
The Effects of Physiotherapy in the Treatment of Cubital Tunnel Syndrome: A Systematic Review

 ,
,  ,
, 

Abstract
:1. Introduction
2. Methods
2.1. Data Sources and Searchers
- P (population)—cubital tunnel syndrome;
- I (intervention)—physiotherapy treatment;
- C (comparator)—control group, placebo group, and sham therapy;
- O (outcomes)—nerve conduction study, discrimination and threshold sensation, functional assessment, and ultrasound imaging measurements (Supplementary Material S1).
2.2. Study Selection
2.3. Data Extraction
2.4. Methodological Quality Assessment
2.5. Data Synthesis and Analysis
3. Results
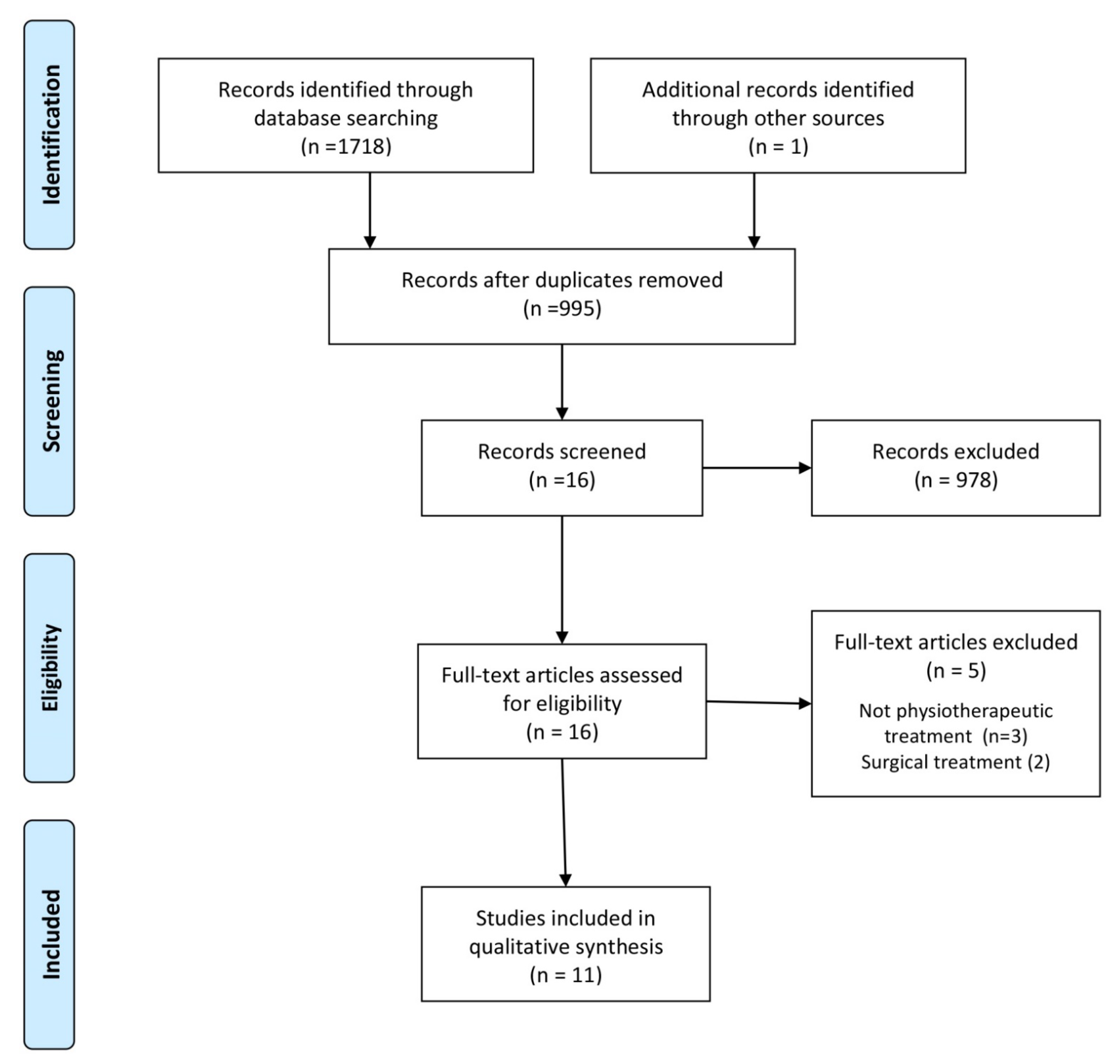
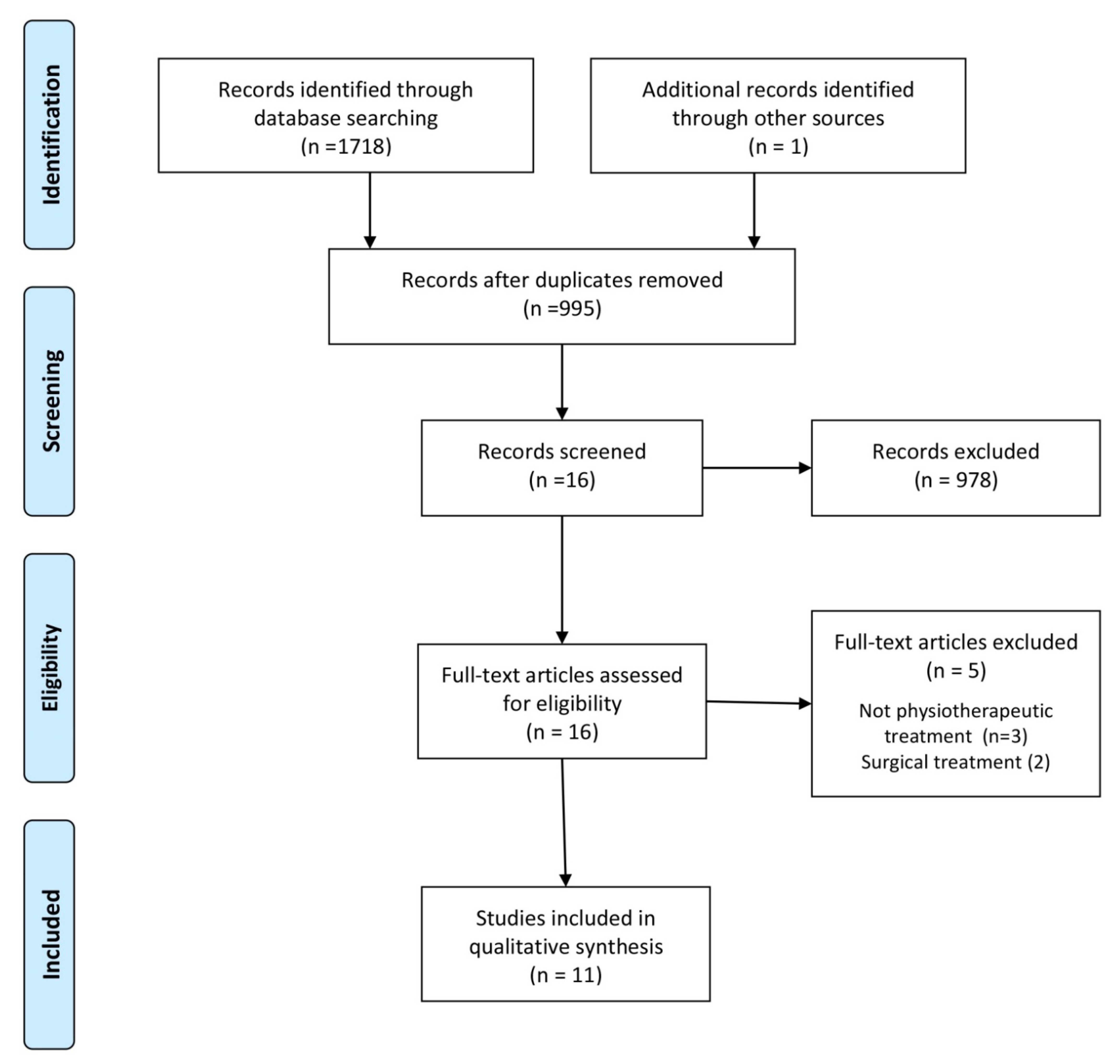
3.1. Study Selection
3.2. Randomised Controlled Trials
3.2.1. Participants
3.2.2. Outcome Measures
3.2.3. Interventions
3.2.4. Risk of Bias
3.2.5. Synthesis of the Results
3.3. Case Studies
3.3.1. Outcome Measures
3.3.2. Interventions
3.3.3. Therapeutic Effect
3.3.4. Risk of Bias
4. Discussion
4.1. Limitations
4.2. Implications for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Elhassan, B.; Steinmann, S.P. Entrapment neuropathy of the ulnar nerve. J. Am. Acad. Orthop. Surg. 2007, 15, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Robertson, C.; Saratsiotis, J. A review of compression ulnar neuropathy at the elbow. J. Manip. Physiol. Ther. 2005, 28, 345. [Google Scholar] [CrossRef] [PubMed]
- Mondelli, M.; Giannini, F.; Ballerini, M.; Ginanneschi, F.; Martorelli, M. Incidence of ulnar neuropathy at the elbow in the province of Siena (Italy). J. Neurol. Sci. 2005, 234, 5–10. [Google Scholar] [CrossRef] [PubMed]
- An, T.W.; Evanoff, B.A.; Boyer, M.I.; Osei, D.A. The Prevalence of Cubital Tunnel Syndrome: A Cross-Sectional Study in a U.S. Metropolitan Cohort. J. Bone Jt. Surg. 2017, 99, 408–416. [Google Scholar] [CrossRef] [Green Version]
- Kooner, S.; Cinats, D.; Kwong, C.; Matthewson, G.; Dhaliwal, G. Conservative treatment of cubital tunnel syndrome: A systematic review. Orthop. Rev. 2019, 11, 7955. [Google Scholar] [CrossRef] [Green Version]
- McGowan, J. The results of transposition of the ulnar nerve for traumatic ulnar neuritis. J. Bone Jt. Surg. Br. 1950, 32, 293–301. [Google Scholar] [CrossRef]
- Ochiai, N.; Honmo, J.; Tsunjino, A.; Nisiura, Y. Electrodiagnosis in entrapment neuropathy by the arcade of struthers. Clin. Orthop. Relat. Res. 2001, 378, 129–135. [Google Scholar] [CrossRef]
- Sunderland, S. Nerves and Nerve Injuries; Churchill Livingstone: Edinburgh, UK; London, UK; New York, NY, USA, 1978. [Google Scholar]
- Assmus, H.; Antoniadis, G.; Bischoff, C.; Hoffmann, R.; Martini, A.-K.; Preissler, K.; Scheglmann, K.; Schwerdtfeger, K.; Wessels, K.D.; Wustner-Hofmann, M. Cubital tunnel syndrome—a review and management guidelines. Cent. Eur. Neurosurg. 2011, 72, 90–98. [Google Scholar] [CrossRef]
- Palmer, B.A.; Hughes, T.B. Cubital tunnel syndrome. J. Hand Surg. Am. 2010, 35, 153–163. [Google Scholar] [CrossRef]
- Bartels, R.H.; Verbeek, A.L. Risk factors for ulnar nerve compression at the elbow: A case control study. Acta Neurochir. 2007, 149, 669–674. [Google Scholar] [CrossRef] [Green Version]
- Cutts, S. Cubital tunnel syndrome. Postgrad. Med. J. 2007, 83, 28–31. [Google Scholar] [CrossRef] [PubMed]
- Svernlov, B.; Larsson, M.; Rehn, K.; Adolfsson, L. Conservative treatment of the cubital tunnel syndrome. J. Hand Surg. 2009, 34B, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Lund, A.T.; Amadio, P.C. Treatment of cubital tunel syndrome: Perspectives for the therapist. J. Hand Ther. 2006, 19, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Wolny, T.; Saulicz, E.; Linek, P.; Shacklock, M.; Myśliwiec, A. Efficacy of Manual Therapy Including Neurodynamic Techniques for the Treatment of Carpal Tunnel Syndrome: A Randomized Controlled Trial. J. Manip. Physiol. Ther. 2017, 40, 263–272. [Google Scholar] [CrossRef]
- Wolny, T.; Linek, P. Neurodynamic Techniques Versus “Sham” Therapy in the Treatment of Carpal Tunnel Syndrome: A Randomized Placebo-Controlled Trial. Arch. Phys. Med. Rehabil. 2018, 99, 843–854. [Google Scholar] [CrossRef]
- Wolny, T.; Linek, P. Is manual therapy based on neurodynamic techniques effective in the treatment of carpal tunnel syndrome? A randomized controlled trial. Clin. Rehabil. 2019, 33, 408–417. [Google Scholar] [CrossRef]
- Wolny, T.; Linek, P. Long-term patient observation after conservative treatment of carpal tunnel syndrome: A summary of two randomised controlled trials. PeerJ 2019, 7, e8012. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Cleland, J.; Palacios-Ceña, M.; Fuensalida-Novo, S.; Alonso-Blanco, C.; Pareja, J.A.; Alburquerque-Sendín, F. Effectiveness of manual therapy versus surgery in pain processing due to carpal tunnel syndrome: A randomized clinical trial. Eur. J. Pain 2017, 21, 1266–1276. [Google Scholar] [CrossRef] [Green Version]
- Kearns, G.L.; Wang, S. Medical diagnosis of cubital tunnel syndrome ameliorated with thrust manipulation of the elbow and carpals. J. Man. Manip. Ther. 2012, 20, 90–95. [Google Scholar] [CrossRef] [Green Version]
- Oskay, D.; Meriç, A.; Nuray, K.; Firat, T.; Ayhan, C.; Leblebicioğlu, G. Neurodynamic mobilization in the conservative treatment of cubital tunnel syndrome: Long-term follow-up of 7 cases. J. Manip. Physiol. Ther. 2010, 33, 156–163. [Google Scholar] [CrossRef]
- Shen, Y.P.; Wu, Y.Y.; Chu, H.Y.; Li, T.Y.; Chen, L.C.; Wu, Y.T. Extracorporeal shock wave therapy in cubital tunnel syndrome: A pilot study. Neurol. Asia 2018, 23, 233–238. [Google Scholar]
- Anandkumar, S.; Manivasagam, M. Effect of dry needling on cubital tunnel syndrome: Three case reports. Physiother. Theory Pract. 2019, 35, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preffered Reporting Items for Systematic Reviews and Mata-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centre for Reviews and Dissemination. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care; University of York: York, UK, 2008. [Google Scholar]
- Risk of Bias Tools—Current Version of RoB 2. Available online: https://www.riskofbias.info/welcome/rob-2-0-tool (accessed on 8 April 2021).
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetc, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic reviews of etiology and risk. In Joanna Briggs Institute Reviewer’s Manual 2017; Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Badur, N.B.; Ozkan, F.U.; Aktas, I. Efficacy of shortwave diathermy in ulnar nerve entrapment at the elbow: A double-blind randomized controlled clinical trial. Clin. Rehabil. 2020, 34, 1048–1055. [Google Scholar] [CrossRef]
- Ozkan, F.U.; Saygi, E.K.; Senol, S.; Kapci, S.; Aydeniz, B.; Aktas, I.; Gozke, E. New treatment alternatives in the ulnar neuropathy at the elbow: Ultrasound and low-level laser therapy. Acta Neurol. Belg. 2015, 115, 355–360. [Google Scholar] [CrossRef]
- Illes, J.D.; Johnson, T.L., Jr. Chiropractic management of a patient with ulnar nerve compression symptoms: A case report. J. Chirop. Med. 2013, 12, 66–73. [Google Scholar] [CrossRef] [Green Version]
- Coppieters, M.W.; Bartholomeeusen, K.E.; Stappaerts, K.H. Incorporating nerve-gliding techniques in the conservative treatment of cubital tunnel syndrome. J. Manip. Physiol. Ther. 2004, 27, 560–568. [Google Scholar] [CrossRef]
- Kwak, S.; Daeun, J.; Choo, Y.J.; Chang, M.C. Management of neuropathic pain induced by cubital tunnel syndrome using pulsed radiofrequency: Two case report. Medicine 2019, 98, e15599. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Arias-Buría, J.L.; El Bachiri, Y.R.; Plaza-Manzano, G.; Cleland, J.A. Ultrasound-guided percutaneous electrical stimulation for a patient with cubital tunnel syndrome: A case report with a one-year follow-up. Physiother. Theory Pract. 2020, 6, 1–6. [Google Scholar] [CrossRef]
- Johnson, E.W. Diagnosis of carpal tunnel syndrome. The gold standard. Am. J. Phys. Med. Rehabil. 1993, 72, 1. [Google Scholar] [CrossRef] [PubMed]
- David, C.; Preston, D.C.; Barbara, E.; Shapiro, B.E. Electromyography and Neuromuscular Disorders. Clinical-Electrophysiologic Correlations, 2nd ed.; Elsevier: Philadelphia, PA, USA, 1998. [Google Scholar]
- Nee, R.J.; Jull, G.A.; Vicenzino, B.; Coppieters, M.W. The validity of upper-limb neurodynamic tests for detecting peripheral neuropathic pain. J. Orthop. Sports Phys. Therapy 2012, 42, 413–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novak, C.B.; Lee, G.W.; Mackinnon, S.E.; Lay, L. Provocative testing for cubital tunnel syndrome. J. Hand Surg. 1994, 19, 817–820. [Google Scholar] [CrossRef]
- Gillard, J.; Perez-Cousin, M.; Hachulla, E.; Remy, J.; Hurtevent, J.F.; Vinckier, L. Diagnosis thoracic outlet syndrome: Contribution of provocative test, ultrasonography, electrophysiology, and helical computed tomography in 48 patient. Jt. Bone Spine 2001, 68, 416–424. [Google Scholar] [CrossRef]
- Carlson, H.; Colbert, A.; Frydl, J.; Arnall, E.; Elliot, M.; Carlson, M. Current options for nonsurgical management of carpal tunnel syndrome. Int. J. Clin. Rheumtol. 2010, 5, 129–142. [Google Scholar] [CrossRef] [Green Version]
- Chang, M.H.; Chiang, H.T.; Ger, L.P.; Yang, D.A.; Lo, Y.K. The cause of slowed forearm median conduction velocity in carpal tunnel syndrome. Clin. Neurophysiol. 2000, 111, 1039–1044. [Google Scholar] [CrossRef]

{kind=link}
| Study | Participants | Outcome Measures | Control/ Comparison | Intervention | Results |
|---|---|---|---|---|---|
| Svernlov et al. [13] | n = 70 Sex: 39 female; 31 male Age: 17–72 | Measurement at baseline and 6-month follow-up; Activities scale (COPM); Grip strength (JAMAR dynamometer); Pain (VAS); Neurophysiological examination (NCS, electromyography). | Three groups | Group A—elbow orthosis (3-month treatment); Group B—nerve gliding exercises (3-month treatment); Group C—information (exercise modification). | There was a significant improvement in each group after the applied therapy. There were no between-group differences. |
| Badur et al. [29] | n = 61 Sex: 32 female; 29 male Age: 16–79 | Measurement at baseline, after treatment, and 1- and 3-month follow-up; Pain (VAS); Upper-extremity disability and symptoms (DASH); Overall health (SF-36 questionnaire); Grip strength (dynamometer). | Two groups | Group 1—continuous shortwave diathermy (10 treatments); Group 2—placebo shortwave diathermy (10 treatments). | There were no changes in the assessed parameters in both groups after the applied therapy. |
| Ozkan et al. [30] | n = 32 Sex: 16 female; 16 male Age: mean = 43.5 | Measurement at baseline, after treatment, and 1- and 3-month follow-up; Pain (VAS); Grip strength (dynamometer); Sensory threshold (Semmes–Weinstein monofilament test; Neurophysiological examination (NCS); patient satisfaction scale. | Two groups | Group 1—low-level laser therapy (10 treatments); Group 2—ultrasound therapy (10 treatments). | There was a significant improvement in both groups after the applied therapy. There were no between-group. |
| Study | Participants | Outcome Measures | Control/ Comparison | Intervention | Results |
|---|---|---|---|---|---|
| Kearns and Wang [20] | n = 1 Sex: female Age: 45 | Measured at baseline and 4 weeks post-treatment; Tissue tension (STTT); range of motion (goniometer); symptom provocation (ULTT, elbow flexion test); structural dysfunction (PAM); pain (NPRS). | No | Thrust manipulation (humeroulnar joint 2 treatments, radiocarpal joint 1 treatment). | After 3 treatment sessions, pain and paraesthesia were resolved; all other tests were negative. |
| Oskay et al. [21] | n = 7 Sex: not specified Age range: 35–70 | Measured at baseline, after treatment, and 12-month follow-up; Symptom provocation (elbow flexion test); palmar gripping and grasping (pinchmeter and grip dynamometer); pain (VAS); loss of sensation (Semmes–Weinstein monofilaments); upper-extremity disability and symptoms (DASH). | No | Cold application; pulsed ultrasound (10 treatments); nerve mobilisation techniques (10 treatments); strengthening exercises; postural adaptations; education; ergonomic modifications. | Pain, Tinel’s sign, and Disability of Arm, Shoulder, and Hand Index scores were decreased; grip and pinch strength increased during the observation period. |
| Shen et al. [22] | n = 7 Sex: not specified Age: 35–71 | Measured at baseline and 4-, 8-, and 12-week follow-up; Severity of paraesthesia/dysaesthesia (VAS); upper-extremity disability and symptoms (DASH). | No | Extracorporeal shock wave therapy (3 treatments). | The VAS and Quick DASH scores demonstrated improvements at all follow-up time points in all treated elbows. |
| Anandkumar and Manivasagam [23] | n = 3 Sex: 2 male; 1 female Age: 35,45,50 | Measured at baseline, beginning of each treatment session, and at 6-month follow-up; Pain (NPRS); function limitation (PSFS); pain-free grip strength (JAMAR dynamometer); self-reported outcome measure (GROC). | No | Dry needling (4 treatments, twice a week). | All patients achieved complete pain reduction and full recovery of function; the strength of the pain-free grip also improved; all self-reported significant improvement after therapy; the effect lasted 6 months after the therapy. |
| Illes and Johnson [31] | n = 1 Sex: female Age: 41 | Measured at baseline and after treatment; Severity of numbness (VAS); Symptom provocation (EAST, Tinel sign); Grip strength (Blood pressure cuff); | No | Chiropractic manipulative therapy; myofascial therapy (11 treatments); elastic therapeutic taping (no number specified); home exercises (8 treatments). | After 11 treatment sessions, symptoms resolved completely. |
| Coppieters et al. [32] | n = 1 Sex: female Age: 17 | Measured at baseline, beginning of each treatment session, and at 6- and 10-month follow-up; Pain (VAS); range of motion (goniometer); clinical tests (neural provocation test, elbow flexion test, Tinel’s sign); functional status (NPQ). | No | Neurodynamic mobilisation (5 treatments); Elbow mobilisation (4 treatments); home exercises—active ulnar nerve-sliding (5 treatments); high-velocity distraction/rotation thrust (3 treatments); education (1 instruction). | After the applied therapy, in each of the tests used, the symptoms were eliminated; The effect lasted 10 months after the therapy. |
| Kwak et al. [33] | n = 2 Sex: male Age: 39 and 40 | Measured at baseline, after treatment, and at 1, 2, 3, and 6 months post-treatment; Pain (NPRS); NCS; elbow imaging (MRI). | No | PRF (1 treatment). | After 1 treatment session, the pain was completely relieved. At the 1-, 2-, 3-, and 6-month follow-up assessments after the procedure, the previously reported pain had not recurred. |
| Fernández-de-Las-Peñas al. [34] | n = 1 Sex: male Age: 48 | Measured at baseline and at 1, 3, 6, and 12 months post-treatment; Upper-extremity disability and symptoms (DASH); neuropathic pain (S-LANSS); self-reported outcome measure (GROC). | No | PENS of the ulnar nerve (3 treatments); self-neural glides as a home program (2–3 weeks). | After three treatment sessions, there was an elimination of pain and symptoms and an improvement in functional status; the effect lasted 12 months after the therapy. |
| Study | Domain 1 Risk of Bias Arising from the Randomisation Process | Domain 2 Risk of Bias Due to Deviations from the Intended Interventions | Domain 3 Missing Outcome Data | Domain 4 Risk of Bias in Measurement of the Outcome | Domain 5 Risk of Bias in Selection of the Reported Result | Overall Risk of Bias |
|---|---|---|---|---|---|---|
| Svernlov et al. [13] | Low | Some concerns | Low | High | Low | High |
| Badur et al. [29] | Low | Some concerns | Low | Low | Low | Some concerns |
| Ozkan et al. [30] | Low | Some concerns | Low | Low | Low | Some concerns |
| Critical Appraisal Checklist | Kearns and Wang [20] | Oskay et al. [21] | Shen et al. [22] | Anandkumar and Manivasagam [23] | Illes and Johnson [31] | Coppieters et al. [32] | Kwak et al. [33] | Fernández-de-Las-Peñas et al. [34] |
|---|---|---|---|---|---|---|---|---|
| 1. Were the patient’s demographic characteristics clearly described? | Yes | Unclear | Yes | Yes | Yes | Yes | Yes | Yes |
| 2. Was the patient’s history clearly described and presented as a timeline? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 3. Was the current clinical condition of the patient on presentation clearly described? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 4. Were diagnostic tests or assessment methods and the results clearly described? | Unclear | Yes | Yes | Unclear | Unclear | Unclear | Yes | Unclear |
| 5. Was the intervention(s) or treatment procedure(s) clearly described? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 6. Was the post-intervention clinical condition clearly described? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 7. Were adverse events (harms) or unanticipated events identified and described? | No | Unclear | Unclear | Unclear | No | Unclear | Unclear | No |
| 8. Does the case report provide takeaway lessons? | No | Yes | Yes | Yes | No | No | Yes | Unclear |
| Study | Bias Due to Confounding | Bias in Selection of Participants in the Study | Bias in Classification of Interventions | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of the Reported Result | Overall Bias |
|---|---|---|---|---|---|---|---|---|
| Kearns and Wang [20] | Serious | Moderate | Serious | Serious | Moderate | Serious | Moderate | Serious |
| Oskay et al. [21] | Serious | Moderate | Serious | Serious | Moderate | Serious | Moderate | Serious |
| Shen et al. [22] | Moderate | Low | Moderate | Moderate | Low | Moderate | Moderate | Moderate |
| Anandkumar and Manivasagam [23] | Moderate | Low | Moderate | Moderate | Low | Moderate | Moderate | Moderate |
| Illes and Johnson [31] | Serious | Moderate | Serious | Serious | Moderate | Serious | Moderate | Serious |
| Coppieters et al. [32] | Serious | Moderate | Serious | Serious | Moderate | Serious | Moderate | Serious |
| Kwak et al. [33] | Moderate | Low | Moderate | Moderate | Low | Moderate | Moderate | Moderate |
| Fernández-de-Las-Peñas et al. [34] | Serious | Moderate | Serious | Serious | Moderate | Serious | Moderate | Serious |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolny, T.; Fernández-de-las Peñas, C.; Buczek, T.; Domin, M.; Granek, A.; Linek, P. The Effects of Physiotherapy in the Treatment of Cubital Tunnel Syndrome: A Systematic Review. J. Clin. Med. 2022, 11, 4247. https://doi.org/10.3390/jcm11144247
Wolny T, Fernández-de-las Peñas C, Buczek T, Domin M, Granek A, Linek P. The Effects of Physiotherapy in the Treatment of Cubital Tunnel Syndrome: A Systematic Review. Journal of Clinical Medicine. 2022; 11(14):4247. https://doi.org/10.3390/jcm11144247
Chicago/Turabian StyleWolny, Tomasz, César Fernández-de-las Peñas, Tomasz Buczek, Magdalena Domin, Arkadiusz Granek, and Paweł Linek. 2022. "The Effects of Physiotherapy in the Treatment of Cubital Tunnel Syndrome: A Systematic Review" Journal of Clinical Medicine 11, no. 14: 4247. https://doi.org/10.3390/jcm11144247
APA StyleWolny, T., Fernández-de-las Peñas, C., Buczek, T., Domin, M., Granek, A., & Linek, P. (2022). The Effects of Physiotherapy in the Treatment of Cubital Tunnel Syndrome: A Systematic Review. Journal of Clinical Medicine, 11(14), 4247. https://doi.org/10.3390/jcm11144247