
A Systematic Review and Meta-Analysis on Metabolic Bone Disease in Patients with Primary Sclerosing Cholangitis

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
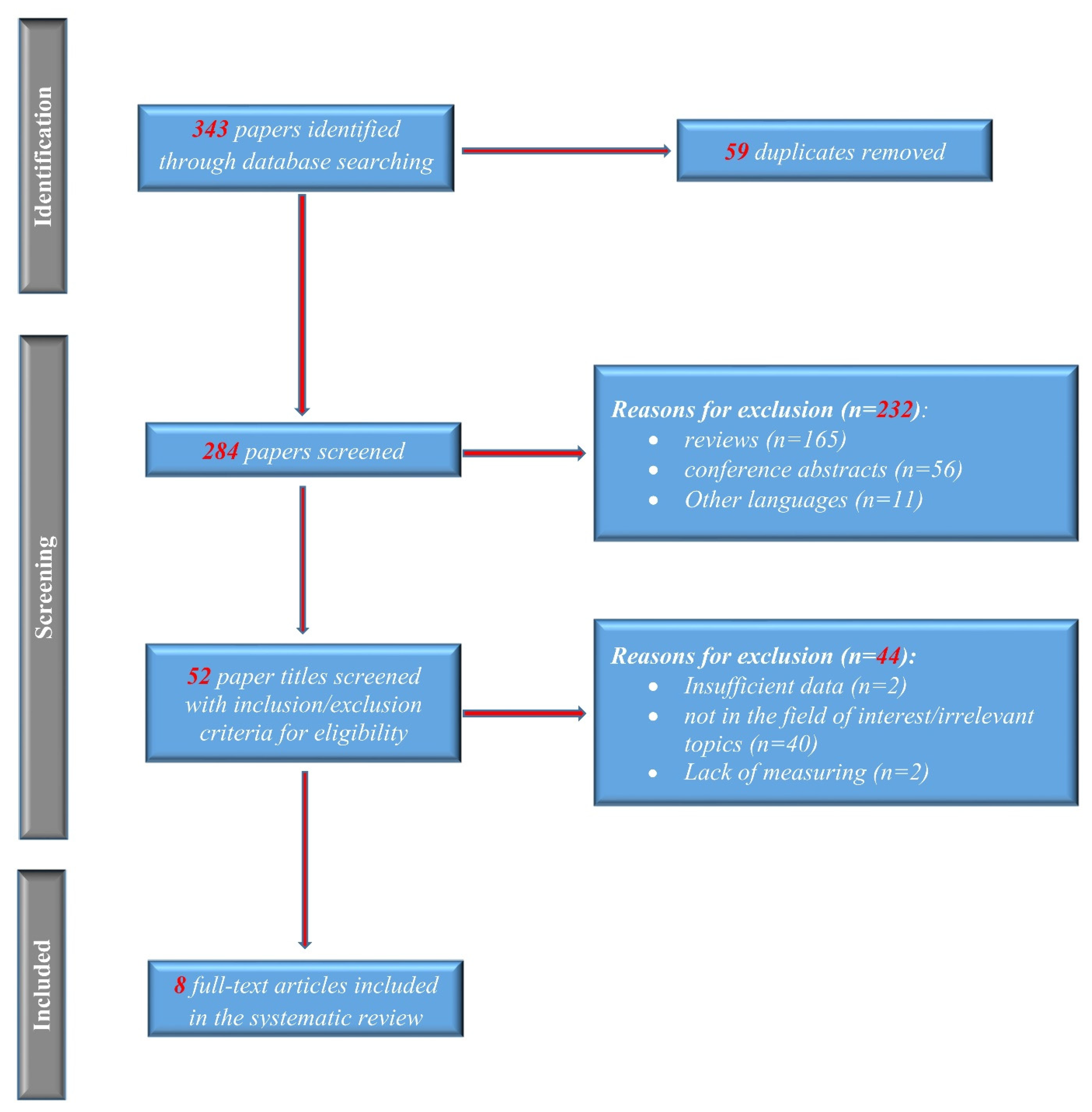
3.1. Study Selection and Characteristics of Included Studies
3.2. Lumbar Spine BMD
3.2.1. PSC vs. Healthy
3.2.2. PSC vs. PBC
3.3. Lumbar Spine T-Score
3.4. Lumbar Spine Z-Score
3.5. Hip BMD
3.5.1. Vitamin D PSC vs. Healthy
3.5.2. Calcium PSC vs. Healthy
3.5.3. Bilirubin PSC vs. Healthy
3.5.4. Alkaline Phosphatase PSC vs. Healthy
3.6. Prevalence of Fractures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hirschfield, G.M.; Karlsen, T.H.; Lindor, K.D.; Adams, D.H. Primary sclerosing cholangitis. Lancet 2013, 382, 1587–1599. [Google Scholar] [CrossRef]
- Talwalkar, J.A.; Lindor, K.D. Primary sclerosing cholangitis. Inflamm. Bowel Dis. 2005, 11, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Rouillard, S.; Lane, N.E. Hepatic osteodystrophy. Hepatology 2001, 33, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Angulo, P.; Peter, J.B.; Gershwin, M.; DeSotel, C.K.; Shoenfeld, Y.; Ahmed, A.E.; Lindor, K.D. Serum autoantibodies in patients with primary sclerosing cholangitis. J. Hepatol. 2000, 32, 182–187. [Google Scholar] [CrossRef]
- Hov, J.R.; Boberg, K.M.; Karlsen, T.H. Autoantibodies in primary sclerosing cholangitis. World J. Gastroenterol. 2008, 14, 3781–3791. [Google Scholar] [CrossRef]
- Connolly, M.P.; Melodi, K.K. Projection of liver transplant activity per indication in France and United Kingdom. J. Hepatol. 2020, 73, S123–S400. [Google Scholar] [CrossRef]
- Yadlapati, S.; Judge, T.A. Risk of hepatobiliary-gastrointestinal malignancies and appropriate cancer surveillance in patients with primary sclerosing cholangitis. Cureus 2021, 13, e19922. [Google Scholar] [CrossRef]
- Ghosh, S.; Cowen, S.; Hannan, W.J.; Ferguson, A. Low bone mineral density in Crohn’s disease, but not in ulcerative colitis, at diagnosis. Gastroenterology 1994, 107, 1031–1039. [Google Scholar] [CrossRef]
- Lopez-Larramona, G.; Lucendo, A.J.; Gonzalez-Castillo, S.; Tenias, J.M. Hepatic osteodystrophy: An important matter for consideration in chronic liver disease. World J. Hepatol. 2011, 3, 300–307. [Google Scholar] [CrossRef]
- Lupoli, R.; Di Minno, A.; Spadarella, G.; Ambrosino, P.; Panico, A.; Tarantino, L.; Lupoli, G.; Lupoli, G.; Di Minno, M.N.D. The risk of osteoporosis in patients with liver cirrhosis: A meta-analysis of literature studies. Clin. Endocrinol. 2016, 84, 30–38. [Google Scholar] [CrossRef]
- Karoli, Y.; Karoli, R.; Fatima, J.; Manhar, M. Study of Hepatic Osteodystrophy in Patients with Chronic Liver Disease. J. Clin. Diagn. Res. 2016, 10, OC31–OC34. [Google Scholar] [CrossRef] [PubMed]
- Ranjan, R.; Rampal, S.; Jaiman, A.; Tokgöz, M.A.; Koong, J.K.; Ramayah, K.; Rajaram, R. Common musculoskeletal disorders in chronic liver disease patients. Jt. Dis. Relat. Surg. 2021, 32, 818–823. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, P.; Krogh, K.; Rejnmark, L.; Laurberg, S.; Mosekilde, L. Fracture risk is increased in Crohn’s disease, but not in ulcerative colitis. Gut 2000, 46, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Seki, A.; Ikeda, F.; Miyatake, H.; Takaguchi, K.; Hayashi, S.; Osawa, T.; Fujioka, S.; Tanaka, R.; Ando, M.; Seki, H.; et al. Risk of secondary osteoporosis due to lobular cholestasis in non-cirrhotic primary biliary cholangitis. J. Gastroenterol. Hepatol. 2017, 32, 1611–1616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wariaghli, G.; Allali, F.; El Maghraoui, A.; Hajjaj-Hassouni, N. Osteoporosis in patients with primary biliary cirrhosis. Eur. J. Gastroenterol. Hepatol. 2010, 22, 1397–1401. [Google Scholar] [CrossRef] [PubMed]
- Guañabens, N.; Parés, A.; Ros, I.; Caballería, L.; Pons, F.; Vidal, S.; Monegal, A.; Peris, P.; Rode, J. Severity of cholestasis and advanced histological stage but not menopausal status are the major risk factors for osteoporosis in primary biliary cirrhosis. J. Hepatol. 2005, 42, 573–577. [Google Scholar] [CrossRef]
- Wariaghli, G.; Mounach, A.; Achemlal, L.; Benbaghdadi, I.; Aouragh, A.; Bezza, A.; El Maghraoui, A. Osteoporosis in chronic liver disease: A case-control study. Rheumatol. Int. 2010, 30, 893–899. [Google Scholar] [CrossRef]
- Campbell, M.S.; Lichtenstein, G.R.; Rhim, A.D.; Pazianas, M.; Faust, T. Severity of liver disease does not predict osteopenia or low bone mineral density in primary sclerosing cholangitis. Liver Int. 2005, 25, 311–316. [Google Scholar] [CrossRef]
- Angulo, P.; Grandison, G.A.; Fong, D.G.; Keach, J.C.; Lindor, K.D.; Bjornsson, E.; Koch, A. Bone disease in patients with primary sclerosing cholangitis. Gastroenterology 2011, 140, 180–188. [Google Scholar] [CrossRef] [Green Version]
- Compston, J.E.; McClung, M.R.; Leslie, W.D. Osteoporosis. Lancet 2019, 393, 364–376. [Google Scholar] [CrossRef]
- Tu, K.N.; Lie, J.D.; Wan, C.K.V.; Cameron, M.; Austel, A.G.; Nguyen, J.K.; Van, K.; Hyun, D. Osteoporosis: A review of treatment options. Pharm. Ther. 2018, 43, 92–104. [Google Scholar]
- Eastell, R.; Rosen, C.J.; Black, D.M.; Cheung, A.M.; Murad, M.H.; Shoback, D. Pharmacological management of osteoporosis in postmenopausal women: An endocrine society* clinical practice guideline. J. Clin. Endocrinol. Metab. 2019, 104, 1595–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danford, C.J.; Trivedi, H.D.; Bonder, A. Bone health in patients with liver diseases. J. Clin. Densitom. 2020, 23, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwel, P. The Newcastle Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses; 2011. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 21 January 2022).
- McPheeters, M.L.; Kripalani, S.; Peterson, N.B.; Idowu, R.T.; Jerome, R.N.; Potter, S.A.; Andrews, J.C. Closing the quality gap: Revisiting the state of the science (vol. 3: Quality improvement interventions to address health disparities). Evid. Rep. Technol. Assess 2012, 208.3, 1–475. [Google Scholar]
- Viechtbauer, W. Conducting Meta-Analyses in R with the Metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Lacher, D.A.; Hughes, J.P.; Carroll, M.D. Biological variation of laboratory analytes based on the 1999-2002 National Health and Nutrition Examination Survey. Natl. Health Stat. Rep. 2010, 21, 1–7. [Google Scholar]
- Angulo, P.; Therneau, T.M.; Jorgensen, R.A.; DeSotel, C.K.; Egan, K.S.; Dickson, E.R.; Hay, J.E.; Lindor, K.D. Bone disease in patients with primary sclerosing cholangitis: Prevalence, severity and prediction of progression. J. Hepatol. 1998, 29, 729–735. [Google Scholar] [CrossRef]
- Guichelaar, M.M.J.; Kendall, R.; Malinchoc, M.; Hay, J.E. Bone mineral density before and after OLT: Long-term follow-up and predictive factors. Liver. Transplant. 2006, 12, 1390–1402. [Google Scholar] [CrossRef]
- Hay, J.E.; Lindor, K.D.; Wiesner, R.H.; Dickson, E.R.; Krom, R.A.; LaRusso, N.F. The metabolic bone disease of primary sclerosing cholangitis. Hepatology 1991, 14, 257–261. [Google Scholar] [CrossRef]
- Keller, S.; Ittrich, H.; Schramm, C.; Lohse, A.W.; Amling, M.; Adam, G.; Yamamura, J. Diffusion-weighted MRI for detection of hepatic osteodystrophy in primary sclerosing cholangitis: A comparison study with dual-energy X-ray absorptiometry. Jpn. J. Radiol. 2016, 34, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, T.; Schwinge, D.; Rolvien, T.; Jeschke, A.; Schmidt, C.; Neven, M.; Butscheidt, S.; Kriz, M.; Kunzmann, L.; Mussawy, H.; et al. Th17 cell frequency is associated with low bone mass in primary sclerosing cholangitis. J. Hepatol. 2019, 70, 941–953. [Google Scholar] [CrossRef] [PubMed]
- Raszeja-Wyszomirska, J.; Kucharski, R.; Zygmunt, M.; Safranow, K.; Miazgowski, T. The impact of fragility fractures on health-related quality of life in patients with primary sclerosing cholangitis. Hepat. Mon. 2015, 15, e25539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The National Institutes of Health (NIH) Consensus Development Program: Osteoporosis Prevention, Diagnosis, and Therapy. Available online: https://consensus.nih.gov/2000/2000osteoporosis111html.htm (accessed on 21 January 2022).
- George, J.; Ganesh, H.K.; Acharya, S.; Bandgar, T.R.; Shivane, V.; Karvat, A.; Bhatia, S.J.; Shah, S.; Menon, P.S.; Shah, N. Bone mineral density and disorders of mineral metabolism in chronic liver disease. World J. Gastroenterol. 2009, 15, 3516–3522. [Google Scholar] [CrossRef]
- Chapman, R.; Fevery, J.; Kalloo, A.; Nagorney, D.M.; Boberg, K.M.; Shneider, B.; Gores, G.J. American Association for the Study of Liver Diseases. Diagnosis and management of primary sclerosing cholangitis. Hepatology 2010, 51, 660–678. [Google Scholar] [CrossRef]
- Janes, C.H.; Dickson, E.R.; Okazaki, R.; Bonde, S.; McDonagh, A.F.; Riggs, B.L. Role of hyperbilirubinemia in the impairment of osteoblast proliferation associated with cholestatic jaundice. J. Clin. Investig. 1995, 95, 2581–2586. [Google Scholar] [CrossRef] [Green Version]
- Gasser, R.W. Cholestasis and metabolic bone disease—A clinical review. Wien. Med. Wochenschr. 2008, 158, 553–557. [Google Scholar] [CrossRef]
- Gatta, A.; Verardo, A.; Di Pascoli, M.; Giannini, S.; Bolognesi, M. Hepatic osteodystrophy. Clin. Cases Miner. Bone Metab. 2014, 11, 185–191. [Google Scholar] [CrossRef]
- Steinberg, K.K.; Bonkovsky, H.L.; Caudill, S.P.; Bernhardt, R.K.; Hawkins, M. Osteocalcin and bone alkaline phosphatase in the serum of women with liver disease. Ann. Clin. Lab. Sci. 1991, 21, 305–314. [Google Scholar]
- Porayko, M.K.; Wiesner, R.H.; Hay, J.E.; Krom, R.A.; Dickson, E.R.; Beaver, S.; Schwerman, L. Bone disease in liver transplant recipients: Incidence, timing, and risk factors. Transplant. Proc. 1991, 23, 1462–1465. [Google Scholar]
- Eastell, R.; Dickson, E.R.; Hodgson, S.F.; Wiesner, R.H.; Porayko, M.K.; Wahner, H.W.; Cedel, S.L.; Riggs, B.L.; Krom, A.F. Rates of vertebral bone loss before and after liver transplantation in women with primary biliary cirrhosis. Hepatology 1991, 14, 296–300. [Google Scholar] [CrossRef] [PubMed]
- de Vries, E.M.G.; Wang, J.; Leeflang, M.M.G.; Boonstra, K.; Weersma, R.K.; Beuers, U.H.; Geskus, S.B.; Ponsioen, C.Y. Alkaline phosphatase at diagnosis of primary sclerosing cholangitis and 1 year later: Evaluation of prognostic value. Liver Int. 2016, 36, 1867–1875. [Google Scholar] [CrossRef] [PubMed]
- Chapman, M.H.; Thorburn, D.; Hirschfield, G.M.; Webster, G.G.J.; Rushbrook, S.M.; Alexander, G.; Collier, J.; Dyson, J.K.; Jones, D.E.; Patanwala, I.; et al. British Society of Gastroenterology and UK-PSC guidelines for the diagnosis and management of primary sclerosing cholangitis. Gut 2019, 68, 1356–1378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68, s1–s106. [Google Scholar] [CrossRef] [PubMed] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Country | Study Type | Gender Male/Female PSC, Control | Age (Mean), Years PSC, Control | Mean Duration of Disease (Months) | Severity of Disease | Treatment | Quality Assessments (NOS) | Number of PSC Patients/Controls | Outcomes | Osteodensitometry Machine Used | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PSC Mayo Risk Score | MELD PSC, Control | |||||||||||
| Angulo P et al., 1998 [29] | USA | Clinical study | 44/37/NA | 42.9 ± 11.5 | 31 ± 34, NA | 2.9 ± 1.2 | NA | NA | 8 | 81/81 | Prevalence of osteoporosis, lumbar spine BMD | Hologic |
| Angulo P et al., 2011 [19] | USA | Cohort study | 42%/58%, NA | 45.5 ± 0.8, 45.5 ± 0.8 | 63.4 ± 4.6, NA | 1.19 ± 0.09 | NA | Budesonide, biphosphonates (Cumulative prednisone dose) | 9 | 237/237 | Prevalence of fractures, osteoporosis, lumbar spine BMD and T-score, hip BMD and T-score | Hologic |
| Campbell MS et al., 2005 [18] | USA | Clinical study | 25/5, NA | 46.9 ± 13.4, 46.9 ±13.4 | NA | 1.52 ± 1.07 | 10.5 ± 4.5 | Biphosphonates, steroids (no doses mentioned), calcium, vitamin D, ursodeoxycholic acid | 8 | 30/30 | Lumbar spine BMD | Lunar and Norland |
| Guichelaar MMJ et al., 2006 [30] | USA | Cohort study | 142/ 218 | 46.8 ± 11.0/53.2 ± 8.6 | 85.2 ± 63.6 /94.8 ± 63.6 | NA | 17.0 ± 8.7/17.6 ± 8.8 | Glucocorticoids (prednisone 10 mg per day), biphosphonates, ursodeoxycholic acid | 9 | 204/156 | Prevalence of fractures and osteoporosis, lumbar spine BMD and T-score | Hologic |
| Hay JE et al., 1991 [31] | USA | Clinical study | 19/11, 13/5 | 39.4 ± 0.3, 42.7 ± 0.7 | 91.44, NA | NA | NA | NA | 8 | 30/18 | Prevalence of osteopenia, lumbar spine BMD | - |
| Keller S et al., 2016 [32] | Germany | Clinical study | 20/20, NA | 50 ± 12.6, 49.5 ± 13.0 | 102 ± 98.4, NA | NA | NA | Ursodeoxycholic acid, prednisolone (10 mg per day) | 8 | 40/10 | Prevalence of osteoporosis, lumbar spine BMD and T- score | GE Lunar |
| Schmidt T et al., 2019 [33] | Germany | Cohort study | 136/ 102, 132/ 210 | 47.1 ±13.8 | 79.1 ± 75.4/71.9 ± 62.7 | NA | NA | Glucocorticoids, biphosphonates, ursodeoxycholic acid, Prednisolone (no doses mentioned) | 8 | 238/242 | Prevalence of fractures, osteoporosis, lumbar spine BMD and the femoral neck | GE Lunar |
| Wyszomirska JR et al., 2015 [34] | Poland | Clinical study | 22/11, NA | 35.3 ± 13.38 | 40.56 ± 24.2 | NA | NA | NA | 8 | 33/33 | Prevalence of fractures | Hologic |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ionele, C.M.; Turcu-Stiolica, A.; Subtirelu, M.S.; Ungureanu, B.S.; Cioroianu, G.O.; Rogoveanu, I. A Systematic Review and Meta-Analysis on Metabolic Bone Disease in Patients with Primary Sclerosing Cholangitis. J. Clin. Med. 2022, 11, 3807. https://doi.org/10.3390/jcm11133807
Ionele CM, Turcu-Stiolica A, Subtirelu MS, Ungureanu BS, Cioroianu GO, Rogoveanu I. A Systematic Review and Meta-Analysis on Metabolic Bone Disease in Patients with Primary Sclerosing Cholangitis. Journal of Clinical Medicine. 2022; 11(13):3807. https://doi.org/10.3390/jcm11133807
Chicago/Turabian StyleIonele, Claudiu Marinel, Adina Turcu-Stiolica, Mihaela Simona Subtirelu, Bogdan Silviu Ungureanu, George Ovidiu Cioroianu, and Ion Rogoveanu. 2022. "A Systematic Review and Meta-Analysis on Metabolic Bone Disease in Patients with Primary Sclerosing Cholangitis" Journal of Clinical Medicine 11, no. 13: 3807. https://doi.org/10.3390/jcm11133807
APA StyleIonele, C. M., Turcu-Stiolica, A., Subtirelu, M. S., Ungureanu, B. S., Cioroianu, G. O., & Rogoveanu, I. (2022). A Systematic Review and Meta-Analysis on Metabolic Bone Disease in Patients with Primary Sclerosing Cholangitis. Journal of Clinical Medicine, 11(13), 3807. https://doi.org/10.3390/jcm11133807