
Delayed Gastric Emptying Does Not Influence Cancer-Specific Survival after Pancreatoduodenectomy for Pancreatic Ductal Adenocarcinoma

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
Statistical Analyses
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [Green Version]
- Seufferlein, T.; Porzner, M.; Becker, T.; Budach, V.; Ceyhan, G.; Esposito, I.; Fietkau, R.; Follmann, M.; Friess, H.; Galle, P.; et al. S3-guideline exocrine pancreatic cancer. Z. Gastroenterol. 2013, 51, 1395–1440. [Google Scholar] [CrossRef] [Green Version]
- Krautz, C.; Nimptsch, U.; Weber, G.F.; Mansky, T.; Grützmann, R. Effect of Hospital Volume on In-Hospital Morbidity and Mortality Following Pancreatic Surgery in Germany. Ann. Surg. 2018, 267, 411–417. [Google Scholar] [CrossRef]
- Keck, T.; Wellner, U.F.; Bahra, M.; Klein, F.; Sick, O.; Niedergethmann, M.; Wilhelm, T.J.; Farkas, S.A.; Börner, T.; Bruns, C.; et al. Pancreatogastrostomy Versus Pancreatojejunostomy for RECOnstruction After PANCreatoduodenectomy (RECOPANC, DRKS 00000767): Perioperative and Long-Term Results of a Multicenter Randomized Controlled Trial. Ann. Surg. 2016, 263, 440–449. [Google Scholar] [CrossRef]
- Kamphues, C.; Bova, R.; Schricke, D.; Hippler-Benscheidt, M.; Klauschen, F.; Stenzinger, A.; Seehofer, D.; Glanemann, M.; Neuhaus, P.; Bahra, M. Postoperative Complications Deteriorate Long-Term Outcome in Pancreatic Cancer Patients. Ann. Surg. Oncol. 2012, 19, 856–863. [Google Scholar] [CrossRef]
- Aoyama, T.; Murakawa, M.; Katayama, Y.; Yamaoku, K.; Kanazawa, A.; Higuchi, A.; Shiozawa, M.; Morimoto, M.; Yoshikawa, T.; Yamamoto, N.; et al. Impact of Postoperative Complications on Survival and Recurrence in Pancreatic Cancer. Anticancer Res. 2015, 35, 2401–2409. [Google Scholar]
- Sandini, M.; Ruscic, K.J.; Ferrone, C.R.; Qadan, M.; Eikermann, M.; Warshaw, A.L.; Lillemoe, K.D.; Castillo, C.F.-D. Major Complications Independently Increase Long-Term Mortality After Pancreatoduodenectomy for Cancer. J. Gastrointest Surg. 2019, 23, 1984–1990. [Google Scholar] [CrossRef]
- Wente, M.N.; Bassi, C.; Dervenis, C.; Fingerhut, A.; Gouma, D.J.; Izbicki, J.R.; Neoptolemos, J.P.; Padbury, R.T.; Sarr, M.G.; Traverso, L.W.; et al. Delayed Gastric Emptying (DGE) after Pancreatic Surgery: A Suggested Definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2007, 142, 761–768. [Google Scholar] [CrossRef]
- Futagawa, Y.; Kanehira, M.; Furukawa, K.; Kitamura, H.; Yoshida, S.; Usuba, T.; Misawa, T.; Okamoto, T.; Yanaga, K. Impact of Delayed Gastric Emptying after Pancreaticoduodenectomy on Survival. J. Hepatobiliary Pancreat Sci. 2017, 24, 466–474. [Google Scholar] [CrossRef]
- He, J.; Ahuja, N.; Makary, M.A.; Cameron, J.L.; Eckhauser, F.E.; Choti, M.A.; Hruban, R.H.; Pawlik, T.M.; Wolfgang, C.L. 2564 Resected Periampullary Adenocarcinomas at a Single Institution: Trends over Three Decades. HPB 2014, 16, 83–90. [Google Scholar] [CrossRef] [Green Version]
- Ferrone, C.R.; Pieretti-Vanmarcke, R.; Bloom, J.P.; Zheng, H.; Szymonifka, J.; Wargo, J.A.; Thayer, S.P.; Lauwers, G.Y.; Deshpande, V.; Mino-Kenudson, M.; et al. Pancreatic Ductal Adenocarcinoma: Long-Term Survival Does Not Equal Cure. Surgery 2012, 152, S43–S49. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- Gillen, S.; Schuster, T.; Meyer Zum Büschenfelde, C.; Friess, H.; Kleeff, J. Preoperative/Neoadjuvant Therapy in Pancreatic Cancer: A Systematic Review and Meta-Analysis of Response and Resection Percentages. PLoS Med. 2010, 7, e1000267. [Google Scholar] [CrossRef] [Green Version]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.-L.; Choné, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. N. Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Palmer, D.H.; Ghaneh, P.; Psarelli, E.E.; Valle, J.W.; Halloran, C.M.; Faluyi, O.; O’Reilly, D.A.; Cunningham, D.; Wadsley, J.; et al. Comparison of Adjuvant Gemcitabine and Capecitabine with Gemcitabine Monotherapy in Patients with Resected Pancreatic Cancer (ESPAC-4): A Multicentre, Open-Label, Randomised, Phase 3 Trial. Lancet 2017, 389, 1011–1024. [Google Scholar] [CrossRef]
- Sinn, M.; Bahra, M.; Liersch, T.; Gellert, K.; Messmann, H.; Bechstein, W.; Waldschmidt, D.; Jacobasch, L.; Wilhelm, M.; Rau, B.M.; et al. CONKO-005: Adjuvant Chemotherapy With Gemcitabine Plus Erlotinib Versus Gemcitabine Alone in Patients After R0 Resection of Pancreatic Cancer: A Multicenter Randomized Phase III Trial. J. Clin. Oncol. 2017, 35, 3330–3337. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications: A New Proposal with Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Wente, M.N.; Veit, J.A.; Bassi, C.; Dervenis, C.; Fingerhut, A.; Gouma, D.J.; Izbicki, J.R.; Neoptolemos, J.P.; Padbury, R.T.; Sarr, M.G.; et al. Postpancreatectomy Hemorrhage (PPH): An International Study Group of Pancreatic Surgery (ISGPS) Definition. Surgery 2007, 142, 20–25. [Google Scholar] [CrossRef]
- Bassi, C.; Dervenis, C.; Butturini, G.; Fingerhut, A.; Yeo, C.; Izbicki, J.; Neoptolemos, J.; Sarr, M.; Traverso, W.; Buchler, M.; et al. Postoperative Pancreatic Fistula: An International Study Group (ISGPF) Definition. Surgery 2005, 138, 8–13. [Google Scholar] [CrossRef]
- Seufferlein, T.; Mayerle, J.; Böck, S.; Brunner, T.; Ettrich, T.J.; Grenacher, L.; Gress, T.M.; Hackert, T.; Heinemann, V.; Kestler, A.; et al. S3-Leitlinie zum exokrinen Pankreaskarzinom—Kurzversion 2.0—Dezember 2021, AWMF-Registernummer: 032/010OL. Z. Gastroenterol. 2022, 60, 991–1037. [Google Scholar] [CrossRef]
- Glowka, T.R.; Webler, M.; Matthaei, H.; Schäfer, N.; Schmitz, V.; Kalff, J.C.; Standop, J.; Manekeller, S. Delayed Gastric Emptying Following Pancreatoduodenectomy with Alimentary Reconstruction According to Roux-En-Y or Billroth-II. BMC Surg. 2017, 17, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hafke, J.; van Beekum, C.; Manekeller, S.; Vilz, T.O.; Kalff, J.C.; Glowka, T.R. Varianten der retrokolischen Rekonstruktion nach partieller Pankreatoduodenektomie und deren Einfluss auf die Magenentleerung—infra- oder suprakolisch. Zentralbl. Chir. 2020, 145, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Klaiber, U.; Leonhardt, C.-S.; Strobel, O.; Tjaden, C.; Hackert, T.; Neoptolemos, J.P. Neoadjuvant and Adjuvant Chemotherapy in Pancreatic Cancer. Langenbecks Arch. Surg. 2018, 403, 917–932. [Google Scholar] [CrossRef]
- Correa, P. Gastric Cancer: Overview. Gastroenterol. Clin. N. Am. 2013, 42, 211–217. [Google Scholar] [CrossRef] [Green Version]
- McArdle, C.S.; McMillan, D.C.; Hole, D.J. Impact of Anastomotic Leakage on Long-Term Survival of Patients Undergoing Curative Resection for Colorectal Cancer. Br. J. Surg. 2005, 92, 1150–1154. [Google Scholar] [CrossRef]
- Murakami, Y.; Uemura, K.; Sudo, T.; Hashimoto, Y.; Kondo, N.; Nakagawa, N.; Sasaki, H.; Sueda, T. Is Pancreatic Fistula Associated with Worse Overall Survival in Patients with Pancreatic Carcinoma? World J. Surg. 2015, 39, 500–508. [Google Scholar] [CrossRef]
- Ausania, F.; Cook, N.; Jamieson, N.; Huguet, E.; Jah, A.; Praseedom, R. Impact of Pancreatic Leaks on Survival Following Pancreaticoduodenectomy. JOP 2010, 11, 226–229. [Google Scholar]
- Hank, T.; Sandini, M.; Ferrone, C.R.; Rodrigues, C.; Weniger, M.; Qadan, M.; Warshaw, A.L.; Lillemoe, K.D.; Fernández-Del Castillo, C. Association Between Pancreatic Fistula and Long-Term Survival in the Era of Neoadjuvant Chemotherapy. JAMA Surg. 2019, 154, 943–951. [Google Scholar] [CrossRef]
- Pugalenthi, A.; Protic, M.; Gonen, M.; Kingham, T.P.; Angelica, M.I.D.; Dematteo, R.P.; Fong, Y.; Jarnagin, W.R.; Allen, P.J. Postoperative Complications and Overall Survival after Pancreaticoduodenectomy for Pancreatic Ductal Adenocarcinoma. J. Surg. Oncol. 2016, 113, 188–193. [Google Scholar] [CrossRef] [Green Version]
- Lu, J.-W.; Ding, H.-F.; Wu, X.-N.; Liu, X.-M.; Wang, B.; Wu, Z.; Lv, Y.; Zhang, X.-F. Intra-Abdominal Hemorrhage Following 739 Consecutive Pancreaticoduodenectomy: Risk Factors and Treatments. J. Gastroenterol. Hepatol. 2019, 34, 1100–1107. [Google Scholar] [CrossRef]
- Vandermeeren, C.; Loi, P.; Closset, J. Does Pancreaticogastrostomy Decrease the Occurrence of Delayed Gastric Emptying After Pancreatoduodenectomy? Pancreas 2017, 46, 1064–1068. [Google Scholar] [CrossRef] [PubMed]
- Welsch, T.; Borm, M.; Degrate, L.; Hinz, U.; Büchler, M.W.; Wente, M.N. Evaluation of the International Study Group of Pancreatic Surgery Definition of Delayed Gastric Emptying after Pancreatoduodenectomy in a High-Volume Centre. Br. J. Surg. 2010, 97, 1043–1050. [Google Scholar] [CrossRef] [PubMed]
- Mackay, T.M.; Smits, F.J.; Roos, D.; Bonsing, B.A.; Bosscha, K.; Busch, O.R.; Creemers, G.-J.; van Dam, R.M.; van Eijck, C.H.J.; Gerhards, M.F.; et al. The Risk of Not Receiving Adjuvant Chemotherapy after Resection of Pancreatic Ductal Adenocarcinoma: A Nationwide Analysis. HPB 2020, 22, 233–240. [Google Scholar] [CrossRef]
- Nussbaum, D.P.; Adam, M.A.; Youngwirth, L.M.; Ganapathi, A.M.; Roman, S.A.; Tyler, D.S.; Sosa, J.A.; Blazer, D.G. Minimally Invasive Pancreaticoduodenectomy Does Not Improve Use or Time to Initiation of Adjuvant Chemotherapy for Patients With Pancreatic Adenocarcinoma. Ann. Surg. Oncol. 2016, 23, 1026–1033. [Google Scholar] [CrossRef] [PubMed]
- Dhir, M.; Zenati, M.S.; Hamad, A.; Singhi, A.D.; Bahary, N.; Hogg, M.E.; Zeh, H.J.; Zureikat, A.H. FOLFIRINOX Versus Gemcitabine/Nab-Paclitaxel for Neoadjuvant Treatment of Resectable and Borderline Resectable Pancreatic Head Adenocarcinoma. Ann. Surg. Oncol. 2018, 25, 1896–1903. [Google Scholar] [CrossRef]
- Ellis, R.J.; Gupta, A.R.; Hewitt, D.B.; Merkow, R.P.; Cohen, M.E.; Ko, C.Y.; Bilimoria, K.Y.; Bentrem, D.J.; Yang, A.D. Risk Factors for Post-Pancreaticoduodenectomy Delayed Gastric Emptying in the Absence of Pancreatic Fistula or Intra-Abdominal Infection. J. Surg. Oncol. 2019, 119, 925–931. [Google Scholar] [CrossRef]
- Enderes, J.; Teschke, J.; von Websky, M.; Manekeller, S.; Kalff, J.C.; Glowka, T.R. Active Smokers Show Ameliorated Delayed Gastric Emptying after Pancreatoduodenectomy. BMC Surg. 2021, 21, 316. [Google Scholar] [CrossRef]
- Hüttner, F.J.; Klotz, R.; Ulrich, A.; Büchler, M.W.; Probst, P.; Diener, M.K. Antecolic versus Retrocolic Reconstruction after Partial Pancreaticoduodenectomy. Cochrane Database Syst. Rev. 2022, 1, CD011862. [Google Scholar] [CrossRef]
- Klaiber, U.; Probst, P.; Strobel, O.; Michalski, C.W.; Dörr-Harim, C.; Diener, M.K.; Büchler, M.W.; Hackert, T. Meta-Analysis of Delayed Gastric Emptying after Pylorus-Preserving versus Pylorus-Resecting Pancreatoduodenectomy. Br. J. Surg. 2018, 105, 339–349. [Google Scholar] [CrossRef]
- Klaiber, U.; Probst, P.; Knebel, P.; Contin, P.; Diener, M.K.; Büchler, M.W.; Hackert, T. Meta-Analysis of Complication Rates for Single-Loop versus Dual-Loop (Roux-En-Y) with Isolated Pancreaticojejunostomy Reconstruction after Pancreaticoduodenectomy. Br. J. Surg. 2015, 102, 331–340. [Google Scholar] [CrossRef]
- Park, J.S.; Hwang, H.K.; Kim, J.K.; Cho, S.I.; Yoon, D.S.; Lee, W.J.; Chi, H.S. Clinical Validation and Risk Factors for Delayed Gastric Emptying Based on the International Study Group of Pancreatic Surgery (ISGPS) Classification. Surgery 2009, 146, 882–887. [Google Scholar] [CrossRef] [PubMed]
- Kunstman, J.W.; Fonseca, A.L.; Ciarleglio, M.M.; Cong, X.; Hochberg, A.; Salem, R.R. Comprehensive Analysis of Variables Affecting Delayed Gastric Emptying Following Pancreaticoduodenectomy. J. Gastrointest. Surg. 2012, 16, 1354–1361. [Google Scholar] [CrossRef] [PubMed]
- Enderes, J.; Teschke, J.; Manekeller, S.; Vilz, T.O.; Kalff, J.C.; Glowka, T.R. Chronic Liver Disease Increases Mortality Following Pancreatoduodenectomy. J. Clin. Med. 2021, 10, 2521. [Google Scholar] [CrossRef] [PubMed]
- Enderes, J.; Pillny, C.; Matthaei, H.; Manekeller, S.; Kalff, J.C.; Glowka, T.R. Obesity Does Not Influence Delayed Gastric Emptying Following Pancreatoduodenectomy. Biology 2022, 11, 763. [Google Scholar] [CrossRef] [PubMed]
- Croome, K.P.; Farnell, M.B.; Que, F.G.; Reid-Lombardo, K.M.; Truty, M.J.; Nagorney, D.M.; Kendrick, M.L. Total Laparoscopic Pancreaticoduodenectomy for Pancreatic Ductal Adenocarcinoma: Oncologic Advantages over Open Approaches? Ann. Surg. 2014, 260, 633–638; discussion 638–640. [Google Scholar] [CrossRef]


{kind=link}
| No DGE | Clinically Relevant DGE (°B/C) | p Value | |
|---|---|---|---|
| Variables | n = 102 | n = 31 | |
| Female | 51 (50%) | 12 (38.7%) | 0.27 |
| Age > 75 years | 36 (35.3%) | 11 (35.5%) | 0.985 |
| Active Smoker | 28 (27.5%) | 5 (16.1%) | 0.175 |
| Smoker | 51 (50%) | 12 (38.7%) | 0.337 |
| Alcohol consumption | 30 (29.4%) | 10 (32.3%) | 0.729 |
| Pre-operative weight loss | 65 (63.7%) | 17 (54.8%) | 0.407 |
| Pre-operative biliary stenting | 53 (52%) | 15 (48.4%) | 0.727 |
| Pre-existing diabetes mellitus | 40 (39.2%) | 10 (32.3%) | 0.484 |
| Chronic pulmonary disease | 8 (7.8%) | 9 (29%) | 0.005 |
| Previous abdominal surgery | 56 (5.9%) | 16 (51.6%) | 0.755 |
| Charlson Comorbidity Index | 3 (2–3) | 3 (2–4) | 0.031 |
| Exitus < 30 days | 5(4.9%) | 1 (3.2%) | 0.573 |
| No DGE | Clinically Relevant DGE (°B/C) | p Value | |
|---|---|---|---|
| Variables | n = 102 | n = 31 | |
| Hospital stay postoperative | 18 (14–24) | 29 (25–37) | <0.001 |
| ICU stay | 2 (1–3) | 1 (1–5) | 0.911 |
| Intraoperative blood loss (mL) | 700 (400–1100) | 600 (350–1000) | 0.563 |
| Single loop reconstruction | 83 (81.4%) | 28 (90.3%) | 0.24 |
| Antecolic reconstruction | 18 (17.6%) | 2 (6.5%) | 0.155 |
| Multivisceral resection | 7 (6.9%) | 2 (6.5%) | 1.0 |
| Pylorus preservation | 80 (78.4%) | 27 (87.1%) | 0.287 |
| Extended lymphadenectomy | 63 (61.8%) | 20 (64.5%) | 0.782 |
| Portal venous resection | 31 (30.4%) | 6 (19.4%) | 0.219 |
| Bile duct > 5 cm | 30 (29.4%) | 4 (12.9%) | 0.099 |
| PPH | 32 (31.4%) | 16 (51.6%) | 0.04 |
| Clinically relevant PPH (°B/C) | 25 (24.5%) | 14 (45.2%) | 0.027 |
| PF | 17 (16.7%) | 5 (16.1%) | 0.927 |
| Clinically relevant PF (°B/C) | 4 (3.9%) | 4 (12.9%) | 0.087 |
| Surgical site infection | 16 (15.7%) | 5 (16.1%) | 1.0 |
| Intra-abdominal collection/abscess | 9 (8.8%) | 3 (9.7%) | 1.0 |
| Bacterobilia | 54 (52.9%) | 14 (45.2%) | 0.388 |
| Clavien-Dindo stage Major (°III–V) | 39 (38.2%) | 27 (87.1%) | <0.001 |
| No DGE | Clinically Relevant DGE (°B/C) | p Value | |
|---|---|---|---|
| Variables | n = 102 | n = 31 | |
| Tumor size (cm) | 3.15 (2.5–4.2) | 2.75 (2.32–3.5) | 0.051 |
| Tumor size > 3 cm | 59 (57.8%) | 12 (38.7%) | 0.129 |
| Lymph node metastasis | 79 (77.5%) | 21 (67.7%) | 0.352 |
| Microlymphatic invasion | 38 (37.3%) | 13 (41.9%) | 0.695 |
| Microvascular invasion | 19 (18.6%) | 6 (19.4%) | 0.965 |
| Perineural invasion | 72 (70.6%) | 23 (74.2%) | 0.617 |
| Surgical margin positive | 30 (29.4%) | 8 (25.8%) | 0.748 |
| Variables | No. of Patients | Median Survival (Months) | p Value |
|---|---|---|---|
| Pre-operative biliary stenting | 0.988 | ||
| yes | 68 | 15 | |
| no | 65 | 18 | |
| Bacterobilia | 0.677 | ||
| yes | 68 | 15 | |
| no | 59 | 15 | |
| Former or active nicotine consumption | 0.969 | ||
| yes | 63 | 18 | |
| no | 65 | 15 | |
| Active Nicotine consumption | 0.826 | ||
| yes | 33 | 15 | |
| no | 97 | 15 | |
| DM with TOD | 0.004 | ||
| yes | 6 | 7 | |
| no | 126 | 15 | |
| Portal venous resection | 0.108 | ||
| yes | 37 | 10 | |
| no | 95 | 19 | |
| DGE | 0.376 | ||
| yes | 67 | 15 | |
| no | 66 | 19 | |
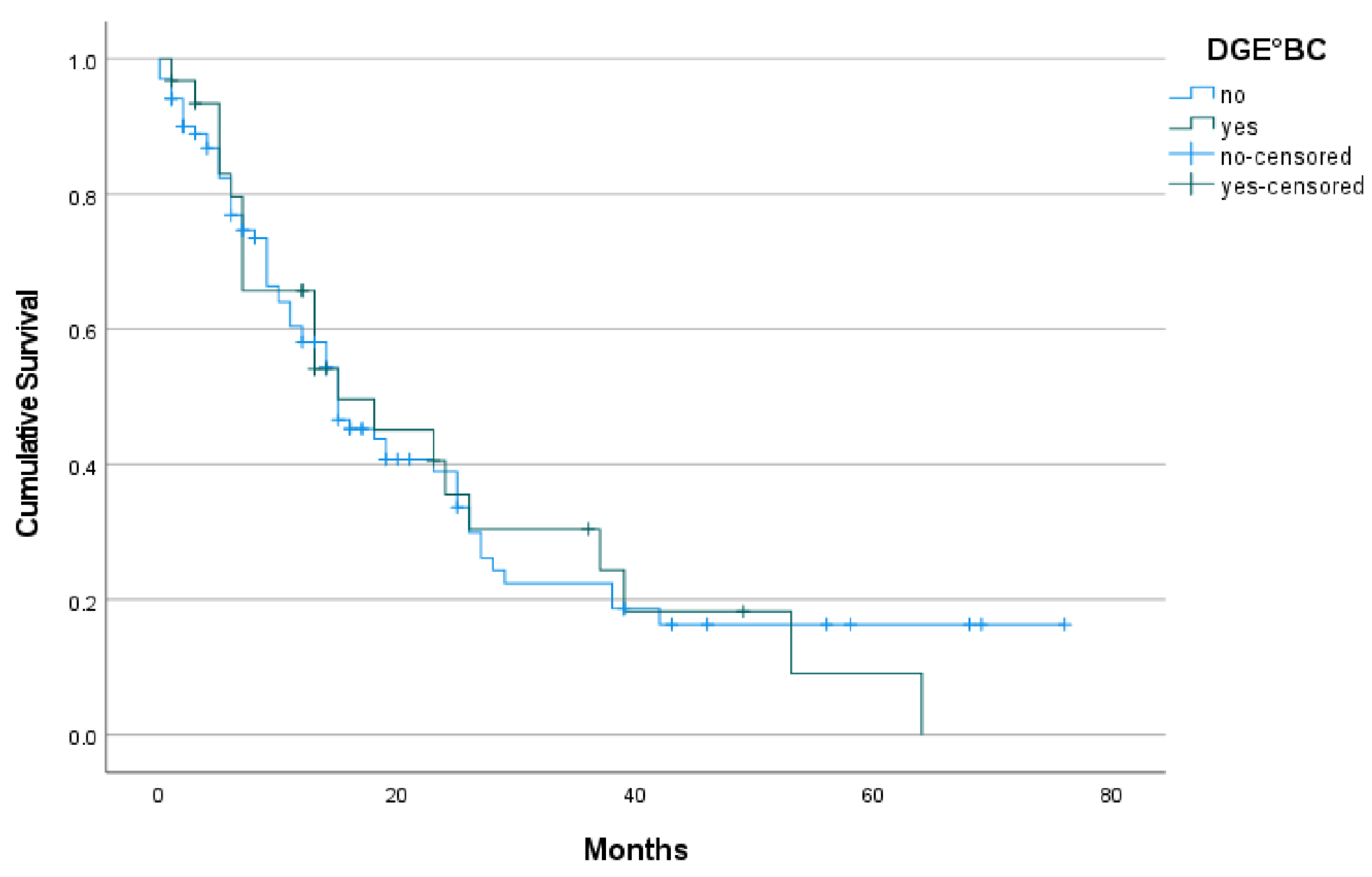
| Clinically relevant DGE (°B/C) | 0.916 | ||
| yes | 31 | 15 | |
| no | 102 | 15 | |
| Clinically relevant PF (°B/C) | |||
| yes | 8 | 64 | 0.458 |
| no | 124 | 15 | |
| Clinically relevant PPH (°B/C) | 0.881 | ||
| yes | 39 | 15 | |
| no | 94 | 15 | |
| PPH | 0.587 | ||
| yes | 48 | 15 | |
| no | 85 | 15 | |
| Lymph node metastasis | 0.174 | ||
| yes | 100 | 15 | |
| no | 31 | 18 | |
| Positive surgical margin | 0.006 | ||
| yes | 93 | 14 | |
| no | 38 | 18 | |
| Tumor size >3 cm | |||
| yes | 71 | 11 | 0.003 |
| no | 57 | 26 |
| Odds Ratio | 95% CI | p | |
|---|---|---|---|
| Clinically relevant PPH (°B/C) | 4.802 | 1.092–21.113 | 0.024 |
| Medical complications | 6.445 | 1.247–33.307 | 0.009 |
| Study | Number of Patients | Study Type | Parameter Effecting DGE | Effect |
|---|---|---|---|---|
| Reconstruction Techniques | ||||
| Hüttner et al., 2022 [38] | 650 | CDR | Ante-/retrocolic position | ante = retro |
| Klaiber et al., 2018 [39] | 992 | Meta | Pylorus preservation | pp = pr |
| Klaiber et al., 2015 [40] | 802 | Meta | Single/dual-loop | single = dual |
| Risk Factors | ||||
| Park et al., 2009 [41] | 129 | ROT | Pancreatic fistula | more DGE |
| Kunstman et al., 2012 [42] | 235 | ROT | Intraoperative blood loss | more DGE |
| Hafke et al., 2020 [22] | 138 | ROT | Supra-/infracolic DE | No effect |
| Enderes et al., 2021 [37] | 295 | ROT | Active smoking | less DGE |
| Enderes et al., 2021 [43] | 275 | ROT | Liver cirrhosis | no effect |
| Enderes et al., 2022 [44] | 211 | ROT | Obesity | no effect |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pillny, C.; Teschke, J.; Enderes, J.; Manekeller, S.; Kalff, J.C.; Glowka, T.R. Delayed Gastric Emptying Does Not Influence Cancer-Specific Survival after Pancreatoduodenectomy for Pancreatic Ductal Adenocarcinoma. J. Clin. Med. 2022, 11, 4200. https://doi.org/10.3390/jcm11144200
Pillny C, Teschke J, Enderes J, Manekeller S, Kalff JC, Glowka TR. Delayed Gastric Emptying Does Not Influence Cancer-Specific Survival after Pancreatoduodenectomy for Pancreatic Ductal Adenocarcinoma. Journal of Clinical Medicine. 2022; 11(14):4200. https://doi.org/10.3390/jcm11144200
Chicago/Turabian StylePillny, Christiane, Jessica Teschke, Jana Enderes, Steffen Manekeller, Jörg C. Kalff, and Tim R. Glowka. 2022. "Delayed Gastric Emptying Does Not Influence Cancer-Specific Survival after Pancreatoduodenectomy for Pancreatic Ductal Adenocarcinoma" Journal of Clinical Medicine 11, no. 14: 4200. https://doi.org/10.3390/jcm11144200
APA StylePillny, C., Teschke, J., Enderes, J., Manekeller, S., Kalff, J. C., & Glowka, T. R. (2022). Delayed Gastric Emptying Does Not Influence Cancer-Specific Survival after Pancreatoduodenectomy for Pancreatic Ductal Adenocarcinoma. Journal of Clinical Medicine, 11(14), 4200. https://doi.org/10.3390/jcm11144200