
Factors Related to Beliefs about Medication in Ischemic Stroke Patients

Abstract
:1. Introduction
2. Methods
2.1. Study Design and Subjects
2.2. Measurement
2.3. Beliefs about Medicine Questionnaire: BMQ-Specific
2.4. ENRICHD Social Support Inventory (ESSI)
2.5. Type D Personality Scale-14: DS14
2.6. Health Literacy
2.7. State-Trait Anxiety Inventory (STAI)
2.8. Knowledge about Stroke Medication
2.9. Data Collection
2.10. Statistical Analysis
3. Results
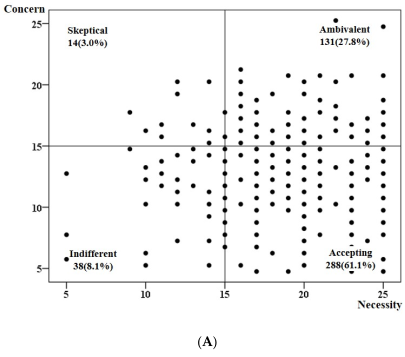
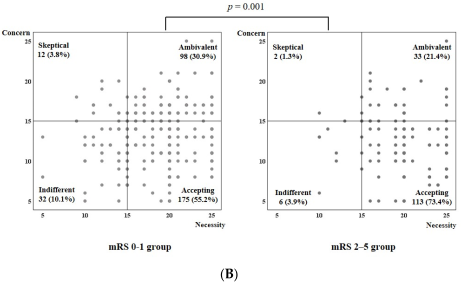
3.1. Participants’ Medication Beliefs and Belief Attitudes
3.2. Factors Related to Necessity, Concerns, and Medication Beliefs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, J.Y.; Kang, K.; Kang, J.; Koo, J.; Kim, D.H.; Kim, B.J.; Kim, W.J.; Kim, E.G.; Kim, J.G.; Kim, J.M.; et al. Executive summary of stroke statistics in Korea 2018: A report from the Epidemiology Research Council of the Korean Stroke Society. J. Stroke 2019, 21, 42–59. [Google Scholar] [CrossRef] [PubMed]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Deruyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L.; et al. Guidelines for adult stroke rehabilitation and recovery: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Gong, Y.; Zhao, Y.; Jiang, N.; Wang, J.; Yin, X. Post-stroke medication adherence and persistence rates: A meta-analysis of observational studies. J. Neurol. 2021, 268, 2090–2098. [Google Scholar] [CrossRef] [PubMed]
- Kumbhani, D.J.; Steg, P.G.; Cannon, C.P.; Eagle, K.A.; Smith, S.C., Jr.; Hoffman, E.; Goto, S.; Ohman, E.M.; Bhatt, D.L.; REduction of Atherothrombosis for Continued Health Registry Investigators. Adherence to secondary prevention medications and four-year outcomes in outpatients with atherosclerosis. Am. J. Med. 2013, 126, 693–700.e1. [Google Scholar] [CrossRef] [PubMed]
- Arkan, G.; Sarigol Ordin, Y.; Ozturk, V.; Ala, R.T. Investigation of medication adherence and factors affecting it in patients with stroke. J. Neurosci. Nurs. 2022, 54, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Horne, R.; Chapman, S.C.; Parham, R.; Freemantle, N.; Forbes, A.; Cooper, V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: A meta-analytic review of the Necessity-Concerns Framework. PLoS ONE 2013, 8, e80633. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.G.; Chae, D.H.; Park, M.S.; Yoo, S.H. Factors influencing 1-year medication adherence of Korean ischemic stroke survivors. Int. J. Behav. Med. 2020, 27, 225–234. [Google Scholar] [CrossRef]
- Horne, R.; Weinman, J. Predicting treatment adherence: An overview of theoretical models. In Adherence to Treatment in Medical Conditions; CRC Press: Boca Raton, FL, USA, 2020. [Google Scholar] [CrossRef]
- Horne, R.; Weinman, J.; Hankins, M. The beliefs about medicines questionnaire: The development and evaluation of a new method for assessing the cognitive representation of medication. Psychol. Health 1999, 14, 1–24. [Google Scholar] [CrossRef]
- Marshall, V.K.; Given, B.A. Factors associated with medication beliefs in patients with cancer: An integrative review. Oncol. Nurs. Forum. 2018, 45, 508–526. [Google Scholar] [CrossRef]
- Wilhelm, M.; Rief, W.; Doering, B.K. It’s all a matter of necessity and concern: A structural equation model of adherence to antihypertensive medication. Patient Educ. Couns. 2018, 101, 497–503. [Google Scholar] [CrossRef]
- Kim, S.R.; Kim, J.Y.; Kim, H.Y.; So, H.Y.; Chung, S.J. Factors associated with medication beliefs in patients with Parkinson’s disease: A cross-sectional study. J. Mov. Disord. 2021, 14, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Ko, Y.; Lee, S.; Chung, J.W.; Han, M.K.; Park, J.M.; Kang, K.; Park, T.H.; Park, S.S.; Cho, Y.J.; Hong, K.S.; et al. MRI-based algorithm for acute ischemic stroke subtype classification. J. Stroke 2014, 16, 161–172. [Google Scholar] [CrossRef] [Green Version]
- Banks, J.L.; Marotta, C.A. Outcomes validity and reliability of the modified Rankin scale: Implications for stroke clinical trials: A literature review and synthesis. Stroke 2007, 38, 1091–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomalla, G.; Fiebach, J.B.; Østergaard, L.; Pedraza, S.; Thijs, V.; Nighoghossian, N.; Roy, P.; Muir, K.W.; Ebinger, M.; Cheng, B.; et al. A multicenter, randomized, double-blind, placebo-controlled trial to test efficacy and safety of magnetic resonance imaging-based thrombolysis in wake-up stroke (WAKE-UP). Int. J. Stroke 2014, 9, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Suh, M.; Choi-Kwon, S. Structural equation modeling on quality of life in stroke survivors. J. Korean Acad. Nurs. 2010, 40, 533–541. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, P.H.; Powell, L.; Blumenthal, J.; Norten, J.; Ironson, G.; Pitula, C.R.; Froelicher, E.S.; Czajkowski, S.; Youngblood, M.; Huber, M.; et al. A short social support measure for patients recovering from myocardial infarction: The ENRICHD Social Support Inventory. J. Cardiopulm. Rehabil. 2003, 23, 398–403. [Google Scholar] [CrossRef]
- Denollet, J. DS14: Standard assessment of negative affectivity, social inhibition, and type D personality. Psychosom. Med. 2005, 67, 89–97. [Google Scholar] [CrossRef]
- Arozullah, A.M.; Yarnold, P.R.; Bennett, C.L.; Soltysik, R.C.; Wolf, M.S.; Ferreira, R.M.; Lee, S.Y.D.; Costello, S.; Shakir, A.; Denwood, C.; et al. Development and validation of a short-form, rapid estimate of adult literacy in medicine. Med. Care 2007, 45, 1026–1033. [Google Scholar] [CrossRef]
- Han, D.W.; Lee, C.H.; Chon, K.K. Korean adaptation of Spielberger’s STAI (K-STAI). Kor. J. Health Psychol. 1996, 1, 1–14. [Google Scholar]
- Hong, K.S.; Yu, K.H.; Rha, J.H.; Kim, H.Y.; Koo, J.; Park, J.M.; Seo, D.H.; Park, I.S.; Cho, K.H.; Jung, K.H.; et al. Review of evidences and updates of the Korean clinical practice guidelines for stroke in 2013. J. Korean Neurol. Assoc. 2013, 31, 143–157. [Google Scholar]
- Declaration Helsinki. Ethical Principles for Medical Research Involving Human Subject. World Medical Association. Available online: https://www.wma.net/wp-content/uploads/2016/11/DoH-Oct2013-JAMA.pdf (accessed on 19 April 2020).
- Jung, J.H.; Kim, Y.H.; Han, D.J.; Kim, K.S.; Chu, S.H. Medication adherence in patients taking immunosuppressants after kidney transplantation. J. Korean Soc. Transplant. 2010, 24, 289–297. [Google Scholar] [CrossRef] [Green Version]
- Bae, S.G.; Jeon, H.J.; Yang, H.S.; Kim, B.K.; Park, K.S. Medication adherence and its predictors in community elderly patients with hypertension. Korean J. Health Promot. 2015, 15, 121–128. [Google Scholar] [CrossRef]
- Vrettos, I.; Voukelatou, P.; Katsoras, A.; Theotoka, D.; Kalliakmanis, A. Diseases linked to polypharmacy in elderly patients. Curr. Gerontol. Geriatr. Res. 2017, 2017, 4276047. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Lee, J.E.; Jung, K.Y.; Kim, M.Y.; Yoo, S.-H.; Yoon, J.-L. Polypharmacy and inappropriate drug prescription in community-dwelling elderly. Korean J. Fam. Med. 2008, 29, 925–931. [Google Scholar]
- Morgan, S.G.; Weymann, D.; Pratt, B.; Smolina, K.; Gladstone, E.J.; Raymond, C.; Mintzes, B. Sex differences in the risk of receiving potentially inappropriate prescriptions among older adults. Age Ageing 2016, 45, 535–542. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.J.; Shin, K.R.; Yi, H.R.; Ju, S.K. Knowledge, health belief, and self-efficacy related to osteoporosis. Taehan Kanho Hakhoe Chi. 2005, 35, 757–850. [Google Scholar] [CrossRef]
- Williams, L.; O’Connor, R.C.; Grubb, N.; O’Carroll, R. Type D personality predicts poor medication adherence in myocardial infarction patients. Psychol. Health 2011, 26, 703–712. [Google Scholar] [CrossRef]
- Crayton, E.; Fahey, M.; Ashworth, M.; Besser, S.J.; Weinman, J.; Wright, A.J. Psychological determinants of medication adherence in stroke survivors: A systematic review of observational studies. Ann. Behav. Med. 2017, 51, 833–845. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| (n = 471) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics | Medication Beliefs | ||||||||||
| n (%) or M ± SD | Necessity | Concerns | Total score | ||||||||
| M ± SD | t or F or r | p | M ± SD | t or F or r | p | M ± SD | t or F or r | p | |||
| Socio-economic factors | |||||||||||
| Age (year) | 63.42 ± 12.16 | 0.30 | <0.001 | −0.26 | <0.001 | 0.37 | <0.001 | ||||
| Gender | Male | 324 (68.8) | 18.86 ± 4.25 | −3.89 | <0.001 | 12.65 ± 3.95 | 2.72 | 0.007 | 6.21 ± 5.87 | −4.24 | <0.001 |
| Female | 147 (31.2) | 20.46 ± 3.82 | 11.48 ± 4.52 | 8.98 ± 6.86 | |||||||
| Education level | |||||||||||
| Primary school and under a | 138 (29.3) | 20.67 ± 3.76 | 7.55 | <0.001 | 11.04 ± 4.72 | 6.19 | <0.001 | 9.63 ± 6.93 | 12.17 | <0.001 | |
| Middle school b | 69 (14.6) | 19.45 ± 3.51 | a > c,d †† | 12.67 ± 3.75 | a < b,c,d †† | 6.78 ± 5.83 | a > b,c,d †† | ||||
| High school c | 165 (35.0) | 18.79 ± 3.98 | 12.69 ± 3.86 | 6.10 ± 5.25 | |||||||
| Above college d | 99 (21.0) | 18.42 ± 5.01 | 13.08 ± 3.80 | 5.34 ± 6.40 | |||||||
| Marital status | Married a | 375 (79.6) | 19.16 ± 4.12 | 6.75 | 0.001 | 12.50 ± 4.00 | 11.65 | <0.001 | 6.66 ± 5.98 | 16.09 | <0.001 |
| Widowed b | 61 (13.0) | 21.11 ± 3.77 | b > a,c † | 10.11 ± 4.78 | a,c > b † | 11.00 ± 7.08 | b > a,c † | ||||
| Single c | 35 (7.4) | 18.49 ± 4.77 | 13.83 ± 3.68 | 4.66 ± 5.94 | |||||||
| Job | Employed | 270 (57.3) | 18.69 ± 4.28 | −4.14 | <0.001 | 12.94 ± 3.86 | 3.93 | <0.001 | 5.74 ± 5.69 | −5.32 | <0.001 |
| Unemployed | 201 (42.7) | 20.27 ± 3.87 | 11.41 ± 4.41 | 8.86 ± 6.69 | |||||||
| ESSI: social support | 20.96 ± 3.90 | −0.09 | 0.045 | −0.13 | 0.006 | 0.02 | 0.641 | ||||
| Psychological factors | |||||||||||
| Health literacy | 3.62 ± 2.87 | −0.001 | 0.982 | 0.16 | 0.001 | −0.11 | 0.022 | ||||
| D type | Yes | 235 (49.9) | 19.79 ± 3.69 | 2.24 | 0.025 | 13.59 ± 4.01 | 7.13 | <0.001 | 6.20 ± 5.81 | −3.02 | 0.003 |
| personality | No | 236 (50.1) | 18.93 ± 4.58 | 10.99 ± 3.92 | 7.94 ± 6.69 | ||||||
| STAI: state anxiety | 43.74 ± 11.71 | −0.14 | 0.002 | 0.16 | 0.001 | −0.20 | <0.001 | ||||
| Knowledge about medication | 4.98 ± 1.87 | 0.05 | 0.289 | −0.16 | <0.001 | 0.14 | 0.002 | ||||
| Condition-related factors | |||||||||||
| Stroke risk factors § | |||||||||||
| HTN | Yes | 301 (63.9) | 19.72 ± 4.21 | 2.53 | 0.012 | 11.77 ± 4.31 | −3.79 | <0.001 | 7.96 ± 6.55 | 4.29 | <0.001 |
| No | 170 (36.1) | 18.72 ± 4.05 | 13.21 ± 3.74 | 5.51 ± 5.58 | |||||||
| DM | Yes | 141 (29.9) | 19.88 ± 4.14 | 1.76 | 0.078 | 11.32 ± 4.13 | −3.33 | 0.001 | 8.56 ± 6.59 | 3.37 | 0.001 |
| No | 330 (70.1) | 19.14 ± 4.18 | 12.70 ± 4.12 | 6.44 ± 6.11 | |||||||
| Hyperlipidemia | Yes | 191 (40.6) | 19.94 ± 3.80 | 2.49 | 0.011 | 13.09 ± 4.23 | 3.49 | 0.001 | 6.85 ± 6.19 | −0.64 | 0.522 |
| No | 280 (59.4) | 18.97 ± 4.38 | 11.74 ± 4.05 | 7.23 ± 6.42 | |||||||
| MI | Yes | 47 (10.0) | 20.57 ± 3.72 | 2.11 | 0.036 | 11.60 ± 4.35 | −1.20 | 0.232 | 8.98 ± 6.07 | 2.19 | 0.029 |
| No | 424 (90.0) | 19.23 ± 4.21 | 12.36 ± 4.15 | 6.86 ± 6.32 | |||||||
| Afib | Yes | 53 (11.3) | 20.38 ± 4.41 | 1.89 | 0.060 | 13.36 ± 4.90 | 1.72 | 0.090 | 7.02 ± 7.23 | −0.07 | 0.946 |
| No | 418 (88.7) | 19.23 ± 4.14 | 12.15 ± 4.05 | 7.08 ± 6.21 | |||||||
| Current | Yes | 151 (32.1) | 18.07 ± 4.26 | −4.70 | <0.001 | 12.50 ± 3.44 | 0.85 | 0.396 | 5.57 ± 5.50 | −3.83 | <0.001 |
| smoking | No | 320 (67.9) | 19.97 ± 4.01 | 12.18 ± 4.48 | 7.78 ± 6.57 | ||||||
| Stroke subtype (n = 442) | Ischemic | 433 (91.9) | 19.47 ± 4.23 | 1.90 | 0.058 | 12.19 ± 4.20 | −1.71 | 0.088 | 7.28 ± 6.40 | 3.00 | 0.004 |
| TIA | 38 (8.1) | 18.13 ± 3.42 | 13.39 ± 3.68 | 4.74 ± 4.87 | |||||||
| TOAST (n = 433) | LAA a | 104 (22.1) | 19.39 ± 4.48 | 5.09 | 0.002 | 11.52 ± 4.19 | 3.55 | 0.015 | 7.88 ± 6.95 | 6.18 | <0.001 |
| CE b | 63 (13.4) | 19.97 ± 4.22 | d > c † | 12.83 ± 4.79 | 7.14 ± 6.47 | d > c †† | |||||
| SVO c | 193 (41.0) | 18.79 ± 3.93 | 12.69 ± 3.90 | 6.09 ± 5.69 | |||||||
| Others d | 73 (15.5) | 20.95 ± 4.26 | 11.26 ± 4.21 | 9.68 ± 6.64 | |||||||
| mRS at discharge | 1.31 ± 1.27 | 0.19 | <0.001 | −0.19 | <0.001 | 0.24 | <0.001 | ||||
| mRS subgroup | mRS 0–1 | 317 (67.3) | 18.85 ± 4.26 | 3.87 | <0.001 | 12.73 ± 4.02 | −3.36 | 0.001 | 6.12 ± 5.94 | 4.83 | <0.001 |
| mRS 2–5 | 154 (32.7) | 20.42 ± 3.82 | 11.37 ± 4.33 | 9.05 ± 6.64 | |||||||
| Therapy-related factors | |||||||||||
| Frequency of medication | 2.28 ± 0.58 | 0.18 | <0.001 | 0.04 | 0.453 | 0.09 | 0.041 | ||||
| Number of medications | 6.38 ± 2.55 | 0.29 | <0.001 | −0.02 | 0.632 | 0.20 | <0.001 | ||||
| Type of stroke medicine § | |||||||||||
| Anti-platelet | Yes | 416 (88.3) | 19.21 ± 4.19 | −2.21 | 0.027 | 12.16 ± 4.09 | −1.77 | 0.078 | 7.04 ± 6.28 | −0.29 | 0.770 |
| No | 55 (11.7) | 20.53 ± 3.96 | 13.22 ± 4.69 | 7.31 ± 6.70 | |||||||
| Warfarin | Yes | 13 (2.8) | 20.15 ± 4.02 | 0.69 | 0.488 | 12.85 ± 4.81 | 0.49 | 0.624 | 7.31 ± 6.92 | 0.14 | 0.893 |
| No | 458 (97.2) | 19.34 ± 4.19 | 12.27 ± 4.16 | 7.07 ± 6.31 | |||||||
| NOAC | Yes | 56 (11.9) | 20.41 ± 4.34 | 2.01 | 0.045 | 13.13 ± 4.70 | 1.61 | 0.109 | 7.29 ± 6.43 | 0.27 | 0.790 |
| No | 415 (88.1) | 19.22 ± 4.14 | 12.17 ± 4.09 | 7.05 ± 6.32 | |||||||
| Anti-HTN | Yes | 250 (53.1) | 19.69 ± 4.11 | 1.81 | 0.071 | 11.68 ± 4.25 | −3.40 | 0.001 | 8.01 ± 6.34 | 3.45 | 0.001 |
| agent | No | 221 (46.9) | 18.99 ± 4.23 | 12.97 ± 3.98 | 6.02 ± 6.14 | ||||||
| Anti-diabetic | Yes | 123 (26.1) | 19.82 ± 4.21 | 1.42 | 0.156 | 11.24 ± 3.86 | −3.29 | 0.001 | 8.59 ± 6.41 | 3.11 | 0.002 |
| agent | No | 348 (73.9) | 19.20 ± 4.16 | 12.66 ± 4.22 | 6.54 ± 6.21 | ||||||
| Anti-lipidemic | Yes | 451 (95.8) | 19.37 ± 4.17 | 0.12 | 0.904 | 12.25 ± 4.13 | −0.78 | 0.435 | 7.11 ± 6.34 | 0.60 | 0.552 |
| agent | No | 20 (4.2) | 19.25 ± 4.60 | 13.00 ± 4.96 | 6.25 ± 6.01 | ||||||
| Healthcare team-related factors | |||||||||||
| Satisfaction with healthcare providers’ explanation | 3.98 ± 0.91 | 0.12 | 0.008 | −0.05 | 0.248 | 0.12 | 0.012 | ||||
| (n = 471) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics | Medication Beliefs | |||||||||||
| Necessity | Concerns | Total score | ||||||||||
| B | S.E. | β | p | B | S.E. | β | p | B | S.E. | β | p | |
| Age | 0.08 | 0.02 | 0.23 | <0.001 | −0.05 | 0.02 | −0.14 | 0.005 | 0.15 | 0.02 | 0.28 | <0.001 |
| Male | −1.28 | 0.38 | −0.14 | 0.001 | −1.87 | 0.56 | −0.14 | 0.001 | ||||
| Education level: Primary school and under | −1.17 | 0.44 | −0.13 | 0.008 | ||||||||
| Type D personality | 0.79 | 0.36 | 0.10 | 0.028 | 1.94 | 0.36 | 0.23 | <0.001 | −1.22 | 0.53 | −0.10 | 0.023 |
| State anxiety | −0.04 | 0.02 | −0.12 | 0.005 | 0.05 | 0.02 | 0.14 | 0.001 | −0.09 | 0.02 | −0.1 | <0.001 |
| Diabetes mellitus | −1.29 | 0.38 | −0.14 | 0.001 | ||||||||
| Hyperlipidemia | 1.04 | 0.36 | 0.12 | 0.004 | ||||||||
| Stroke severity according to mRS | 0.34 | 0.15 | 0.10 | 0.021 | −0.32 | 0.14 | −0.10 | 0.026 | 0.72 | 0.21 | 0.14 | 0.001 |
| Number of medications | 0.39 | 0.07 | 0.24 | <0.001 | 0.44 | 0.10 | 0.18 | <0.001 | ||||
| Knowledge about medication | −0.26 | 0.10 | −0.11 | 0.008 | 0.47 | 0.14 | 0.14 | 0.001 | ||||
| R2 (ΔR2) = 0.46 (0.209), adjusted R2 = 0.20, F = 20.20, p < 0.001 | R2 (ΔR2) = 0.48 (0.234), adjusted R2 = 0.22, F = 17.46, p < 0.001 | R2 (ΔR2) = 0.52 (0.268), adjusted R2 = 0.26, F = 24.07, p < 0.001 | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, G.-G.; Yoo, S.-H.; Park, M.-S.; Park, H.-Y.; Cha, J.-K. Factors Related to Beliefs about Medication in Ischemic Stroke Patients. J. Clin. Med. 2022, 11, 3825. https://doi.org/10.3390/jcm11133825
Kim G-G, Yoo S-H, Park M-S, Park H-Y, Cha J-K. Factors Related to Beliefs about Medication in Ischemic Stroke Patients. Journal of Clinical Medicine. 2022; 11(13):3825. https://doi.org/10.3390/jcm11133825
Chicago/Turabian StyleKim, Gye-Gyoung, Sung-Hee Yoo, Man-Seok Park, Hyun-Young Park, and Jae-Kwan Cha. 2022. "Factors Related to Beliefs about Medication in Ischemic Stroke Patients" Journal of Clinical Medicine 11, no. 13: 3825. https://doi.org/10.3390/jcm11133825
APA StyleKim, G.-G., Yoo, S.-H., Park, M.-S., Park, H.-Y., & Cha, J.-K. (2022). Factors Related to Beliefs about Medication in Ischemic Stroke Patients. Journal of Clinical Medicine, 11(13), 3825. https://doi.org/10.3390/jcm11133825