
Gait Characterization and Analysis of Hereditary Amyloidosis Associated with Transthyretin Patients: A Case Series

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Assessment
2.3. Experimental Setup
2.4. Marker Setup and Biomechanical Model
2.5. Experimental Procedures
2.6. Data Processing
2.7. Statistical Analysis
3. Results
3.1. Clinical Assessment
3.2. Summary of Results
3.2.1. Linear Kinematics
3.2.2. Ground Reaction Forces
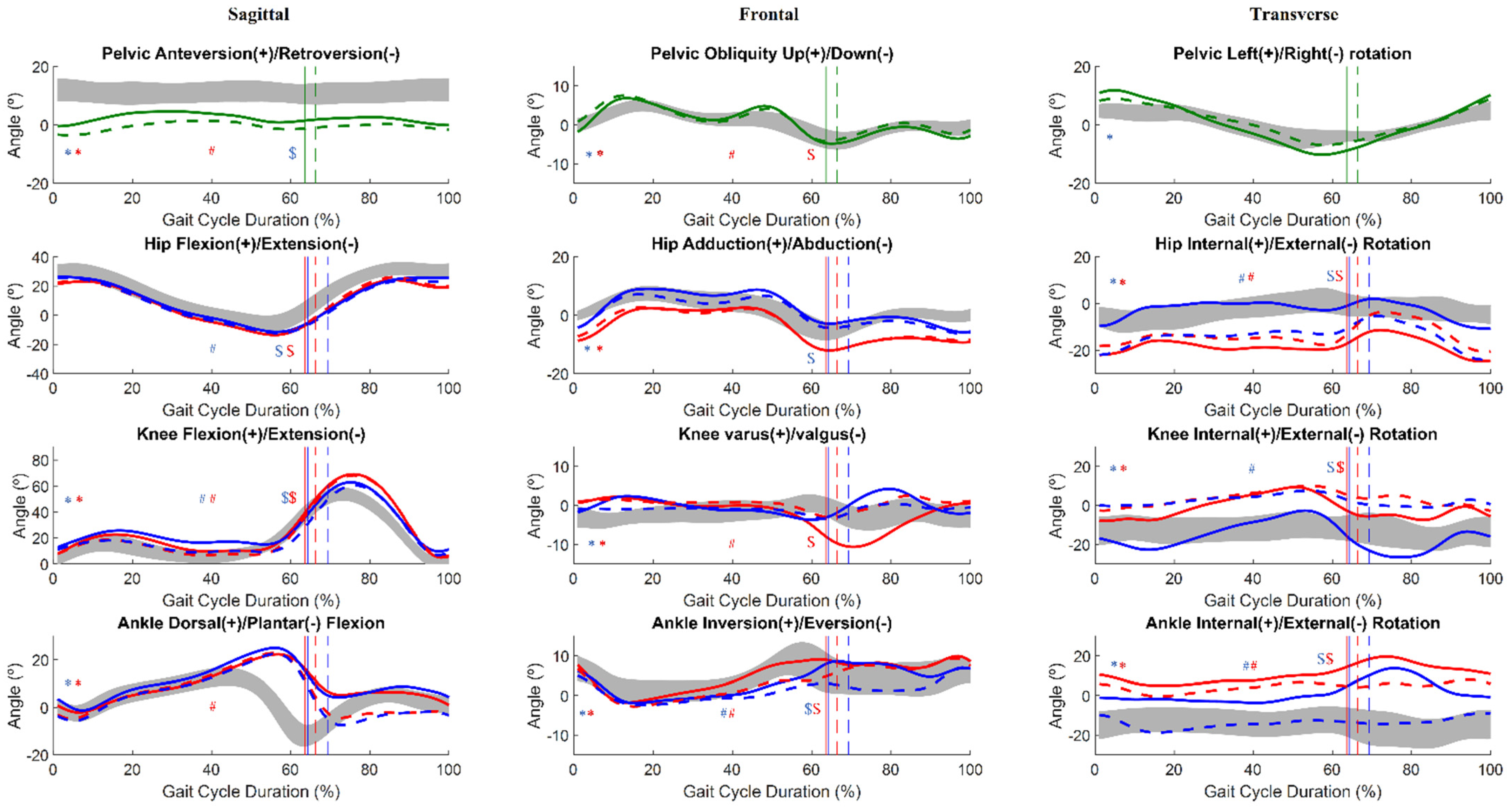
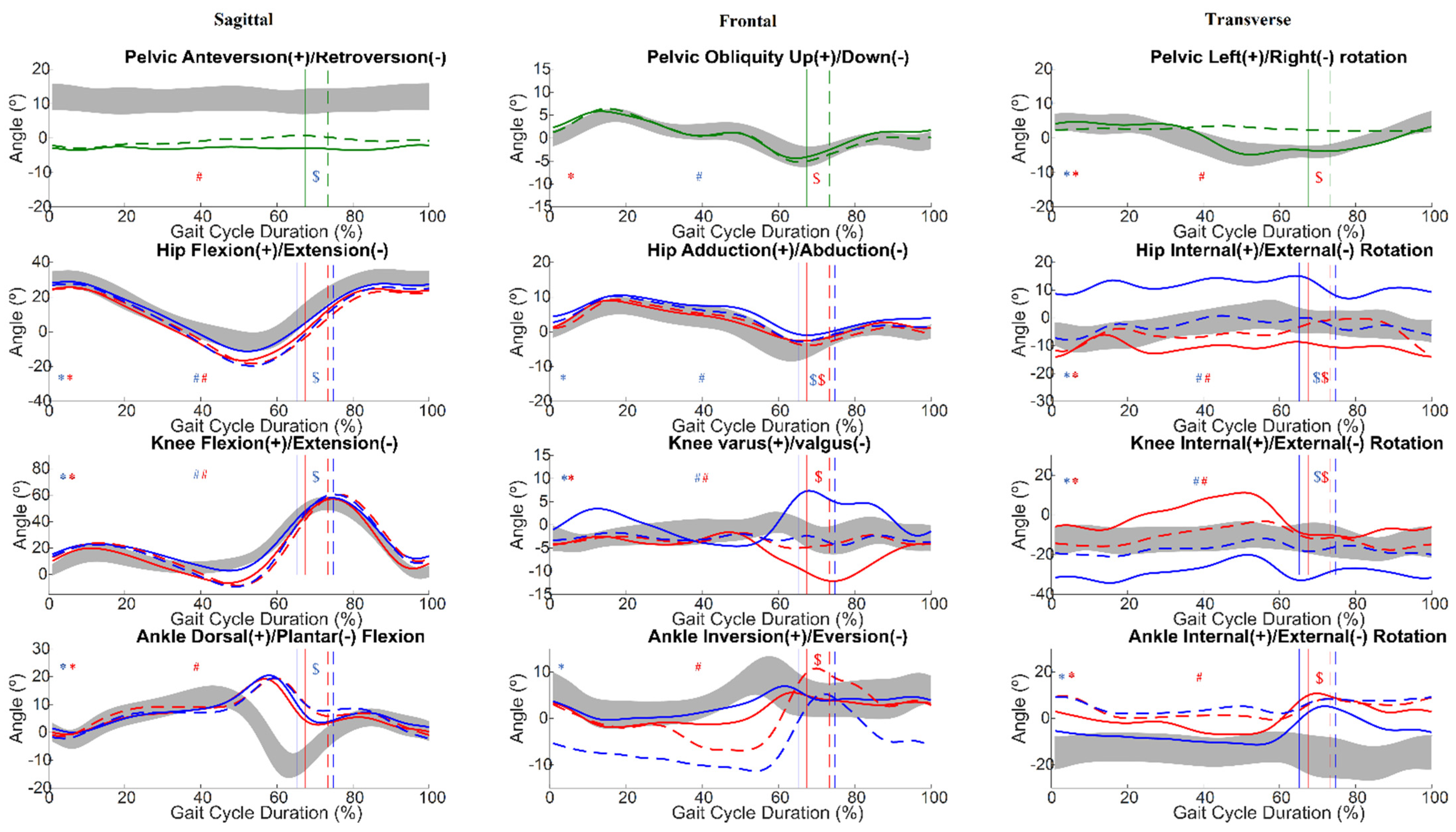
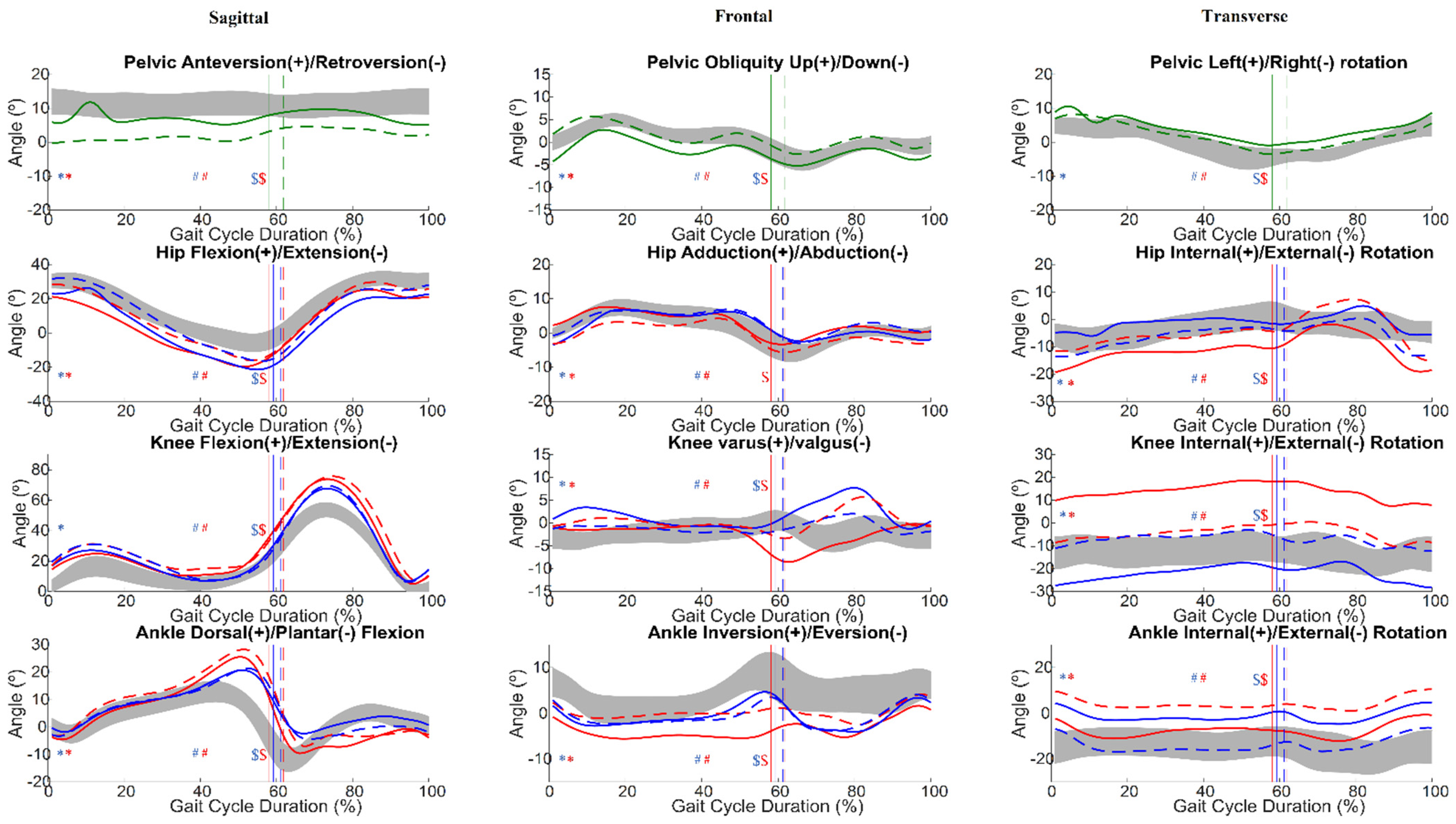
3.2.3. Angular Kinematics
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Spatiotemporal Analysis
Appendix A.1. Participant 1

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | T0 | T1 | ||
|---|---|---|---|---|
| LLL | RLL | LLL | RLL | |
| Speed (m/s) | 0.955 | 0.826 | ||
| Stride width (m) | 0.156 ± 0.021 | 0.156 ± 0.025 | ||
| Stride length (m) | 1.088 ± 0.034 | 0.995 ± 0.038 | ||
| Step length (m) | 0.529 ± 0.023 | 0.559 ± 0.019 | 0.487 ± 0.029 | 0.503 ± 0.020 |
| Double Limb Support (s) | 0.158 ± 0.026 | 0.157 ± 0.013 | 0.160 ± 0.016 | 0.172 ± 0.027 |
| Cycle Time (s) | 1.137 ± 0.053 | 1.143 ± 0.084 | 1.183 ± 0.04 | 1.225 ± 0.071 |
| Stance Time (%) | 63.6 | 64.3 | 66.3 | 69.3 |
| Swing Time (%) | 36.3 | 36.2 | 37.7 | 38.4 |
| Cadence (steps/min) | 104.163 ± 5.926 | 106.346 ± 6.943 | 97.782 ± 7.512 | 100.591 ± 5.446 |
Appendix A.2. Participant 2
| Parameter | T0 | T1 | ||
|---|---|---|---|---|
| LLL | RLL | LLL | RLL | |
| Speed (m/s) | 0.944 | 0.788 | ||
| Stride width (m) | 0.093 ± 0.046 | 0.108 ± 0.045 | ||
| Stride length (m) | 1.166 ± 0.047 | 1.01 ± 0.046 | ||
| Step length (m) | 0.523 ± 0.022 | 0.634 ± 0.038 | 0.476 ± 0.033 | 0.524 ± 0.031 |
| Double Limb Support (s) | 0.129 ± 0.014 | 0.122 ± 0.016 | 0.166 ± 0.021 | 0.161 ± 0.025 |
| Cycle Time (s) | 1.239 ± 0.047 | 1.228 ± 0.047 | 1.28 ± 0.044 | 1.281 ± 0.057 |
| Stance Time (%) | 61.4 | 59.5 | 61.9 | 62.7 |
| Swing Time (%) | 38.6 | 40.6 | 38.1 | 37.4 |
| Cadence (steps/min) | 99.813 ± 4.258 | 93.951 ± 5.085 | 93.245 ± 5.459 | 93.089 ± 4.858 |
Appendix A.3. Participant 3
| Parameter | T0 | T1 | ||
|---|---|---|---|---|
| LLL | RLL | LLL | RLL | |
| Speed (m/s) | 0.854 | 0.860 | ||
| Stride width (m) | 0.104 ± 0.019 | 0.121 ± 0.022 | ||
| Stride length (m) | 0.959 ± 0.038 | 0.926 ± 0.100 | ||
| Step length (m) | 0.463 ± 0.024 | 0.493 ± 0.024 | 0.431 ± 0.108 | 0.482 ± 0.043 |
| Double Limb Support (s) | 0.151 ± 0.025 | 0.154 ± 0.030 | 0.169 ± 0.044 | 0.149 ± 0.025 |
| Cycle Time (s) | 1.128 ± 0.072 | 1.119 ± 0.053 | 1.079 ± 0.167 | 1.074 ± 0.050 |
| Stance Time (%) | 67.5 | 65.2 | 73.4 | 74.8 |
| Swing Time (%) | 42.4 | 44.6 | 45.2 | 44.6 |
| Cadence (steps/min) | 105.897 ± 6.684 | 107.852 ± 7.452 | 116.099 ± 28.739 | 107.825 ± 11.058 |
Appendix A.4. Participant 4
| Parameter | T0 | T1 | ||
|---|---|---|---|---|
| LLL | RLL | LLL | RLL | |
| Speed (m/s) | 0.669 | 0.757 | ||
| Stride width (m) | 0.177 ± 0.026 | 0.165 ± 0.030 | ||
| Stride length (m) | 0.769 ± 0.046 | 0.845 ± 0.112 | ||
| Step length (m) | 0.371 ± 0.033 | 0.396 ± 0.030 | 0.416 ± 0.036 | 0.434 ± 0.019 |
| Double Limb Support (s) | 0.158 ± 0.025 | 0.167 ± 0.041 | 0.161 ± 0.025 | 0.159 ± 0.036 |
| Cycle Time (s) | 1.148 ± 0.078 | 1.151 ± 0.070 | 1.134 ± 0.054 | 1.103 ± 0.197 |
| Stance Time (%) | 65.5 | 64.0 | 63.6 | 65.8 |
| Swing Time (%) | 36.9 | 36.0 | 36.4 | 37.0 |
| Cadence (steps/min) | 102.715 ± 8.615 | 105.822 ± 8.256 | 106.139 ± 8.520 | 105.713 ± 7.669 |
Appendix A.5. Participant 5
| Parameter | T0 | T1 | ||
|---|---|---|---|---|
| LLL | RLL | LLL | RLL | |
| Speed (m/s) | 0.995 | 0.939 | ||
| Stride width (m) | 0.093 ± 0.022 | 0.117 ± 0.026 | ||
| Stride length (m) | 1.160 ± 0.032 | 1.167 ± 0.064 | ||
| Step length (m) | 0.593 ± 0.016 | 0.561 ± 0.027 | 0.574 ± 0.059 | 0.585 ± 0.027 |
| Double Limb Support (s) | 0.089 ± 0.024 | 0.117 ± 0.013 | 0.123 ± 0.030 | 0.157 ± 0.026 |
| Cycle Time (s) | 1.157 ± 0.033 | 1.170 ± 0.025 | 1.222 ± 0.053 | 1.254 ± 0.061 |
| Stance Time (%) | 58.1 | 59.2 | 61.8 | 61.2 |
| Swing Time (%) | 41.9 | 40.8 | 38.2 | 38.8 |
| Cadence (steps/min) | 98.711 ± 3.223 | 106.280 ± 4.570 | 93.612 ± 7.640 | 98.656 ± 4.491 |
Appendix B. Ground Reaction Forces
Appendix B.1. Participant 1
| Parameter (% Body Weight) | T0 | T1 | Effect Size | |||
|---|---|---|---|---|---|---|
| LLL | RLL | LLL | RLL | LLL | RLL | |
| FA1 | −14.67 ± 2.26 | −16.76 ± 1.96 | −13.32 ± 1.35 | −10.42 ± 1.73 | 0.27 | 0.83 * |
| FA3 | 14.96 ± 2.06 | 15.67 ± 1.82 | 9.58 ± 1.58 | 13.04 ± 1.66 | 0.83 * | 0.69 * |
| FM1 | −5.41 ± 1.77 | −7.06 ± 1.84 | −3.25 ± 1.27 | −2.84 ± 1.06 | 0.50 * | 0.76 * |
| FM2 | 6.38 ± 1.43 | 7.22 ± 0.66 | 6.49 ± 1.38 | 5.43 ± 1.46 | 0.08 | 0.54 * |
| FM3 | 9.13 ± 1.62 | 11.09 ± 0.87 | 9.66 ± 1.31 | 9.94 ± 3.22 | 0.01 | 0.20 |
| FV1 | 115.49 ± 6.12 | 120.25 ± 4.67 | 113.45 ± 5.64 | 108.17 ± 5.54 | 0.08 | 0.72 * |
| FV2 | 74.15 ± 6.63 | 72.83 ± 4.98 | 78.86 ± 4.15 | 83.6 ± 2.77 | 0.24 | 0.77 * |
| FV3 | 102.34 ± 7.55 | 113.24 ± 3.69 | 105.43 ± 3.18 | 113.74 ± 3.92 | 0.60 * | 0.00 |
Appendix B.2. Participant 2
| Parameter (% Body Weight) | T0 | T1 | Effect Size | |||
|---|---|---|---|---|---|---|
| LLL | RLL | LLL | RLL | LLL | RLL | |
| FA1 | −25.64 ± 6.3 | −27.48 ± 5.38 | −25.01 ± 3.27 | −21.52 ± 4.06 | 0.10 | 0.60 * |
| FA3 | 21.12 ± 1.64 | 20.75 ± 1.74 | 18.25 ± 1.15 | 19.57 ± 0.8 | 0.03 * | 0.10 |
| FM1 | −5.29 ± 1.97 | −6.4 ± 2.61 | −3.94 ± 2.02 | −3.33 ± 1.73 | 0.34 | 0.50 * |
| FM2 | 6.66 ± 3.53 | 5.78 ± 2.48 | 6.1 ± 3.22 | 5.88 ± 2.85 | 0.10 | 0.00 |
| FM3 | 5.28 ± 1.56 | 5.99 ± 1.77 | 5.78 ± 2.58 | 4.98 ± 1.65 | 0.00 | 0.13 |
| FV1 | 131.65 ± 4.32 | 127.51 ± 8.19 | 136.91 ± 4.76 | 138.01 ± 6.49 | 0.34 | 0.40 * |
| FV2 | 68.47 ± 5.82 | 68.56 ± 6.82 | 73.63 ± 5.93 | 71.6 ± 7.95 | 0.33 | 0.06 |
| FV3 | 111.74 ± 7.44 | 107.22 ± 6.04 | 107.93 ± 2.59 | 112.05 ± 3.16 | 0.04 | 0.06 |
Appendix B.3. Participant 3
| Parameter (% Body Weight) | T0 | T1 | Effect Size | |||
|---|---|---|---|---|---|---|
| LLL | RLL | LLL | RLL | LLL | RLL | |
| FA1 | −12.9 ± 1.9 | −11.8 ± 1.6 | −13.9 ± 2.3 | −15.8 ± 2.9 | 0.1 | 0.1 |
| FA3 | 12.1 ± 2.1 | 14.6 ± 2.6 | 15.5 ± 1.6 | 15.8 ± 1.2 | 0.0 | 0.0 |
| FM1 | −3.6 ± 1.3 | −4.2 ± 1.7 | −3.4 ± 1.5 | −5.4 ± 1.1 | 0.3 | 0.2 |
| FM2 | 6.2 ± 1.3 | 6.0 ± 1.1 | 7.2 ± 1.5 | 7.7 ± 1.7 | 0.1 | 0.1 |
| FM3 | 6.8 ± 1.0 | 6.8 ± 0.9 | 7.4 ± 1.2 | 7.0 ± 1.4 | 0.3 * | 0.1 |
| FV1 | 111.6 ± 4.9 | 107.8 ± 4.5 | 117.4 ± 5.7 | 116.9 ± 5.1 | 0.3 * | 0.1 |
| FV2 | 76.5 ± 4.3 | 78.6 ± 2.7 | 75.0 ± 2.7 | 75.6 ± 3.7 | 0.5 * | 0.3 |
| FV3 | 108.2 ± 3.2 | 110.6 ± 4.1 | 113.7 ± 5.1 | 113.3 ± 5.5 | 0.8 * | 0.3 |
Appendix B.4. Participant 4
| Parameter (% body weight) | T0 | T1 | Effect Size | |||
|---|---|---|---|---|---|---|
| LLL | RLL | LLL | RLL | LLL | RLL | |
| FA1 | −17.5 ± 4.4 | −17.2 ± 3.2 | −14.5 ± 3.2 | −17.1 ± 2.0 | 0.16 | 0.00 |
| FA3 | 12.6 ± 2.4 | 14.6 ± 1.9 | 14.0 ± 1.3 | 11.9 ± 1.6 | 0.29 | 0.56 * |
| FM1 | −2.3 ± 3.7 | −3.5 ± 1.3 | −1.4 ± 1.4 | −3.33 ± 1.7 | 0.00 | 0.00 |
| FM2 | 10.7 ± 1.4 | 11.4 ± 1.4 | 10.6 ± 1.3 | 10.7 ± 2.9 | 0.04 | 0.05 |
| FM3 | 9.9 ± 1.6 | 9.7 ± 1.3 | 9.4 ± 1.5 | 9.9 ± 1.7 | 0.06 | 0.03 |
| FV1 | 107.0 ± 10.1 | 116.0 ± 3.9 | 105.0 ± 5.0 | 109.7 ± 4.4 | 0.00 | 0.54 * |
| FV2 | 95.6 ± 6.2 | 92.7 ± 4.1 | 85.2 ± 2.6 | 85.3 ± 3.7 | 0.69 * | 0.66 * |
| FV3 | 103.7 ± 5.9 | 103.3 ± 3.5 | 108.1 ± 4.6 | 98.8 ± 6.6 | −0.40 | −0.50 * |
Appendix B.5. Participant 5
| Parameter (% Body Weight) | T0 | T1 | Effect Size | |||
|---|---|---|---|---|---|---|
| LLL | RLL | LLL | RLL | LLL | RLL | |
| FA1 | −17.8 ± 4.8 | −16.9 ± 3.3 | −17.6 ± 2.0 | −17.9 ± 3.6 | 0.02 | 0.03 |
| FA3 | 17.3 ± 1.8 | 17.3 ± 2.7 | 15.0 ± 1.5 | 17.0 ± 0.9 | 0.61 * | 0.00 |
| FM1 | −7.5 ± 2.3 | −7.6 ± 2.8 | −4.7 ± 1.2 | −8.0 ± 2.2 | −0.58 * | 0.03 |
| FM2 | 4.8 ± 1.4 | 5.4 ± 1.5 | 6.2 ± 1.0 | 5.0 ± 1.1 | 0.29 * | 0.03 |
| FM3 | 7.5 ± 1.9 | 7.6 ± 1.9 | 6.5 ± 0.9 | 8.8 ± 1.1 | 0.21 | 0.25 |
| FV1 | 113.9 ± 4.2 | 114.2 ± 4.8 | 114.0 ± 4.1 | 116.2 ± 3.7 | 0.00 | 0.17 |
| FV2 | 79.6 ± 4.1 | 78.2 ± 4.3 | 80.1 ± 4.1 | 79.1 ± 2.9 | 0.03 | 0.03 |
| FV3 | 112.4 ± 8.2 | 113.6 ± 6.3 | 110.2 ± 5.1 | 104.5 ± 35.9 | −0.24 | −0.16 |
Appendix C. Angular Kinematics
Appendix C.1. Participant 1
| Joint Angle (Degrees) | Time of Assessment | Left Lower Limb | Right Lower Limb | ||||
|---|---|---|---|---|---|---|---|
| HS | MD | TO | HS | MD | TO | ||
| Pelvis | T0 | 4.07 ± 0.86 | −0.55 ± 0.83 | 6.57 ± 0.64 | −2.08 ± 1.02 | 1.31 ± 1.06 | −4.85 ± 0.76 |
| T1 | 3.62 ± 1.15 | 0.57 ± 0.49 | 6.83 ± 0.78 | 0.26 ± 1.55 | 1.16 ± 0.84 | −3.78 ± 0.80 | |
| p-value | 0.016 a | 0.011 a | 0.213 b | 0.000 a | 0.305 c | 0.003 a | |
| Left Hip | T0 | 20.31 ± 1.98 | 1.26 ± 1.87 | −5.11 ± 2.44 | −11.56 ± 1.21 | 21.09 ± 7.36 | 19.98 ± 2.08 |
| T1 | 21.36 ± 2.10 | 0.23 ± 1.58 | −2.98 ± 2.95 | −10.38 ± 2.20 | 24.98 ± 1.65 | 17.91 ± 3.05 | |
| p-value | 0.083 a | 0.083 a | 0.022 a | 0.134 b | 0.000 a | 0.011 a | |
| Right Hip | T0 | −9.83 ± 1.36 | 21.55 ± 1.97 | 21.47 ± 2.33 | 25.93 ± 1.28 | 3.98 ± 5.54 | −4.28 ± 1.9 |
| T1 | −11.09 ± 1.45 | 20.76 ± 2.90 | 17.81 ± 3.39 | 24.43 ± 3.20 | −0.46 ± 1.76 | −5.17 ± 2.23 | |
| p-value | 0.025 b | 0.334 c | 0.001 a | 0.016 b | 0.000 a | 0.691 c | |
| Left Knee | T0 | 7.31 ± 1.47 | 12.4 ± 1.9 | 43.56 ± 3.83 | 10.15 ± 0.48 | 59.47 ± 11.38 | 22.08 ± 3.77 |
| T1 | 7.60 ± 1.50 | 8.05 ± 2.32 | 40.56 ± 4.44 | 7.11 ± 1.33 | 60.85 ± 2.03 | 17.84 ± 3.31 | |
| p-value | 0.697 c | 0.000 a | 0.008 b | 0.000 a | 0.741 c | 0.001 a | |
| Right Knee | T0 | 15.09 ± 1.58 | 53.61 ± 1.42 | 25.47 ± 2.99 | 12.52 ± 1.38 | 16.85 ± 3.05 | 40.46 ± 5.38 |
| T1 | 9.01 ± 0.84 | 51.67 ± 4.96 | 18.4 ± 4.26 | 10.58 ± 3.32 | 8.81 ± 1.93 | 35.48 ± 5.14 | |
| p-value | 0.000 a | 0.460 c | 0.000 a | 0.030 b | 0.000 a | 0.639 c | |
| Left Ankle | T0 | −3.86 ± 0.97 | 8.56 ± 0.91 | 7.08 ± 3.31 | 20.2 ± 0.74 | −2.45 ± 5.37 | 1.69 ± 1.76 |
| T1 | −3.31 ± 1.53 | 9.57 ± 1.10 | 8.74 ± 2.53 | 21.58 ± 1.05 | −1.89 ± 1.50 | 2.42 ± 1.70 | |
| p-value | 0.247 c | 0.000 a | 0.068 b | 0.017 b | 0.073 b | 0.017 b | |
| Right Ankle | T0 | 22.7 ± 1.87 | 7.19 ± 0.59 | 3.34 ± 1.55 | 3.37 ± 0.79 | 10.21 ± 2.05 | 12.01 ± 2.84 |
| T1 | 20.45 ± 1.68 | 6.54 ± 1.30 | 2.78 ± 2.29 | 0.26 ± 1.68 | 8.5 ± 1.72 | 12.63 ± 2.10 | |
| p-value | 0.000 a | 0.053 a | 0.768 c | 0.000 a | 0.006 b | 0.427 c | |
| Joint Angle (Degrees) | Time of Assessment | Left Lower Limb | Right Lower Limb | ||||
|---|---|---|---|---|---|---|---|
| HS | MD | TO | HS | MD | TO | ||
| Pelvis | T0 | −2.07 ± 1.17 | −2.48 ± 1.73 | −2.96 ± 1.34 | 0.23 ± 1.02 | −4.57 ± 1.98 | −1.62 ± 1.51 |
| T1 | −0.01 ± 1.31 | −0.48 ± 1.21 | 0.19 ± 2.78 | 2.59 ± 1.75 | −2.24 ± 1.87 | 0.24 ± 1.82 | |
| p-value | 0.000 a | 0.001 a | 0.000 a | 0.000 a | 0.002 b | 0.047 b | |
| Left Hip | T0 | −8.80 ± 1.30 | 1.37 ± 0.98 | −11.91 ± 1.02 | −0.28 ± 1 | −7.28 ± 2.07 | 1.71 ± 1.62 |
| T1 | −7.61 ± 1.49 | 0.73 ± 0.98 | −12.27 ± 1.49 | −1.34 ± 1.59 | −7.41 ± 1.13 | 2.20 ± 1.36 | |
| p-value | 0.000 a | 0.234 a | 0.147 a | 0.009 b | 0.244 a | 0.338 b | |
| Right Hip | T0 | 6.57 ± 1.05 | −0.70 ± 1.04 | 7.99 ± 1.54 | −4.97 ± 1.90 | 6.06 ± 3.15 | −2.99 ± 1.06 |
| T1 | 5.51 ± 1.53 | −2.25 ± 1.16 | 6.96 ± 1.35 | −4.66 ± 2.01 | 4.36 ± 1.62 | −4.39 ± 1.32 | |
| p-value | 0.007 a | 0.003 c | 0.042 b | 0.715 c | 0.006 c | 0.046 a | |
| Left Knee | T0 | 0.60 ± 0.47 | −0.27 ± 0.48 | −8.66 ± 1.03 | −1.01 ± 0.69 | −5.76 ± 1.76 | 1.95 ± 2.43 |
| T1 | 1.13 ± 0.60 | 0.77 ± 0.55 | −3.08 ± 1.18 | 0.46 ± 0.40 | 2.13 ± 1.74 | 1.50 ± 1.10 | |
| p-value | 0.001 a | 0.000 a | 0.254 a | 0.000 a | 0.254 a | 0.733 c | |
| Right Knee | T0 | 2.98 ± 1.41 | 4.07 ± 2.26 | 2.36 ± 2.05 | −1.67 ± 0.89 | −0.56 ± 1.06 | −2.40 ± 2.18 |
| T1 | −1.22 ± 0.67 | 0.38 ± 1.54 | −0.89 ± 1.06 | −0.79 ± 1.82 | −0.71 ± 0.63 | −3.48 ± 1.03 | |
| p-value | 0.254 b | 0.001 a | 0.000 a | 0.217 c | 0.099 c | 0.069 b | |
| Left Ankle | T0 | 7.71 ± 1.04 | 1.62 ± 1.04 | 9.07 ± 1.21 | 7.85 ± 0.95 | 7.40 ± 0.72 | −1.74 ± 0.51 |
| T1 | 6.65 ± 1.05 | −0.54 ± 1.67 | 5.42 ± 1.93 | 3.41 ± 1.22 | 6.74 ± 1.04 | −3.29 ± 1.31 | |
| p-value | 0.002 a | 0.001 a | 0.000 a | 0.000 a | 0.027 b | 0.000 a | |
| Right Ankle | T0 | 3.01 ± 1.23 | 7.19 ± 0.76 | −1.77 ± 0.99 | 6.36 ± 1.05 | −0.26 ± 2.13 | 8.27 ± 1.70 |
| T1 | 1.07 ± 1.31 | 1.43 ± 0.89 | −2.66 ± 1.37 | 5.18 ± 1.37 | −1.17 ± 1.32 | 3.00 ± 1.18 | |
| p-value | 0.002 a | 0.000 a | 0.130 b | 0.004 a | 0.455 c | 0.000 a | |
| Joint Angle (Degrees) | Time of Assessment | Left Lower Limb | Right Lower Limb | ||||
|---|---|---|---|---|---|---|---|
| HS | MD | TO | HS | MD | TO | ||
| Pelvis | T0 | 80.93 ± 2.86 | 89.49 ± 1.12 | 98.11 ± 2.35 | 100.6 ± 2.45 | 90.25 ± 3.55 | 82.35 ± 2.64 |
| T1 | 83.66 ± 2.87 | 89.69 ± 2.64 | 96.84 ± 3.09 | 98.55 ± 3.08 | 91.15 ± 2.88 | 83.64 ± 2.83 | |
| p-value | 0.000 a | 0.691 c | 0.050 b | 0.019 b | 0.322 c | 0.360 b | |
| Left Hip | T0 | −23.28 ± 2.89 | −19.29 ± 1.27 | −16.00 ± 2.73 | −19.69 ± 1.42 | −15.07 ± 1.91 | −15.77 ± 5.17 |
| T1 | −19.3 ± 2.52 | −14.91 ± 2.65 | −11.03 ± 2.96 | −15.01 ± 2.52 | −6.70 ± 2.25 | −14.15 ± 2.61 | |
| p-value | 0.001 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.434 b | |
| Right Hip | T0 | −1.85 ± 3.12 | −1.30 ± 3.03 | −1.29 ± 3.38 | −10.04 ± 2.16 | −0.45 ± 4.58 | −0.58 ± 4.13 |
| T1 | −11.79 ± 2.46 | −10.74 ± 3.39 | −14.44 ± 2.84 | −22.56 ± 3.21 | −13.85 ± 2.76 | −8.82 ± 2.55 | |
| p-value | 0.001 b | 0.001 a | 0.000 a | 0.000 a | 0.000 a | 0.003 a | |
| Left Knee | T0 | −7.00 ± 3.02 | 2.24 ± 1.69 | −4.02 ± 4.30 | 10.41 ± 3.19 | −6.85 ± 4.43 | −7.45 ± 3.09 |
| T1 | −3.00 ± 2.52 | 4.34 ± 3.04 | 5.29 ± 2.93 | 9.51 ± 2.32 | 2.54 ± 1.30 | −0.74 ± 2.70 | |
| p-value | 0.000 a | 0.009 b | 0.000 a | 0.114 c | 0.000 b | 0.001 a | |
| Right Knee | T0 | 15.09 ± 1.58 | −25.87 ± 2.23 | −22.64 ± 4.00 | −16.74 ± 1.99 | −12.43 ± 2.75 | −18.55 ± 7.88 |
| T1 | 7.42 ± 2.14 | −0.95 ± 3.71 | 0.48 ± 3.87 | 0.21 ± 3.52 | 4.18 ± 2.18 | 1.46 ± 2.24 | |
| p-value | 0.000 a | 0.052 a | 0.000 a | 0.000 a | 0.001 a | 0.001 b | |
| Left Ankle | T0 | 10.81 ± 2.34 | 7.44 ± 1.98 | 15.45 ± 2.39 | 9.9 ± 2.02 | 16.11 ± 2.14 | 5.16 ± 2.27 |
| T1 | 5.66 ± 1.17 | 2.59 ± 2.60 | 4.75 ± 2.04 | 6.55 ± 1.84 | 4.91 ± 1.06 | −1.14 ± 2.31 | |
| p-value | 0.000 a | 0.001 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Right Ankle | T0 | −0.85 ± 1.37 | 10.52 ± 1.85 | −1.91 ± 1.46 | −0.88 ± 1.18 | −3.22 ± 1.56 | 6.37 ± 5.38 |
| T1 | −12.64 ± 2.96 | −13.59 ± 1.73 | −18.66 ± 3.13 | −9.70 ± 1.89 | −15.06 ± 2.78 | −13.00 ± 2.27 | |
| p-value | 0.000 a | 0.001 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |

Appendix C.2. Participant 2
| Joint Angle (Degrees) | Time of Assessment | Left Lower Limb | Right Lower Limb | ||||
|---|---|---|---|---|---|---|---|
| HS | MD | TO | HS | MD | TO | ||
| Pelvis | T0 | 6.53 ± 0.98 | 5.67 ± 0.95 | 2.80 ± 0.86 | −2.10 ± 0.89 | −1.43 ± 1.01 | 0.84 ± 1.35 |
| T1 | 5.94 ± 1.01 | 3.74 ± 0.89 | 1.74 ± 1.00 | −3.77 ± 1.35 | −1.55 ± 1.04 | −0.07 ± 1.37 | |
| p-value | 0.005 a | 0.000 a | 0.004 b | 0.000 a | 0.943 c | 0.003 b | |
| Left Hip | T0 | 27.92 ± 1.70 | 12.99 ± 1.67 | −8.20 ± 1.78 | −10.18 ± 2.69 | 40.50 ± 1.85 | 30.04 ± 2.02 |
| T1 | 24.27 ± 2.15 | 8.75 ± 1.83 | −3.89 ± 2.97 | −14.68 ± 2.83 | 35.52 ± 1.92 | 20.76 ± 5.80 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Right Hip | T0 | −11.71 ± 2.13 | 37.42 ± 2.64 | 30.31 ± 2.08 | 27.06 ± 2.51 | 9.15 ± 1.82 | −4.83 ± 2.17 |
| T1 | −16.24 ± 2.07 | 33.62 ± 2.43 | 20.01 ± 2.25 | 19.29 ± 1.85 | 4.55 ± 1.58 | −3.69 ± 4.28 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.601 c | |
| Left Knee | T0 | 15.81 ± 2.45 | 23.95 ± 3.40 | 43.61 ± 4.68 | 23.63 ± 4.41 | 77.63 ± 2.23 | 35.01 ± 2.68 |
| T1 | 15.36 ± 3.84 | 17.80 ± 2.02 | 47.76 ± 4.34 | 9.2 ± 3.05 | 73.84 ± 2.39 | 31.19 ± 5.12 | |
| p-value | 0.493 c | 0.000 a | 0.006 a | 0.000 a | 0.000 a | 0.000 a | |
| Right Knee | T0 | −1.78 ± 0.84 | 75.87 ± 1.92 | 34.47 ± 3.29 | 15.91 ± 2.85 | 17.54 ± 2.24 | 37.75 ± 3.02 |
| T1 | 1.24 ± 1.95 | 70.13 ± 3.03 | 27.99 ± 3.14 | 10.23 ± 3.00 | 11.75 ± 2.83 | 42.93 ± 7.45 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Left Ankle | T0 | 1.76 ± 1.75 | 28.12 ± 2.66 | 32.94 ± 2.77 | 47.60 ± 3.26 | 8.42 ± 2.11 | 21.92 ± 1.96 |
| T1 | −4.47 ± 2.00 | 9.01 ± 1.90 | 6.68 ± 4.32 | 19.18 ± 2.96 | −12.22 ± 3.30 | 8.97 ± 2.62 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Right Ankle | T0 | 20.36 ± 2.28 | −13.29 ± 2.48 | 5.94 ± 1.58 | −3.13 ± 1.24 | 10.61 ± 1.26 | 16.05 ± 1.83 |
| T1 | 16.87 ± 2.72 | −11.05 ± 2.40 | 8.66 ± 2.39 | −3.93 ± 1.65 | −1.55 ± 1.04 | 8.36 ± 3.59 | |
| p-value | 0.000 a | 0.001 a | 0.000 a | 0.587 c | 0.000 a | 0.000 a | |
| Joint Angle (Degrees) | Time of Assessment | Left Lower Limb | Right Lower Limb | ||||
|---|---|---|---|---|---|---|---|
| HS | MD | TO | HS | MD | TO | ||
| Pelvis | T0 | 1.12 ± 1.20 | 0.22 ± 1.61 | −1.63 ± 1.11 | −1.10 ± 1.07 | 0.29 ± 1.72 | 0.28 ± 1.57 |
| T1 | −0.55 ± 0.82 | −0.67 ± 1.23 | −2.56 ± 1.17 | −2.10 ± 0.99 | −1.63 ± 1.06 | −2.68 ± 0.90 | |
| p-value | 0.000 a | 0.062 c | 0.088 c | 0.017 a | 0.000 a | 0.000 a | |
| Left Hip | T0 | −8.06 ± 1.63 | −1.96 ± 1.68 | −2.70 ± 2.23 | 0.68 ± 2.11 | 2.87 ± 1.34 | 0.75 ± 1.98 |
| T1 | −6.92 ± 2.30 | −1.90 ± 2.09 | −3.31 ± 2.21 | 1.67 ± 2.71 | 0.81 ± 1.95 | 1.42 ± 2.08 | |
| p-value | 0.011 a | 0.833 c | 0.902 c | 0.073 b | 0.000 a | 0.115 b | |
| Right Hip | T0 | 6.37 ± 2.04 | −0.81 ± 1.02 | 0.63 ± 1.79 | −7.76 ± 1.83 | 0.94 ± 2.26 | 1.34 ± 1.48 |
| T1 | 6.60 ± 1.89 | −1.83 ± 1.53 | −0.54 ± 2.48 | −8.90 ± 2.25 | −0.41 ± 2.49 | −0.55 ± 2.56 | |
| p-value | 0.853 a | 0.075 c | 0.285 c | 0.163 b | 0.019 b | 0.001 b | |
| Left Knee | T0 | −2.95 ± 1.42 | −3.45 ± 0.96 | −6.57 ± 2.42 | −3.62 ± 1.73 | −6.39 ± 2.34 | −3.03 ± 1.89 |
| T1 | 1.34 ± 1.11 | 1.34 ± 1.00 | −1.58 ± 2.51 | 1.87 ± 0.94 | 9.49 ± 3.96 | 2.80 ± 2.01 | |
| p-value | 0.001 a | 0.000 a | 0.003 a | 0.000 a | 0.003 a | 0.000 a | |
| Right Knee | T0 | −2.53 ± 1.50 | 12.12 ± 2.20 | 7.41 ± 2.26 | 2.34 ± 0.96 | 3.69 ± 0.83 | 5.99 ± 1.47 |
| T1 | 4.88 ± 1.40 | 12.05 ± 2.66 | 5.15 ± 1.96 | 2.38 ± 1.09 | 4.48 ± 1.11 | 6.51 ± 4.41 | |
| p-value | 0.003 b | 0.361 c | 0.000 a | 0.361 c | 0.093 c | 0.575 c | |
| Left Ankle | T0 | 1.72 ± 1.81 | −10.04 ± 1.08 | −3.13 ± 1.30 | −7.72 ± 1.63 | −5.15 ± 4.05 | −10.37 ± 1.30 |
| T1 | 7.36 ± 1.77 | 4.00 ± 1.01 | 8.75 ± 1.22 | 11.47 ± 1.52 | 5.20 ± 2.69 | 3.50 ± 1.88 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Right Ankle | T0 | 3.83 ± 1.98 | 3.12 ± 2.78 | −3.51 ± 1.19 | 5.03 ± 1.82 | −1.98 ± 1.35 | 5.62 ± 0.57 |
| T1 | 5.48 ± 1.88 | 7.48 ± 2.76 | −3.05 ± 1.93 | 5.95 ± 2.54 | −1.63 ± 1.06 | 3.39 ± 1.92 | |
| p-value | 0.003 b | 0.000 a | 0.463 c | 0.009 a | 0.143 c | 0.000 a | |
| Joint Angle (Degrees) | Time of Assessment | Left Lower Limb | Right Lower Limb | ||||
|---|---|---|---|---|---|---|---|
| HS | MD | TO | HS | MD | TO | ||
| Pelvis | T0 | 80.91 ± 2.70 | 92.93 ± 2.71 | 100.20 ± 2.53 | 106.72 ± 3.43 | 94.48 ± 2.71 | 85.78 ± 2.60 |
| T1 | 82.6 ± 2.62 | 90.43 ± 2.79 | 94.28 ± 2.91 | 98.19 ± 3.48 | 92.22 ± 3.37 | 87.3 ± 2.86 | |
| p-value | 0.001 b | 0.009 c | 0.000 a | 0.000 a | 0.004 b | 0.029 a | |
| Left Hip | T0 | −16.47 ± 4.22 | −9.95 ± 2.08 | −5.65 ± 3.27 | −5.51 ± 4.01 | −2.83 ± 2.74 | −9.63 ± 2.45 |
| T1 | −5.29 ± 3.63 | −2.9 ± 2.52 | 0.54 ± 2.89 | 2.86 ± 3.82 | 10.58 ± 4.37 | −2.21 ± 2.62 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Right Hip | T0 | 1.92 ± 4.55 | 3.28 ± 2.70 | −1.59 ± 3.21 | −9.75 ± 3.28 | −0.48 ± 3.89 | 1.98 ± 3.18 |
| T1 | −1.64 ± 3.13 | 2.62 ± 2.74 | −10.83 ± 3.35 | −22.34 ± 3.15 | −7.56 ± 3.42 | −1.79 ± 7.59 | |
| p-value | 0.001 b | 0.072 c | 0.000 a | 0.000 a | 0.000 a | 0.000 b | |
| Left Knee | T0 | −1.49 ± 3.35 | 2.65 ± 2.32 | −4.43 ± 4.59 | 9.53 ± 4.26 | −10.71 ± 5.35 | −4.58 ± 3.63 |
| T1 | −34.33 ± 3.53 | −22.25 ± 2.00 | −26.19 ± 2.37 | −21.55 ± 2.69 | −29.86 ± 3.74 | −25.85 ± 2.97 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 b | 0.000 a | |
| Right Knee | T0 | 8.29 ± 1.67 | −18.79 ± 2.99 | −29.62 ± 3.14 | −28.71 ± 3.42 | −23.09 ± 1.9 | −30.18 ± 3.10 |
| T1 | −25.11 ± 2.41 | −25.39 ± 4.18 | −24.07 ± 2.52 | −25.85 ± 3.25 | −25.74 ± 1.61 | −32.97 ± 7.68 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.004 b | 0.000 b | 0.067 c | |
| Left Ankle | T0 | 1.48 ± 1.51 | 6.18 ± 1.36 | 10.73 ± 1.84 | 6.07 ± 1.55 | 11.9 ± 4.68 | 5.21 ± 2.39 |
| T1 | 19.63 ± 2.81 | 8.91 ± 1.35 | 15.81 ± 3.15 | 11.73 ± 1.31 | 21.33 ± 4.01 | 8.16 ± 1.46 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Right Ankle | T0 | 0.14 ± 2.08 | 15.31 ± 3.33 | 0.95 ± 1.45 | 4.76 ± 1.25 | −2.09 ± 1.32 | 5.89 ± 2.80 |
| T1 | 0.94 ± 1.46 | 12.09 ± 3.81 | −3.02 ± 1.55 | 10.3 ± 2.42 | 92.22 ± 3.37 | 3.43 ± 2.86 | |
| p-value | 0.057 c | 0.002 c | 0.000 a | 0.000 a | 0.000 a | 0.001 a | |

Appendix C.3. Participant 3
| Joint Angle (Degrees) | Time of Assessment | Left Lower Limb | Right Lower Limb | ||||
|---|---|---|---|---|---|---|---|
| HS | MD | TO | HS | HS | MD | ||
| Pelvis | T0 | 0.68 ± 0.84 | 0.28 ± 0.59 | 5.71 ± 0.69 | 2.12 ± 0.67 | 1.82 ± 0.69 | −4.31 ± 0.71 |
| T1 | 0.60 ± 1.72 | −0.79 ± 0.87 | 6.26 ± 1.13 | 0.89 ± 1.17 | 1.64 ± 0.87 | −5.30 ± 0.77 | |
| p-value | 0.812 c | 0.000 a | 0.013 b | 0.000 a | 0.480 c | 0.000 a | |
| Left Hip | T0 | 24.31 ± 1.57 | 2.80 ± 0.89 | −5.20 ± 2.26 | −16.05 ± 1.51 | 23.84 ± 1.49 | 19.7 ± 3.26 |
| T1 | 23.45 ± 4.22 | 2.43 ± 2.22 | −5.02 ± 5.11 | −19.19 ± 2.50 | 22.80 ± 3.48 | 19.00 ± 3.20 | |
| p-value | 0.057 b | 0.057 b | 0.657 c | 0.000 a | 0.008 b | 0.302 c | |
| Right Hip | T0 | −11.48 ± 4.40 | 25.41 ± 2.31 | 23.54 ± 2.98 | 27.85 ± 2.51 | 6.91 ± 3.45 | 0.47 ± 3.29 |
| T1 | −18.07 ± 5.30 | 23.39 ± 2.27 | 20.85 ± 7.73 | 25.87 ± 3.12 | 2.20 ± 2.58 | −5.90 ± 2.86 | |
| p-value | 0.000 a | 0.000 a | 0.004 b | 0.001 b | 0.000 a | 0.000 a | |
| Left Knee | T0 | 9.81 ± 2.38 | 4.35 ± 0.94 | 32.07 ± 4.94 | −4.89 ± 2.2 | 46.2 ± 2.64 | 17.6 ± 3.92 |
| T1 | 12.89 ± 4.21 | 8.16 ± 1.55 | 34.92 ± 6.12 | −8.55 ± 2.52 | 49.19 ± 5.58 | 22.59 ± 2.51 | |
| p-value | 0.002 b | 0.000 a | 0.035 c | 0.000 a | 0.001 b | 0.000 a | |
| Right Knee | T0 | 3.77 ± 1.03 | 49.62 ± 3.39 | 23.12 ± 3.92 | 15.3 ± 3.63 | 12.58 ± 5.45 | 40.2 ± 5.71 |
| T1 | −8.02 ± 5.92 | 51.14 ± 3.63 | 21.04 ± 5.88 | 12.4 ± 4.49 | 6.88 ± 3.42 | 35.76 ± 5.27 | |
| p-value | 0.000 a | 0.087 c | 0.008 b | 0.001 b | 0.000 a | 0.001 b | |
| Left Ankle | T0 | 1.21 ± 1.30 | 6.61 ± 1.19 | 9.94 ± 3.13 | 14.11 ± 2.37 | 5.65 ± 0.77 | 2.58 ± 1.51 |
| T1 | −0.90 ± 2.35 | 9.03 ± 1.14 | 12.8 ± 3.39 | 13.17 ± 2.38 | 6.97 ± 1.13 | 6.08 ± 1.79 | |
| p-value | 0.029 b | 0.000 a | 0.001 b | 0.000 a | 0.000 b | 0.000 a | |
| Right Ankle | T0 | 15.55 ± 5.38 | 7.45 ± 2.15 | 2.77 ± 1.34 | 1.81 ± 1.56 | 7.54 ± 1.86 | 11.97 ± 4.39 |
| T1 | 11.18 ± 3.08 | 8.58 ± 1.25 | 3.29 ± 2.38 | −2.13 ± 2.41 | 6.83 ± 1.54 | 13.70 ± 2.41 | |
| p-value | 0.000 a | 0.012 b | 0.307 c | 0.000 a | 0.002 b | 0.155 c | |
| Joint Angle (Degrees) | Time of Assessment | Left Lower Limb | Right Lower Limb | ||||
|---|---|---|---|---|---|---|---|
| HS | MD | TO | HS | MD | TO | ||
| Pelvis | T0 | 2.55 ± 0.67 | 3.38 ± 0.81 | 2.61 ± 0.88 | 2.46 ± 1.01 | 3.10 ± 0.76 | 2.81 ± 0.76 |
| T1 | 0.37 ± 1.61 | 1.49 ± 2.17 | 1.80 ± 1.82 | 1.47 ± 1.47 | 0.98 ± 1.81 | 0.20 ± 2.75 | |
| p-value | 0.000 a | 0.000 b | 0.001 a | 0.000 b | 0.000 a | 0.000 b | |
| Left Hip | T0 | 1.36 ± 1.32 | 6.24 ± 0.70 | −2.41 ± 0.85 | 2.36 ± 0.94 | 1.50 ± 0.74 | 9.19 ± 1.08 |
| T1 | 0.38 ± 2.23 | 6.29 ± 1.08 | −4.07 ± 1.36 | 2.62 ± 1.40 | 0.36 ± 1.05 | 9.28 ± 1.13 | |
| p-value | 0.088 a | 0.044 b | 0.000 a | 0.334 a | 0.000 a | 0.558 b | |
| Right Hip | T0 | 5.79 ± 1.84 | 1.97 ± 0.79 | 10.02 ± 0.91 | 4.18 ± 0.92 | 8.31 ± 0.66 | −1.12 ± 1.51 |
| T1 | 4.14 ± 1.80 | 1.40 ± 1.01 | 9.75 ± 1.39 | 2.30 ± 1.60 | 7.46 ± 1.14 | −3.07 ± 1.32 | |
| p-value | 0.000 b | 0.018 c | 0.088 b | 0.000 a | 0.001 b | 0.000 a | |
| Left Knee | T0 | −4.33 ± 0.52 | −4.43 ± 0.39 | −8.73 ± 0.99 | −1.95 ± 1.02 | −9.91 ± 1.07 | −3.38 ± 1.61 |
| T1 | −4.15 ± 0.86 | −3.75 ± 0.69 | −5.08 ± 0.65 | −1.40 ± 0.92 | −2.10 ± 1.05 | −2.64 ± 1.01 | |
| p-value | 0.596 c | 0.000 a | 0.000 a | 0.011 c | 0.000 a | 0.046 c | |
| Right Knee | T0 | −14.23 ± 3.12 | 5.47 ± 3.00 | 3.11 ± 2.07 | −0.87 ± 1.48 | −1.75 ± 1.16 | 5.82 ± 3.69 |
| T1 | −1.54 ± 1.39 | −3.11 ± 2.01 | −1.66 ± 1.52 | −3.49 ± 1.64 | −3.07 ± 1.02 | −2.85 ± 1.82 | |
| p-value | 0.000 a | 0.463 c | 0.000 a | 0.000 a | 0.075 b | 0.899 c | |
| Left Ankle | T0 | 1.12 ± 1.11 | −0.95 ± 1.89 | 5.51 ± 1.28 | −0.55 ± 1.37 | 3.18 ± 1.09 | −1.68 ± 1.73 |
| T1 | 2.65 ± 1.69 | −1.26 ± 0.82 | 5.78 ± 1.69 | 0.06 ± 0.85 | 3.71 ± 1.13 | −2.12 ± 1.22 | |
| p-value | 0.973 c | 0.392 c | 0.436 c | 0.044 b | 0.026 c | 0.336 c | |
| Right Ankle | T0 | 2.41 ± 6.95 | 4.00 ± 1.93 | −0.29 ± 2.31 | 3.58 ± 1.47 | 0.24 ± 4.80 | 5.82 ± 3.46 |
| T1 | 1.65 ± 1.65 | 1.08 ± 0.83 | −1.93 ± 1.22 | 0.69 ± 1.17 | −1.04 ± 0.95 | 3.92 ± 1.02 | |
| p-value | 0.070 c | 0.000 a | 0.000 b | 0.000 a | 0.509 c | 0.000 a | |
| Joint Angle (Degrees) | Time of Assessment | Left Lower Limb | Right Lower Limb | ||||
|---|---|---|---|---|---|---|---|
| HS | MD | TO | HS | MD | TO | ||
| Pelvis | T0 | 84.81 ± 2.62 | 87.49 ± 1.95 | 93.89 ± 2.17 | 93.89 ± 2.07 | 93.51 ± 2.01 | 86.01 ± 2.63 |
| T1 | 84.55 ± 3.14 | 85.41 ± 2.11 | 92.94 ± 3.45 | 92.11 ± 2.30 | 92.35 ± 2.71 | 84.03 ± 2.16 | |
| p-value | 0.000 a | 0.000 a | 0.294 c | 0.001 a | 0.062 c | 0.008 a | |
| Left Hip | T0 | −14.13 ± 2.01 | −12.67 ± 0.96 | −8.90 ± 1.53 | −10.84 ± 1.36 | −10.26 ± 1.08 | −6.94 ± 3.07 |
| T1 | −13.00 ± 4.62 | −7.60 ± 1.65 | −3.13 ± 4.10 | −5.82 ± 1.81 | −0.08 ± 1.95 | −4.76 ± 2.54 | |
| p-value | 0.017 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.001 b | |
| Right Hip | T0 | 13.18 ± 4.99 | 8.07 ± 3.79 | 12.95 ± 4.49 | 8.91 ± 3.14 | 11.5 ± 4.79 | 14.3 ± 4.77 |
| T1 | 0.31 ± 4.74 | −3.78 ± 3.32 | −2.79 ± 2.51 | −6.39 ± 5.65 | −2.41 ± 2.22 | −0.37 ± 3.74 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Left Knee | T0 | −5.54 ± 2.45 | 2.64 ± 2.19 | −7.47 ± 4.13 | 10.88 ± 2.25 | −11.05 ± 1.74 | −7.20 ± 2.02 |
| T1 | −15.04 ± 3.10 | −8.83 ± 1.86 | −11.05 ± 2.27 | −3.21 ± 1.83 | −15.86 ± 2.11 | −15.77 ± 2.36 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Right Knee | T0 | 4.22 ± 6.81 | −25.63 ± 15.2 | −32.39 ± 15.18 | −30.58 ± 13.86 | −27.93 ± 18.71 | −30.00 ± 14.83 |
| T1 | −14.94 ± 7.28 | −15.91 ± 2.44 | −20.92 ± 2.98 | −19.71 ± 2.86 | −17.64 ± 3.38 | −17.25 ± 2.93 | |
| p-value | 0.000 c | 0.052 c | 0.000 c | 0.000 c | 0.001 c | 0.001 b | |
| Left Ankle | T0 | 1.47 ± 1.46 | −1.54 ± 1.93 | 5.93 ± 3.94 | −6.21 ± 2.30 | 6.62 ± 1.93 | −0.73 ± 2.36 |
| T1 | 9.19 ± 1.70 | 1.09 ± 1.21 | 4.36 ± 2.70 | 1.05 ± 1.06 | 6.34 ± 1.48 | 0.73 ± 1.26 | |
| p-value | 0.000 a | 0.000 a | 0.038 a | 0.000 a | 0.000 c | 0.002 b | |
| Right Ankle | T0 | −13.10 ± 23.26 | −1.69 ± 16.01 | −9.28 ± 17.48 | −6.77 ± 15.44 | −9.95 ± 21.76 | −3.35 ± 17.26 |
| T1 | 5.48 ± 2.22 | 7.41 ± 1.63 | 3.17 ± 1.57 | 9.15 ± 3.21 | 3.08 ± 1.49 | 4.52 ± 1.42 | |
| p-value | 0.000 b | 0.000 b | 0.000 b | 0.000 b | 0.000 b | 0.000 b | |

Appendix C.4. Participant 4
| Joint Angle (Degrees) | Time of Assessment | Left Lower Limb | Right Lower Limb | ||||
|---|---|---|---|---|---|---|---|
| HS | MD | TO | HS | MD | TO | ||
| Pelvis | T0 | −0.35 ± 1.15 | 0.36 ± 1.08 | −0.06 ± 1.03 | −1.55 ± 1.16 | −3.60 ± 1.25 | −4.80 ± 1.07 |
| T1 | 4.89 ± 1.24 | 3.63 ± 0.60 | 5.67 ± 0.86 | 3.25 ± 1.18 | 3.04 ± 0.87 | −0.40 ± 1.16 | |
| p-value | 0.000 a | 0.001 a | 0.000 a | 0.000 a | 0.001 a | 0.000 a | |
| Left Hip | T0 | 30.09 ± 1.93 | 7.93 ± 2.89 | 0.38 ± 6.70 | −9.56 ± 5.68 | 34.19 ± 2.67 | 23.78 ± 2.61 |
| T1 | 24.82 ± 2.39 | 0.02 ± 0.65 | −9.10 ± 3.99 | −17.18 ± 1.97 | 24.8 ± 2.20 | 16.15 ± 5.72 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Right Hip | T0 | −3.29 ± 3.36 | 32.03 ± 2.13 | 27.15 ± 2.28 | 31.33 ± 1.45 | 14.25 ± 1.65 | 0.44 ± 3.10 |
| T1 | −15.27 ± 2.92 | 23.91 ± 1.26 | 20.71 ± 2.05 | 25.20 ± 1.97 | 5.53 ± 1.48 | −9.06 ± 6.02 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Left Knee | T0 | 20.48 ± 3.48 | 18.46 ± 3.54 | 41.9 ± 5.96 | 12.61 ± 5.05 | 65.36 ± 4.20 | 29.78 ± 2.65 |
| T1 | 19.08 ± 3.06 | 15.91 ± 1.81 | 38.49 ± 4.20 | 8.59 ± 3.91 | 62.45 ± 2.89 | 28.74 ± 4.86 | |
| p-value | 0.024 c | 0.014 b | 0.005 b | 0.000 b | 0.094 a | 0.288 c | |
| Right Knee | T0 | −4.05 ± 2.11 | 70.39 ± 4.08 | 35.19 ± 1.94 | 25.25 ± 1.99 | 27.48 ± 2.00 | 45.84 ± 3.07 |
| T1 | 5.51 ± 4.50 | 23.91 ± 1.26 | 30.65 ± 3.07 | 18.87 ± 4.57 | 21.05 ± 1.92 | 40.81 ± 6.26 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.001 b | 0.000 a | |
| Left Ankle | T0 | 3.62 ± 3.58 | 11.63 ± 3.34 | −0.72 ± 2.24 | 18.67 ± 3.70 | −2.96 ± 3.82 | 6.61 ± 3.54 |
| T1 | −0.77 ± 1.63 | 9.64 ± 0.86 | 2.31 ± 3.30 | 15.85 ± 1.50 | −4.55 ± 2.25 | 6.33 ± 2.05 | |
| p-value | 0.800 c | 0.116 b | 0.000 b | 0.312 c | 0.331 c | 0.372 c | |
| Right Ankle | T0 | 20.1 ± 2.19 | −4.37 ± 2.03 | 6.23 ± 1.55 | −4.74 ± 1.37 | 12.64 ± 1.37 | 10.55 ± 2.28 |
| T1 | 18.01 ± 2.70 | −2.58 ± 2.02 | 5.97 ± 2.08 | −3.27 ± 1.65 | 12.16 ± 1.72 | 5.07 ± 3.72 | |
| p-value | 0.001 b | 0.222 a | 0.545 c | 0.000 b | 0.354 b | 0.000 a | |
| Joint Angle (Degrees) | Time of Assessment | Left Lower Limb | Right Lower Limb | ||||
|---|---|---|---|---|---|---|---|
| HS | MD | TO | HS | MD | TO | ||
| Pelvis | T0 | −0.69 ± 1.66 | −3.20 ± 1.95 | −2.72 ± 2.4 | −3.58 ± 1.86 | −1.36 ± 1.84 | −2.99 ± 1.88 |
| T1 | −2.89 ± 1.61 | −5.32 ± 0.57 | −4.70 ± 2.3 | −4.58 ± 1.87 | −3.72 ± 1.48 | −5.44 ± 1.98 | |
| p-value | 0.000 a | 0.037 a | 0.000 b | 0.002 b | 0.024 a | 0.000 a | |
| Left Hip | T0 | 3.49 ± 3.20 | 11.28 ± 2.51 | 5.41 ± 2.16 | 12.79 ± 2.31 | 4.36 ± 1.99 | 12.00 ± 2.12 |
| T1 | 0.48 ± 2.40 | 7.31 ± 1.37 | 1.29 ± 1.65 | 7.25 ± 1.86 | 1.61 ± 1.06 | 9.26 ± 1.50 | |
| p-value | 0.000 b | 0.028 a | 0.000 a | 0.000 a | 0.002 a | 0.000 b | |
| Right Hip | T0 | 4.87 ± 1.71 | −4.88 ± 1.54 | 2.27 ± 1.22 | −2.54 ± 1.96 | 2.17 ± 1.29 | −7.83 ± 1.53 |
| T1 | 10.39 ± 1.93 | −0.45 ± 0.59 | 9.90 ± 1.58 | 3.52 ± 1.70 | 9.51 ± 1.63 | −1.15 ± 1.36 | |
| p-value | 0.000 b | 0.028 a | 0.000 a | 0.000 a | 0.000 a | 0.005 b | |
| Left Knee | T0 | −6.98 ± 6.74 | −12.45 ± 4.17 | −11.81 ± 10.89 | −12.72 ± 8.29 | −1.44 ± 9.61 | −3.29 ± 6.73 |
| T1 | −9.4 ± 1.05 | −9.27 ± 0.35 | −0.43 ± 2.30 | −11.13 ± 0.81 | 3.92 ± 1.39 | −5.09 ± 2.24 | |
| p-value | 0.018 c | 0.000 a | 0.000 b | 0.000 b | 0.000 a | 0.196 c | |
| Right Knee | T0 | −10.36 ± 4.95 | 3.73 ± 4.66 | 0.16 ± 2.71 | −0.91 ± 2.64 | −3.57 ± 2.57 | −5.49 ± 3.45 |
| T1 | −10.24 ± 0.81 | −0.45 ± 0.59 | −6.58 ± 1.24 | −7.22 ± 1.53 | −7.28 ± 0.64 | −5.77 ± 1.54 | |
| p-value | 0.000 a | 0.000 a | 0.000 b | 0.000 b | 0.000 a | 0.000 c | |
| Left Ankle | T0 | 6.90 ± 6.84 | 3.08 ± 7.54 | −1.86 ± 1.61 | 6.41 ± 6.41 | 4.03 ± 7.37 | −0.27 ± 7.07 |
| T1 | 6.93 ± 1.78 | 2.99 ± 1.38 | 7.40 ± 2.95 | 5.28 ± 1.69 | 6.98 ± 1.29 | 1.02 ± 1.35 | |
| p-value | 0.186 c | 0.028 c | 0.000 a | 0.918 c | 0.001 b | 0.000 b | |
| Right Ankle | T0 | 6.49 ± 1.58 | −3.70 ± 1.61 | 0.73 ± 1.45 | 3.55 ± 1.58 | 1.02 ± 1.46 | 2.22 ± 1.83 |
| T1 | 4.71 ± 1.28 | −0.19 ± 1.80 | 0.39 ± 1.43 | 1.49 ± 2.01 | 0.83 ± 1.42 | 2.38 ± 2.23 | |
| p-value | 0.000 a | 0.054 a | 0.226 c | 0.000 a | 0.063 a | 0.707 c | |
| Joint Angle (Degrees) | Time of Assessment | Left Lower Limb | Right Lower Limb | ||||
|---|---|---|---|---|---|---|---|
| HS | MD | TO | HS | MD | TO | ||
| Pelvis | T0 | 84.10 ± 2.74 | 86.55 ± 2.16 | 92.58 ± 2.47 | 92.06 ± 2.52 | 91.16 ± 2.52 | 84.67 ± 2.37 |
| T1 | 88.67 ± 2.29 | 91.79 ± 1.51 | 93.44 ± 2.43 | 95.43 ± 2.33 | 94.31 ± 2.16 | 89.17 ± 2.43 | |
| p-value | 0.000 a | 0.017 a | 0.121 c | 0.000 a | 0.001 a | 0.000 a | |
| Left Hip | T0 | −7.3 ± 9.13 | −13.23 ± 6.89 | −15.61 ± 11.6 | −12.11 ± 18.20 | −10.99 ± 10.06 | −3.00 ± 9.21 |
| T1 | 4.65 ± 3.86 | 3.21 ± 1.01 | 5.06 ± 2.58 | 5.76 ± 2.98 | 4.38 ± 1.37 | 5.14 ± 2.33 | |
| p-value | 0.000 a | 0.028 a | 0.000 a | 0.000 a | 0.001 a | 0.000 b | |
| Right Hip | T0 | −6.31 ± 3.82 | −6.06 ± 4.59 | −1.60 ± 3.43 | 0.05 ± 3.95 | −3.72 ± 3.89 | −10.28 ± 3.96 |
| T1 | −6.25 ± 2.87 | −10.03 ± 2.17 | −8.66 ± 2.58 | −12.33 ± 5.91 | −6.23 ± 3.23 | −5.32 ± 3.52 | |
| p-value | 0.725 c | 0.249 b | 0.000 a | 0.000 a | 0.683 c | 0.000 a | |
| Left Knee | T0 | −13.98 ± 9.31 | −4.46 ± 5.52 | −10.22 ± 7.02 | 0.37 ± 24.10 | −18.15 ± 5.28 | −16.34 ± 8.27 |
| T1 | −19.26 ± 2.16 | −16.13 ± 2.64 | −31.03 ± 2.76 | −16.47 ± 1.89 | −25.14 ± 3.96 | −18.35 ± 2.36 | |
| p-value | 0.001 a | 0.096 c | 0.000 a | 0.000 a | 0.003 a | 0.036 c | |
| Right Knee | T0 | −3.29 ± 3.36 | −8.49 ± 3.60 | −13.66 ± 3.53 | −18.66 ± 4.47 | −10.95 ± 4.33 | −4.46 ± 4.38 |
| T1 | 6.10 ± 2.03 | −10.03 ± 2.17 | 0.40 ± 1.93 | −0.99 ± 1.93 | 2.06 ± 1.49 | −1.52 ± 1.55 | |
| p-value | 0.000 a | 0.052 a | 0.000 a | 0.000 a | 0.001 a | 0.001 b | |
| Left Ankle | T0 | 4.29 ± 4.25 | −29.49 ± 2.14 | −0.02 ± 1.87 | −29.40 ± 3.66 | −27.30 ± 3.78 | −30.90 ± 2.87 |
| T1 | −24.37 ± 0.83 | −28.99 ± 0.30 | −30.84 ± 1.39 | −28.51 ± 1.11 | −24.47 ± 0.92 | −30.25 ± 1.04 | |
| p-value | 0.399 c | 0.046 a | 0.000 b | 0.000 c | 0.000 c | 0.041 c | |
| Right Ankle | T0 | −6.65 ± 2.35 | −9.04 ± 2.47 | −9.11 ± 3.16 | −1.70 ± 2.88 | −8.20 ± 2.41 | −7.32 ± 2.66 |
| T1 | −18.05 ± 1.05 | −10.21 ± 0.68 | −19.78 ± 1.81 | −13.49 ± 1.57 | −19.39 ± 1.32 | −17.46 ± 2.79 | |
| p-value | 0.000 a | 0.506 b | 0.000 a | 0.000 a | 0.001 a | 0.000 a | |

Appendix C.5. Participant 5
| Joint Angle (Degrees) | Time of Assessment | Left Lower Limb | Right Lower Limb | ||||
|---|---|---|---|---|---|---|---|
| HS | MD | LTO | HS | MD | TO | ||
| Pelvis | T0 | −1.73 ± 1.63 | −1.81 ± 1.10 | 5.74 ± 22.57 | −3.85 ± 2.80 | −2.01 ± 0.69 | −4.50 ± 1.08 |
| T1 | 1.58 ± 0.79 | 1.10 ± 0.88 | 5.30 ± 0.91 | 1.03 ± 1.41 | 0.19 ± 0.94 | −2.14 ± 0.82 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Left Hip | T0 | 21.24 ± 1.69 | −4.48 ± 1.33 | −7.81 ± 24.89 | −19.64 ± 2.11 | 23.59 ± 1.53 | 17.83 ± 1.39 |
| T1 | 27.16 ± 2.50 | 1.66 ± 1.93 | −4.68 ± 3.14 | −13.89 ± 1.74 | 29.02 ± 1.57 | 22.93 ± 4.11 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Right Hip | T0 | −20.86 ± 1.49 | 17.43 ± 1.40 | 23.55 ± 19.51 | 22.63 ± 1.63 | −4.68 ± 1.70 | −17.47 ± 1.40 |
| T1 | −15.33 ± 2.55 | 24.06 ± 1.45 | 26.08 ± 3.16 | 30.13 ± 2.93 | 2.31 ± 2.74 | −10.57 ± 4.49 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Left Knee | T0 | 13.69 ± 2.13 | 12.97 ± 2.01 | 39.18 ± 2.21 | 12.96 ± 1.74 | 66.3 ± 1.79 | 24.01 ± 2.15 |
| T1 | 14.71 ± 4.16 | 16.05 ± 4.04 | 47.93 ± 5.89 | 15.14 ± 3.6 | 29.02 ± 1.57 | 30.21 ± 3.78 | |
| p-value | 0.257 c | 0.001 b | 0.000 a | 0.006 b | 0.000 a | 0.000 a | |
| Right Knee | T0 | 4.87 ± 1.71 | 59.10 ± 2.13 | 26.25 ± 2.79 | 16.51 ± 1.85 | 11.39 ± 2.58 | 33.90 ± 2.19 |
| T1 | 11.93 ± 1.89 | 60.38 ± 2.31 | 29.79 ± 2.83 | 17.95 ± 3.05 | 13.87 ± 2.49 | 39.85 ± 5.87 | |
| p-value | 0.013 b | 0.015 a | 0.000 a | 0.004 a | 0.002 a | 0.000 a | |
| Left Ankle | T0 | 1.11 ± 1.10 | 9.15 ± 1.20 | 7.23 ± 2.81 | 25.02 ± 1.14 | −6.15 ± 1.07 | −1.54 ± 2.09 |
| T1 | −3.11 ± 0.81 | 12.06 ± 1.78 | 2.45 ± 4.81 | 27.33 ± 1.98 | −2.65 ± 1.33 | 4.15 ± 2.28 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Right Ankle | T0 | 20.25 ± 1.30 | 2.21 ± 0.81 | 2.98 ± 1.55 | −0.01 ± 1.02 | 10.82 ± 1.22 | 6.89 ± 2.27 |
| T1 | 21.24 ± 1.34 | −1.37 ± 1.33 | 4.44 ± 1.94 | −2.68 ± 0.85 | 11.05 ± 1.28 | 3.53 ± 3.93 | |
| p-value | 0.005 a | 0.000 a | 0.002 a | 0.000 a | 0.371 c | 0.000 a | |
| Joint Angle (Degrees) | Time of Assessment | Left Lower Limb | Right Lower Limb | ||||
|---|---|---|---|---|---|---|---|
| HS | MD | TO | HS | MD | TO | ||
| Pelvis | T0 | −6.20 ± 1.40 | −8.65 ± 1.68 | −6.35 ± 1.25 | −5.75 ± 1.27 | −7.31 ± 1.09 | −8.14 ± 1.43 |
| T1 | −1.15 ± 1.07 | −3.34 ± 1.92 | −1.67 ± 3.12 | −0.68 ± 2.47 | −1.87 ± 2.22 | −4.33 ± 1.33 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Left Hip | T0 | 1.58 ± 1.93 | 5.28 ± 1.13 | −3.48 ± 1.31 | 3.87 ± 2.51 | 2.09 ± 0.81 | 5.56 ± 1.84 |
| T1 | −3.01 ± 1.44 | 2.41 ± 1.62 | −6.22 ± 1.67 | 0.50 ± 2.59 | −1.10 ± 1.03 | 1.71 ± 1.84 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.434 b | |
| Right Hip | T0 | 4.11 ± 2.17 | 0.14 ± 1.16 | 3.56 ± 4.56 | −3.23 ± 3.13 | 5.46 ± 0.88 | −0.86 ± 1.50 |
| T1 | 5.42 ± 1.64 | 1.87 ± 1.78 | 6.39 ± 2.13 | −0.51 ± 2.72 | 5.46 ± 2.14 | −1.83 ± 1.53 | |
| p-value | 0.001 b | 0.001 b | 0.000 b | 0.001 b | 0.829 c | 0.000 b | |
| Left Knee | T0 | −0.89 ± 0.57 | −0.97 ± 0.46 | −7.42 ± 1.45 | −1.56 ± 0.52 | −4.24 ± 1.51 | −1.26 ± 0.96 |
| T1 | −0.59 ± 0.67 | −0.27 ± 0.61 | −2.45 ± 4.06 | −0.96 ± 0.66 | −1.10 ± 1.03 | 0.91 ± 1.26 | |
| p-value | 0.097 b | 0.000 b | 0.000 b | 0.000 a | 0.000 a | 0.000 a | |
| Right Knee | T0 | −6.31 ± 3.82 | 7.91 ± 1.79 | 3.23 ± 2.14 | 0.86 ± 0.58 | −0.32 ± 0.37 | 0.67 ± 0.66 |
| T1 | −2.17 ± 0.64 | 2.31 ± 1.01 | −0.70 ± 1.16 | −1.48 ± 0.86 | −1.48 ± 0.69 | −1.18 ± 1.40 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Left Ankle | T0 | 0.97 ± 0.96 | −4.53 ± 1.00 | −4.10 ± 1.35 | −5.00 ± 0.91 | −5.30 ± 1.06 | −3.57 ± 1.24 |
| T1 | 2.74 ± 1.00 | 0.06 ± 1.23 | 0.46 ± 1.11 | 0.50 ± 1.49 | −2.62 ± 0.80 | −1.26 ± 1.16 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Right Ankle | T0 | 3.76 ± 1.11 | −4.05 ± 0.53 | −2.72 ± 1.27 | 1.71 ± 0.78 | −1.47 ± 1.18 | 3.40 ± 1.58 |
| T1 | 0.90 ± 1.32 | −3.73 ± 2.05 | −2.71 ± 1.84 | 2.84 ± 1.70 | −1.76 ± 1.20 | 1.49 ± 2.14 | |
| p-value | 0.000 a | 0.014 b | 0.857 c | 0.001 a | 0.475 c | 0.005 a | |
| Joint Angle (Degrees) | Time of Assessment | Left Lower Limb | Right Lower Limb | ||||
|---|---|---|---|---|---|---|---|
| HS | MD | TO | HS | MD | TO | ||
| Pelvis | T0 | 89.55 ± 1.64 | 92.86 ± 1.72 | 101.39 ± 8.13 | 99.45 ± 1.62 | 94.12 ± 1.34 | 89.76 ± 1.72 |
| T1 | 87.40 ± 1.72 | 90.58 ± 1.68 | 97.02 ± 1.50 | 96.73 ± 1.84 | 92.25 ± 1.52 | 87.21 ± 1.90 | |
| p-value | 0.000 b | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Left Hip | T0 | −18.62 ± 3.40 | −11.72 ± 1.90 | −8.22 ± 13.92 | −9.09 ± 1.78 | −4.08 ± 2.11 | −14.53 ± 2.78 |
| T1 | −12.83 ± 2.52 | −5.93 ± 3.84 | −1.01 ± 4.84 | −4.63 ± 3.56 | 6.23 ± 3.15 | −9.73 ± 2.15 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Right Hip | T0 | −0.65 ± 1.89 | 4.60 ± 2.77 | −5.24 ± 15.06 | −5.13 ± 2.38 | −0.43 ± 1.97 | −1.67 ± 1.75 |
| T1 | −3.22 ± 2.36 | −0.55 ± 2.91 | −10.39 ± 2.25 | −13.44 ± 2.00 | −4.66 ± 2.86 | −4.18 ± 2.01 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Left Knee | T0 | 8.93 ± 2.54 | 13.96 ± 1.13 | 17.25 ± 1.62 | 18.06 ± 1.45 | 13.81 ± 1.43 | 10.67 ± 2.37 |
| T1 | −8.55 ± 2.36 | −4.18 ± 2.24 | −0.76 ± 2.50 | −0.60 ± 1.31 | 6.23 ± 3.15 | −5.94 ± 1.92 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Right Knee | T0 | 13.57 ± 2.83 | −18.78 ± 1.95 | −25.08 ± 3.46 | −27.53 ± 1.90 | −21.18 ± 1.41 | −20.37 ± 1.50 |
| T1 | −2.96 ± 1.42 | −6.50 ± 2.28 | −7.25 ± 2.93 | −11.38 ± 3.11 | −6.39 ± 2.17 | −7.66 ± 2.59 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Left Ankle | T0 | 1.32 ± 1.30 | −8.29 ± 1.80 | −7.80 ± 2.33 | −6.99 ± 1.65 | −11.44 ± 1.12 | −8.59 ± 2.03 |
| T1 | 10.12 ± 2.47 | 3.32 ± 2.68 | 3.44 ± 2.14 | 2.33 ± 1.55 | 2.02 ± 1.24 | 4.19 ± 2.29 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |
| Right Ankle | T0 | −1.42 ± 1.27 | −3.86 ± 1.59 | −1.92 ± 1.64 | 4.41 ± 0.87 | −1.89 ± 1.46 | 1.09 ± 2.37 |
| T1 | −15.64 ± 1.20 | −15.86 ± 1.94 | −16.46 ± 2.54 | −6.61 ± 1.57 | −15.76 ± 1.43 | −12.62 ± 2.30 | |
| p-value | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | 0.000 a | |

References
- Planté-Bordeneuve, V.; Said, G. Familial amyloid polyneuropathy. Lancet Neurol. 2011, 10, 1086–1097. [Google Scholar] [CrossRef]
- Schmidt, H.H.; Waddington-Cruz, M.; Botteman, M.F.; Carter, J.A.; Chopra, A.S.; Hopps, M.; Stewart, M.; Fallet, S.; Amass, L. Estimating the global prevalence of transthyretin familial amyloid polyneuropathy. Muscle Nerve 2018, 57, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Ines, M.; Coelho, T.; Conceicao, I.; Duarte-Ramos, F.; de Carvalho, M.; Costa, J. Epidemiology of Transthyretin Familial Amyloid Polyneuropathy in Portugal: A Nationwide Study. Neuroepidemiology 2018, 51, 177–182. [Google Scholar] [CrossRef]
- Kato-Motozaki, Y.; Ono, K.; Shima, K.; Morinaga, A.; Machiya, T.; Nozaki, I.; Shibata-Hamaguchi, A.; Furukawa, Y.; Yanase, D.; Ishida, C.; et al. Epidemiology of familial amyloid polyneuropathy in Japan: Identification of a novel endemic focus. J. Neurol. Sci. 2008, 270, 133–140. [Google Scholar] [CrossRef]
- Dardiotis, E.; Koutsou, P.; Papanicolaou, E.Z.; Vonta, I.; Kladi, A.; Vassilopoulos, D.; Hadjigeorgiou, G.; Christodoulou, K.; Kyriakides, T. Epidemiological, clinical and genetic study of familial amyloidotic polyneuropathy in Cyprus. Amyloid 2009, 16, 32–37. [Google Scholar] [CrossRef]
- Parman, Y.; Adams, D.; Obici, L.; Galan, L.; Guergueltcheva, V.; Suhr, O.B.; Coelho, T. Sixty years of transthyretin familial amyloid polyneuropathy (TTR-FAP) in Europe: Where are we now? A European network approach to defining the epidemiology and management patterns for TTR-FAP. Curr. Opin. Neurol. 2016, 29 (Suppl. S1), S3–S13. [Google Scholar] [CrossRef] [Green Version]
- Coutinho, P.; Martins da Silva, A.; Lopes Lima, J.; Resende-Barbosa, A. Forty Years of Experience with Type I Amyloid Neuropathy. In Amyloid and Amyloidosis; Review of 483 cases; Glenner, G.G., Pinho e Costa, P., Falcão de Freitas, A., Eds.; Excerpta Medica: Amsterdam, The Netherlands, 1980; pp. 88–98. [Google Scholar]
- Zhao, Y.; Xin, Y.; Song, Z.; He, Z.; Hu, W. Tafamidis, a Noninvasive Therapy for Delaying Transthyretin Familial Amyloid Polyneuropathy: Systematic Review and Meta-Analysis. J. Clin. Neurol. 2019, 15, 108–115. [Google Scholar] [CrossRef]
- Adams, D.; Gonzalez-Duarte, A.; O’Riordan, W.D.; Yang, C.-C.; Ueda, M.; Kristen, A.V.; Tournev, I.; Schmidt, H.H.; Coelho, T.; Berk, J.L.; et al. Patisiran, an RNAi Therapeutic, for Hereditary Transthyretin Amyloidosis. N. Engl. J. Med. 2018, 379, 11–21. [Google Scholar] [CrossRef]
- Benson, M.D.; Waddington-Cruz, M.; Berk, J.L.; Polydefkis, M.; Dyck, P.J.; Wang, A.K.; Planté-Bordeneuve, V.; Barroso, F.A.; Merlini, G.; Obici, L.; et al. Inotersen Treatment for Patients with Hereditary Transthyretin Amyloidosis. N. Engl. J. Med. 2018, 379, 22–31. [Google Scholar] [CrossRef]
- Plante-Bordeneuve, V. Transthyretin familial amyloid polyneuropathy: An update. J. Neurol. 2018, 265, 976–983. [Google Scholar] [CrossRef]
- Escolano-Lozano, F.; Barreiros, A.P.; Birklein, F.; Geber, C. Transthyretin familial amyloid polyneuropathy (TTR-FAP): Parameters for early diagnosis. Brain Behav. 2018, 8, e00889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinik, E.J.; Hayes, R.P.; Oglesby, A.; Bastyr, E.; Barlow, P.; Ford-Molvik, S.L.; Vinik, A.I. The Development and Validation of the Norfolk QOL-DN, a New Measure of Patients’ Perception of the Effects of Diabetes and Diabetic Neuropathy. Diabetes Technol. Ther. 2005, 7, 497–508. [Google Scholar] [CrossRef] [PubMed]
- Vilas-Boas, M.d.C.; Cunha, J.P.S. Movement Quantification in Neurological Diseases: Methods and Applications. IEEE Rev. Biomed. Eng. 2016, 9, 15–31. [Google Scholar] [CrossRef]
- Adams, D.; Koike, H.; Slama, M.; Coelho, T. Hereditary transthyretin amyloidosis: A model of medical progress for a fatal disease. Nat. Rev. Neurol. 2019, 15, 387–404. [Google Scholar] [CrossRef] [PubMed]
- Adams, D. Recent advances in the treatment of familial amyloid polyneuropathy. Ther. Adv. Neurol. Disord. 2013, 6, 129–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whittle, M.W. Gait Analysis An Introduction, 4th ed.; Elsevier Ltd.: Amsterdam, The Netherlands, 2007. [Google Scholar]
- Roetenberg, D. Inertial and Magnetic Sensing of Human Motion. Ph.D. Thesis, University of Twente, Enschede, The Netherlands, 2006. [Google Scholar]
- Vilas-Boas, M.C.; Rocha, A.P.; Choupina, H.M.P.; Fernandes, J.M.; Coelho, T.; Cunha, J.P.S. The First Transthyretin Familial Amyloid Polyneuropathy Gait Quantification Study—Preliminary Results. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017. [Google Scholar]
- Vilas-Boas, M.D.C.; Rocha, A.P.; Cardoso, M.N.; Fernandes, J.M.; Coelho, T.; Cunha, J.P.S. Clinical 3-D Gait Assessment of Patients With Polyneuropathy Associated With Hereditary Transthyretin Amyloidosis. Front. Neurol. 2020, 11, 605282. [Google Scholar] [CrossRef]
- Vilas-Boas, M.d.C.; Rocha, A.P.; Cardoso, M.N.; Fernandes, J.M.; Coelho, T.; Cunha, J.P.S. Supporting the Assessment of Hereditary Transthyretin Amyloidosis Patients Based On 3-D Gait Analysis and Machine Learning. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 1350–1362. [Google Scholar] [CrossRef] [PubMed]
- Compston, A. Aids to the Investigation of Peripheral Nerve Injuries. Medical Research Council: Nerve Injuries Research Committee. His Majesty’s Stationery Office: 1942; pp. 48 (iii) and 74 figures and 7 diagrams; with Aids to the Examination of the Peripheral Nervous System. By Michael O’Brien for the Guarantors of Brain. Saunders Elsevier: 2010; pp. [8] 64 and 94 Figures. Brain 2010, 133, 2838–2844. [Google Scholar] [CrossRef]
- Adams, D.; Suhr, O.B.; Hund, E.; Obici, L.; Tournev, I.; Campistol, J.M.; Slama, M.S.; Hazenberg, B.P.; Coelho, T. First European consensus for diagnosis, management, and treatment of transthyretin familial amyloid polyneuropathy. Curr. Opin. Neurol. 2016, 29 (Suppl. S1), S14–S26. [Google Scholar] [CrossRef]
- Cappozzo, A.; Catan, F.; Croce, U.D.; Leardini, A. Position and orientation in space of bones during movement: Experimental artefacts. Clin. Biomech. 1995, 10, 171–178. [Google Scholar] [CrossRef]
- Benedetti, M.G.; Catani, F.; Leardini, A.; Pignotti, E.; Giannini, S. Data management in gait analysis for clinical applications. Clin. Biomech. 1998, 13, 204–215. [Google Scholar] [CrossRef]
- Kim, K.; Song, W.K.; Lee, J.; Lee, H.Y.; Park, D.S.; Ko, B.W.; Kim, J. Kinematic analysis of upper extremity movement during drinking in hemiplegic subjects. Clin. Biomech. 2014, 29, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.W. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Richards, J. Biomechanics in Clinic and Research; Churcill Livingstone Elsevier: London, UK, 2009. [Google Scholar]
- Martinelli, A.R.; Mantovani, A.M.; Nozabieli, A.J.L.; Ferreira, D.M.A.; Barela, J.A.; Camargo, M.R.d.; Fregonesi, C.E.P.T. Muscle strength and ankle mobility for the gait parameters in diabetic neuropathies. Foot 2013, 23, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Perry, J. Gait Analysis—Normal and Pathological Function; SLACK Incorporated: Thorofare, NJ, USA, 1992. [Google Scholar]
- Abu-Zidan, F.M.; Abbas, A.K.; Hefny, A.I. Clinical “case series”: A concept analysis. Afr. Health Sci. 2013, 12, 557–562. [Google Scholar] [CrossRef] [Green Version]
- Katoulis, E.C.; Ebdon-Parry, M.; Lanshammar, H.; Vlleikyte, L.; Kulkarni, J.; Boulton, A.J.M. Gait Abnormalities in Diabetic Neuropathy. Diabetes Care 1997, 20, 1904–1907. [Google Scholar] [CrossRef]
- Brown, S.J.; Handsaker, J.C.; Bowling, F.L.; Maganaris, C.N.; Boulton, A.J.; Reeves, N.D. Do patients with diabetic neuropathy use a higher proportion of their maximum strength when walking? J. Biomech. 2014, 47, 3639–3644. [Google Scholar] [CrossRef]
- Karmakar, M.K.; Samy, W.; Li, J.W.; Lee, A.; Chan, W.C.; Chen, P.P.; Ho, A.M.-H. Thoracic paravertebral block and its effects on chronic pain and health-related quality of life after modified radical mastectomy. Reg. Anesth. Pain Med. 2014, 39, 289–298. [Google Scholar] [CrossRef]
- Adams, D.; Samuel, D.; Goulon-Goeau, C.; Nakazato, M.; Costa, P.M.; Feray, C.; Planté, V.; Ducot, B.; Ichai, P.; Lacroix, C.; et al. The course and prognostic factors of familial amyloid polyneuropathy after liver transplantation. Brain 2000, 123, 1495–1504. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, S.; Wilczek, H.E.; Nowak, G.; Larsson, M.; Oksanen, A.; Iwata, T.; Gjertsen, H.; Soderdahl, G.; Wikstrom, L.; Ando, Y.; et al. Liver transplantation for familial amyloidotic polyneuropathy (FAP): A single-center experience over 16 years. Am. J. Transpl. 2007, 7, 2597–2604. [Google Scholar] [CrossRef]
- Coelho, T. Familial amyloid polyneuropathy: New develpments in genetics and treatment. Curr. Opin. Neurol. 1996, 9, 355–359. [Google Scholar] [CrossRef]
- Fabio, A.B.; Daniel, P.J.; Ben, E.; Huihua, L.; Michelle, S.; Amass, L.; Sultan, M.B. Long-term safety and efficacy of tafamidis for the treatment of hereditary transthyretin amyloid polyneuropathy: Results up to 6 years. Amyloid 2017, 24, 194–204. [Google Scholar] [CrossRef]
- Monteiro, C.; Mesgazardeh, J.S.; Anselmo, J.; Fernandes, J.; Novais, M.; Rodrigues, C.; Brighty, G.J.; Powers, D.L.; Powers, E.T.; Coelho, T.; et al. Predictive model of response to tafamidis in hereditary ATTR polyneuropathy. JCI Insight 2019, 4, e126526. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| Patient | Gender 1 | Height (m) | Weight (kg) | Age (Years) | BMI (kg/m2) | BMI Variation (kg/m2) | Years of Disease Progression | Years since Diagnosis |
|---|---|---|---|---|---|---|---|---|
| P1 | M | 1.72 | 72.0 | 34 | 24.34 | 0.0 | 9 | 8 |
| P2 | M | 1.73 | 58.5 | 33 | 19.55 | 1.5 | 8 | 8 |
| P3 | F | 1.68 | 63.8 | 48 | 22.60 | 0.6 | 5 | 2 |
| P4 | F | 1.48 | 61.5 | 54 | 28.08 | −1.4 | 18 | 17 |
| P5 | M | 1.71 | 53.0 | 52 | 18.13 | 0.9 | 13 | 13 |
| Patient | MRC 1 Scores at T0 | MRC 1 Scores at T1 | PND Score 2,* | TTR-FAP Score 2,* | Treatment at T0 |
|---|---|---|---|---|---|
| P1 | Dorsiflexion deficit (4), minor vibration anesthesia on the hallux | Dorsiflexion deficit (4−), minor vibration anesthesia on the hallux | II | I | Transplant 6 years ago |
| P2 | Dorsiflexion (0), plantar-flexion (1), knee flexion and extension (4), sensory ataxia and high steppage | Dorsiflexion (0), plantar-flexion (0), knee flexion and extension (4), sensory ataxia and high steppage | II | I | Tafamidis for 3.5 years |
| P3 | Only vibration anesthesia on the hallux, minor difficulties on heels or tip toes gait | Only vibration anesthesia on the hallux, minor difficulties on heels or tip toes gait | II | I | Tafamidis for 1 year |
| P4 | Dorsiflexion (4), plantar-flexion (4), sensory ataxia, low steppage | Dorsiflexion (3), plantar-flexion (4), sensory ataxia, steppage | II | I | Transplant 12 years ago |
| P5 | Dorsiflexion and plantar-flexion (2), sensory ataxia and high steppage | Dorsiflexion (0), plantar-flexion (1), sensory ataxia and high steppage | II | I | Transplant 18 years ago |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vilas-Boas, M.d.C.; Fonseca, P.F.P.; Sousa, I.M.; Cardoso, M.N.; Cunha, J.P.S.; Coelho, T. Gait Characterization and Analysis of Hereditary Amyloidosis Associated with Transthyretin Patients: A Case Series. J. Clin. Med. 2022, 11, 3967. https://doi.org/10.3390/jcm11143967
Vilas-Boas MdC, Fonseca PFP, Sousa IM, Cardoso MN, Cunha JPS, Coelho T. Gait Characterization and Analysis of Hereditary Amyloidosis Associated with Transthyretin Patients: A Case Series. Journal of Clinical Medicine. 2022; 11(14):3967. https://doi.org/10.3390/jcm11143967
Chicago/Turabian StyleVilas-Boas, Maria do Carmo, Pedro Filipe Pereira Fonseca, Inês Martins Sousa, Márcio Neves Cardoso, João Paulo Silva Cunha, and Teresa Coelho. 2022. "Gait Characterization and Analysis of Hereditary Amyloidosis Associated with Transthyretin Patients: A Case Series" Journal of Clinical Medicine 11, no. 14: 3967. https://doi.org/10.3390/jcm11143967
APA StyleVilas-Boas, M. d. C., Fonseca, P. F. P., Sousa, I. M., Cardoso, M. N., Cunha, J. P. S., & Coelho, T. (2022). Gait Characterization and Analysis of Hereditary Amyloidosis Associated with Transthyretin Patients: A Case Series. Journal of Clinical Medicine, 11(14), 3967. https://doi.org/10.3390/jcm11143967