
Tumor Necrosis Factor-Related Apoptosis-Inducing Ligand (TRAIL): A Novel Biomarker for Prognostic Assessment and Risk Stratification of Acute Pulmonary Embolism

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
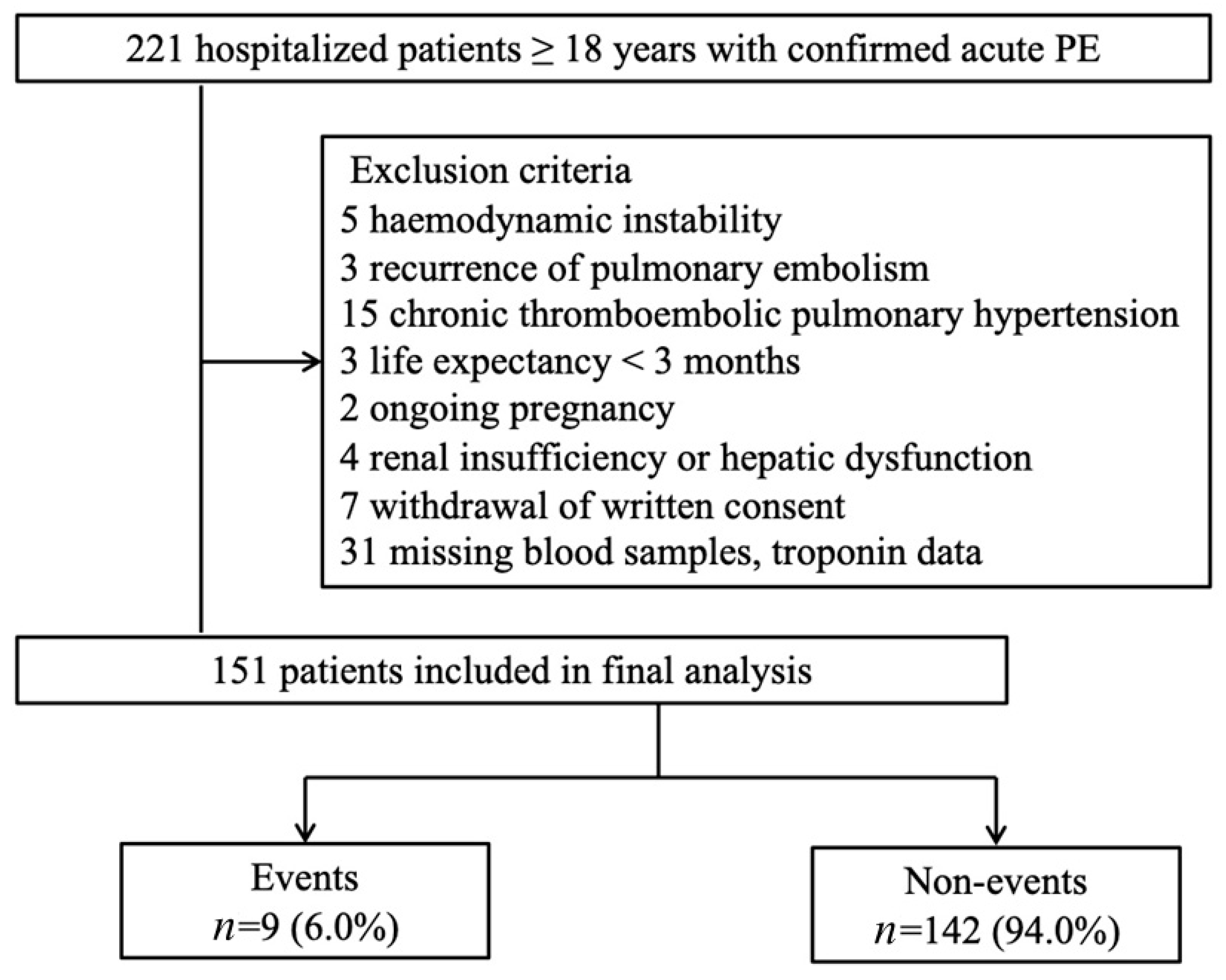
2.2. Selection of Participants
2.3. Methods of Measurement
2.4. Outcome Measures
2.5. Biomarker-Based Risk Algorithm
2.6. Statistical Analyses
3. Results
3.1. Characteristics of Study Subjects
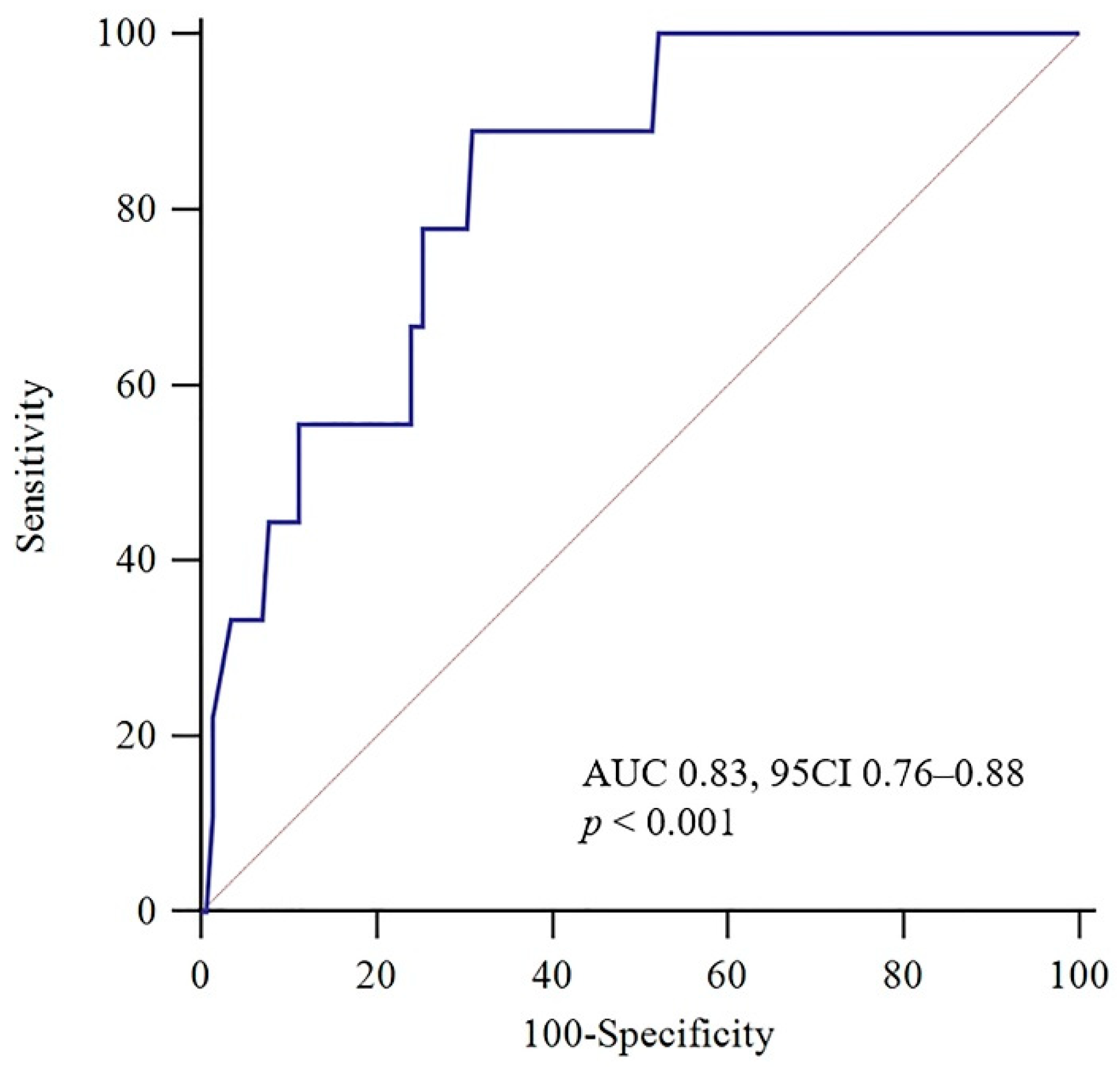
3.2. Association between TRAIL Levels and Short-Term Prognosis
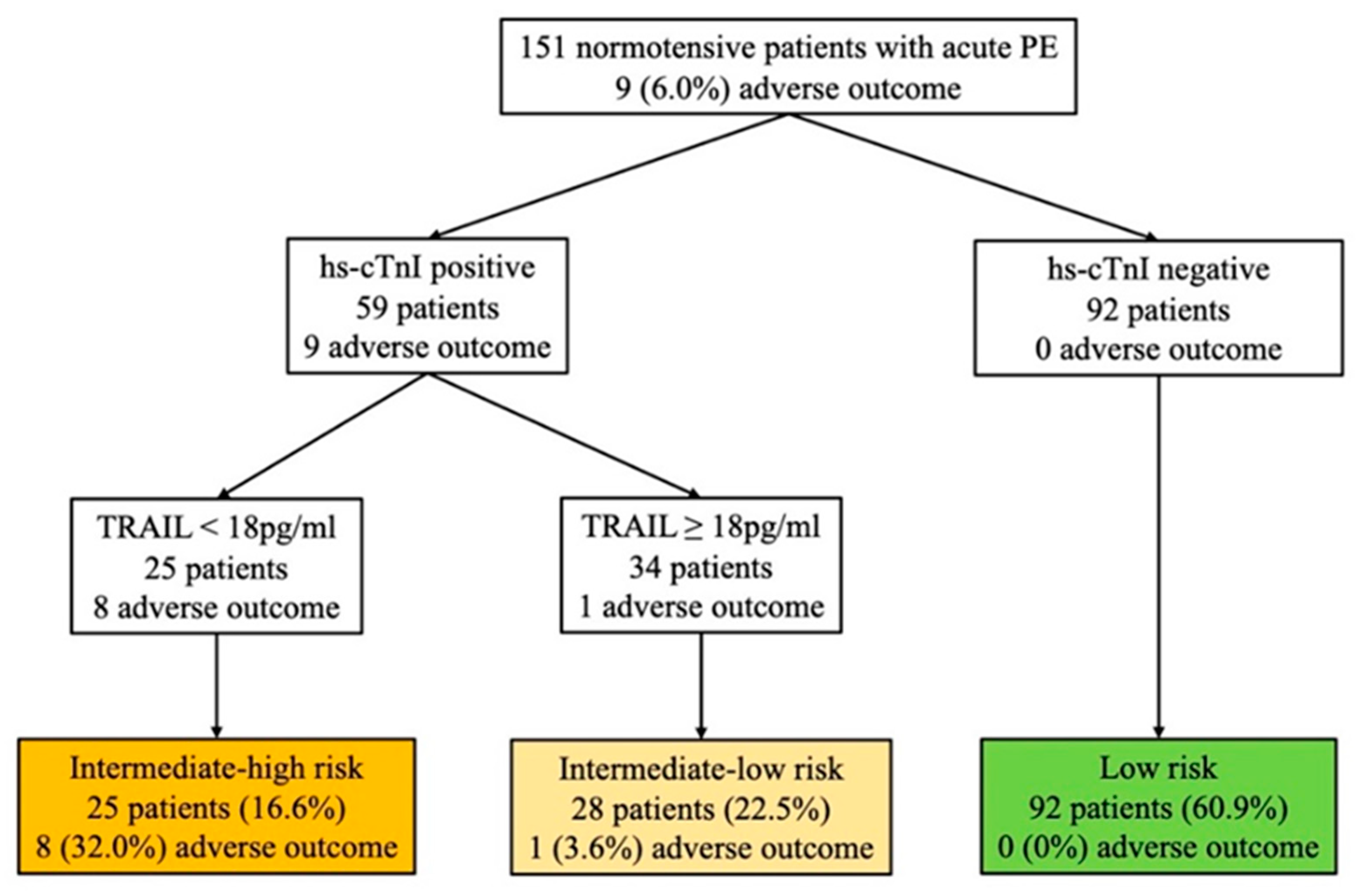
3.3. TRAIL’s Role in Risk Stratification
4. Discussion
4.1. The Potential Role of TRAIL in PE
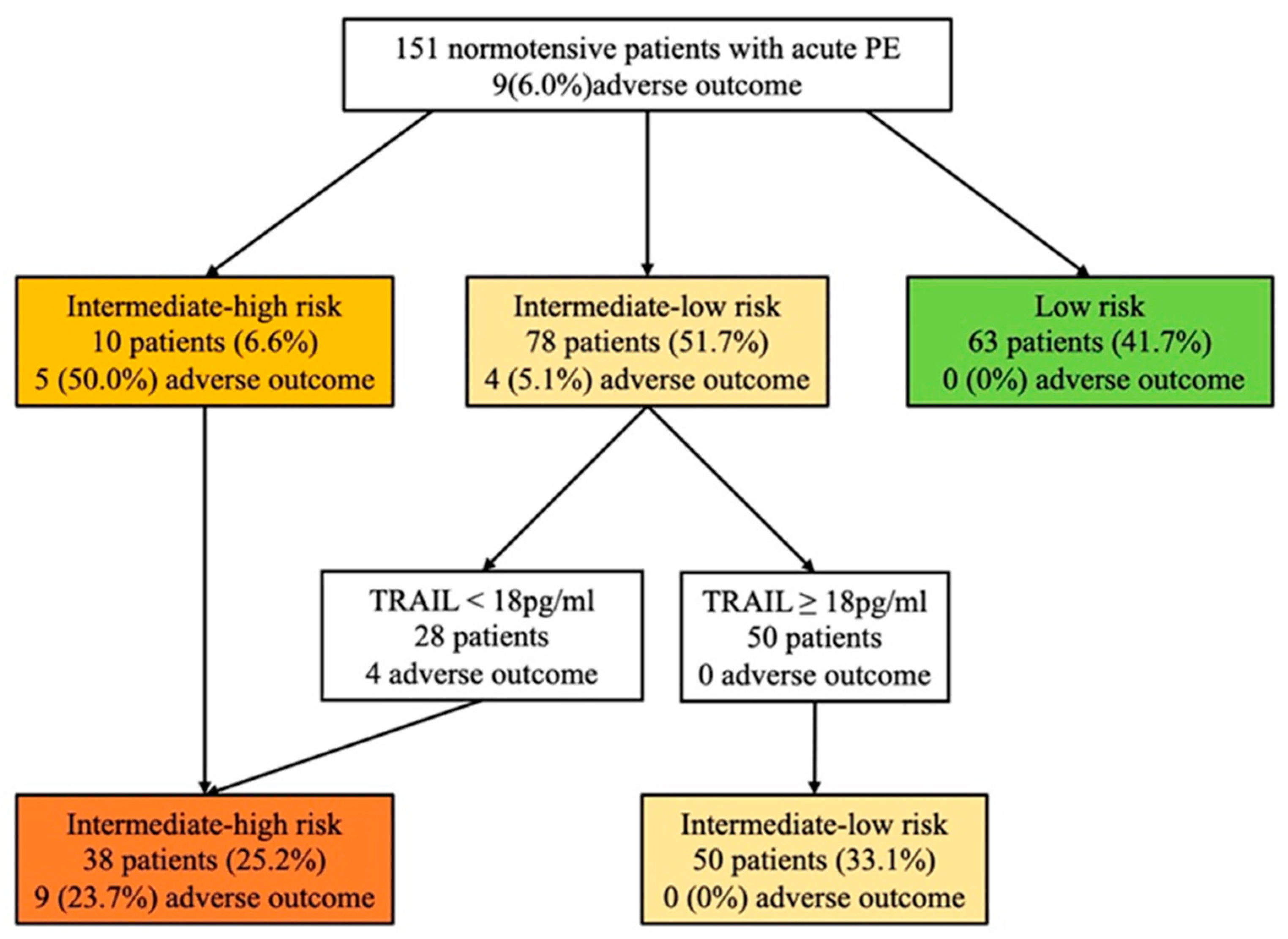
4.2. The Combination of TRAIL and the 2019 ESC Algorithm for Risk Assessment in Normotensive Patients with Acute PE
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raskob, G.E.; Angchaisuksiri, P.; Blanco, A.N.; Buller, H.; Gallus, A.; Hunt, B.J.; Hylek, E.M.; Kakkar, T.L.; Konstantinides, S.V.; McCumber, M.; et al. Thrombosis: A major contributor to global disease burden. Semin. Thromb. Hemost. 2014, 40, 724–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naess, I.A.; Christiansen, S.C.; Romundstad, P.; Cannegieter, S.C.; Rosendaal, F.R.; Hammerstrom, J. Incidence and mortality of venous thrombosis: A population-based study. J. Thromb. Haemost. 2007, 5, 692–699. [Google Scholar] [CrossRef]
- Alotaibi, G.S.; Wu, C.; Senthilselvan, A.; McMurtry, M.S. Secular Trends in Incidence and Mortality of Acute Venous Thromboembolism: The AB-VTE Population-Based Study. Am. J. Med. 2016, 129, 879.e19–879.e25. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Lei, J.; Shao, X.; Dong, F.; Wang, J.; Wang, D.; Wu, S.; Xie, W.; Wan, J.; Chen, H.; et al. Trends in Hospitalization and In-Hospital Mortality From VTE, 2007 to 2016, in China. Chest 2019, 155, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jimenez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piazza, G. Advanced Management of Intermediate- and High-Risk Pulmonary Embolism: JACC Focus Seminar. J. Am. Coll. Cardiol. 2020, 76, 2117–2127. [Google Scholar] [CrossRef]
- Wiley, S.R.; Schooley, K.; Smolak, P.J.; Din, W.S.; Huang, C.P.; Nicholl, J.K.; Sutherland, G.R.; Smith, T.D.; Rauch, C.; Smith, C.A.; et al. Identification and characterization of a new member of the TNF family that induces apoptosis. Immunity 1995, 3, 673–682. [Google Scholar] [CrossRef] [Green Version]
- Gochuico, B.R.; Zhang, J.; Ma, B.Y.; Marshak-Rothstein, A.; Fine, A. TRAIL expression in vascular smooth muscle. Am. J. Physiol. Lung Cell Mol. Physiol. 2000, 278, L1045–L1050. [Google Scholar] [CrossRef]
- Tecchio, C.; Huber, V.; Scapini, P.; Calzetti, F.; Margotto, D.; Todeschini, G.; Pilla, L.; Martinelli, G.; Pizzolo, G.; Rivoltini, L.; et al. IFNα-stimulated neutrophils and monocytes release a soluble form of TNF-related apoptosis-inducing ligand (TRAIL/Apo-2 ligand) displaying apoptotic activity on leukemic cells. Blood 2004, 103, 3837–3844. [Google Scholar] [CrossRef] [Green Version]
- Simoncini, S.; Njock, M.S.; Robert, S.; Camoin-Jau, L.; Sampol, J.; Harle, J.R.; Nguyen, C.; Dignat-George, F.; Anfosso, F. TRAIL/Apo2L mediates the release of procoagulant endothelial microparticles induced by thrombin in vitro: A potential mechanism linking inflammation and coagulation. Circ. Res. 2009, 104, 943–951. [Google Scholar] [CrossRef]
- Secchiero, P.; Corallini, F.; Ceconi, C.; Parrinello, G.; Volpato, S.; Ferrari, R.; Zauli, G. Potential prognostic significance of decreased serum levels of TRAIL after acute myocardial infarction. PLoS ONE 2009, 4, e4442. [Google Scholar] [CrossRef] [PubMed]
- Niessner, A.; Hohensinner, P.J.; Rychli, K.; Neuhold, S.; Zorn, G.; Richter, B.; Hulsmann, M.; Berger, R.; Mortl, D.; Huber, K.; et al. Prognostic value of apoptosis markers in advanced heart failure patients. Eur. Heart J. 2009, 30, 789–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, B.; Koller, L.; Hohensinner, P.J.; Zorn, G.; Brekalo, M.; Berger, R.; Mortl, D.; Maurer, G.; Pacher, R.; Huber, K.; et al. A multi-biomarker risk score improves prediction of long-term mortality in patients with advanced heart failure. Int. J. Cardiol. 2013, 168, 1251–1257. [Google Scholar] [CrossRef]
- Lankeit, M.; Jimenez, D.; Kostrubiec, M.; Dellas, C.; Hasenfuss, G.; Pruszczyk, P.; Konstantinides, S. Predictive value of the high-sensitivity troponin T assay and the simplified Pulmonary Embolism Severity Index in hemodynamically stable patients with acute pulmonary embolism: A prospective validation study. Circulation 2011, 124, 2716–2724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanni, S.; Jimenez, D.; Nazerian, P.; Morello, F.; Parisi, M.; Daghini, E.; Pratesi, M.; Lopez, R.; Bedate, P.; Lobo, J.L.; et al. Short-term clinical outcome of normotensive patients with acute PE and high plasma lactate. Thorax 2015, 70, 333–338. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.; Liu, Z.; Lu, J.; Yang, X.; Yan, X.X.; Mi, Y.; Hua, L.; Li, Y.; Jing, Z.C.; Du, J. Lipocalin-2 Predicts Long-Term Outcome of Normotensive Patients with Acute Pulmonary Embolism. Cardiovasc. Toxicol. 2020, 20, 101–110. [Google Scholar] [CrossRef]
- Schulman, S.; Kearon, C.; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef]
- Hellenkamp, K.; Schwung, J.; Rossmann, H.; Kaeberich, A.; Wachter, R.; Hasenfuß, G.; Konstantinides, S.; Lankeit, M. Risk stratification of normotensive pulmonary embolism: Prognostic impact of copeptin. Eur. Respir. J. 2015, 46, 1701–1710. [Google Scholar] [CrossRef] [Green Version]
- Hellenkamp, K.; Pruszczyk, P.; Jimenez, D.; Wyzgal, A.; Barrios, D.; Ciurzynski, M.; Morillo, R.; Hobohm, L.; Keller, K.; Kurnicka, K.; et al. Prognostic impact of copeptin in pulmonary embolism: A multicentre validation study. Eur. Respir. J. 2018, 51, 1702037. [Google Scholar] [CrossRef] [Green Version]
- Nash, M.; McGrath, J.P.; Cartland, S.P.; Patel, S.; Kavurma, M.M. Tumour necrosis factor superfamily members in ischaemic vascular diseases. Cardiovasc. Res. 2019, 115, 713–720. [Google Scholar] [CrossRef] [Green Version]
- Harper, E.; Forde, H.; Davenport, C.; Rochfort, K.D.; Smith, D.; Cummins, P.M. Vascular calcification in type-2 diabetes and cardiovascular disease: Integrative roles for OPG, RANKL and TRAIL. Vascul. Pharmacol. 2016, 82, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Forde, H.; Harper, E.; Davenport, C.; Rochfort, K.D.; Wallace, R.; Murphy, R.P.; Smith, D.; Cummins, P.M. The beneficial pleiotropic effects of tumour necrosis factor-related apoptosis-inducing ligand (TRAIL) within the vasculature: A review of the evidence. Atherosclerosis 2016, 247, 87–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Auria, F.; Centurione, L.; Centurione, M.A.; Angelini, A.; Di Pietro, R. Tumor Necrosis Factor Related Apoptosis Inducing Ligand (Trail) in endothelial response to biomechanical and biochemical stresses in arteries. J. Cell. Biochem. 2015, 116, 2427–2434. [Google Scholar] [CrossRef] [PubMed]
- Rochette, L.; Meloux, A.; Rigal, E.; Zeller, M.; Cottin, Y.; Vergely, C. The role of osteoprotegerin in the crosstalk between vessels and bone: Its potential utility as a marker of cardiometabolic diseases. Pharmacol. Ther. 2018, 182, 115–132. [Google Scholar] [CrossRef] [PubMed]
- Volpato, S.; Ferrucci, L.; Secchiero, P.; Corallini, F.; Zuliani, G.; Fellin, R.; Guralnik, J.M.; Bandinelli, S.; Zauli, G. Association of tumor necrosis factor-related apoptosis-inducing ligand with total and cardiovascular mortality in older adults. Atherosclerosis 2011, 215, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Osmancik, P.; Teringova, E.; Tousek, P.; Paulu, P.; Widimsky, P. Prognostic value of TNF-related apoptosis inducing ligand (TRAIL) in acute coronary syndrome patients. PLoS ONE 2013, 8, e53860. [Google Scholar] [CrossRef] [Green Version]
- Ajala, O.; Zhang, Y.; Gupta, A.; Bon, J.; Sciurba, F.; Chandra, D. Decreased serum TRAIL is associated with increased mortality in smokers with comorbid emphysema and coronary artery disease. Respir. Med. 2018, 145, 21–27. [Google Scholar] [CrossRef]
- Di Bartolo, B.A.; Cartland, S.P.; Prado-Lourenco, L.; Griffith, T.S.; Gentile, C.; Ravindran, J.; Azahri, N.S.; Thai, T.; Yeung, A.W.; Thomas, S.R.; et al. Tumor Necrosis Factor-Related Apoptosis-Inducing Ligand (TRAIL) Promotes Angiogenesis and Ischemia-Induced Neovascularization Via NADPH Oxidase 4 (NOX4) and Nitric Oxide-Dependent Mechanisms. J. Am. Heart Assoc. 2015, 4, e002527. [Google Scholar] [CrossRef] [Green Version]
- Cartland, S.P.; Genner, S.W.; Zahoor, A.; Kavurma, M.M. Comparative Evaluation of TRAIL, FGF-2 and VEGF-A-Induced Angiogenesis In Vitro and In Vivo. Int. J. Mol. Sci. 2016, 17, 2025. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.; Xiang, G.; Lu, J.; Xiang, L.; Dong, J.; Mei, W. TRAIL protects against endothelium injury in diabetes via Akt-eNOS signaling. Atherosclerosis 2014, 237, 718–724. [Google Scholar] [CrossRef]
- Manuneedhi Cholan, P.; Cartland, S.P.; Dang, L.; Rayner, B.S.; Patel, S.; Thomas, S.R.; Kavurma, M.M. TRAIL protects against endothelial dysfunction in vivo and inhibits angiotensin-II-induced oxidative stress in vascular endothelial cells in vitro. Free Radic. Biol. Med. 2018, 126, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Michowitz, Y.; Goldstein, E.; Roth, A.; Afek, A.; Abashidze, A.; Ben Gal, Y.; Keren, G.; George, J. The involvement of tumor necrosis factor-related apoptosis-inducing ligand (TRAIL) in atherosclerosis. J. Am. Coll. Cardiol. 2005, 45, 1018–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bova, C.; Sanchez, O.; Prandoni, P.; Lankeit, M.; Konstantinides, S.; Vanni, S.; Jimenez, D. Identification of intermediate-risk patients with acute symptomatic pulmonary embolism. Eur. Respir. J. 2014, 44, 694–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez, O.; Trinquart, L.; Caille, V.; Couturaud, F.; Pacouret, G.; Meneveau, N.; Verschuren, F.; Roy, P.M.; Parent, F.; Righini, M.; et al. Prognostic factors for pulmonary embolism: The prep study, a prospective multicenter cohort study. Am. J. Respir. Crit. Care Med. 2010, 181, 168–173. [Google Scholar] [CrossRef]
- Lankeit, M.; Friesen, D.; Schafer, K.; Hasenfuss, G.; Konstantinides, S.; Dellas, C. A simple score for rapid risk assessment of non-high-risk pulmonary embolism. Clin. Res. Cardiol. 2013, 102, 73–80. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 151) | Non-Events (n = 142) | Events (n = 9) | p Value | |
|---|---|---|---|---|
| Age, years | 66 (60–73) | 66 (60–73) | 62 (48–72) | 0.453 |
| Male | 63 (41.7) | 60 (42.3) | 3 (33.3) | 0.735 |
| Risk factors for VTE | ||||
| History of VTE | 19 (12.6) | 19 (13.4) | 0 | 0.603 |
| Immobility | 13 (8.6) | 12 (8.5) | 1 (11.1) | 0.566 |
| Recent surgery | 8 (5.3) | 7 (4.9) | 1 (11.1) | 0.396 |
| Recent long travel | 2 (1.3) | 2 (1.4) | 0 | 1.000 |
| Recent fracture | 9 (6.0) | 8 (5.6) | 1 (11.1) | 0.434 |
| Comorbidities | ||||
| Cancer | 9 (6.0) | 9 (6.3) | 0 | 1.000 |
| COPD | 8 (5.3) | 7 (4.9) | 1 (11.1) | 0.396 |
| Coronary heart disease | 25 (16.6) | 1 (11.1) | 24 (16.9) | 1.000 |
| Symptoms and signs | ||||
| Chest pain | 39 (25.8) | 38 (26.8) | 1 (11.1) | 0.448 |
| Dyspnea | 139 (92.1) | 130 (91.5) | 9 (100.0) | 1.000 |
| Syncope | 30 (19.9) | 24 (16.9) | 6 (66.7) | 0.002 |
| SBP, mmHg | 124 (114.5–124) | 124 (115–138) | 120 (113–134) | 0.691 |
| SBP < 100 mmHg | 4 (2.6) | 3 (2.1) | 1 (11.1) | 0.220 |
| Heart rate, bpm | 82 (73–98) | 82 (72–96) | 97 (84–102) | 0.010 |
| Heart rate ≥ 110 bpm | 9 (6.0) | 7 (4.9) | 2 (22.2) | 0.092 |
| SaO2 < 90% | 15 (9.9) | 13 (9.2) | 2 (22.2) | 0.220 |
| Elevated PASP | 49 (32.5) | 45 (31.7) | 4 (44.4) | 0.473 |
| RV dysfunction (on TTE) | 15 (9.9) | 10 (7.0) | 5 (55.6) | 0.001 |
| LVEF, % | 63 (60–67) | 64 (60–68) | 60 (56–64) | 0.083 |
| Laboratory biomarkers | ||||
| D-Dimer, ng/mL | 2166 (1076–3134) | 2114 (1056–3110) | 2823 (2389–3134) | 0.088 |
| Creatinine, µmol/L | 73.5 (61.1–83.7) | 73.2 (60.5–83.8) | 75.0 (62.6–83.1) | 0.75 |
| BNP, pg/mL | 141 (46–364) | 118 (44.0–310.0) | 1000 (653–2054) | 0.001 |
| hs-cTnI, ng/mL | 0.03 (0.01–0.15) | 0.02 (0.01–0.11) | 0.27 (0.09–0.91) | 0.001 |
| TRAIL, pg/mL | 23.1 (15.0–32.3) | 23.5 (16.1–32.6) | 10.1 (3.6–16.4) | 0.001 |
| sPESI ≥ 1 | 55 (36.4) | 47 (33.1) | 8(88.9) | 0.001 |
| Treatment | ||||
| Thrombolytic therapy | 9 (6.0) | 4 (2.8) | 5 (55.6) | 0.000 |
| OR | 95%CI | p Value | |
|---|---|---|---|
| Univariable analysis a | |||
| Age > 80 years | 3.43 | 0.36–32.90 | 0.286 |
| Cancer | - | - | - |
| COPD | 2.41 | 0.26–22.05 | 0.436 |
| Syncope | 9.83 | 2.30–42.08 | 0.002 |
| SBP < 100 mmHg | 5.79 | 0.54–62.12 | 0.147 |
| Heart rate ≥ 110 bpm | 5.51 | 0.96–31.57 | 0.055 |
| SaO2 < 90% | 2.84 | 0.53–15.09 | 0.222 |
| RV dysfunction (on TTE) | 16.5 | 3.82–71.30 | 0.000 |
| BNP, pg/mL, per SD | 3.60 | 1.91–6.78 | 0.000 |
| hs-cTnI, ng/mL, per SD | 1.25 | 0.85–1.85 | 0.254 |
| TRAIL, pg/mL, per SD | 0.18 | 0.06–0.56 | 0.003 |
| sPESI ≥ 1 | 16.17 | 1.96–133.11 | 0.010 |
| Multivariable analysis | |||
| Syncope | 2.48 | 0.20–31.12 | 0.481 |
| RV dysfunction (on TTE) | 16.47 | 1.06–256.27 | 0.045 |
| BNP, pg/mL, per SD | 3.68 | 1.24–10.89 | 0.019 |
| hs-cTnI, ng/mL, per SD | 1.45 | 0.64–3.32 | 0.375 |
| TRAIL, pg/mL, per SD | 0.19 | 0.04–0.90 | 0.036 |
| sPESI ≥ 1 | 1.09 | 0.06–21.54 | 0.956 |
| Biomarker-Based Algorithm (95% CI) | 2019 ESC Algorithm (95% CI) | Combination of TRAIL and the 2019 ESC Algorithm (95% CI) | |
|---|---|---|---|
| Low-risk vs. intermediate-low- and intermediate-high-risk | |||
| Sensitivity, % | 100 (66–100) | 100 (66–100) | 100 (66–100) |
| Specificity, % | 65 (56–73) | 44 (36–53) | 80 (72–86) |
| PPV, % | 15 (13–18) | 10 (9–12) | 24 (18–30) |
| NPV, % | 100 | 100 | 100 |
| +LR | 2.84 (2.3–3.5) | 1.80 (1.6–2.1) | 5 (3.5–6.8) |
| −LR | 0 | 0 | 0 |
| Low-risk and intermediate-low- vs. intermediate-high-risk | |||
| Sensitivity, % | 89 (52–100) | 56 (21–86) | - |
| Specificity, % | 88 (82–93) | 96 (92–99) | - |
| PPV, % | 32 (22–44) | 50 (26–74) | - |
| NPV, % | 99 (95–99) | 97 (94–99) | - |
| +LR | 7.42 (4.5–12.3) | 15.78 (5.6–44.7) | - |
| −LR | 0.13 (0.02–0.8) | 0.46 (0.2–1.0) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, H.; Rong, W.; Yang, J.; Lu, J.; Ma, K.; Liu, Z.; Yuan, H.; Xu, L.; Li, Y.; Jing, Z.-C.; et al. Tumor Necrosis Factor-Related Apoptosis-Inducing Ligand (TRAIL): A Novel Biomarker for Prognostic Assessment and Risk Stratification of Acute Pulmonary Embolism. J. Clin. Med. 2022, 11, 3908. https://doi.org/10.3390/jcm11133908
Yu H, Rong W, Yang J, Lu J, Ma K, Liu Z, Yuan H, Xu L, Li Y, Jing Z-C, et al. Tumor Necrosis Factor-Related Apoptosis-Inducing Ligand (TRAIL): A Novel Biomarker for Prognostic Assessment and Risk Stratification of Acute Pulmonary Embolism. Journal of Clinical Medicine. 2022; 11(13):3908. https://doi.org/10.3390/jcm11133908
Chicago/Turabian StyleYu, Haixu, Wei Rong, Jie Yang, Jie Lu, Ke Ma, Zhuohui Liu, Hui Yuan, Lei Xu, Yulin Li, Zhi-Cheng Jing, and et al. 2022. "Tumor Necrosis Factor-Related Apoptosis-Inducing Ligand (TRAIL): A Novel Biomarker for Prognostic Assessment and Risk Stratification of Acute Pulmonary Embolism" Journal of Clinical Medicine 11, no. 13: 3908. https://doi.org/10.3390/jcm11133908
APA StyleYu, H., Rong, W., Yang, J., Lu, J., Ma, K., Liu, Z., Yuan, H., Xu, L., Li, Y., Jing, Z.-C., & Du, J. (2022). Tumor Necrosis Factor-Related Apoptosis-Inducing Ligand (TRAIL): A Novel Biomarker for Prognostic Assessment and Risk Stratification of Acute Pulmonary Embolism. Journal of Clinical Medicine, 11(13), 3908. https://doi.org/10.3390/jcm11133908