
Efficacy and Safety of Transcranial Electric Stimulation during the Perinatal Period: A Systematic Literature Review and Three Case Reports

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Methods
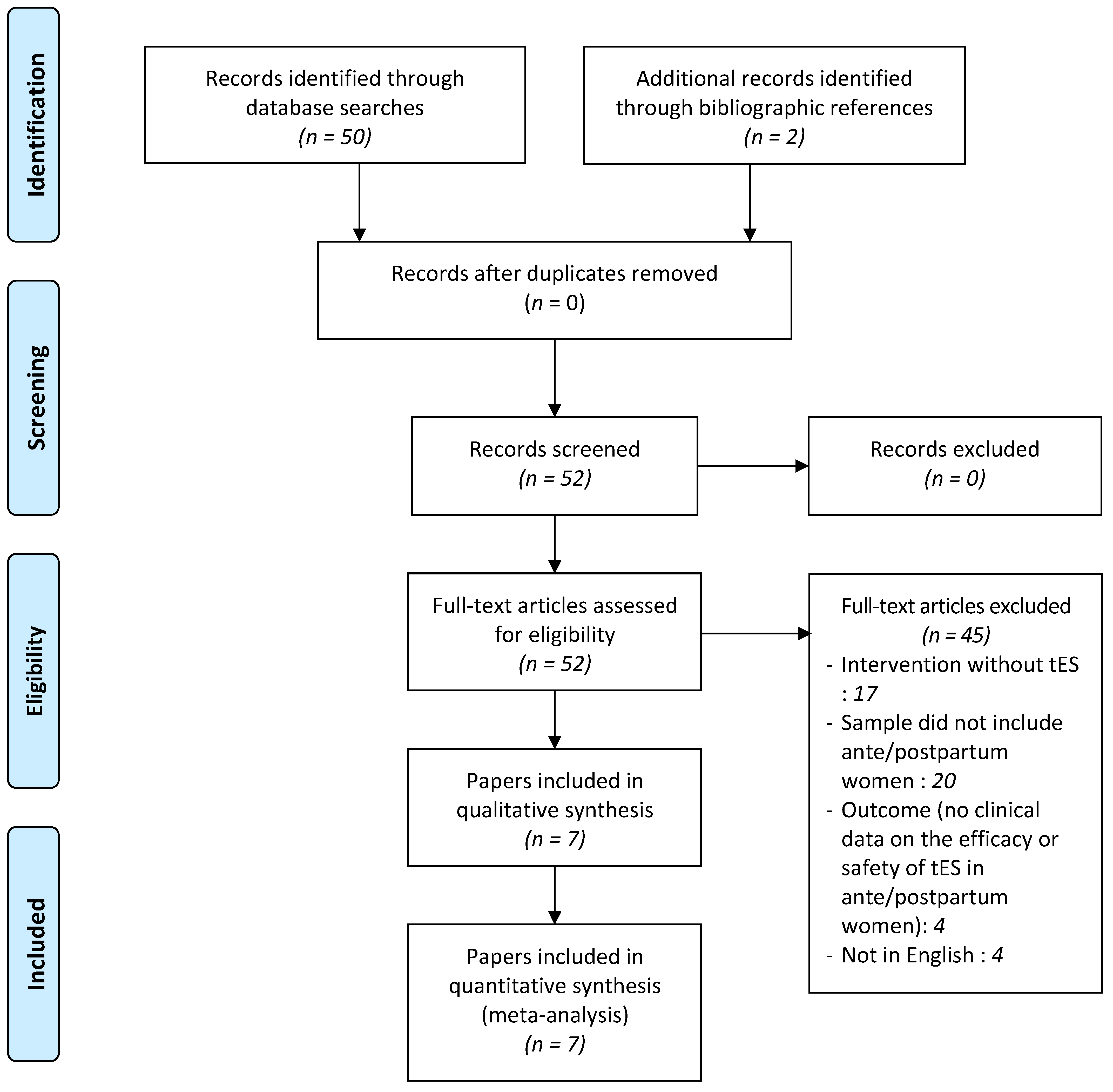
2.1. Eligibility Criteria
2.2. Selection Methods
2.3. Data Collection Process
2.4. Case Reports
2.5. Statistical Analysis
2.6. Ethics
3. Results
3.1. Characteristics of the Studies
3.2. Case Reports
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Munk-Olsen, T.; Maegbaek, M.L.; Johannsen, B.M.; Liu, X.; Howard, L.M.; di Florio, A.; Bergink, V.; Meltzer-Brody, S. Perinatal psychiatric episodes: A population-based study on treatment incidence and prevalence. Transl. Psychiatry 2016, 6, e919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dagher, R.K.; Bruckheim, H.E.; Colpe, L.J.; Edwards, E.; White, D.B. Perinatal Depression: Challenges and Opportunities. J. Women’s Health 2021, 30, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Paschetta, E.; Berrisford, G.; Coccia, F.; Whitmore, J.; Wood, A.G.; Pretlove, S.; Ismail KM, K. Perinatal psychiatric disorders: An overview. Am. J. Obstet. Gynecol. 2014, 210, 501–509.e6. [Google Scholar] [CrossRef] [PubMed]
- Woody, C.A.; Ferrari, A.J.; Siskind, D.J.; Whiteford, H.A.; Harris, M.G. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J. Affect. Disord. 2017, 219, 86–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perry, A.; Gordon-Smith, K.; Di Florio, A.; Craddock, N.; Jones, L.; Jones, I. Mood episodes in pregnancy and risk of postpartum recurrence in bipolar disorder: The Bipolar Disorder Research Network Pregnancy Study. J. Affect. Disord. 2021, 294, 714–722. [Google Scholar] [CrossRef]
- Wesseloo, R.; Kamperman, A.M.; Munk-Olsen, T.; Pop, V.J.M.; Kushner, S.A.; Bergink, V. Risk of Postpartum Relapse in Bipolar Disorder and Postpartum Psychosis: A Systematic Review and Meta-Analysis. AJP 2016, 173, 117–127. [Google Scholar] [CrossRef] [Green Version]
- Chan, J.; Natekar, A.; Einarson, A.; Koren, G. Risks of untreated depression in pregnancy. Can. Fam. Physician 2014, 60, 242–243. [Google Scholar]
- Thombre, M.K.; Talge, N.M.; Holzman, C. Association Between Pre-Pregnancy Depression/Anxiety Symptoms and Hypertensive Disorders of Pregnancy. J. Women’s Health 2015, 24, 228–236. [Google Scholar] [CrossRef] [Green Version]
- Hare, D.L.; Toukhsati, S.R.; Johansson, P.; Jaarsma, T. Depression and cardiovascular disease: A clinical review. Eur. Heart J. 2014, 35, 365–372. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, J.J.; Smith, V.C. Epidemiology of perinatal substance use: Exploring trends in maternal substance use. Semin. Fetal Neonatal Med. 2019, 24, 86–89. [Google Scholar] [CrossRef]
- Guillard, V.; Gressier, F. Suicidality during perinatal period. Presse Med. 2017, 46, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Hermon, N.; Wainstock, T.; Sheiner, E.; Golan, A.; Walfisch, A. Impact of maternal depression on perinatal outcomes in hospitalized women—A prospective study. Arch. Womens Ment. Health 2019, 22, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Gentile, S.; Fusco, M.L. Untreated perinatal paternal depression: Effects on offspring. Psychiatry Res. 2017, 252, 325–332. [Google Scholar] [CrossRef]
- Barnes, J.; Theule, J. Maternal depression and infant attachment security: A meta-analysis. Infant Mental. Health J. 2019, 40, 817–834. [Google Scholar] [CrossRef]
- Gentile, S. Untreated depression during pregnancy: Short- and long-term effects in offspring. Syst. Rev. Neurosci. 2017, 342, 154–166. [Google Scholar] [CrossRef]
- Millett, L.; Taylor, B.L.; Howard, L.M.; Bick, D.; Stanley, N.; Johnson, S. Experiences of Improving Access to Psychological Therapy Services for Perinatal Mental Health Difficulties: A Qualitative Study of Women’s and Therapists’ Views. Behav. Cogn. Psychother. 2018, 46, 421–436. [Google Scholar] [CrossRef] [Green Version]
- Dubovicky, M.; Belovicova, K.; Csatlosova, K.; Bogi, E. Risks of using SSRI/SNRI antidepressants during pregnancy and lactation. Interdiscip Toxicol. 2017, 10, 30–34. [Google Scholar] [CrossRef] [Green Version]
- Lupattelli, A.; Spigset, O.; Björnsdóttir, I.; Hämeen-Anttila, K.; Mårdby, A.-C.; Panchaud, A.; Juraski, R.G.; Rudolf, G.; Odalovic, M.; Drozd, M.; et al. Patterns and Factors Associated with Low Adherence to Psychotropic Medications During Pregnancy—A Cross-Sectional, Multinational Web-Based Study. Depress. Anxiety 2015, 32, 426–436. [Google Scholar] [CrossRef]
- Petersen, I.; McCrea, R.L.; Sammon, C.J.; Osbon, D.P.; Evans, S.J.; Cowen, P.J.; Freemantle, N.; Nazareth, I. Risks and benefits of psychotropic medication in pregnancy: Cohort studies based on UK electronic primary care health records. Health Technol. Assess. 2016, 20, 1–176. [Google Scholar] [CrossRef] [Green Version]
- Petersen, I.; Gilbert, R.E.; Evans, S.J.W.; Man, S.-L.; Nazareth, I. Pregnancy as a Major Determinant for Discontinuation of Antidepressants: An Analysis of Data From The Health Improvement Network. J. Clin. Psychiatry 2011, 72, 15209. [Google Scholar] [CrossRef]
- Rose, S.; Dotters-Katz, S.K.; Kuller, J.A. Electroconvulsive Therapy in Pregnancy: Safety, Best Practices, and Barriers to Care. Obstet. Gynecol. Surv. 2020, 75, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Hebel, T.; Schecklmann, M.; Langguth, B. Transcranial magnetic stimulation in the treatment of depression during pregnancy: A review. Arch. Womens Ment. Health 2020, 23, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Fu, C.; Xiong, F.; Zhang, Q.; Liang, Z.; Chen, L.; He, C.; Wei, Q. Effects of repetitive transcranial magnetic stimulation on depression symptoms and cognitive function in treating patients with postpartum depression: A systematic review and meta-analysis of randomized controlled trials. Psychiatry Res. 2020, 290, 113124. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Sumiyoshi, T. Neurobiological Mechanisms of Transcranial Direct Current Stimulation for Psychiatric Disorders; Neurophysiological, Chemical, and Anatomical Considerations. Front. Hum. Neurosci. 2021, 15, 631836. [Google Scholar] [CrossRef]
- Lefaucheur, J.P. Méthodologies tDCS/tACS/tRNS. Neurophysiol. Clin. 2019, 43, 182. [Google Scholar] [CrossRef]
- Elyamany, O.; Leicht, G.; Herrmann, C.S.; Mulert, C. Transcranial alternating current stimulation (tACS): From basic mechanisms towards first applications in psychiatry. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 135–156. [Google Scholar] [CrossRef]
- Moret, B.; Donato, R.; Nucci, M.; Cona, G.; Campana, G. Transcranial random noise stimulation (tRNS): A wide range of frequencies is needed for increasing cortical excitability. Sci Rep. 2019, 9, 15150. [Google Scholar] [CrossRef] [Green Version]
- Herrera-Melendez, A.-L.; Bajbouj, M.; Aust, S. Application of Transcranial Direct Current Stimulation in Psychiatry. NPS 2020, 79, 372–383. [Google Scholar] [CrossRef]
- Kuo, M.-F.; Chen, P.-S.; Nitsche, M.A. The application of tDCS for the treatment of psychiatric diseases. Int. Rev. Psychiatry 2017, 29, 146–167. [Google Scholar] [CrossRef] [Green Version]
- Kuo, M.-F.; Paulus, W.; Nitsche, M.A. Therapeutic effects of non-invasive brain stimulation with direct currents (tDCS) in neuropsychiatric diseases. Neuroimage 2014, 85, 948–960. [Google Scholar] [CrossRef]
- Razza, L.B.; Palumbo, P.; Moffa, A.H.; Carvalho, A.F.; Solmi, M.; Loo, C.K.; Brunoni, A.R. A systematic review and meta-analysis on the effects of transcranial direct current stimulation in depressive episodes. Depress. Anxiety 2020, 37, 594–608. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.W.C.; Louie, L.L.C.; Wong, Y.L.; Wong, S.M.C.; Leung, W.Y.; Nitsche, M.A.; Chan, W.C. The effects of transcranial direct current stimulation (tDCS) on clinical symptoms in schizophrenia: A systematic review and meta-analysis. Asian J. Psychiatry 2020, 53, 102392. [Google Scholar] [CrossRef]
- Ahmadizadeh, M.J.; Rezaei, M.; Fitzgerald, P.B. Transcranial direct current stimulation (tDCS) for post-traumatic stress disorder (PTSD): A randomized, double-blinded, controlled trial. Brain Res. Bulletin. 2019, 153, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Van’t Wout, M.; Shea, M.T.; Larson, V.C.; Greenberg, B.D.; Philip, N.S. Combined transcranial direct current stimulation with virtual reality exposure for posttraumatic stress disorder: Feasibility and pilot results. Brain Stimul. 2019, 12, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Aparício, L.V.M.; Guarienti, F.; Razza, L.B.; Carvalho, A.F.; Fregni, F.; Brunoni, A.R. A Systematic Review on the Acceptability and Tolerability of Transcranial Direct Current Stimulation Treatment in Neuropsychiatry Trials. Brain Stimul. 2016, 9, 671–681. [Google Scholar] [CrossRef]
- Bikson, M.; Grossman, P.; Thomas, C.; Zannou, A.L.; Jiang, J.; Adnan, T.; Mourdoukoutas, A.P.; Kronberg, G.; Truong, D.; Boggio, P.; et al. Safety of Transcranial Direct Current Stimulation: Evidence Based Update 2016. Brain Stimul. 2016, 9, 641–661. [Google Scholar] [CrossRef] [Green Version]
- Buchanan, D.M.; Bogdanowicz, T.; Khanna, N.; Lockman-Dufour, G.; Robaey, P.; D’Angiulli, A. Systematic Review on the Safety and Tolerability of Transcranial Direct Current Stimulation in Children and Adolescents. Brain Sci. 2021, 11, 212. [Google Scholar] [CrossRef]
- Moffa, A.H.; Brunoni, A.R.; Fregni, F.; Palm, U.; Padberg, F.; Blumberger, D.M.; Daskalakis, Z.J.; Bennabi, D.; Haffen, E.; Alonzo, A.; et al. Safety and acceptability of transcranial direct current stimulation for the acute treatment of major depressive episodes: Analysis of individual patient data. J. Affect. Disord. 2017, 221, 1–5. [Google Scholar] [CrossRef]
- Nikolin, S.; Huggins, C.; Martin, D.; Alonzo, A.; Loo, C.K. Safety of repeated sessions of transcranial direct current stimulation: A systematic review. Brain Stimul. 2018, 11, 278–288. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Montgomery, S.A.; Asberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Beamesderfer, A. Assessment of Depression: The Depression Inventory; Psychological measurements in psychopharmacology; Karger Publishers: Basel, Switzerland, 1974; Volume 7, pp. 151–169. [Google Scholar]
- Ashbaugh, A.R.; Houle-Johnson, S.; Herbert, C.; El-Hage, W.; Brunet, A. Psychometric Validation of the English and French Versions of the Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5). PLoS ONE 2016, 11, e0161645. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.W.; Blake, D.D.; Schnurr, P.P.; Kaloupek, D.G.; Marx, B.P.; Keane, T.M.; The clinician-administered PTSD scale for DSM-5 (CAPS-5). Interview Available from the National Center for PTSD at Www Ptsd va Gov 2013. Available online: https://www.ptsd.va.gov (accessed on 14 October 2019).
- Chevalier, J.; de Pouvourville, G. Valuing EQ-5D using time trade-off in France. Eur. J. Health Econ. 2013, 14, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Sauvaget, A.; Lagalice, L.; Schirr-Bonnans, S.; Volteau, C.; Péré, M.; Dert, C.; Rivalland, A.; Tessier, F.; Lepage, A.; Tostivint, A. Cost-utility analysis of transcranial direct current stimulation (tDCS) in non-treatment-resistant depression: The DISCO randomised controlled study protocol. BMJ Open 2020, 10, e033376. [Google Scholar] [CrossRef] [Green Version]
- Shenoy, S.; Bose, A.; Chhabra, H.; Dinakaran, D.; Agarwal, S.M.; Shivakumar, V.; Narayanaswamy, J.C.; Sivakumar, P.T.; Venkatasubramanian, G. Transcranial Direct Current Stimulation (tDCS) for Auditory Verbal Hallucinations in Schizophrenia During Pregnancy: A Case Report. Brain Stimul. Basic Transl. Clin. Res. Neuromodul. 2015, 8, 163–164. [Google Scholar] [CrossRef]
- Sreeraj, V.S.; Bose, A.; Shanbhag, V.; Narayanaswamy, J.C.; Venkatasubramanian, G.; Benegal, V. Monotherapy With tDCS for Treatment of Depressive Episode During Pregnancy: A Case Report. Brain Stimul. Basic Transl. Clin. Res. Neuromodul. 2016, 9, 457–458. [Google Scholar] [CrossRef]
- Strube, W.; Kirsch, B.; Padberg, F.; Hasan, A.; Palm, U. Transcranial Direct Current Stimulation as Monotherapy for the Treatment of Auditory Hallucinations During Pregnancy: A Case Report. J. Clin. Psychopharmacol. 2016, 36, 534–535. [Google Scholar] [CrossRef]
- Palm, U.; Kirsch, B.; Leitner, D.; Padberg, F. Transcranial direct current stimulation (tDCS) for the treatment of depression during pregnancy: A pilot study. Clin. Neurophysiol. 2017, 128, e17–e18. [Google Scholar] [CrossRef]
- Wilkening, A.; Kurzeck, A.; Dechantsreiter, E.; Padberg, F.; Palm, U. Transcranial alternating current stimulation for the treatment of major depression during pregnancy. Psychiatry Res. 2019, 279, 399–400. [Google Scholar] [CrossRef]
- Vigod, S.N.; Murphy, K.E.; Dennis, C.-L.; Oberlander, T.F.; Ray, J.G.; Daskalakis, Z.J.; Blumberger, D.M. Transcranial direct current stimulation (tDCS) for depression in pregnancy: A pilot randomized controlled trial. Brain Stimul. 2019, 12, 1475–1483. [Google Scholar] [CrossRef] [PubMed]
- Kurzeck, A.K.; Dechantsreiter, E.; Wilkening, A.; Kumpf, U.; Nenov-Matt, T.; Padberg, F.; Palm, U. Transcranial Direct Current Stimulation (tDCS) for Depression during Pregnancy: Results from an Open-Label Pilot Study. Brain Sci. 2021, 11, 947. [Google Scholar] [CrossRef] [PubMed]
- Brunelin, J.; Mondino, M.; Gassab, L.; Haesebaert, F.; Gaha, L.; Suaud-Chagny, M.-F.; Saoud, M.; Mechri, A.; Poulet, E. Examining transcranial direct-current stimulation (tDCS) as a treatment for hallucinations in schizophrenia. Am. J. Psychiatry 2012, 169, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Kurzeck, A.; Kirsch, B.; Weidinger, E.; Padberg, F.; Palm, U. Transcranial Direct Current Stimulation (tDCS) for Depression during Pregnancy: Scientific Evidence and What Is Being Said in the Media—A Systematic Review. Brain Sci. 2018, 8, 155. [Google Scholar] [CrossRef] [Green Version]
- Konstantinou, G.N.; Vigod, S.N.; Mehta, S.; Daskalakis, Z.J.; Blumberger, D.M. A systematic review of non-invasive neurostimulation for the treatment of depression during pregnancy. J. Affect. Disord. 2020, 272, 259–268. [Google Scholar] [CrossRef]
- Pacheco, F.; Guiomar, R.; Brunoni, A.R.; Buhagiar, R.; Evagorou, O.; Roca-Lecumberri, A.; Poleszczyk, A.; Lambregtse-van den Berg, M.; Caparros-Gonzalez, R.A.; Fonseca, A.; et al. Efficacy of non-invasive brain stimulation in decreasing depression symptoms during the peripartum period: A systematic review. J. Psychiatr. Res. 2021, 140, 443–460. [Google Scholar] [CrossRef]
- Haxton, C.; Kelly, S.; Young, D.; Cantwell, R. The Efficacy of Electroconvulsive Therapy in a Perinatal Population: A Comparative Pilot Study. J. ECT 2016, 32, 113–115. [Google Scholar] [CrossRef] [Green Version]
- Rundgren, S.; Brus, O.; Båve, U.; Landén, M.; Lundberg, J.; Nordanskog, P.; Nordenskjöld, A. Improvement of postpartum depression and psychosis after electroconvulsive therapy: A population-based study with a matched comparison group. J. Affect. Disord. 2018, 235, 258–264. [Google Scholar] [CrossRef]
- Rönnqvist, I.; Brus, O.; Hammar, Å.; Landén, M.; Lundberg, J.; Nordanskog, P.; Nordenskjöld, A. Rehospitalization of Postpartum Depression and Psychosis After Electroconvulsive Therapy: A Population-Based Study With a Matched Control Group. J. ECT 2019, 35, 264–271. [Google Scholar] [CrossRef]
- Rudroff, T.; Workman, C.D.; Fietsam, A.C.; Kamholz, J. Response Variability in Transcranial Direct Current Stimulation: Why Sex Matters. Front. Psychiatry 2020, 11, 585. [Google Scholar] [CrossRef]
- Fonteneau, C.; Mondino, M.; Arns, M.; Baeken, C.; Bikson, M.; Brunoni, A.R.; Burke, M.J.; Neuvonen, T.; Padberg, F.; Pascual-Leone, A.; et al. Sham tDCS: A hidden source of variability? Reflections for further blinded, controlled trials. Brain Stimul. 2019, 12, 668–673. [Google Scholar] [CrossRef] [PubMed]
- Bhide, A.; Shah, P.S.; Acharya, G. A simplified guide to randomized controlled trials. Acta Obs. Gynecol. Scand. 2018, 97, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Bjekic, J.; Zivanovic, M.; Filipović, S. Transcranial Direct Current Stimulation (tDCS) for Memory Enhancement. J. Vis. Exp. 2021, 175, e62681. [Google Scholar] [CrossRef]
- Matsumoto, H.; Ugawa, Y. Adverse events of tDCS and tACS: A review. Clin. Neurophysiol. Pract. 2017, 2, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Raimundo, R.J.S.; Uribe, C.E.; Brasil-Neto, J.P. Lack of clinically detectable acute changes on autonomic or thermoregulatory functions in healthy subjects after transcranial direct current stimulation (tDCS). Brain Stimul. 2012, 5, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Dowswell, T.; Bedwell, C.; Lavender, T.; Neilson, J.P. Transcutaneous electrical nerve stimulation (TENS) for pain management in labour. Cochrane Database Syst. Rev. 2009, CD007214. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Kim, S.M.; Kwon, J.Y. Repetitive transcranial magnetic stimulation treatment for peripartum depression: Systematic review & meta-analysis. BMC Pregnancy Childbirth 2021, 21, 118. [Google Scholar] [CrossRef]
- Kim, D.R.; Snell, J.L.; Ewing, G.C.; O’Reardon, J. Neuromodulation and antenatal depression: A review. Neuropsychiatr. Dis. Treat. 2015, 11, 975–982. [Google Scholar] [CrossRef] [Green Version]
- Pridmore, S.; Turnier-Shea, Y.; Rybak, M.; Pridmore, W. Transcranial Magnetic Stimulation (TMS) during pregnancy: A fetal risk factor. Australas Psychiatry 2021, 29, 226–229. [Google Scholar] [CrossRef]
- Kibret, B.; Premaratne, M.; Sullivan, C.; Thomson, R.H.; Fitzgerald, P.B. Electroconvulsive therapy (ECT) during pregnancy: Quantifying and assessing the electric field strength inside the foetal brain. Sci. Rep. 2018, 8, 4128. [Google Scholar] [CrossRef]
- Alonzo, A.; Fong, J.; Ball, N.; Martin, D.; Chand, N.; Loo, C. Pilot trial of home-administered transcranial direct current stimulation for the treatment of depression. J. Affect. Disord. 2019, 252, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Sauvaget, A.; Tostivint, A.; Etcheverrigaray, F.; Pichot, A.; Dert, C.; Schirr-Bonnais, S.; Clouet, J.; Sellal, O.; Mauduit, N.; Leux, C.; et al. Hospital production cost of transcranial direct current stimulation (tDCS) in the treatment of depression. Neurophysiol. Clin. Clin. Neurophysiol. 2019, 49, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Martin, B. Empowerment and freedom in psychiatry. Perspect. Psy. 2017, 56, 211–216. [Google Scholar] [CrossRef]


{kind=link}
| Studies | #Patients | Age (Years) | Term of Pregnancy (Gestational Weeks) | Disease Treated by tES | Type of tES (tES Device) | Anode Position | Cathode Position | Sponge Size | Stimulation Parameters | Results | Tolerance and Adverse Effects | Obstetrical and Fetal Data |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [48] Case report | 1 | 25 | 18 | Schizophrenia | tDCS (pharmacotherapy adjuvant) TCT device | F3-FP1 | T3-P3 | Not stated | 2 mA, 2 × 20 min/day, 3 h between two daily sessions, over 5 days (fade-in/fade-out not stated) | Progressive reduction in AHRS score from 29/42 to 22/42 (–24%) after treatment, then 2/42 (–93%) after one month follow-up. | No adverse effect occurred. | Repeat sonography showed healthy fetus (22 weeks) without any abnormalities, pregnancy was uneventful. |
| [49] Case report | 1 | 23 | 6 | Recurrent depressive disorder | tDCS (monotherapy) Neuroconn DC Stimulator Plus device | F3 | F4 | 25 cm2 | 2 mA, 20 s fade-in/fade-out, 30 min/day, over 10 days | One month after the end of treatment, HAM-D reduced from 18 to 5 (–72%) and HAM-A reduced from 32 to 6 (–81%) and patient was in remission. | Minor adverse effect reported (3/10 sessions) during the fade-in phase: transient, mild burning sensations and fleeting experience of phosphenes | No information about fetal or obstetrical data. |
| [50] Case report | 1 | 36 | 32 | Schizophrenia | tDCS (monotherapy) Eldith DC-Stimulator (NeuroConn, Ilmenau, Germany) | F3 | Tp3 | Not stated | 2 mA, 2 × 20 min/day, 3 h between two daily sessions, over 10 days (fade-in/fade-out not stated) | Changes in clinical scale scores at baseline, 2 weeks and 5 weeks follow-up were respectively: 18/49, 12/49 (–33%), 10/49 (–44%) for PANSS positive; 22/49, 23/49 (+5%), 24/49 (+9%) for PANSS negative; 39/112, 27/112 (–31%), 33/112 (–15%) for PANSS general (i.e., 15% reduction in total PANSS score); 27/42, 0/42 (–100%), 0/42 (–100%) for AHRS; 12/27, 8/27 (–33%), 7/27 (–41%) for CDSS; 45/100, 60/100 (+33), 71/100 (+57%) for GAF. | No adverse effect occurred. | Fetal examination via normal ultrasound at follow-up (35th gestational week) revealed no changes or abnormalities. The spontaneous delivery of the healthy child occurred without any complications. |
| [51] Open label trial | 3 | 23, 28 and 32 | 19 to 31 | Major depressive disorder | tDCS (monotherapy) (device not stated) | F3 | F4 | Not stated | 2 mA, 2 × 30 min/day, over 10 days (interval between two daily sessions not stated) ± 1 × 30 min/day over 10 days (fade-in/fade-out not stated) | Mean HAMD-21 total score reduced from 24.7 ± 10.7 to 15.7 ± 3.7 (–36%) after two weeks, then 7.0 ± 7.1 after four weeks (–72%). Mean baseline BDI-13 declined from 35.3 ± 12.5 to 12.0 ± 1.73 at week 2 (–66%), then to 11.0 ± 2.8 (–69%) at week 4. One patient achieved remission | tDCS was well tolerated, no adverse effect occurred. Mean baseline TMT-A was 25.0 ± 6.4 and changed to 23.3 ± 9.7 (–6.8%) in week 2, and to 18.5 ± 4.9 (–26%) in week 4. Mean baseline TMT-B was 81.0 ± 56.9 and sank to 69.3 ± 42.4 (–14%) in week 2, and to 40.5 ± 12.0 (–50%) in week 4. | No information about fetal or obstetrical data. |
| [52] Case report | 1 | 38 | 6 | Recurrent depressive disorder | Gamma-tACS (monotherapy) NeuroConn DC-Stimulator Plus | F3 | F4 | 35 cm2 | 2 mA, 20 min, 40 Hz, 48,000 cycles, 9 sessions Offset at 1 mA without ramp-in/ramp-out | The scores at baseline, after 9 stimulations and then at 2 weeks follow-up were respectively 19 to 11 (–42%) then 10 (–47%) for HAMD-21; 24 to 12 (–50%) then 9 (–63%) for BDI; 26, 17 (–35%) then 15 (–42%) for PANAS negative affected scores; 15, 22 (+47%) then 30 (+100%) at PANAS positive affected scores After 3 months, the patient was in remission with a HAMD-21 score of 3 (–84%) and a BDI score of 7 (–71%). | Gamma-tACS was well tolerated with only mild phosphenes during stimulation and no further side effects. The scores at baseline, after 9 stimulations and then at 2 weeks follow-up were respectively 25s to 19s (–24%) then 15s (–40%) for TMT-A; and 82s to 50s (–40%) then 35s (–57%) for TMT-B. | No complications reported at 27 gestational weeks. |
| [53] RCT | 20 (10:10) | 26 to 43 (average age: 32.3 ± 4.15) | 21 (median value) | Major depressive disorder | tDCS (monotherapy) Magstim device | F3 | F4 | 35 cm2 | 2 mA (or sham), 1 × 30 min/day, 15 days over 3 weeks (fade-in/fade-out not stated) | At baseline, the total MADRS score was 23.5/60 (SD: 5.15) in the tDCS group, and 26.8/60 (SD: 7.48) in the sham-group. After, treatment, and using analysis of covariance, the estimated marginal mean MADRS score was 11.8/60 (SE: 2.66) in the tDCS group, and 15.4/60 (SE: 2.51) in the sham group (F = 0.97, p = 0.34). After treatment, the remission rate (MADRS score < 10) in the active and sham groups was 37.5% and 22% respectively, increased to 75% in the active group at 4 and 12 weeks postpartum versus 22% and 25% in the sham group. | The only side effects reported more than 3 times in either group was « buzzing » or « tingling » at the electrode site. There was no between-group difference in reported adverse effects. Two withdrawals in each group, for a retention rate of 88%, and the tDCS satisfaction rate was 87.5%. | Maternal heart rate, blood pressure and fetal monitoring were all within normal limits in both groups. No abnormalities noted on continuous fetal monitoring for women ≥ 24 weeks. No serious pregnancy complications reported in either group. Mean gestational age at birth was 39.0 week ± 1.4 in tDCS, and 38.9 week ± 1.1 in sham-control. Mean birth weight was 7.0 lbs ± 0.54 and 7.1 lbs ± 1.2 in tDCS and sham groups respectively. There was 1 child in each group with an Apgar score less than 8 at 1 min after birth and no infants with an Apgar score less than 8 at 5 min after birth. One infant in the tDCS group had a spontaneous preterm birth (36 weeks and 5 days gestation) with no known further sequelae. There were no other neonatal complications. There were no differences between groups on any of the infant developmental-behavioural outcome indicators. |
| [54] Open label pilot trial | 6 | 23 to 43 | 12 to 33 | Recurrent depressive disorder | tDCS (psychotherapy adjuvant) Eldith-DC-stimulator (NeuroCareGroup, Munich, Germany) | F3 | F4 | 35 cm2 | 2 mA, 15 s fade-in/fade-out, 2 × 30 min/day, 10 days, accompanied by standard group psychotherapy sessions twice a week for 90 min each (phase 1) (interval between two daily sessions not stated) ± 1 × 30 min/day over 10 days (n = 4) (phase 2) | In phase 1 (n = 6), mean HAMD-21 total score decreased from 22.50 ± 7.56 to 13.67 ± 3.93 (–39%) after two weeks: two patients were responders defined by a 50% reduction of the HAMD-21 total score. Mean BDI-13 total score decreased from 26 ± 13.90 to 11.17 ± 5.46 (–57%) after two weeks: two patients were responders, and one patient was in remission defined by a HAMD-21 total score ≤ 7. CGI improved by 28.57%. Significant improvement of the WHOQOL “Psychological health “ sub-score. For patients who have completed phases 1 + 2 (n = 4), no significant reduction was found in HAMD-21 and BDI-13 sum scores after the phase 2. | The tDCS was well tolerated with no serious adverse effects. Patients reported the following transient adverse effects in association with tDCS: mild headache, phosphenes, and feeling of itching. The mean scores for CRQ questions 1, 2 and 3 were 19.8, 14.6 and 1.5, respectively. The TMT-A/B scores did not change during the phase 1. For patients who have completed phases 1 + 2 (n = 4), only TMT-A showed significant reduction (baseline: 25.79 ± 4.91; after phase 2: 19.33 ± 3.20). | Irregularities of fetal and maternal health were not detected during prenatal and neonatal periods in regularly performed check-ups in accordance with the obstetricians, including fetal heart rate measurement. |
| Current report #1 | 1 | 28 | 3 to 5 | Bipolar type 2 depression | tDCS (pharmacotherapy adjuvant) Soterix device | F3 | F4 | 25 cm2 | 2 mA, 15 s fade-in/fade-out, 1 × 30 min/day, 5 days per week, over 3 consecutives weeks | Reduction in MADRS scores from 32/60 to 15/60 (–53%) four days after the end of treatment, then 18/60 (–43%) and 13/60 (–59%) at 2 months and 6 months respectively. Improvement in BDI-13 scores from 21/39 to 12/39 (–43%) four days after the end of treatment, then 12/39 (–43%) and 11/39 (–48%) at 2 months and 6 months respectively. Improved quality of life (EroQol-5D scores from 40/100 to 50/100 (+25%)). | tDCS was well tolerated without severe adverse effect. The patient reported paresthesia of the scalp during the tDCS sessions and asthenia after the sessions. MoCA scores improved from 25/30 to 26/30 after treatment. | The pregnancy went well with an induced labor at 40 weeks and 5 days. The baby was born healthy (Apgar score 10/10 at one minute, birth weight: 3.500 kg) |
| Current report #2 | 1 | 34 | 3 | PTSD | Sham (placebo) tDCS during the reading of a traumatic script (pharmacotherapy adjuvant) Starstim device (NeuroElectrics, Barcelona, Spain) NIC software | F3 | Fp2 | 20 cm2 | Sham stimulation, 30 s fade-in/fade-out, 2 sessions/day, over 5 consecutive days, 30 min between two daily sessions | One month after tDCS treatment, reduction in CAPS-5 scores from 23/80 to 17/80 (–26%), PCL-5 from 50/80 to 35/80 (–30%) and BDI-13 from 12/39 to 8/39 (–33%). PTSD in remission at delivery. | The tDCS was well tolerated with no major adverse effect, the patient reported minor and transient adverse effects during tDCS sessions such as tingling, difficulty concentrating, fatigue, scalp pain, itching, burning or redness. | The pregnancy went well with a scheduled cesarean delivery at 39 weeks and 2 days of amenorrhea for disabling fibromyalgia pain. Birth of a healthy child with a birth weight of 3.120 kg, a birth height of 52 cm, Apgar scores of 10/10 at one and five minutes, arterial pH of 7.31. |
| Current report #3 | 1 | 28 | Breastfeeding woman during the postpartum period | Recurrent depressive disorder | tDCS (pharmacotherapy adjuvant) Starstim device (NeuroElectrics, Barcelona, Spain) NIC software | F3 | F4 | 25 cm2 | 2 mA, 15 s fade-in/fade-out, 1 × 30 min/day, 5 days per week, over 3 consecutives weeks, then 4 weekly maintenance tDCS sessions | Reduction of MADRS score from 36/60 to 25/60 (–30%) after tDCS treatment with a relapse of depression at 1 month. | The side effects reported were minor and transient, included mild fatigue, paresthesias of the scalp, and a headache of low intensity. | Not applicable |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laurin, A.; Nard, N.; Dalmont, M.; Bulteau, S.; Bénard, C.; Bonnot, O.; Winer, N.; Dupont, F.; Apter, G.; Terranova-Commessie, F.; et al. Efficacy and Safety of Transcranial Electric Stimulation during the Perinatal Period: A Systematic Literature Review and Three Case Reports. J. Clin. Med. 2022, 11, 4048. https://doi.org/10.3390/jcm11144048
Laurin A, Nard N, Dalmont M, Bulteau S, Bénard C, Bonnot O, Winer N, Dupont F, Apter G, Terranova-Commessie F, et al. Efficacy and Safety of Transcranial Electric Stimulation during the Perinatal Period: A Systematic Literature Review and Three Case Reports. Journal of Clinical Medicine. 2022; 11(14):4048. https://doi.org/10.3390/jcm11144048
Chicago/Turabian StyleLaurin, Andrew, Noémie Nard, Marine Dalmont, Samuel Bulteau, Cloé Bénard, Olivier Bonnot, Norbert Winer, Françoise Dupont, Gisèle Apter, Frédérique Terranova-Commessie, and et al. 2022. "Efficacy and Safety of Transcranial Electric Stimulation during the Perinatal Period: A Systematic Literature Review and Three Case Reports" Journal of Clinical Medicine 11, no. 14: 4048. https://doi.org/10.3390/jcm11144048
APA StyleLaurin, A., Nard, N., Dalmont, M., Bulteau, S., Bénard, C., Bonnot, O., Winer, N., Dupont, F., Apter, G., Terranova-Commessie, F., Guillin, O., El-Hage, W., Sauvaget, A., & Rothärmel, M. (2022). Efficacy and Safety of Transcranial Electric Stimulation during the Perinatal Period: A Systematic Literature Review and Three Case Reports. Journal of Clinical Medicine, 11(14), 4048. https://doi.org/10.3390/jcm11144048