
Influence of Depression and Sleep Quality on Postoperative Outcomes after Total Hip Arthroplasty: A Prospective Study


 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preoperative Depression
2.2. Preoperative Sleep Quality
2.3. Postoperative Scores
2.4. Statistical Analysis
3. Results
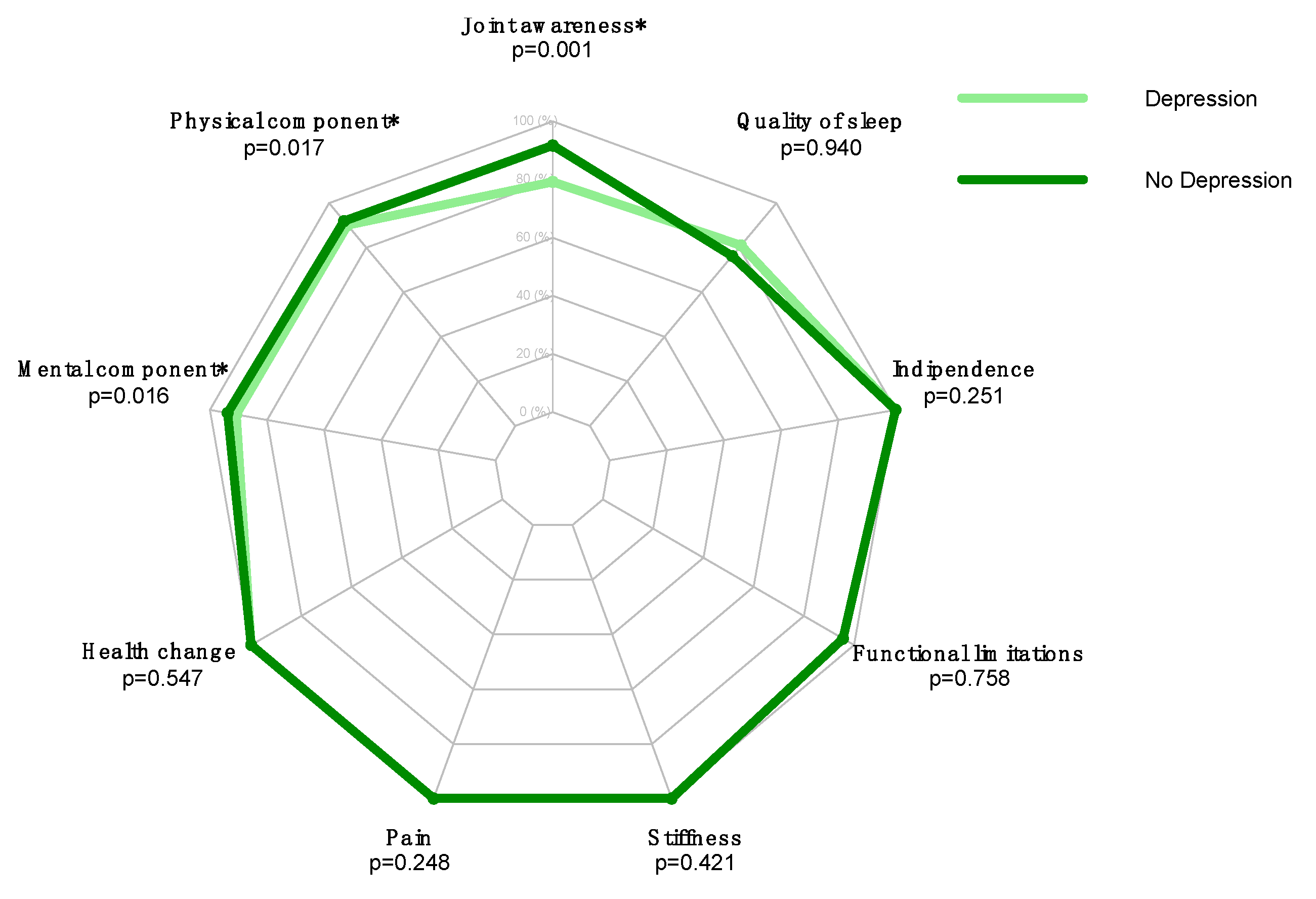
3.1. Preoperative Depression
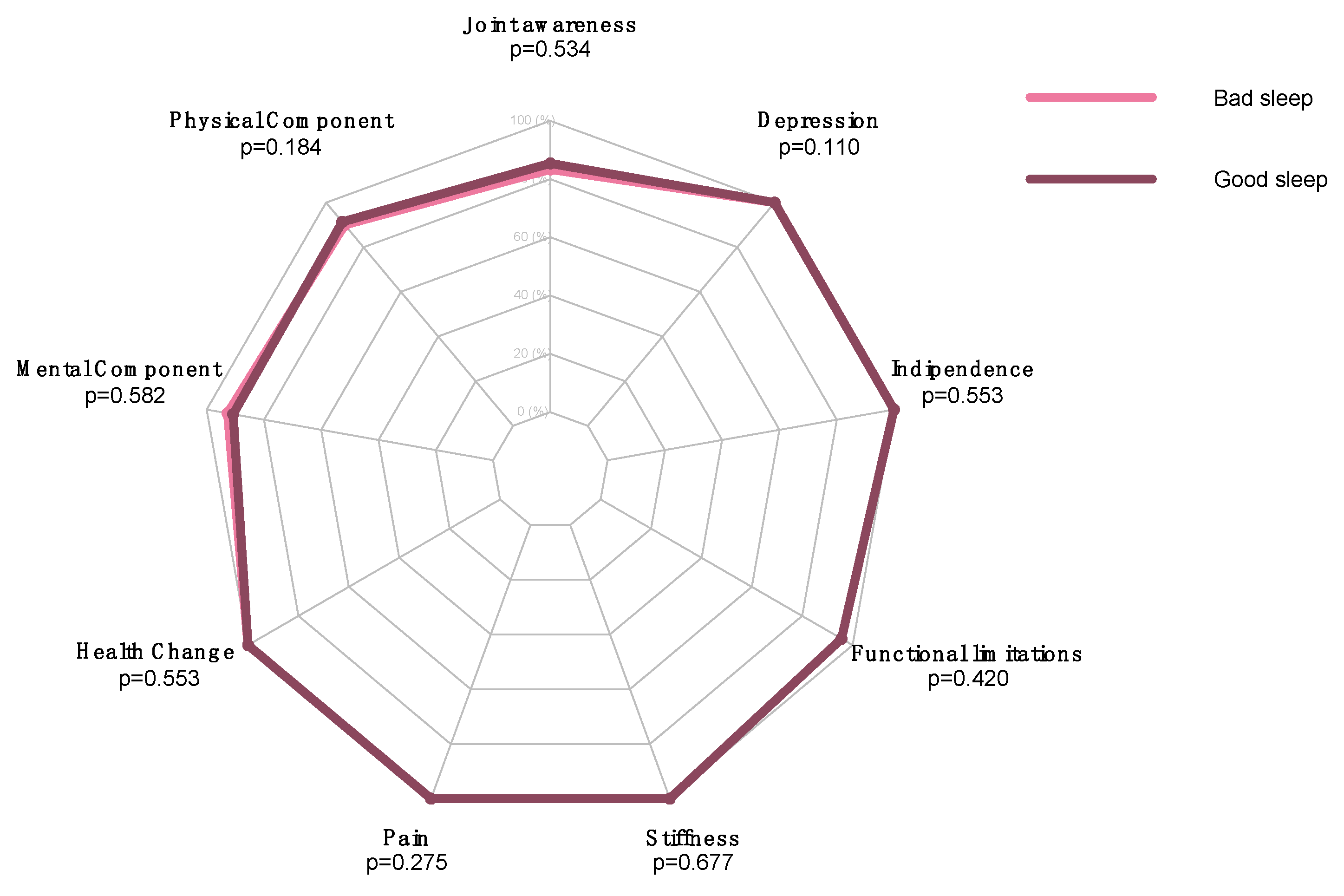
3.2. Preoperative Quality of Sleep
4. Discussion
4.1. Depression and THA Outcomes
4.2. Sleep and THA Outcomes
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DG | Depressed Group |
| FJS-12 | Forgotten Joint Score 12 |
| GDS | Geriatric Depression Scale |
| HOOS | Hip disability and Osteoarthritis Outcome Score |
| NDG | Non-Depressed Group |
| PSQI | Pittsburgh Sleep Quality Index |
| SF-36 | 36-item Short-Form Health Survey |
| SF-36-MCS | 36-item Short-Form Health Survey—Mental Component Summary |
| SF-36-PCS | 36-item Short-Form Health Survey—Physical Component Summary |
| THA | Total Hip Arthroplasty |
| TKA | Total Knee Arthroplasty |
| WOMAC | Western Ontario and McMaster University Osteoarthritis Index |
References
- Vina, E.R.; Kwoh, C.K. Epidemiology of osteoarthritis: Literature update. Curr. Opin. Rheumatol. 2018, 30, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Felson, D.T. Epidemiology of hip and knee osteoartrritis. Epidemiol. Rev. 1988, 10, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Maradit Kremers, H.; Larson, D.R.; Crowson, C.S.; Kremers, W.K.; Washington, R.E.; Steiner, C.A.; Jiranek, W.A.; Berry, D.J. Prevalence of Total Hip and Knee Replacement in the United States. J. Bone Jt. Surg. Am. Vol. 2015, 97, 1386–1397. [Google Scholar] [CrossRef] [Green Version]
- Frankel, S.; Eachus, J.; Pearson, N.; Greenwood, R.; Chan, P.; Peters, T.J.; Donovan, J.; Smith, G.D.; Dieppe, P. Population requirement for primary hip-replacement surgery: A cross-sectional study. Lancet 1999, 353, 1304–1309. [Google Scholar] [CrossRef]
- Chethan, K.N.; Bhat, S.; Zuber, M.; Shenoy, S. Finite Element Analysis of Different Hip Implant Designs along with Femur under Static Loading Conditions. J. Biomed. Phys. Eng. 2019, 9, 507–516. [Google Scholar] [CrossRef] [Green Version]
- Bhandari, M.; Busse, J.W.; Hanson, B.P.; Leece, P.; Ayeni, O.R.; Schemitsch, E.H. Psychological distress and quality of life after orthopedic trauma: An observational study. Can. J. Surg. 2008, 51, 15–22. [Google Scholar]
- Kumar, S.; Verma, V.; Kushwaha, U.; Hynes, E.J.C.; Arya, A.; Agarwal, A. Prevalence and association of depression in in-patient orthopaedic trauma patients: A single centre study in India. J. Clin. Orthop. Trauma 2020, 11, S573–S577. [Google Scholar] [CrossRef]
- Longo, U.G.; Berton, A.; De Salvatore, S.; Piergentili, I.; Casciani, E.; Faldetta, A.; De Marinis, M.G.; Denaro, V. Minimal Clinically Important Difference and Patient Acceptable Symptom State for the Pittsburgh Sleep Quality Index in Patients Who Underwent Rotator Cuff Tear Repair. Int. J. Environ. Res. Public Health 2021, 18, 8666. [Google Scholar] [CrossRef]
- Beetz, G.; Babiloni, A.H.; Jodoin, M.; Charlebois-Plante, C.; Lavigne, G.J.; De Beaumont, L.; Rouleau, D.M. Relevance of Sleep Disturbances to Orthopaedic Surgery: A Current Concepts Narrative and Practical Review. J. Bone Jt. Surg. 2021, 103, 2045–2056. [Google Scholar] [CrossRef]
- Luo, Z.-Y.; Li, L.-L.; Wang, D.; Wang, H.-Y.; Pei, F.-X.; Zhou, Z.-K. Preoperative sleep quality affects postoperative pain and function after total joint arthroplasty: A prospective cohort study. J. Orthop. Surg. Res. 2019, 14, 387. [Google Scholar] [CrossRef] [Green Version]
- Kohn, M.D.; Sassoon, A.A.; Fernando, N.D. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clin. Orthop. Relat. Res. 2016, 474, 1886–1893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galeoto, G.; Sansoni, J.; Scuccimarri, M.; Bruni, V.; De Santis, R.; Colucci, M.; Valente, D.; Tofani, M. A Psychometric Properties Evaluation of the Italian Version of the Geriatric Depression Scale. Depress. Res. Treat. 2018, 2018, 1797536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehra, A.; Agarwal, A.; Bashar, M.; Grover, S. Evaluation of Psychometric Properties of Hindi Versions of Geriatric Depression Scale and Patient Health Questionnaire in Older Adults. Indian J. Psychol. Med. 2021, 43, 319–324. [Google Scholar] [CrossRef]
- Curcio, G.G.; Tempesta, D.; Scarlata, S.; Marzano, C.; Moroni, F.; Rossini, P.M.; Ferrara, M.; De Gennaro, L. Validity of the Italian Version of the Pittsburgh Sleep Quality Index (PSQI). Neurol. Sci. 2013, 34, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Giesinger, J.M.; Behrend, H.; Hamilton, D.F.; Kuster, M.S.; Giesinger, K. Normative Values for the Forgotten Joint Score-12 for the US General Population. J. Arthroplast. 2019, 34, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; De Salvatore, S.; Di Naro, C.; Sciotti, G.; Cirimele, G.; Piergentili, I.; De Marinis, M.G.; Denaro, V. Unicompartmental knee arthroplasty: The Italian version of the Forgotten Joint Score-12 is valid and reliable to assess prosthesis awareness. Knee Surg. Sports Traumatol. Arthrosc. 2021, 30, 1250–1256. [Google Scholar] [CrossRef]
- Apolone, G.; Mosconi, P. The Italian SF-36 Health Survey: Translation, Validation and Norming. J. Clin. Epidemiol. 1998, 51, 1025–1036. [Google Scholar] [CrossRef]
- MacKay, C.; Clements, N.; Wong, R.; Davis, A.M. A systematic review of estimates of the minimal clinically important difference and patient acceptable symptom state of the Western Ontario and McMaster Universities Osteoarthritis Index in patients who underwent total hip and total knee replacement. Osteoarthr. Cartil. 2019, 27, 1408–1419. [Google Scholar] [CrossRef]
- Salaffi, F.; Leardini, G.; Canesi, B.; Mannoni, A.; Fioravanti, A.; Caporali, R.; Lapadula, G.; Punzi, L.; GOnorthrosis and Quality Of Life Assessment (GOQOLA). Reliability and validity of the Western Ontario and McMaster Universities (WOMAC) Osteoarthritis Index in Italian patients with osteoarthritis of the knee. Osteoarthr. Cartil. 2003, 11, 551–560. [Google Scholar] [CrossRef] [Green Version]
- Martinez, R.; Reddy, N.; Mulligan, E.P.; Hynan, L.S.; Wells, J. Sleep quality and nocturnal pain in patients with hip osteoarthritis. Medicine 2019, 98, e17464. [Google Scholar] [CrossRef] [PubMed]
- Wongpakaran, N.; Wongpakaran, T.; Kuntawong, P. Evaluating hierarchical items of the geriatric depression scale through factor analysis and item response theory. Heliyon 2019, 5, e02300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duivenvoorden, T.; Vissers, M.M.; Verhaar, J.A.; Busschbach, J.J.; Gosens, T.; Bloem, R.M.; Bierma-Zeinstra, S.M.; Reijman, M. Anxiety and depressive symptoms before and after total hip and knee arthroplasty: A prospective multicentre study. Osteoarthr. Cartil. 2013, 21, 1834–1840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, U.-S.D.T.; Perneger, T.; Franklin, P.D.; Barea, C.; Hoffmeyer, P.; Lübbeke, A. Improvement in mental health following total hip arthroplasty: The role of pain and function. BMC Musculoskelet. Disord. 2019, 20, 307. [Google Scholar] [CrossRef]
- Santić, V.; Legović, D.; Sestan, B.; Jurdana, H.; Marinović, M. Measuring improvement following total hip and knee arthroplasty using the SF-36 Health Survey. Coll. Antropol. 2012, 36, 207–212. [Google Scholar]
- Ng, C.Y.; Ballantyne, J.A.; Brenkel, I.J. Quality of life and functional outcome after primary total hip replacement. A five-year follow-up. J. Bone Jt. Surg. Br. Vol. 2007, 89, 868–873. [Google Scholar] [CrossRef]
- Longo, U.G.; Ciuffreda, M.; Candela, V.; Berton, A.; Maffulli, N.; Denaro, V. Hip scores: A current concept review. Br. Med Bull. 2019, 131, 81–96. [Google Scholar] [CrossRef]
- Punwar, S.; Khan, W.S.; Longo, U.G. The use of computer navigation in hip arthroplasty: Literature review and evidence today. Ortop. Traumatol. Rehabil. 2011, 13, 431–438. [Google Scholar] [CrossRef] [Green Version]
- Larsson, A.; Rolfson, O.; Kärrholm, J. Evaluation of Forgotten Joint Score in total hip arthroplasty with Oxford Hip Score as reference standard. Acta Orthop. 2019, 90, 253–257. [Google Scholar] [CrossRef] [Green Version]
- Sethy, S.S.; Goyal, T.; Paul, S.; Das, S.L.; Choudhury, A.K.; Kalia, R.B. Translation and Validation of Forgotten Joint Score for Total Hip Arthroplasty for Indian Population. Indian J. Orthop. 2020, 54, 892–900. [Google Scholar] [CrossRef]
- Longo, U.G.; De Salvatore, S.; Piergentili, I.; Indiveri, A.; Di Naro, C.; Santamaria, G.; Marchetti, A.; Marinis, M.G.; Denaro, V. Total Hip Arthroplasty: Minimal Clinically Important Difference and Patient Acceptable Symptom State for the Forgotten Joint Score 12. Int. J. Environ. Res. Public Health 2021, 18, 2267. [Google Scholar] [CrossRef] [PubMed]
- Loppini, M.; Longo, U.G.; Caldarella, E.; Rocca, A.D.; Denaro, V.; Grappiolo, G. Femur first surgical technique: A smart non-computer-based procedure to achieve the combined anteversion in primary total hip arthroplasty. BMC Musculoskelet. Disord. 2017, 18, 331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seagrave, K.G.; Lewin, A.M.; Harris, I.A.; Badge, H.; Naylor, J. Association between pre-operative anxiety and/or depression and outcomes following total hip or knee arthroplasty. J. Orthop. Surg. 2021, 29, 2309499021992605. [Google Scholar] [CrossRef] [PubMed]
- Götz, J.S.; Benditz, A.; Reinhard, J.; Schindler, M.; Zeman, F.; Grifka, J.; Greimel, F.; Leiss, F. Influence of Anxiety/Depression, Age, Gender and ASA on 1-Year Follow-Up Outcomes Following Total Hip and Knee Arthroplasty in 5447 Patients. J. Clin. Med. 2021, 10, 3095. [Google Scholar] [CrossRef] [PubMed]
- Bulamu, N.B.; Kaambwa, B.; Ratcliffe, J. A systematic review of instruments for measuring outcomes in economic evaluation within aged care. Health Qual. Life Outcomes 2015, 13, 179. [Google Scholar] [CrossRef] [Green Version]
- Tristaino, V.; Lantieri, F.; Tornago, S.; Gramazio, M.; Carriere, E.; Camera, A. Effectiveness of psychological support in patients undergoing primary total hip or knee arthroplasty: A controlled cohort study. J. Orthop. Traumatol. 2016, 17, 137–147. [Google Scholar] [CrossRef] [Green Version]
- Bay, S.; Kuster, L.; McLean, N.; Byrnes, M.; Kuster, M.S. A systematic review of psychological interventions in total hip and knee arthroplasty. BMC Musculoskelet. Disord. 2018, 19, 201. [Google Scholar] [CrossRef]
- Van Meirhaeghe, J.P.; Salmon, L.J.; O’Sullivan, M.D.; Gooden, B.R.; Lyons, M.C.; Pinczewski, L.A.; Roe, J.P. Improvement in Sleep Patterns After Hip and Knee Arthroplasty: A Prospective Study in 780 Patients. J. Arthroplast. 2021, 36, 442–448. [Google Scholar] [CrossRef]
- Hochreiter, J.; Kindermann, H.; Georg, M.; Ortmaier, R.; Mitterer, M. Sleep improvement after hip arthroplasty: A study on short-stem prosthesis. Int. Orthop. 2020, 44, 69–73. [Google Scholar] [CrossRef] [Green Version]
- Shakya, H.; Wang, D.; Zhou, K.; Luo, Z.-Y.; Dahal, S.; Zhou, Z.-K. Prospective randomized controlled study on improving sleep quality and impact of zolpidem after total hip arthroplasty. J. Orthop. Surg. Res. 2019, 14, 289. [Google Scholar] [CrossRef] [Green Version]
- Gong, L.; Wang, Z.; Fan, D. Sleep Quality Effects Recovery After Total Knee Arthroplasty (TKA)—A Randomized, Double-Blind, Controlled Study. J. Arthroplast. 2015, 30, 1897–1901. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | GDS | |
|---|---|---|
| Rho | p-Value | |
| FJS-12 | 0.322 | 0.011 * |
| SF-36 PCS | 0.328 | 0.01 * |
| SF-36 MCS | 0.293 | 0.022 * |
| SF-36 Health change | 0.057 | 0.665 |
| WOMAC Pain | 0.128 | 0.325 |
| WOMAC Stiffness | 0.062 | 0.632 |
| WOMAC Functional Limitations | 0.085 | 0.513 |
| WOMAC Overall | 0.086 | 0.509 |
| BARTHEL | 0.083 | 0.525 |
| PSQI | −0.014 | 0.913 |
| Parameter | Depression (n = 37) | No Depression (n = 24) | p-Value | ||
|---|---|---|---|---|---|
| Median | Range | Median | Range | ||
| FJS-12 | 79.2 | 22.9–100 | 91.7 | 56.3–100 | 0.001 * |
| SF-36 PCS | 90.0 | 30–98.8 | 91.9 | 75.6–100 | 0.017 * |
| SF-36 MCS | 90.8 | 30.5–100 | 93.8 | 83.8–100 | 0.016 * |
| SF-36 Health change | 100.0 | 75–100 | 100.0 | 75–100 | 0.547 |
| WOMAC Pain | 100.0 | 75–100 | 100.0 | 90–100 | 0.248 |
| WOMAC Stiffness | 100.0 | 87.5–100 | 100.0 | 100–100 | 0.421 |
| WOMAC Functional Limitations | 95.6 | 55.9–100 | 95.6 | 79.4–100 | 0.758 |
| WOMAC Overall | 96.9 | 63.5–100 | 96.9 | 83.3–100 | 0.690 |
| BARTHEL | 100.0 | 50–100 | 100.0 | 100–100 | 0.251 |
| PSQI | 81.0 | 33.3–85.7 | 76.2 | 47.6–95.2 | 0.940 |
| Parameter | PSQI | |
|---|---|---|
| Rho | p-Value | |
| FJS-12 | −0.021 | 0.87 |
| SF-36 PCS | 0.127 | 0.329 |
| SF-36 MCS | 0.017 | 0.9 |
| SF-36 Health change | −0.19 | 0.143 |
| WOMAC Pain | 0.114 | 0.383 |
| WOMAC Stiffness | 0.152 | 0.243 |
| WOMAC Functional Limitations | −0.049 | 0.708 |
| WOMAC Overall | −0.03 | 0.819 |
| BARTHEL | −0.06 | 0.645 |
| GDS | 0.185 | 0.153 |
| Parameter | Bad Sleep (n = 52) | Good Sleep (n = 9) | p-Value | ||
|---|---|---|---|---|---|
| Median | Range | Median | Range | ||
| FJS-12 | 83.3 | 22.9–100 | 85.4 | 56.3–100 | 0.534 |
| SF-36 PCS | 90.0 | 30–100 | 91.3 | 86.3–100 | 0.184 |
| SF-36 MCS | 92.7 | 30.5–100 | 90.8 | 83.8–96.8 | 0.582 |
| SF-36 Health change | 100.0 | 75–100 | 100.0 | 75–100 | 0.553 |
| WOMAC Pain | 100.0 | 75–100 | 100.0 | 95–100 | 0.275 |
| WOMAC Stiffness | 100.0 | 87.5–100 | 100.0 | 100–100 | 0.677 |
| WOMAC Functional Limitations | 95.6 | 55.9–100 | 95.6 | 86.8–100 | 0.420 |
| WOMAC Overall | 96.9 | 63.5–100 | 96.9 | 90.6–100 | 0.419 |
| BARTHEL | 100.0 | 50–100 | 100.0 | 100–100 | 0.553 |
| GDS | 100.0 | 33.3–100 | 100.0 | 96.7–100 | 0.110 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longo, U.G.; De Salvatore, S.; Greco, A.; Marino, M.; Santamaria, G.; Piergentili, I.; De Marinis, M.G.; Denaro, V. Influence of Depression and Sleep Quality on Postoperative Outcomes after Total Hip Arthroplasty: A Prospective Study. J. Clin. Med. 2022, 11, 3845. https://doi.org/10.3390/jcm11133845
Longo UG, De Salvatore S, Greco A, Marino M, Santamaria G, Piergentili I, De Marinis MG, Denaro V. Influence of Depression and Sleep Quality on Postoperative Outcomes after Total Hip Arthroplasty: A Prospective Study. Journal of Clinical Medicine. 2022; 11(13):3845. https://doi.org/10.3390/jcm11133845
Chicago/Turabian StyleLongo, Umile Giuseppe, Sergio De Salvatore, Alessandra Greco, Martina Marino, Giulia Santamaria, Ilaria Piergentili, Maria Grazia De Marinis, and Vincenzo Denaro. 2022. "Influence of Depression and Sleep Quality on Postoperative Outcomes after Total Hip Arthroplasty: A Prospective Study" Journal of Clinical Medicine 11, no. 13: 3845. https://doi.org/10.3390/jcm11133845
APA StyleLongo, U. G., De Salvatore, S., Greco, A., Marino, M., Santamaria, G., Piergentili, I., De Marinis, M. G., & Denaro, V. (2022). Influence of Depression and Sleep Quality on Postoperative Outcomes after Total Hip Arthroplasty: A Prospective Study. Journal of Clinical Medicine, 11(13), 3845. https://doi.org/10.3390/jcm11133845