
Itch in Hidradenitis Suppurativa/Acne Inversa: A Systematic Review

 , , ,
, , ,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
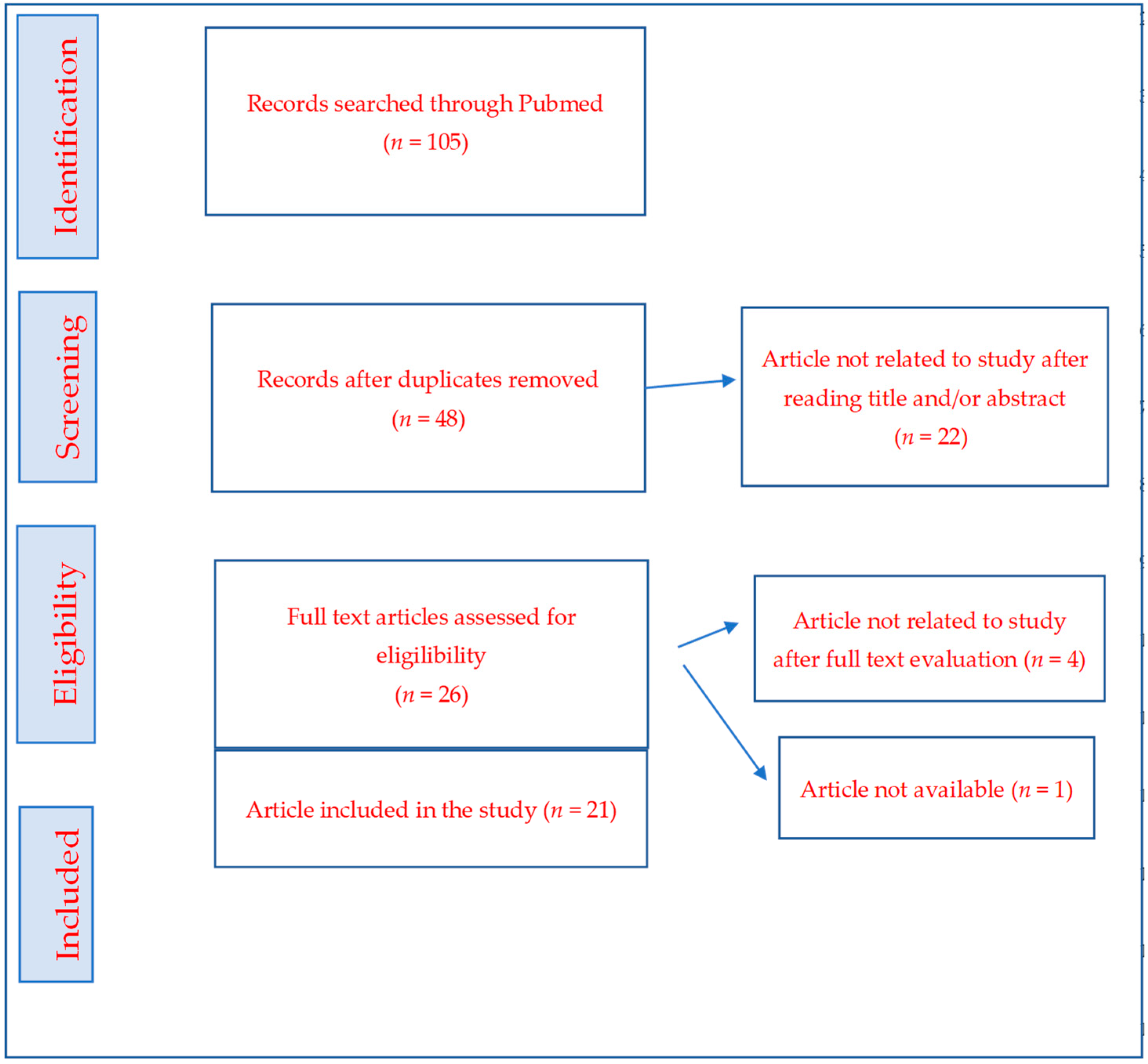
2. Method
3. Epidemiology
4. Etiopathogenesis
5. Clinical Features
6. Treatment
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ralf Paus, L.; Kurzen, H.; Kurokawa, I.; Jemec, G.B.; Emtestam, L.; Sellheyer, K.; Giamarellos-Bourboulis, E.J.; Nagy, I.; Bechara, F.G.; Sartorius, K.; et al. What causes hidradenitis suppurativa? Exp. Dermatol. 2008, 17, 455–472. [Google Scholar] [PubMed]
- Emtestam, L.; Desai, N.; Hunger, R.; Zouboulis, C.C.; Ioannides, D.; Van Der Zee, H.H.; Prens, E.P.; E Jemec, G.B.; Schneider-Burrus, S.; Revuz, J.; et al. European S1 guideline for the treatment of hidradenitis suppurativa/acne inversa. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 619–644. [Google Scholar]
- Nguyen, T.V.; Damiani, G.; Orenstein, L.A.; Hamzavi, I.; Jemec, G.B. Hidradenitis suppurativa: An update on epidemiology, phenotypes, diagnosis, pathogenesis, comorbidities and quality of life. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Chernyshov, P.V.; Zouboulis, C.C.; Tomas-Aragones, L.; Jemec, G.B.; Svensson, A.; Manolache, L.; Tzellos, T.; Sampogna, F.; Pustisek, N.; Van der Zee, H.H.; et al. Quality of life measurement in hidradenitis suppurativa: Position statement of the European Academy of Dermatology and Venereology task forces on Quality of Life and Patient-Oriented Outcomes and Acne, Rosacea and Hidradenitis Suppurativa. J. Eur. Acad. Derm. Venereol. 2019, 33, 1633–1643. [Google Scholar] [CrossRef] [Green Version]
- Yazdanyar, S.; Jemec, G.B.E. Hidradenitis suppurativa: A review of cause and treatment. Curr. Opin. Infect Dis. 2011, 24, 118–123. [Google Scholar] [CrossRef]
- Vinkel, C.; Thomsen, S.F. Hidradenitis Suppurativa: Causes, Features, and Current Treatments. J. Clin. Aesthet. Dermatol. 2018, 11, 17–23. [Google Scholar]
- Krajewski, P.K.; Matusiak, Ł.; von Stebut, E.; Schultheis, M.; Kirschner, U.; Nikolakis, G.; Szepietowski, J.C. Pain in Hidradenitis Suppurativa: A Cross-sectional Study of 1795 Patients. Acta Derm. Venereol. 2021, 101, adv00364. [Google Scholar]
- Napolitano, M.; Megna, M.; Timoshchuk, E.A.; Patruno, C.; Balato, N.; Fabbrocini, G.; Monfrecola, G. Hidradenitis suppurativa: From pathogenesis to diagnosis and treatment. Clin.Cosmet. Investig. Dermatol. 2017, 10, 105–115. [Google Scholar] [CrossRef] [Green Version]
- Fernandez, J.M.; Rizvi, O.H.; Marr, K.D.; Price, K.N.; Hendricks, A.J.; Hsiao, J.L.; Shi, V.Y. Itch and pain by lesion morphology in hidradenitis suppurativa patients. Int. J. Dermatol. 2021, 60, e56–e59. [Google Scholar] [CrossRef]
- Alavi, A.; Hamzavi, I.; Brown, K.; Santos, L.L.; Zhu, Z.; Liu, H.; Howell, M.D.; Kirby, J.S. Janus kinase 1 inhibitor INCB054707 for patients with moderate-to-severe hidradenitis suppurativa: Results from two phase II studies. Br. J. Dermatol. 2022, 186, 803–813. [Google Scholar] [CrossRef]
- Esmann, S.; Jemec, G.B. Psychosocial impact of hidradenitis suppurativa: A qualitative study. Acta Derm. Venereol. 2011, 91, 328–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mac Mahon, J.; Kirthi, S.; Byrne, N.; O’Grady, C.; Tobin, A.M. An update on health-related quality of life and patient-reported outcomes in hidradenitis suppurativa. Patient Relat. Outcome Meas. 2020, 11, 21. [Google Scholar] [CrossRef] [PubMed]
- Pascual, J.C.; Alvarez, P.; Encabo, B.; González, I.; Hispán, P.; Poveda, I.; Romero, D. Comment on: “Assessing Pruritus in Hidradenitis Suppurativa: A Cross-Sectional Study”. Am. J. Clin. Dermatol. 2017, 18, 705–706. [Google Scholar] [CrossRef] [PubMed]
- Molina-Leyva, A.; Cuenca-Barrales, C. Pruritus and Malodour in Patients with Hidradenitis Suppurativa: Impact on Quality of Life and Clinical Features Associated with Symptom Severity. Dermatology 2020, 236, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Kaaz, K.; Szepietowski, J.C.; Matusiak, Ł. Sleep quality among adult patients with chronic dermatoses. Adv. Dermatol. Allergol./Postȩpy Dermatol. I Alergol. 2019, 36, 659. [Google Scholar] [CrossRef] [PubMed]
- List, E.K.; Pascual, J.C.; Zarchi, K.; Nürnberg, B.M.; Jemec, G.B. Mast cells in hidradenitis suppurativa: A clinicopathological study. Arch. Dermatol. Res. 2019, 311, 331–335. [Google Scholar] [CrossRef]
- Posso-De Los Rios, C.J.; Sarfo, A.; Ghias, M.; Alhusayen, R.; Hamzavi, I.; Lowes, M.A.; Alavi, A. Proceeding report of the third symposium on Hidradenitis Suppurativa advances (SHSA) 2018. Exp. Dermatol. 2019, 28, 769–775. [Google Scholar] [CrossRef]
- Nakahigashi, K.; Doi, H. Otsuka e PGD2 induces eotaxin-3 via PPARγ from sebocytes: A possible pathogenesis of eosinophilic pustular folliculitis. J. Allergy Clin. Immunol. 2012, 129, 536–543, Correction in 2014, 133, 604. [Google Scholar] [CrossRef]
- Matusiak, Ł.; Szczęch, J.; Kaaz, K.; Lelonek, E.; Szepietowski, J.C. Clinical Characteristics of Pruritus and Pain in Patients with Hidradenitis Suppurativa. Acta Derm. Venereol. 2018, 98, 191–194. [Google Scholar] [CrossRef] [Green Version]
- Vekic, D.A.; Cains, G.D. Hidradenitis suppurativa, a review of pathogenesis, associations and management. Part 2. Australas. J. Dermatol. 2018, 59, 261–266. [Google Scholar] [CrossRef]
- Kaaz, K.; Szepietowski, J.C.; Matusiak, Ł. Influence of Itch and Pain on Sleep Quality in Patients with Hidradenitis Suppurativa. Acta Derm. Venereol. 2018, 98, 757–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vita, V.; Matusiak, Ł.; Szepietowski, J.C. Comment on: “Assessing Pruritus in Hidradenitis Suppurativa: A Cross-Sectional Study”. Am. J. Clin. Dermatol. 2017, 18, 707–708. [Google Scholar] [CrossRef] [PubMed]
- Ring, H.C.; Theut Riis, P.; Zarchi, K.; Miller, I.M.; Saunte, D.M.; Jemec, G.B. Prodromal symptoms in hidradenitis suppurativa. Clin. Exp. Dermatol. 2017, 42, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Andersen, R.K.; Jemec, G.B.; Saunte, D.M. Umbilical Hidradenitis Suppurativa Symptoms: A Case Series and Review of the Literature. Acta Dermatovenerol. Alp. Pannonica Et Adriat. 2020, 29, 3–6. [Google Scholar]
- Vossen, A.R.J.V.; Schoenmakers, A.; van Straalen, K.R.; Prens, E.P.; Van Der Zee, H.H. Assessing Pruritus in Hidradenitis Suppurativa: A Cross-Sectional Study. Am. J. Clin. Dermatol. 2017, 18, 687–695. [Google Scholar] [CrossRef] [Green Version]
- Riis, P.T.; Vinding, G.R.; Ring, H.C.; Jemec, G.B. Disutility in Patients with Hidradenitis Suppurativa: A Cross-sectional Study Using EuroQoL-5D. Acta Derm. Venereol. 2016, 96, 222–226. [Google Scholar] [CrossRef] [Green Version]
- Horváth, B.; Janse, I.C.; Sibbald, G.R. Pain management in patients with hidradenitis suppurativa. J. Am. Acad. Dermatol. 2015, 73, S47–S51. [Google Scholar] [CrossRef]
- McKenzie, S.A.; Harview, C.L.; Truong, A.K.; Grogan, T.R.; Shi, V.Y.; Bennett, R.G.; Hsiao, J.L. Physical symptoms and psychosocial problems associated with hidradenitis suppurativa: Correlation with Hurley stage. Dermatol. Online J. 2020, 26, 13030. [Google Scholar] [CrossRef]
- Van der Zee, H.; de Ruiter, L.; Boer, J.; Broecke, D.V.D.; Hollander, J.D.; Laman, J.; Prens, E. Alterations in leucocyte subsets and histomorphology in normal-appearing perilesional skin and early and chronic hidradenitis suppurativa lesions. Br. J. Dermatol. 2012, 166, 98–106. [Google Scholar] [CrossRef]
- Monfrecola, G.; Balato, A.; Caiazzo, G.; De Vita, V.; Di Caprio, R.; Donnarumma, M.; Lembo, S.; Fabbrocini, G. Mammalian target of rapamycin, insulin resistance and hidradenitis suppurativa: A possible metabolic loop. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1631–1633. [Google Scholar] [CrossRef] [Green Version]
- Pascual, J.C.; Garcia-Martinez, F.J.; Martorell, A.; González, I.; Hispan, P. Increased total serum IgE levels in moderate-to-severe hidradenitis suppurativa. Br. J. Dermatol. 2016, 175, 1101–1102. [Google Scholar] [CrossRef] [PubMed]
- Schmelz, M. Itch and pain. Neurosci. Biobehav. Rev. 2010, 34, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Obara, I.; Medrano, M.C.; Signoret-Genest, J.; Jiménez-Díaz, L.; Géranton, S.M.; Hunt, S.P. Inhibition of the mammalian target of rapamycin complex 1 signaling pathway reduces itch behaviour in mice. Pain 2015, 156, 1519–1529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vossen, A.R.J.V.; van der Zee, H.H.; Tsoi, L.C.; Xing, X.; Devalaraja, M.; Gudjonsson, J.E.; Prens, E.P. Novel cytokine and chemokine markers of hidradenitis suppurativa reflect chronic inflammation and itch. Allergy 2019, 74, 631–634. [Google Scholar] [CrossRef]
- Wiltz, O.; Schoetz, D.J.; Murray, J.J.; Roberts, P.L.; Coller, J.A.; Veidenheimer, M.C. Perianal hidradenitis suppurativa. Dis. Colon Rectum 1990, 33, 731–734. [Google Scholar] [CrossRef]
- Frew, J.W.; Navrazhina, K.; Grand, D.; Sullivan-Whalen, M.; Gilleaudeau, P.; Garcet, S.; Ungar, J.; Krueger, J.G. The effect of subcutaneous brodalumab on clinical disease activity in hidradenitis suppurativa: An open-label cohort study. J. Am. Acad. Dermatol. 2020, 83, 1341–1348. [Google Scholar] [CrossRef]
- Bordon, Y. JAK in the itch. Nat. Rev. Drug Discov. 2017, 16, 753. [Google Scholar] [CrossRef]
- Verdolini, R.; Clayton, N.; Smith, A.; Alwash, N.; Mannello, B. Metformin for the treatment of hidradenitis suppurativa: A little help along the way. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 1101–1108. [Google Scholar] [CrossRef]
- Arun, B.; Loffeld, A. Long-standing hidradenitis suppurativa treated effectively with metformin. Clin. Exp. Dermatol. 2009, 34, 920–921. [Google Scholar] [CrossRef]
- Clements, A.; Gao, B.; Yeap, S.H.; Wong, M.K.; Ali, S.S.; Gurney, H. Metformin in prostate cancer: Two for the price of one. Ann. Oncol. 2011, 22, 2556–2560. [Google Scholar] [CrossRef]

{kind=link}
| Sr.No | PMID | Name of Article | Primary Findings | Author, Ref. | Journal | Year |
|---|---|---|---|---|---|---|
| 1 | 32662883 | Itch and pain by lesion morphology in hidradenitis suppurativa patients | n = 856 Nearly all (95.2%) participants experienced pain, and 77.5% experienced itch. Pain was more bothersome than itch in 70.7%. Discomfort from HS most commonly interfered with exercise (76.6%). Itch was more prevalent in smokers than nonsmokers (85.7% vs. 72.9%, respectively, p < 0.0001) and in Hurley stages II and III than stage I (9.2%, 47.8% and 43.1% for Hurley stages I, II and III, respectively, p < 0.0001). | Fernandez JM, Rizvi OH, Marr KD, Price KN, Hendricks AJ, Hsiao JL, Shi VY. [9] | Int J Dermatol. 2021 Feb;60(2):e56-e59. doi: 10.1111/ijd.15037. Epub 2020 Jul 14. | 2021 |
| 2 | 32416208 | The effect of subcutaneous brodalumab on clinical disease activity in hidradenitis suppurativa: An open-label cohort study | N = 10 No grade 2/3 adverse events associated with the use of brodalumab were reported. A total of 100% patients achieved HiSCR, and 80% achieved IHS4 category change at Week 12. Significant improvements were seen in pain, itch, quality of life and depression. | Frew JW, Navrazhina K, Grand D, Sullivan-Whalen M, Gilleaudeau P, Garcet S, Ungar J, Krueger JG. [10] | J Am Acad Dermatol. 2020 Nov;83(5):1341-1348. doi: 10.1016/j.jaad.2020.05.007. Epub 2020 May 13. | 2020 |
| 3 | 32206815 | Umbilical hidradenitis suppurativa symptoms: a case series and review of the literature | N = 19 52.6% (10/19) of the HS patients experienced umbilical symptoms in relation to HS flares. 73.7% (14/19) of the patients experienced malodorous or bloody discharge from the umbilicus. 26.3% (5/19) experienced erythema and itching but no discharge. | Kjærsgaard Andersen R, Jemec GBE, Saunte DM. [11] | Acta Dermatovenerol Alp Pannonica Adriat. 2020 Mar;29(1):3-6. | 2020 |
| 4 | 32104123 | An Update on Health-Related Quality of Life and Patient-Reported Outcomes in Hidradenitis Suppurativa | HS patients had higher DQLI scores compared to control population. | Mac Mahon J, Kirthi S, Byrne N, O’Grady C, Tobin AM. [12] | Patient Relat Outcome Meas. 2020 Feb 10;11:21-26. doi: 10.2147/PROM.S174299. eCollection 2020. | 2020 |
| 5 | 33054933 | Physical symptoms and psychosocial problems associated with hidradenitis suppurativa: correlation with Hurley stage | N = 145 Hurley stage III patients had significantly higher mean Dermatology Life Quality Index (DLQI) scores (20.2) compared to patients with Hurley stage I (11.3) and II (13.9), (p < 0.001 and p = 0.001, respectively). >75% of patients reported physical symptoms of drainage, irritation, pain, itching, bleeding and odor. Symptom severity was most strongly correlated with disease severity for odor (correlation coefficient 0.4, p < 0.001), difficulty moving arms (0.323, p < 0.001), negative impact on job/school (0.303, p < 0.001) and negative impact on relationships (0.298, p < 0.001) | McKenzie SA, Harview CL, Truong AK, Grogan TR, Shi VY, Bennett RG, Hsiao JL. [13] | Dermatol Online J. 2020 Sep 15;26(9):13030/qt4rm8w7kn. | 2020 |
| 6 | 31466061 | Pruritus and Malodour in Patients with Hidradenitis Suppurativa: Impact on Quality of Life and Clinical Features Associated with Symptom Severity | N = 233 Both pruritus and malodor positively correlated with worse quality of life (p < 0.05). Pruritus intensity was associated with the number of regions affected by HS, female sex, the intensity of suppuration and the presence of comorbid Crohn’s disease. Statin use was associated with lower levels of pruritus. | Molina-Leyva A, Cuenca-Barrales C. [14] | Dermatology. 2020;236(1):59-65. doi: 10.1159/000502139. Epub 2019 Aug 29. | 2020 |
| 7 | 31997991 | Sleep quality among adult patients with chronic dermatoses | N = 108 HS patients 50 controls, Pittsburgh Sleep Quality Index (PSQI) mean scores assessed as 6.5 ±3.6 points and 3.1 ± 1.9 points, respectively (p< 0.0001). Pain seems to play a crucial role in impairing sleep quality in HS patients. | Kaaz K, Szepietowski JC, Matusiak Ł. [15] | Postepy Dermatol Alergol. 2019 Dec;36(6):659-666. doi: 10.5114/ada.2019.84007. Epub 2019 Apr 9. | 2019 |
| 8 | 30877368 | Mast cells in hidradenitis suppurativa: a clinicopathological study | N = 34 Mast cells (MC) were present to a greater degree in HS-lesions than in perilesional skin (p = 0.004). Disease severity (Sartorius score) was correlated to with MC count and itch when adjusted for sex and age (p = 0.042). A positive correlation between MC count and HS activity was detected, suggesting a potential link between MC and HS. | List EK, Pascual JC, Zarchi K, Nürnberg BM, Jemec GBE. [16] | Arch Dermatol Res. 2019 May;311(4):331-335. doi: 10.1007/s00403-019-01910-3. Epub 2019 Mar 15. | 2019 |
| 9 | 30924968 | Proceeding report of the third symposium on Hidradenitis Suppurativa advances (SHSA) 2018 | Recent studies suggested that pruritus may be an important symptom associated with HS, especially in the prodromal stage. Histopathology reports found an increase in mast cells in all stages of HS (including perilesional skin). The intensity of pruritus correlated positively with impairment of quality of life and has a significant influence on the frequency of insomnia. | Posso-De Los Rios CJ, Sarfo A, Ghias M, Alhusayen R, Hamzavi I, Lowes MA, Alavi A. [17] | Exp Dermatol. 2019 Jul;28(7):769-775. doi: 10.1111/exd.13928. Epub 2019 Apr 29. | 2019 |
| 10 | 30421795 | Novel cytokine and chemokine markers of hidradenitis suppurativa reflect chronic inflammation and itch | CCL-26 is a newly identified inflammatory marker that is upregulated in the circulation of HS patients. IL-16, CCL-4, CXCL-10 and CCL-26 as novel and potentially important players in the pathogenesis of HS. The local and systemic upregulation of CCL-26 in HS patients can be linked to the high pruritus score in HS. | Vossen ARJV, van der Zee HH, Tsoi LC, Xing X, Devalaraja M, Gudjonsson JE, Prens EP. [18] | Allergy. 2019 Mar;74(3):631-634. doi: 10.1111/all.13665. Epub 2018 Dec 10. | 2019 |
| 11 | 28971209 | Clinical Characteristics of Pruritus and Pain in Patients with Hidradenitis Suppurativa | N = 103 A total of 62.1% (64/103) experienced pruritus. Pruritus severity was assessed as 5.0 ± 2.1 points, 5.5 ± 2.3 points and 4.6 ±1.9 points (for VASmax, NRSmax and the 4-item Itch Questionnaire, respectively). (51.2%) of patients with HS reported having moderate pruritus, and more (65.0%) reported mild pain. Pruritus was observed predominantly in the buttocks area (90% of pruritic lesions) and armpits (83% and 87% of pruritic lesions). Pruritus intensity correlated significantly with DLQI (r = 0.45, p = 0.004; r = 0.48, p = 0.002 for VAS and NRS, respectively). | Matusiak Ł, Szczęch J, Kaaz K, Lelonek E, Szepietowski JC. [19] | Acta Derm Venereol. 2018 Feb 7;98(2):191-194. doi: 10.2340/00015555-2815. | 2018 |
| 12 | 29363099 | Hidradenitis suppurativa, a review of pathogenesis, associations and management. Part 2 | - | Vekic DA, Cains GD. [20] | Australas J Dermatol. 2018 Nov;59(4):261-266. doi: 10.1111/ajd.12766. Epub 2018 Jan 23. | 2018 |
| 13 | 29756157 | Influence of Itch and Pain on Sleep Quality in Patients with Hidradenitis Suppurativa | N = 103 Controls = 50 A total of 61% (66/108) experienced itch symptoms. Itch intensity was assessed as 4.1 ± 2.9 and 5.0 ± 2.1 points (for VASmean and VASmax, respectively). No statistically significant differences were found in Athens Insomnia Scale (AIS) scores for patients with HS and controls. The mean scores for Pittsburgh Sleep Quality Index (PSQI) were 6.5 ± 3.6 points (range 0–18) and 3.1 ± 1.9 points (range 0–7) for patients with HS and control subjects, respectively (p < 0.0001). HS do not have significantly more frequent insomnia (AIS) but do have significantly more sleep disturbances (PSQI) than controls. | Kaaz K, Szepietowski JC, Matusiak Ł. [21] | Acta Derm Venereol. 2018 Aug 29;98(8):757-761. doi: 10.2340/00015555-2967. | 2018 |
| 14 | 28755065 | Comment on: “Assessing Pruritus in Hidradenitis Suppurativa: A Cross-Sectional Study” | mTOR has been found to be increased in the lesional as well as non-lesional skin of HS patients. Moreover, mTOR gene expression statistically correlates with the severity of HS. Such altered mTOR signalling might contribute to explain itch in HS patients, since it has been shown that the mTORC1 pathway plays an important role in itch signalling. If proven oral metformin and other drugs inhibiting mTOR could be used to effectively treat HS associated itch. | De Vita V, Matusiak Ł, Szepietowski JC. [22] | Am J Clin Dermatol. 2017 Oct;18(5):707-708. doi: 10.1007/s40257-017-0314-9. | 2017 |
| 15 | 28597178 | Comment on: “Assessing Pruritus in Hidradenitis Suppurativa: A Cross-Sectional Study” | n = 191 The prevalence (NRS score C3) of pruritus was 58.6% (112/191), with a mean pruritus NRS score of 6.2 (±2.3) in this subgroup. The mean intensity of itch in all 191 patients was rated at an NRS score of 3.9 (±3.3). There was significant association with active smoking (OR 1.1–3.8; p = 0.02) but not with Hurley stage or number of inflamed areas, both of which had an association with pruritus in the cohort of Vossen et al. | Pascual JC, Alvarez P, Encabo B, González I, Hispán P, Poveda I, Romero D. [23] | Am J Clin Dermatol. 2017 Oct;18(5):705-706. doi: 10.1007/s40257-017-0304-y. | 2017 |
| 16 | 28194809 | Prodromal symptoms in hidradenitis suppurativa | N = 72 A total of (83.3%; n = 60) confirmed that they experienced one or more symptom(s) prior to the development of inflamed nodules or abscesses. These included: fatigue (32%), malaise (defined as a fever-like sensation) (23%), headache (11%) and nausea (2%). Localized symptoms included skin erythema (75%), paraesthesia (63%) and itching (20%). Prodromes usually occurred > 24 h (45%) or 12-24 h (20%) before the eruption. | Ring HC, Theut Riis P, Zarchi K, Miller IM, Saunte DM, Jemec GB. [24] | Clin Exp Dermatol. 2017 Apr;42(3):261-265. doi: 10.1111/ced.13025. Epub 2017 Feb 14. | 2017 |
| 17 | 28429245 | Assessing Pruritus in Hidradenitis Suppurativa: A Cross-Sectional Study | N = 211 Mean NRS score of 6.1 ± 2.0. Patients with a pruritus NRS score ≥ 3 had more HS-affected body sites than patients with a score < 3 (p < 0.001). NRS score ≥ 3 was associated with Hurley III disease (odds ratio [OR] 7.73; p = 0.003) and pain (OR 1.34; p < 0.001). Pruritus affected sleep and activities of daily living (ADL) in the majority of cases, with an associated modified 5-D itch score of 13.7 ± 3.6 (on a scale from 5 to 25) in 52 HS patients. | Vossen ARJV, Schoenmakers A, van Straalen KR, Prens EP, van der Zee HH. [25] | Am J Clin Dermatol. 2017 Oct;18(5):687-695. doi: 10.1007/s40257-017-0280-2. | 2017 |
| 18 | 25940640 | Disutility in Patients with Hidradenitis Suppurativa: A Cross-sectional Study Using EuroQoL-5D | N = 421 A significantly decreased utility in patients with hidradenitis suppurativa was found for all age group levels, except for 65-74-year-olds. The total index score in the cohort was 0.705 (population mean 0.887), and the VAS was 62.25 (population mean 82.6). Multivariate analysis found significant associations between loss of utility and pain, malodor and pruritus (p < 0.0001). Patients with hidradenitis suppurativa had a significantly decreased EuroQoL-5D (EQ-5D) compared with the background population. | Riis PT, Vinding GR, Ring HC, Jemec GB. [26] | Acta Derm Venereol. 2016 Feb;96(2):222-6. doi: 10.2340/00015555-2129. | 2016 |
| 19 | 21394419 | Psychosocial impact of hidradenitis suppurativa: a qualitative study | N = 12 HS has a great emotional impact on patients and promotes isolation due to fear of stigmatization. Shame and irritation are frequent and relate to smell, scars, itching and pain. Quality of life is adversely affected, and professional support is needed. | Esmann S, Jemec GB. [27] | Acta Derm Venereol. 2011 May;91(3):328-32. doi: 10.2340/00015555-1082. | 2011 |
| 20 | 2390907 | Perianal hidradenitis suppurativa. The Lahey Clinic experience | N = 43 Symptoms, including pain, swelling, purulent discharge and pruritus, had been present for a median of six years. Associated medical conditions included diabetes (12%) and obesity (12%), and 70 percent of patients were smokers. Once the correct diagnosis was established, 72% of patients had wide local excision with healing by secondary intention, and 28% of patients had incision and drainage or limited local excision. Although 67% of the patients had recurrence of disease after initial treatment, wide excision was more successful in preventing recurrence. | Wiltz O, Schoetz DJ Jr, Murray JJ, Roberts PL, Coller JA, Veidenheimer MC. [28] | Dis Colon Rectum. 1990 Sep;33(9):731-4. doi: 10.1007/BF02052316. | 1990 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agarwal, P.; Lunge, S.B.; Shetty, N.S.; Karagaiah, P.; Daveluy, S.; Ortega-Loayza, A.G.; Tzellos, T.; Szepietowski, J.C.; Zouboulis, C.C.; Grabbe, S.; et al. Itch in Hidradenitis Suppurativa/Acne Inversa: A Systematic Review. J. Clin. Med. 2022, 11, 3813. https://doi.org/10.3390/jcm11133813
Agarwal P, Lunge SB, Shetty NS, Karagaiah P, Daveluy S, Ortega-Loayza AG, Tzellos T, Szepietowski JC, Zouboulis CC, Grabbe S, et al. Itch in Hidradenitis Suppurativa/Acne Inversa: A Systematic Review. Journal of Clinical Medicine. 2022; 11(13):3813. https://doi.org/10.3390/jcm11133813
Chicago/Turabian StyleAgarwal, Puneet, Snehal Balvant Lunge, Nandini Sundar Shetty, Priyanka Karagaiah, Steven Daveluy, Alex G. Ortega-Loayza, Thrasyvoulos Tzellos, Jacek C. Szepietowski, Christos C. Zouboulis, Stephan Grabbe, and et al. 2022. "Itch in Hidradenitis Suppurativa/Acne Inversa: A Systematic Review" Journal of Clinical Medicine 11, no. 13: 3813. https://doi.org/10.3390/jcm11133813
APA StyleAgarwal, P., Lunge, S. B., Shetty, N. S., Karagaiah, P., Daveluy, S., Ortega-Loayza, A. G., Tzellos, T., Szepietowski, J. C., Zouboulis, C. C., Grabbe, S., & Goldust, M. (2022). Itch in Hidradenitis Suppurativa/Acne Inversa: A Systematic Review. Journal of Clinical Medicine, 11(13), 3813. https://doi.org/10.3390/jcm11133813