
The Presence of Bacteremia Indicates Higher Inflammatory Response and Augments Disease Severity in Adult Patients with Urinary Tract Infections

Abstract
:1. Introduction
2. Methods
2.1. Patient Selection and Sample Collection
- (1)
- Symptomatic criteria: Any one of the following urinary symptoms were present: dysuria, frequency, urgency, hematuria, flank pain, back pain, suprapubic pain, costovertebral tenderness on physical examination, and nonspecific symptoms. These nonspecific symptoms included nausea, vomiting, loss of appetite, shortness of breath, abdominal tenderness, or mental or functional deterioration while no other obvious infection was discovered [1,3].
- (2)
- (3)
- Microbiological criteria: The microbiological results of the urine culture performed in the ED were positive. A positive result was defined as an organism grown in a quantitative urine culture with a concentration of >105 colony-forming units/mL [11].
- (1)
- Concomitant infectious diseases were observed during hospitalization.
- (2)
- The patient did not undergo blood culture in the ED.
- (3)
- The microbiological results of blood culture and urine culture of the patient were discordant.
- (4)
- The urine culture or blood culture were contaminated, and the isolated pathogens included coagulase-negative staphylococci, Bacillus species, Corynebacterium species, micrococci, and Propionibacterium species [13].
2.2. Comparison of Outcomes and Clinical Features between the Groups
2.3. Statistical Analysis and Study Approval
3. Results
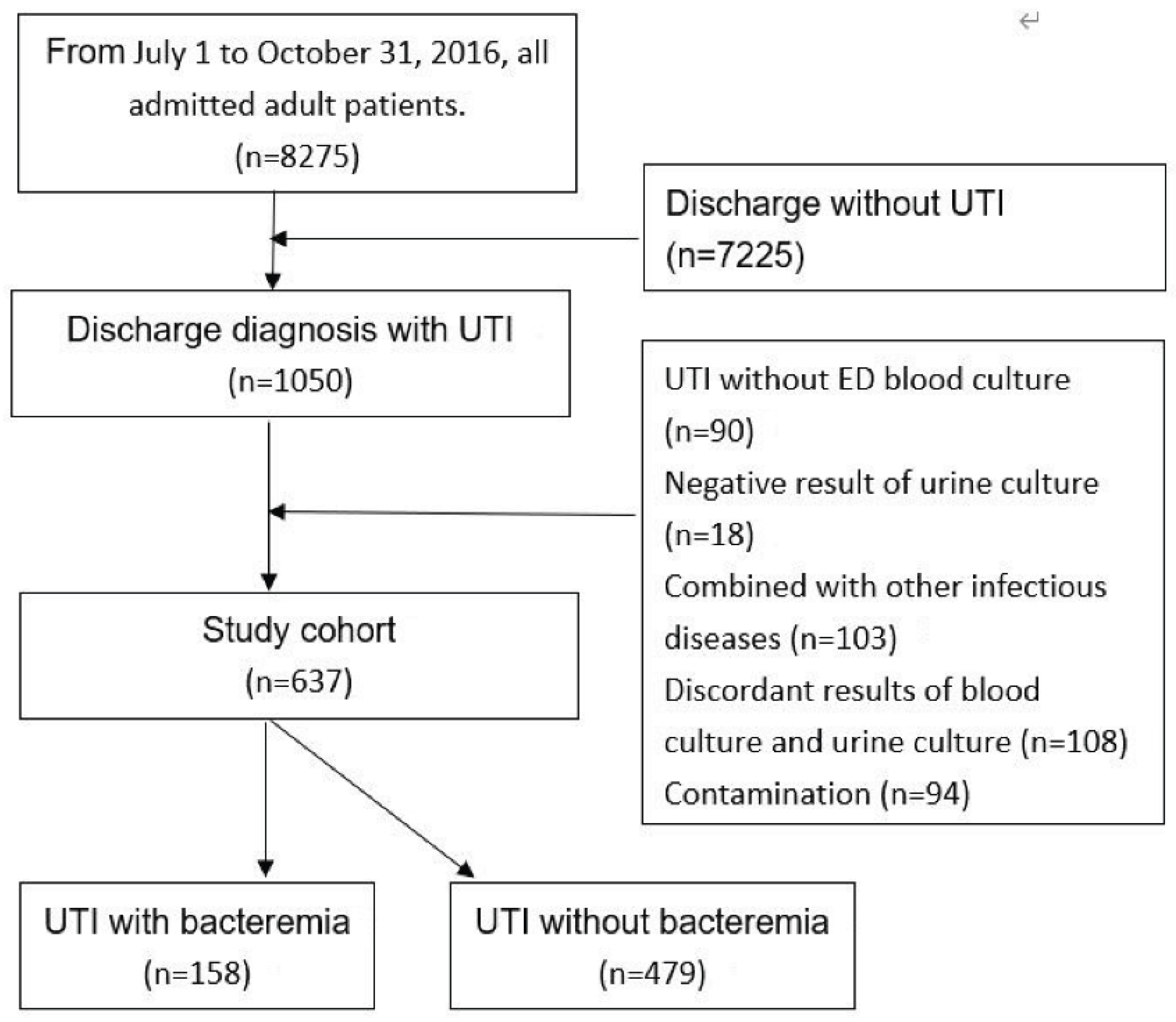
3.1. Patient Selection and General Description
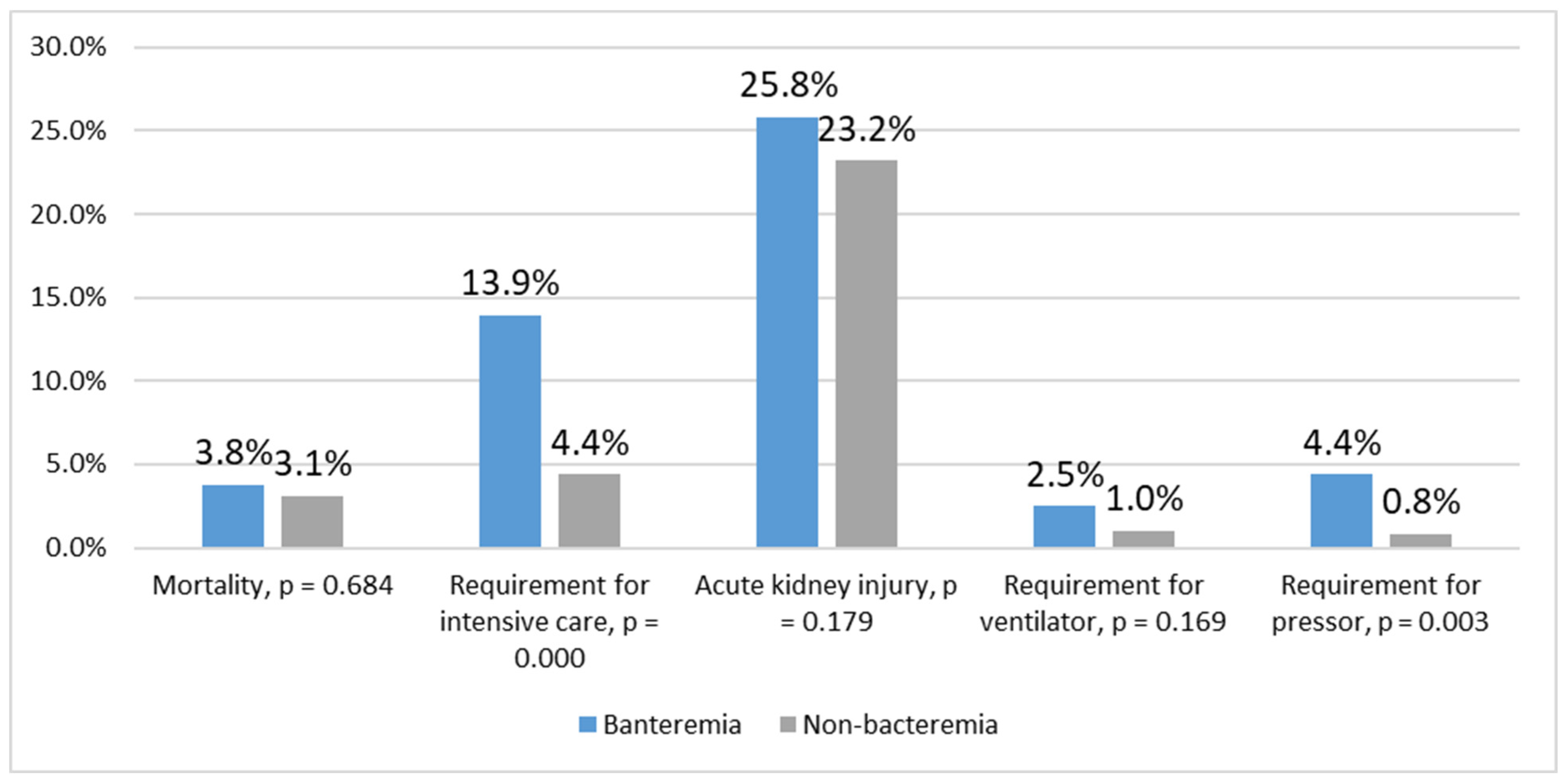
3.2. Comparison between the Bacteremia and Nonbacteremia Groups
3.3. Factors Associated with the Requirement for Intensive Care
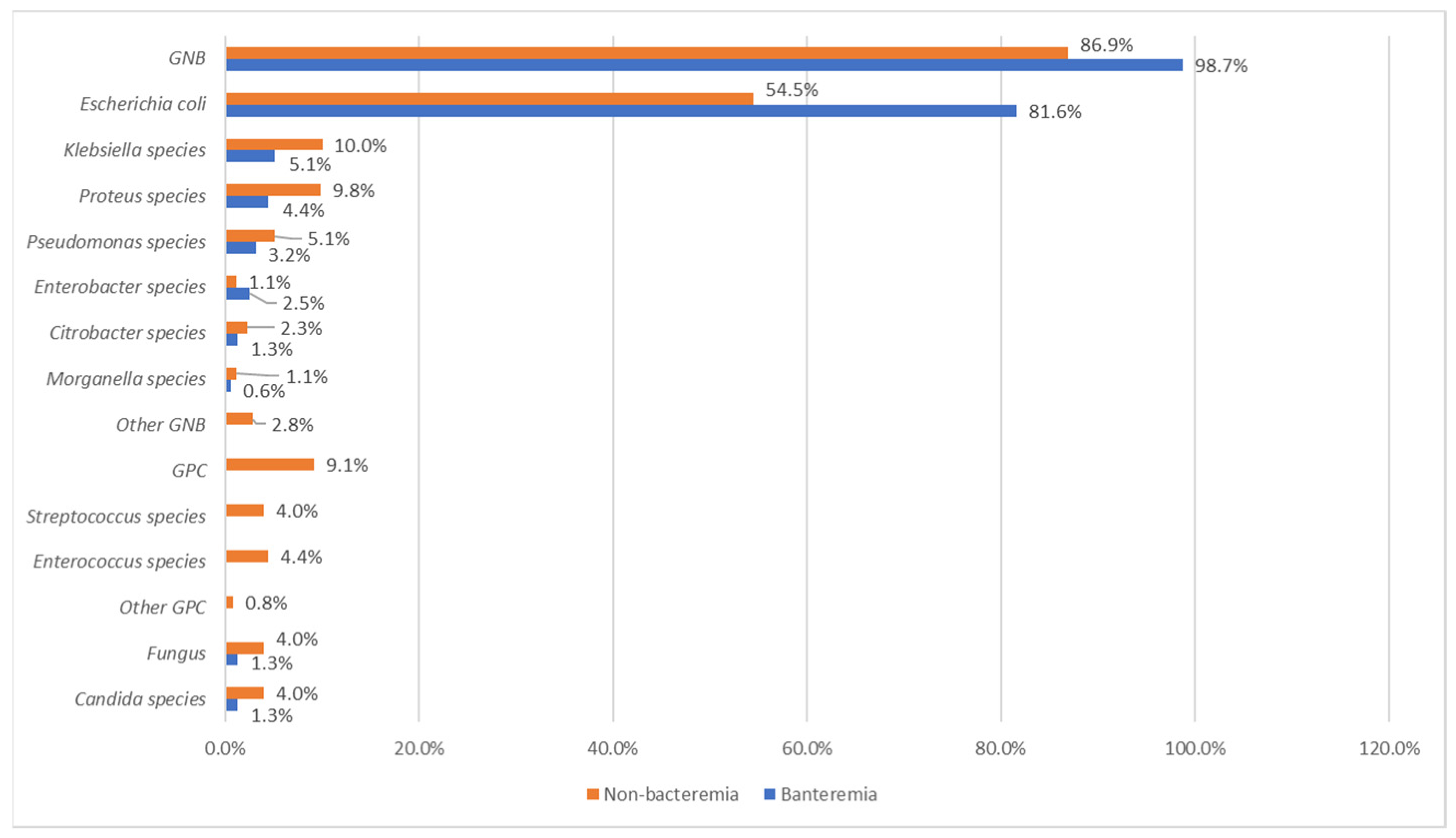
3.4. Results of Microbiological Studies
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hooton, T.M. Uncomplicated Urinary Tract Infection. N. Engl. J. Med. 2012, 366, 1028–1037. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J. International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geerlings, S.E. Clinical Presentations and Epidemiology of Urinary Tract Infections. Microbiol. Spect. 2016, 4, 27–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.; Lee, Y.S.; Jeong, R.; Kim, Y.J.; Ahn, S. Predictive factors of bacteremia in patients with febrile urinary tract infection: An experience at a tertiary care center. Infection 2014, 42, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Bahagon, Y.; Raveh, D.; Schlesinger, Y.; Rudensky, B.; Yinnon, A.M. Prevalence and predictive features of bacteremic urinary tract infection in emergency department patients. Eur. J. Clin. Microbiol. Infect. Dis. 2007, 26, 349–352. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Fang, H.C.; Chou, K.J.; Chen, C.L.; Lee, P.T.; Chung, H.M. The clinical impact of bacteremia in complicated acute pyelonephritis. Am. J. Med. Sci. 2006, 332, 175–180. [Google Scholar] [CrossRef]
- Artero, A.; Esparcia, A.; Eiros, J.M.; Madrazo, M.; Alberola, J.; Nogueira, J.M. Effect of Bacteremia in Elderly Patients with Urinary Tract Infection. Am. J. Med. Sci. 2016, 352, 267–271. [Google Scholar] [CrossRef]
- Saint, S.; Kaufman, S.R.; Rogers, M.A.M.; Baker, P.D.; Boyko, E.J.; Lipsky, B.A. Risk factors for nosocomial urinary tract-related bacteremia: A case-control study. Am. J. Infect. Control 2006, 34, 401–407. [Google Scholar] [CrossRef]
- Nieuwkoop, C.; Bonten, T.N.; Wout, J.W.V.; Becker, M.J.; Groeneveld, G.H.; Jansen, C.L.; Vorm, E.R.; Ijzerman, E.P.; Rothbarth, P.H.; Termeer-Veringa, E.M.; et al. Risk factors for bacteremia with uropathogen not cultured from urine in adults with febrile urinary tract infection. Clin. Infect. Dis. 2010, 50, e69–e72. [Google Scholar] [CrossRef] [Green Version]
- Velasco, M.; Martínez, J.A.; Moreno-Martínez, A.; Horcajada, J.P.; Ruiz, J.; Barranco, M.; Almela, M.; Vila, J.; Mensa, J. Blood cultures for women with uncomplicated acute pyelonephritis: Are they necessary? Clin. Infect. Dis. 2003, 37, 1127–1130. [Google Scholar] [CrossRef]
- Chiu, C.C.; Lin, T.C.; Wu, R.X.; Yang, Y.S.; Hsian, P.J.; Lee, Y.; Lin, J.C.; Chang, F.Y. Etiologies of community-onset urinary tract infections requiring hospitalization and antimicrobial susceptibilities of causative microorganisms. J. Microbiol. Immunol. Infect. 2017, 50, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Nicolle, L.E. Catheter associated urinary tract infections. Antimicrob. Resist. Infect. Control 2014, 3, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phua, J.; Ngerng, W.; See, K.; Tay, C.; Kiong, T.; Lim, H.; Chew, M.; Yip, H.; Tan, A.; Khalizah, H.; et al. Characteristics and outcomes of culture-negative versus culture-positive severe sepsis. Crit. Care 2013, 17, R202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balk, R.A. Systemic inflammatory response syndrome (SIRS) Where did it come from and is it still relevant today? Virulence 2014, 5, 20–26. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, F.L.; Bota, D.P.; Bross, A.; Mélot, C.; Vincent, J.L. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA 2001, 286, 1754–1758. [Google Scholar] [CrossRef] [Green Version]
- Al-Hasan, M.N.; Eckel-Passow, J.E.; Baddour, L.M. Bacteremia complicating gram-negative urinary tract infections: A population-based study. J. Infect. 2010, 60, 278–285. [Google Scholar] [CrossRef] [Green Version]
- Aguilar-Duran, S.; Horcajada, J.P.; Sorlí, L.; Montero, M.; Salvadó, M.; Grau, S.; Gómez, J.; Knobel, H. Community-onset healthcare-related urinary tract infections: Comparison with community and hospital-acquired urinary tract infections. J. Infect. 2012, 64, 478–483. [Google Scholar] [CrossRef]
- Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Javaloyas, M.; Garcia-Somoza, D.; Gudiol, F. Epidemiology and prognosis of bacteremia: A 10-y study in a community hospital. Scand. J. Infect. Dis. 2002, 34, 436–441. [Google Scholar] [CrossRef]
- Kao, C.H.; Kuo, Y.C.; Chen, C.C.; Chang, Y.T.; Chen, Y.S.; Wann, S.R.; Liu, Y.C. Isolated pathogens and clinical outcomes of adult bacteremia in the emergency department: A retrospective study in a tertiary Referral Center. J. Microbiol. Immunol. Infect. 2011, 44, 215–221. [Google Scholar] [CrossRef] [Green Version]
- Magret, M.; Lisboa, T.; Martin-Loeches, I.; Máñez, R.; Nauwynck, M.; Wrigge, H.; Cardellino, S.; Díaz, E.; Koulenti, D.; Rello, J.; et al. Bacteremia is an independent risk factor for mortality in nosocomial pneumonia: A prospective and observational multicenter study. Crit. Care 2011, 15, R62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Micek, S.T.; Hoban, A.P.; Pham, V.; Doherty, J.A.; Zilberberg, M.D.; Shorr, A.F.; Kollef, M.H. Bacteremia increases the risk of death among patients with soft-tissue infections. Surg. Infect. 2010, 11, 169–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, C.C.; Hsu, C.C.; Chen, K.T. Incidence and clinical features of patients with peritoneal dialysis peritonitis complicated by bacteremia. Medicine 2018, 97, e13567. [Google Scholar] [CrossRef] [PubMed]
- Julián-Jiménez, A.; Gutiérrez-Martín, P.; Lizcano-Lizcano, A.; López-Guerrero, M.A.; Barroso-Manso, A.; Heredero-Gálvez, E. Usefulness of procalcitonin and C-reactive protein for predicting bacteremia in urinary tract infections in the emergency department. Actas Urol. Esp. 2015, 39, 502–510. [Google Scholar] [CrossRef]
- Greene, M.T.; Chang, R.; Kuhn, L.; Rogers, M.A.M.; Chenoweth, C.E.; Shuman, E.; Saint, S. Predictors of hospital-acquired urinary tract-related bloodstream infection. Infect. Control Hosp. Epidemiol. 2012, 33, 1001–1007. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Demographic Data | Bacteremia | Non-Bacteremia | p |
|---|---|---|---|
| Sex (female) | 72.8% | 66.8% | 0.161 |
| Age (>64 years) | 55.1% | 62.4% | 0.101 |
| Comorbidity | 51.9% | 64.7% | 0.004 |
| Bedridden | 9.5% | 13.6% | 0.289 |
| GU instrumentation † | 15.8% | 26.3% | 0.007 |
| SIRS criteria ≥ 2 | 79.1% | 49.9% | 0.000 |
| Temperature > 38, <36 °C | 54.4% | 28.4% | 0.000 |
| Heart rate > 90/min | 77.2% | 60.3% | 0.000 |
| Respiratory rate > 20/min | 17.1% | 9.8% | 0.013 |
| WBC > 12,000 *, <4000, band > 10% | 69.5% | 57.6% | 0.009 |
| Sepsis (SOFA score ≥ 2) | 39.2% | 23.2% | 0.000 |
| Platelet < 150,000 μL | 34.2% | 2.8% | 0.000 |
| Creatinine > 1.2 mg/dL | 34.8% | 32.8% | 0.634 |
| GCS < 15 | 15.8% | 20.0% | 0.241 |
| MAP < 70 mmHg | 9.5% | 2.5% | 0.000 |
| T bilirubin > 1.2 mg/dL | 27.3% | 25.5% | 0.878 |
| Requirement for Intensive Care | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |
| Bacteremia | 0.283 | 0.151–0.531 | 0.000 | 0.338 | 0.165–0.692 | 0.003 |
| Sepsis | 0.239 | 0.127–0.450 | 0.000 | 0.291 | 0.150–0.564 | 0.000 |
| SIRS criteria | 0.498 | 0.250–0.984 | 0.045 | 0.594 | 0.282–1.253 | 0.171 |
| Age > 64 years | 0.727 | 0.376–1.405 | 0.343 | |||
| Comorbidity | 1.679 | 0.845–3.336 | 0.139 | |||
| Bedridden | 1.510 | 0.753–3.028 | 0.246 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, C.-C.; Lin, P.-C.; Chen, K.-T. The Presence of Bacteremia Indicates Higher Inflammatory Response and Augments Disease Severity in Adult Patients with Urinary Tract Infections. J. Clin. Med. 2022, 11, 4223. https://doi.org/10.3390/jcm11144223
Hsu C-C, Lin P-C, Chen K-T. The Presence of Bacteremia Indicates Higher Inflammatory Response and Augments Disease Severity in Adult Patients with Urinary Tract Infections. Journal of Clinical Medicine. 2022; 11(14):4223. https://doi.org/10.3390/jcm11144223
Chicago/Turabian StyleHsu, Chien-Chin, Pei-Chen Lin, and Kuo-Tai Chen. 2022. "The Presence of Bacteremia Indicates Higher Inflammatory Response and Augments Disease Severity in Adult Patients with Urinary Tract Infections" Journal of Clinical Medicine 11, no. 14: 4223. https://doi.org/10.3390/jcm11144223
APA StyleHsu, C.-C., Lin, P.-C., & Chen, K.-T. (2022). The Presence of Bacteremia Indicates Higher Inflammatory Response and Augments Disease Severity in Adult Patients with Urinary Tract Infections. Journal of Clinical Medicine, 11(14), 4223. https://doi.org/10.3390/jcm11144223