 1–11. [Google Scholar] [CrossRef]
- Atkinson, M. Tinnitus aurium: Some considerations concerning its origin and treatment. Arch. Otolaryngol. 1947, 45, 68–76. [Google Scholar] [CrossRef]
- Miller, A.L. Epidemiology, etiology, and natural treatment of seasonal affective disorder. Altern. Med. Rev. 2005, 10, 5–13. [Google Scholar]
- Cederroth, C.R.; Schlee, W. Sex and Gender Differences in Tinnitus. Front. Neurosci. 2022, 59. [Google Scholar] [CrossRef]
- Van der Wal, A.; Luyten, T.; Cardon, E.; Jacquemin, L.; Vanderveken, O.M.; Topsakal, V.; Van de Heyning, P.; De Hertogh, W.; Van Looveren, N.; Van Rompaey, V.; et al. Sex differences in the response to different tinnitus treatment. Front. Neurosci. 2020, 14, 422. [Google Scholar] [CrossRef] [PubMed]
- Allgaier, J.; Schlee, W.; Langguth, B.; Probst, T.; Pryss, R. Predicting the gender of individuals with tinnitus based on daily life data of the TrackYourTinnitus mHealth platform. Sci. Rep. 2021, 11, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Basso, L.; Boecking, B.; Brueggemann, P.; Pedersen, N.L.; Canlon, B.; Cederroth, C.R.; Mazurek, B. Gender-specific risk factors and comorbidities of bothersome tinnitus. Front. Neurosci. 2020, 706. [Google Scholar] [CrossRef]
- Jafari, Z.; Kolb, B.E.; Mohajerani, M.H. Age-related hearing loss and tinnitus, dementia risk, and auditory amplification outcomes. Ageing Res. Rev. 2019, 56, 100963. [Google Scholar] [CrossRef] [PubMed]
- Mancini, P.C.; Tyler, R.S.; Smith, S.; Ji, H.; Perreau, A.; Mohr, A.M. Tinnitus: How partners can help? Am. J. Audiol. 2019, 28, 85–94. [Google Scholar] [CrossRef]
- Mavrogeni, P.; Maihoub, S.; Tamás, L.; Molnár, A. Tinnitus characteristics and associated variables on Tinnitus Handicap Inventory among a Hungarian population. J. Otol. 2022, 17, 136–139. [Google Scholar] [CrossRef]
- Biswas, R.; Lugo, A.; Akeroyd, M.A.; Schlee, W.; Gallus, S.; Hall, D. Tinnitus prevalence in Europe: A multi-country cross-sectional population study. Lancet Reg.-Health-Eur. 2022, 12, 100250. [Google Scholar] [CrossRef]
- Puga, C.; Niemann, U.; Unnikrishnan, V.; Schleicher, M.; Schlee, W.; Spiliopoulou, M. Discovery of Patient Phenotypes through Multi-layer Network Analysis on the Example of Tinnitus. In Proceedings of the 2021 IEEE 8th International Conference on Data Science and Advanced Analytics (DSAA), Online, 6–9 October 2021; pp. 1–10. [Google Scholar]
- Jamaludeen, N.; Unnikrishnan, V.; Pryss, R.; Schobel, J.; Schlee, W.; Spiliopoulou, M. Circadian Conditional Granger Causalities on Ecological Momentary Assessment Data from an mHealth App. In Proceedings of the 2021 IEEE 34th International Symposium on Computer-Based Medical Systems (CBMS), Online, 7–9 June 2021; pp. 354–359. [Google Scholar]
- Fioretti, A.; Natalini, E.; Riedl, D.; Moschen, R.; Eibenstein, A. Gender comparison of psychological comorbidities in tinnitus patients—Results of a cross-sectional study. Front. Neurosci. 2020, 704. [Google Scholar] [CrossRef]
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological momentary assessment. Annu. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Torous, J.; Friedman, R.; Keshavan, M. Smartphone ownership and interest in mobile applications to monitor symptoms of mental health conditions. JMIR mHealth uHealth 2014, 2, e2. [Google Scholar] [CrossRef]
- Martínez-Pérez, B.; De La Torre-Díez, I.; López-Coronado, M. Mobile health applications for the most prevalent conditions by the World Health Organization: Review and analysis. J. Med. Internet Res. 2013, 15, e120. [Google Scholar] [CrossRef] [PubMed]
- Schlee, W.; Kraft, R.; Schobel, J.; Langguth, B.; Probst, T.; Neff, P.; Reichert, M.; Pryss, R. Momentary assessment of tinnitus—How smart mobile applications advance our understanding of tinnitus. In Digital Phenotyping and Mobile Sensing; Springer: New York, NY, USA, 2019; pp. 209–220. [Google Scholar]
- Rowland, S.P.; Fitzgerald, J.E.; Holme, T.; Powell, J.; McGregor, A. What is the clinical value of mHealth for patients? NPJ Digit. Med. 2020, 3, 1–6. [Google Scholar] [CrossRef]
- Schlee, W.; Pryss, R.C.; Probst, T.; Schobel, J.; Bachmeier, A.; Reichert, M.; Langguth, B. Measuring the moment-to-moment variability of tinnitus: The TrackYourTinnitus smart phone app. Front. Aging Neurosci. 2016, 8, 294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, S.H.; Powers, B.W.; Hawkins, J.B.; Brownstein, J.S. The digital phenotype. Nat. Biotechnol. 2015, 33, 462–463. [Google Scholar] [CrossRef]
- Unnikrishnan, V.; Schleicher, M.; Shah, Y.; Jamaludeen, N.; Pryss, R.; Schobel, J.; Kraft, R.; Schlee, W.; Spiliopoulou, M. The Effect of Non-Personalised Tips on the Continued Use of Self-Monitoring mHealth Applications. Brain Sci. 2020, 10, 924. [Google Scholar] [CrossRef] [PubMed]
- Pryss, R. Mobile crowdsensing in healthcare scenarios: Taxonomy, conceptual pillars, smart mobile crowdsensing services. In Digital Phenotyping and Mobile Sensing; Springer: New York, NY, USA, 2019; pp. 221–234. [Google Scholar]
- Kraft, R.; Schlee, W.; Stach, M.; Reichert, M.; Langguth, B.; Baumeister, H.; Probst, T.; Hannemann, R.; Pryss, R. Combining Mobile Crowdsensing and Ecological Momentary Assessments in the Healthcare Domain. Front. Neurosci. 2020, 14, 164. [Google Scholar] [CrossRef]
- Probst, T.; Pryss, R.; Langguth, B.; Schlee, W. Emotional states as mediators between tinnitus loudness and tinnitus distress in daily life: Results from the “TrackYourTinnitus” application. Sci. Rep. 2016, 6, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Pryss, R.; Probst, T.; Schlee, W.; Schobel, J.; Langguth, B.; Neff, P.; Spiliopoulou, M.; Reichert, M. Prospective crowdsensing versus retrospective ratings of tinnitus variability and tinnitus–stress associations based on the TrackYourTinnitus mobile platform. Int. J. Data Sci. Anal. 2019, 8, 327–338. [Google Scholar] [CrossRef] [Green Version]
- Kraft, R.; Stach, M.; Reichert, M.; Schlee, W.; Probst, T.; Langguth, B.; Schickler, M.; Baumeister, H.; Pryss, R. Comprehensive insights into the TrackYourTinnitus database. Procedia Comput. Sci. 2020, 175, 28–35. [Google Scholar] [CrossRef]
- Sereda, M.; Smith, S.; Newton, K.; Stockdale, D. Mobile apps for management of tinnitus: Users’ survey, quality assessment, and content analysis. JMIR mHealth uHealth 2019, 7, e10353. [Google Scholar] [CrossRef] [PubMed]
- Mehdi, M.; Riha, C.; Neff, P.; Dode, A.; Pryss, R.; Schlee, W.; Reichert, M.; Hauck, F.J. Smartphone Apps in the Context of Tinnitus: Systematic Review. Sensors 2020, 20, 1725. [Google Scholar] [CrossRef] [Green Version]
- Unnikrishnan, V.; Shah, Y.; Schleicher, M.; Strandzheva, M.; Dimitrov, P.; Velikova, D.; Pryss, R.; Schobel, J.; Schlee, W.; Spiliopoulou, M. Predicting the Health Condition of mHealth App Users with Large Differences in the Number of Recorded Observations-Where to Learn from? In Proceedings of the International Conference on Discovery Science, Thessaloniki, Greece, 19–21 October 2020; pp. 659–673. [Google Scholar]
- Aguilera, A.; Figueroa, C.A.; Hernandez-Ramos, R.; Sarkar, U.; Cemballi, A.; Gomez-Pathak, L.; Miramontes, J.; Yom-Tov, E.; Chakraborty, B.; Yan, X.; et al. mHealth app using machine learning to increase physical activity in diabetes and depression: Clinical trial protocol for the DIAMANTE Study. BMJ Open 2020, 10, e034723. [Google Scholar] [CrossRef]
- Said, A.B.; Mohamed, A.; Elfouly, T.; Abualsaud, K.; Harras, K. Deep learning and low rank dictionary model for mhealth data classification. In Proceedings of the 2018 14th International Wireless Communications & Mobile Computing Conference (IWCMC), Limassol, Cyprus, 25–29 June 2018; pp. 358–363. [Google Scholar]
- Qureshi, K.N.; Din, S.; Jeon, G.; Piccialli, F. An accurate and dynamic predictive model for a smart M-Health system using machine learning. Inf. Sci. 2020, 538, 486–502. [Google Scholar] [CrossRef]
- Cheung, Y.K.; Hsueh, P.Y.S.; Qian, M.; Yoon, S.; Meli, L.; Diaz, K.M.; Schwartz, J.E.; Kronish, I.M.; Davidson, K.W. Are nomothetic or ideographic approaches superior in predicting daily exercise behaviors? Analyzing N-of-1 mHealth data. Methods Inf. Med. 2017, 56, 452. [Google Scholar] [PubMed]
- Bergsma, W. A bias-correction for Cramér’s V and Tschuprow’s T. J. Korean Stat. Soc. 2013, 42, 323–328. [Google Scholar] [CrossRef]
- Tate, R.F. Correlation between a discrete and a continuous variable. Point-biserial correlation. Ann. Math. Stat. 1954, 25, 603–607. [Google Scholar] [CrossRef]
- Friedman, J.H. Greedy function approximation: A gradient boosting machine. Ann. Stat. 2001, 29, 1189–1232. [Google Scholar] [CrossRef]
- Schlee, W.; Simoes, J.; Pryss, R. Auricular Acupressure combined with self-help intervention for treating chronic tinnitus: A longitudinal observational study. J. Clin. Med. 2021, 10, 4201. [Google Scholar] [CrossRef]
- Kim, Y.H. Seasonal affective disorder in patients with chronic tinnitus. Laryngoscope 2016, 126, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Niemann, U.; Boecking, B.; Brueggemann, P.; Mazurek, B.; Spiliopoulou, M. Gender-Specific Differences in Patients With Chronic Tinnitus—Baseline Characteristics and Treatment Effects. Front. Neurosci. 2020, 14, 487. [Google Scholar] [CrossRef] [PubMed]
- Schlee, W.; Hall, D.A.; Canlon, B.; Cima, R.F.; de Kleine, E.; Hauck, F.; Huber, A.; Gallus, S.; Kleinjung, T.; Kypraios, T.; et al. Innovations in doctoral training and research on tinnitus: The European School on Interdisciplinary Tinnitus Research (ESIT) Perspective. Front. Aging Neurosci. 2018, 9, 447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlee, W.; Schoisswohl, S.; Staudinger, S.; Schiller, A.; Lehner, A.; Langguth, B.; Schecklmann, M.; Simoes, J.; Neff, P.; Marcrum, S.C.; et al. Towards a unification of treatments and interventions for tinnitus patients: The EU research and innovation action UNITI. In Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2021; Volume 260, pp. 441–451. [Google Scholar]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allgaier, J.; Schlee, W.; Probst, T.; Pryss, R. Prediction of Tinnitus Perception Based on Daily Life MHealth Data Using Country Origin and Season. J. Clin. Med. 2022, 11, 4270. https://doi.org/10.3390/jcm11154270
Allgaier J, Schlee W, Probst T, Pryss R. Prediction of Tinnitus Perception Based on Daily Life MHealth Data Using Country Origin and Season. Journal of Clinical Medicine. 2022; 11(15):4270. https://doi.org/10.3390/jcm11154270
Chicago/Turabian StyleAllgaier, Johannes, Winfried Schlee, Thomas Probst, and Rüdiger Pryss. 2022. "Prediction of Tinnitus Perception Based on Daily Life MHealth Data Using Country Origin and Season" Journal of Clinical Medicine 11, no. 15: 4270. https://doi.org/10.3390/jcm11154270
APA StyleAllgaier, J., Schlee, W., Probst, T., & Pryss, R. (2022). Prediction of Tinnitus Perception Based on Daily Life MHealth Data Using Country Origin and Season. Journal of Clinical Medicine, 11(15), 4270. https://doi.org/10.3390/jcm11154270