
Chronic Pelvic Pain in Endometriosis: Cross-Sectional Associations with Mental Disorders, Sexual Dysfunctions and Childhood Maltreatment



Abstract
:1. Introduction
2. Materials and Methods
Statistical Analyses
3. Results
3.1. Demographic, Clinical and Endometriosis-Related Data
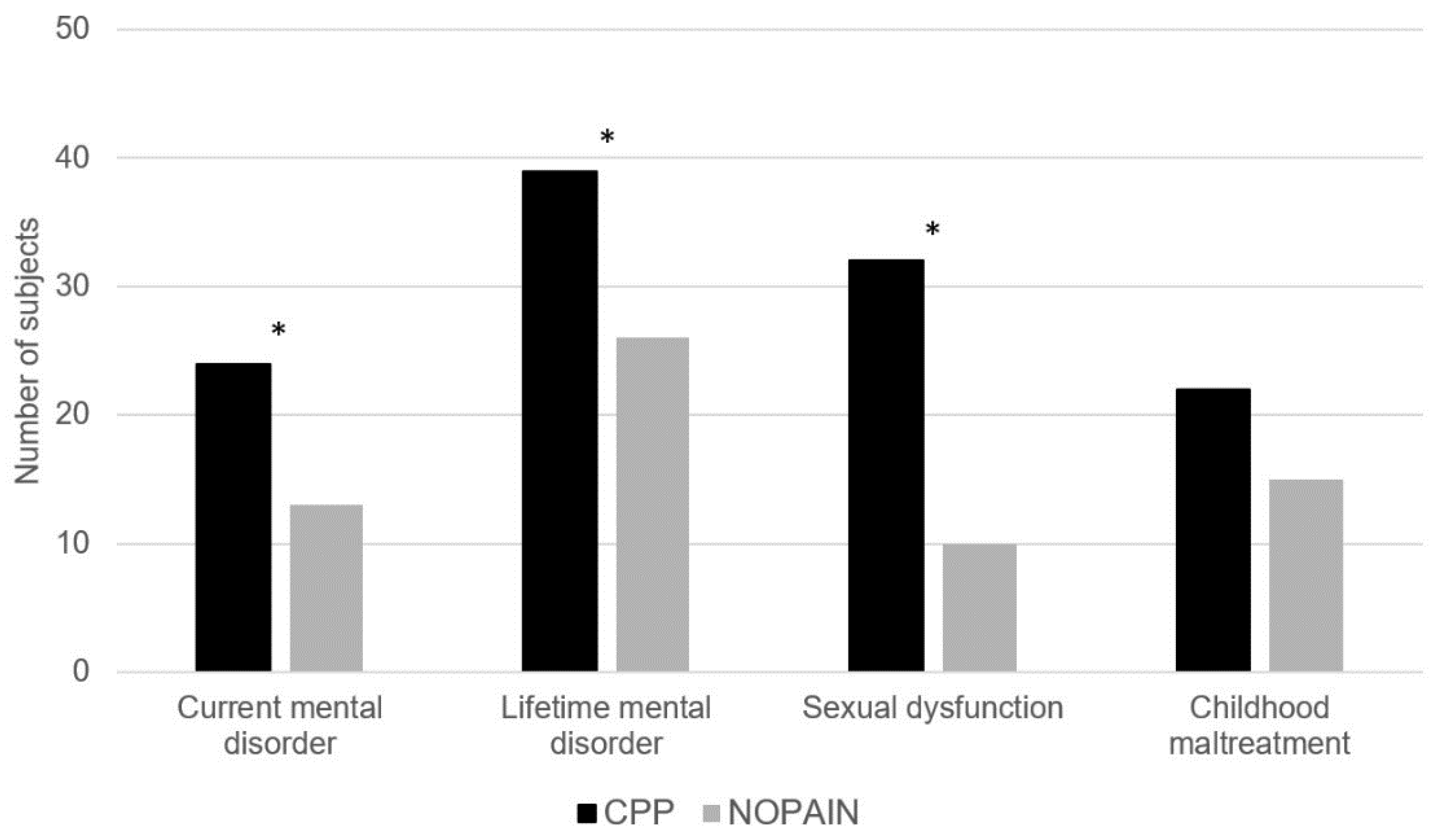
3.2. Mental Disorders, Sexual Dysfunctions and Childhood Maltreatment
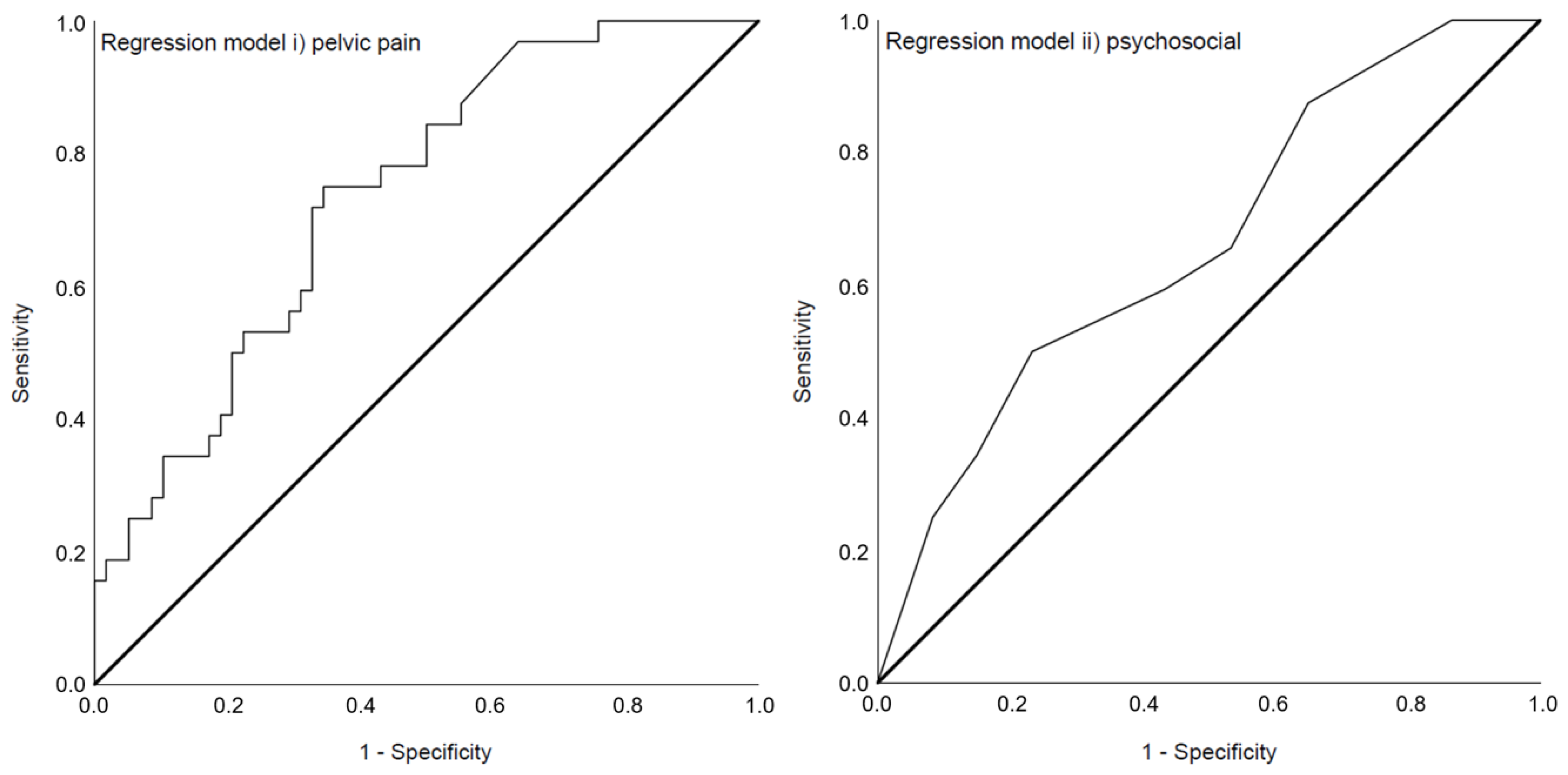
3.3. Prediction Models of a Current Mental Disorder
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B

{kind=link}
{kind=link}
| Variable | Variable | ||
|---|---|---|---|
| Model i) pelvic pain | Pelvic pain days per month | PC_intensity 1 | PC_painrelief 2 |
| Pelvic pain days per month | 1.00 | 0.864 ** | 0.762 ** |
| PC_intensity 1 | 0.864 ** | 1.00 | 0.900 ** |
| PC_painrelief 2 | 0.762 ** | 0.900 ** | 1.00 |
| Model ii) psychosocial | Childhood maltreatment CM 3 | Former mental disorder | Any sexual dysfunction |
| Childhood maltreatment CM 3 | 1.00 | 0.057 | −0.013 |
| Former mental disorder | 0.057 | 1.00 | 0.030 |
| Any sexual dysfunction | −0.013 | 0.030 | 1.00 |
| Collinearity Statistics | ||
|---|---|---|
| Variable | Tolerance | VIF |
| Model i) pelvic pain | ||
| Pelvic pain days per month | 0.247 | 4.048 |
| PC_intensity 1 | 0.134 | 7.457 |
| PC_painrelief 2 | 0.194 | 5.148 |
| Model ii) psychosocial | ||
| Childhood maltreatment CM 3 | 0.997 | 1.003 |
| Former mental disorder | 0.997 | 1.003 |
| Any sexual dysfunction | 1.00 | 1.00 |
References
- Bulun, S.E. Endometriosis. In Yen & Jaffe’s Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management; Elsevier, Inc.: Amsterdam, The Netherlands, 2018; pp. 609–642. [Google Scholar]
- Mechsner, S. Endometriose. Schmerz 2016, 30, 477–490. [Google Scholar] [CrossRef]
- Laganà, A.S.; Condemi, I.; Retto, G.; Muscatello, M.R.A.; Bruno, A.; Zoccali, R.A.; Triolo, O.; Cedro, C. Analysis of psychopathological comorbidity behind the common symptoms and signs of endometriosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 194, 30–33. [Google Scholar] [CrossRef]
- Sepulcri, R.d.P.; do Amaral, V.F. Depressive symptoms, anxiety, and quality of life in women with pelvic endometriosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2009, 142, 53–56. [Google Scholar] [CrossRef]
- Lewis, D.O.; Comite, F.; Mallouh, C.; Zadunaisky, L.; Hutchinson-Williams, K.; Cherksey, B.D.; Yeager, C. Bipolar mood disorder and endometriosis: Preliminary findings. Am. J. Psychiatry 1987, 144, 1588–1591. [Google Scholar]
- Walker, E.; Katon, W.; Jones, L.M.; Russo, J. Relationship between endometriosis and affective disorder. Am. J. Psychiatry 1989, 146, 380–381. [Google Scholar]
- Kumar, V.; Khan, M.; Vilos, G.A.; Sharma, V. Revisiting the association between endometriosis and bipolar disorder. J. Obs. Gynaecol. Can. 2011, 33, 1141–1145. [Google Scholar] [CrossRef]
- Cavaggioni, G.; Lia, C.; Resta, S.; Antonielli, T.; Panici, P.B.; Megiorni, F.; Porpora, M.G. Are mood and anxiety disorders and alexithymia associated with endometriosis? A preliminary study. Biomed. Res. Int. 2014, 2014, 786830. [Google Scholar] [CrossRef]
- Rief, W.; Stenzel, N. Diagnostik Und Klassifikation. In Klinische Psychologie und Psychotherapie für Bachelor—Band I: Grundlagen und Störungswissen; Berking, M., Rief, W., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 9–19. [Google Scholar]
- Gambadauro, P.; Carli, V.; Hadlaczky, G. Depressive symptoms among women with endometriosis: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2019, 220, 230–241. [Google Scholar] [CrossRef]
- van Barneveld, E.; Manders, J.; van Osch, F.; van Poll, M.; Visser, L.; Hanegem, L.; Lim, A.; Bongers, M.; Leue, C. Depression, anxiety and correlating factors in endometriosis: A systematic review and meta-analysis. J. Womens Health 2021, 31, 219–230. [Google Scholar] [CrossRef]
- de Graaff, A.A.; van Lankveld, J.; Smits, L.J.; van Beek, J.J.; Dunselman, G.A.J. Dyspareunia and depressive symptoms are associated with impaired sexual functioning in women with endometriosis, whereas sexual functioning in their male partners is not affected. Hum. Reprod. 2016, 31, 2577–2586. [Google Scholar] [CrossRef] [Green Version]
- Jia, S.; Leng, J.; Sun, P.; Lang, J. Prevalence and associated factors of female sexual dysfunction in women with endometriosis. Obstet. Gynecol. 2013, 121, 601–606. [Google Scholar] [CrossRef]
- Osório, F.L.; Carvalho, A.C.F.; Donadon, M.F.; Moreno, A.L.; Polli-Neto, O. Chronic pelvic pain, psychiatric disorders and early emotional traumas: Results of a cross sectional case-control study. World J. Psychiatry 2016, 6, 339–344. [Google Scholar] [CrossRef]
- Latthe, P.; Mignini, L.; Gray, R.; Hills, R.; Khan, K. Factors predisposing women to chronic pelvic pain: Systematic review. BMJ 2006, 332, 749–755. [Google Scholar] [CrossRef] [Green Version]
- McCrory, E.J.; Viding, E. The theory of latent vulnerability: Reconceptualizing the link between childhood maltreatment and psychiatric disorder. Dev. Psychopathol. 2015, 27, 493–505. [Google Scholar] [CrossRef]
- Harris, H.R.; Wieser, F.; Vitonis, A.F.; Rich-Edwards, J.; Boynton-Jarrett, R.; Bertone-Johnson, E.R.; Missmer, S.A. Early life abuse and risk of endometriosis. Hum. Reprod. 2018, 33, 1657–1668. [Google Scholar] [CrossRef]
- Liebermann, C.; Schwartz, A.S.K.; Charpidou, T.; Geraedts, K.; Rauchfuss, M.; Wöl, M.; Von Orelli, S.; Häberlin, F.; Eberhard, M.; Imesch, P.; et al. Maltreatment during childhood: A risk factor for the development of endometriosis? Hum. Reprod. 2018, 33, 1449–1458. [Google Scholar] [CrossRef] [Green Version]
- Schliep, K.C.; Mumford, S.L.; Johnstone, E.B.; Peterson, C.M.; Sharp, H.T.; Stanford, J.B.; Chen, Z.; Backonja, U.; Wallace, M.E.; Buck Louis, G.M. Sexual and physical abuse and gynecologic disorders. Hum. Reprod. 2016, 31, 1904–1912. [Google Scholar] [CrossRef] [Green Version]
- Haas, D.; Shebl, O.; Shamiyeh, A.; Oppelt, P. The rASRM score and the ENZIAN classification for endometriosis: Their strengths and weaknesses. Acta Obstet. Gynecol. Scand. 2013, 92, 3–7. [Google Scholar] [CrossRef]
- Margraf, J.; Cwik, J.C.; Suppiger, A.; Schneider, S. DIPS Open Access: Diagnostic Interview for Mental Disorders, 5th ed.; Mental Health Research and Treament Center, Ruhr-Universität Bochum: Bochum, Germany, 2017. (In German) [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Margraf, J.; Cwik, J.C.; Pflug, V.; Schneider, S. Structured clinical interviews for mental disorders across the lifespan: Psychometric quality and further developments of the DIPS Open Access Interviews. Z. Klin. Psychol. Psychother. 2017, 46, 176–186. [Google Scholar] [CrossRef]
- Lampert, T.; Kroll, L.E.; Müters, S.; Stolzenberg, H. Messung des sozioökonomischen Status in der Studie “Gesundheit in Deutschland Aktuell“ (GEDA). Bundesgesundheitsblatt 2013, 56, 131–143. [Google Scholar] [CrossRef] [Green Version]
- Klinitzke, G.; Romppel, M.; Häuser, W.; Brähler, E.; Glaesmer, H. The German version of the Childhood Trauma Questionnaire (CTQ)—Psychometric characteristics in a representative sample of the general population. Psychother. Psychosom. Med. Psychol. 2012, 62, 47–51. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, Version 26.0; IBM Corp: Armonk, NY, USA, 2019. [Google Scholar]
- Field, A. Discovering Statistics Using SPSS, 3rd ed.; Sage Publications: London, UK, 2009. [Google Scholar]
- Márki, G.; Bokor, A.; Rigó, J.; Rigó, A. Physical pain and emotion regulation as the main predictive factors of health-related quality of life in women living with endometriosis. Hum. Reprod. 2017, 32, 1432–1438. [Google Scholar] [CrossRef]
- Facchin, F.; Saita, E.; Barbara, G.; Dridi, D.; Vercellini, P. “Free butterflies will come out of these deep wounds”: A grounded theory of how endometriosis affects women’s psychological health. J. Health Psychol. 2017, 23, 538–549. [Google Scholar] [CrossRef]
- Denny, E. “I never know from one day to another how I will feel”: Pain and uncertainty in women with endometriosis. Qual. Health Res. 2009, 19, 985–995. [Google Scholar] [CrossRef]
- Jones, G.; Jenkinson, C.; Kennedy, S. The impact of endometriosis upon quality of life: A qualitative analysis. J. Psychosom. Obstet. Gynecol. 2004, 25, 123–133. [Google Scholar] [CrossRef]
- Krantz, T.E.; Andrews, N.; Petersen, T.R.; Dunivan, G.C.; Montoya, M.; Swanson, N.; Wenzl, C.K.; Zambrano, J.R.; Komesu, Y.M. Adverse childhood experiences among gynecology patients with chronic pelvic pain. Obstet. Gynecol. 2019, 134, 1087–1095. [Google Scholar] [CrossRef]
- Wischmann, T. Psychologische Aspekte bei Endometriose und Kinderwunsch—Einige kritische Anmerkungen. Geburtshilfe Frauenheilkd. 2008, 68, 231–235. [Google Scholar] [CrossRef]
- Münch, F.; Ebert, A.D.; Mechsner, S.; Richter, R.; David, M. Subjective theories of illness in fibroid and endometriosis patients: Similarities, differences, and influencing factors. J. Endometr. Pelvic Pain Disord. 2022, 14, 71–79. [Google Scholar] [CrossRef]
- Hoffman, D. Central and peripheral pain generators in women with chronic pelvic pain: Patient centered assessment and treatment. Curr. Rheumatol. Rev. 2015, 11, 146–166. [Google Scholar] [CrossRef]
- Hortu, I.; Ozceltik, G.; Karadadas, E.; Erbas, O.; Yigitturk, G.; Ulukus, M. The role of ankaferd blood stopper and oxytocin as potential therapeutic agents in endometriosis: A rat model. Curr. Med. Sci. 2020, 40, 556–562. [Google Scholar] [CrossRef]
- Karadadas, E.; Hortu, I.; Ak, H.; Ergenoglu, A.M.; Karadadas, N.; Aydin, H.H. Evaluation of complement systems proteins C3a, C5a and C6 in patients of endometriosis. Clin. Biochem. 2020, 81, 15–19. [Google Scholar] [CrossRef]
- Laganà, A.S.; La Rosa, V.L.; Rapisarda, A.M.C.; Valenti, G.; Sapia, F.; Chiofalo, B.; Rossetti, D.; Frangez, H.B.; Bokal, E.V.; Vitale, S.G. Anxiety and depression in patients with endometriosis: Impact and management challenges. Int. J. Womens Health 2017, 9, 323–330. [Google Scholar] [CrossRef] [Green Version]
- Facchin, F.; Barbara, G.; Dridi, D.; Alberico, D.; Buggio, L.; Somigliana, E.; Saita, E.; Vercellini, P. Mental health in women with endometriosis: Searching for predictors of psychological distress. Hum. Reprod. 2017, 32, 1855–1861. [Google Scholar] [CrossRef]
| Group | |||||
|---|---|---|---|---|---|
| N | CPP (n = 50) 1 | NOPAIN (n = 50) 1 | p-Value | Effect Size 1 | |
| Sociodemographic data | |||||
| Age | 99 | 28.79 (5.59) | 32.71 (6.26) | 0.001 2,7 | d = 0.66 |
| Socioeconomic status | 90 | 10.65 (8.81; 12.04) | 11.80 (10.60; 13.50) | 0.008 3,7 | d = 0.57 |
| Relationship | 100 | 36 (72%) | 43 (86%) | 0.140 4,7 | |
| Children | 100 | 7 (14%) | 12 (24%) | 0.154 4,6 | |
| University degree | 98 | 22 (45%) | 24 (49%) | 0.840 4,7 | |
| Clinical characteristics | |||||
| Time since first diagnosis (years) | 99 | 2.07 (1.34; 4.65) | 3.76 (2.00; 7.21) | 0.008 3,7 | d = 0.56 |
| Number of surgeries | 99 | 2.00 (1.00; 3.00) | 1.00 (1.00; 2.00) | 0.051 3,7 | |
| Hormonal treatment | 100 | 34 (68%) | 30 (60%) | 0.532 4,7 | |
| Hormones: Mode of intake 8 | 63 | - | - | 0.525 4,7 | |
| Hormones: Substance 9 | 100 | - | - | 0.708 5,7 | |
| Hormones: Tolerance | 54 | 2.00 (2.00; 3.00) | 3.00 (3.00; 3.00) | <0.001 3,7 | d = 0.96 |
| Hormones: Pain reduction | 52 | 2.00 (1.50; 3.00) | 5.00 (4.00; 5.00) | <0.001 3,6 | d = 1.85 |
| Infertility | 100 | 18 (36%) | 15 (30%) | 0.335 4,6 | |
| Other medical condition | 100 | 27 (54%) | 21 (42%) | 0.158 4,6 | |
| Additional persistent pain | 100 | 43 (86%) | 14 (28%) | <0.001 4,6 | OR = 15.80 |
| Endometriosis | |||||
| Pelvic pain days per month | 100 | 30.50 (25.00; 31.00) | 1.00 (0.00; 2.50) | <0.001 3,7 | d = 3.40 |
| Dysmenorrhea | 99 | 32 (65%) | 17 (34%) | 0.002 4,6 | OR = 3.65 |
| Primary dysmenorrhea | 38 | 29 (88%) | 12 (80%) | 0.378 5,6 | |
| Pain intensity | 98 | 6.00 (0.00; 8.00) | 0.00 (0.00; 1.00) | <0.001 3,7 | d = 1.05 |
| Pain intensity: treatment-goal | 98 | 3.00 (0.00; 4.00) | 0.00 (0.00; 1.25) | <0.001 3,7 | d = 0.83 |
| Pain intensity: discrepancy | 97 | 2.00 (0.00; 4.00) | 0.00 (0.00; 0.00) | <0.001 3,7 | d = 1.40 |
| Non-menstrual cyclical pelvic pain | 98 | 30 (63%) | 10 (20%) | <0.001 4,6 | OR = 6.67 |
| Duration (years) | 36 | 10.00 (5.00; 15.00) | 7.00 (4.75; 11.00) | 0.351 3,7 | |
| Pain intensity | 99 | 4.00 (0.00; 6.00) | 0.00 (0.00; 0.00) | <0.001 3,7 | d = 1.08 |
| Pain intensity: treatment-goal | 99 | 2.00 (0.00; 3.00) | 0.00 (0.00; 0.00) | <0.001 3,7 | d = 0.85 |
| Pain intensity: discrepancy | 98 | 2.00 (0.00; 3.00) | 0.00 (0.00; 0.00) | <0.001 3,7 | d = 1.22 |
| Non-cyclical pelvic pain | 100 | 50 (100%) | 11 (22%) | <0.001 4,6 | |
| Duration (years) | 48 | 6.00 (3.00; 10.25) | 5.00 (0.85; 7.25) | 0.173 3,7 | |
| Pain intensity | 97 | 5.00 (4.00; 6.00) | 0.00 (0.00; 0.00) | <0.001 3,7 | d = 3.11 |
| Pain intensity: treatment-goal | 97 | 2.00 (1.00; 3.00) | 0.00 (0.00; 0.00) | <0.001 3,7 | d = 1.49 |
| Pain intensity: discrepancy | 96 | 3.00 (2.00; 3.50) | 0.00 (0.00; 0.00) | <0.001 3,7 | d = 2.88 |
| Duration of CPP (years) | 42 | 2.25 (1.50; 5.00) | - | - | |
| Painful sexual intercourse | 100 | 46 (92%) | 27 (54%) | <0.001 4,7 | OR = 9.80 |
| Pain intensity | 99 | 5.00 (3.00; 7.00) | 0.00 (0.00; 2.00) | <0.001 3,7 | d = 1.82 |
| Pain intensity: treatment-goal | 99 | 1.50 (1.00; 3.00) | 0.00 (0.00; 1.00) | <0.001 3,7 | d = 0.83 |
| Pain intensity: discrepancy | 99 | 3.00 (2.00; 4.00) | 0.00 (0.00; 0.13) | <0.001 3,7 | d = 1.73 |
| Dyschezia | 100 | 40 (80%) | 23 (46%) | <0.001 4,7 | OR = 4.70 |
| Pain intensity | 99 | 4.00 (2.00; 5.00) | 0.00 (0.00; 2.00) | <0.001 3,7 | d = 1.15 |
| Pain intensity: treatment-goal | 98 | 2.00 (0.00; 2.00) | 0.00 (0.00; 1.25) | <0.001 3,7 | d = 0.76 |
| Pain intensity: discrepancy | 98 | 2.00 (0.00; 3.00) | 0.00 (0.00; 1.00) | <0.001 3,7 | d = 0.98 |
| Dysuria | 100 | 26 (52%) | 7 (14%) | <0.001 4,7 | OR = 6.65 |
| Pain intensity | 100 | 0.75 (0.00; 4.00) | 0.00 (0.00; 0.00) | <0.001 3,7 | d = 0.72 |
| Pain intensity treatment-goal | 99 | 0.00 (0.00; 2.00) | 0.00 (0.00; 0.00) | <0.001 3,7 | d = 0.66 |
| Pain intensity: discrepancy | 99 | 0.00 (0.00; 2.00) | 0.00 (0.00; 0.00) | <0.001 3,7 | d = 0.58 |
| Psychosocial characteristics | |||||
| Affected career | 98 | 24 (49%) | 16 (33%) | 0.075 4,7 | |
| Affected relationship | 95 | 42 (89%) | 24 (50%) | <0.001 4,7 | OR = 8.4 |
| Group | |||||
|---|---|---|---|---|---|
| N | CPP (n = 50) 1 | NOPAIN (n = 50) 1 | p-Value | Effect Size 1 | |
| Current mental disorder | 100 | 24 (48%) | 13 (26%) | 0.019 2,4 | 2.63 |
| Anxiety | 100 | 19 (38%) | 11 (22%) | 0.063 2,4 | |
| Bipolar | 100 | - | - | - | |
| Depressive | 100 | 5 (10%) | 2 (4%) | 0.218 3,4 | |
| Obsessive-compulsive and related | 100 | 1 (2%) | 2 (4%) | 0.500 3,4 | |
| Trauma- and stressor related | 100 | 4 (8%) | 1 (2%) | 0.181 3,4 | |
| Somatic symptom and related | 100 | 7 (14%) | 1 (2%) | 0.030 3,4 | 7.98 |
| Feeding and eating | 100 | 1 (2%) | - | 0.500 3,4 | |
| Substance-related and addictive | 100 | - | - | - | |
| Former mental disorder | 100 | 32 (64%) | 21 (42%) | 0.022 2,4 | 2.46 |
| Anxiety | 100 | 7 (14%) | 7 (14%) | 0.613 2,4 | |
| Bipolar | 100 | - | - | - | |
| Depressive | 100 | 27 (54%) | 14 (28%) | 0.007 2,4 | 3.02 |
| Obsessive-compulsive and related | 100 | - | 1 (2%) | 0.500 3,4 | |
| Trauma- and stressor related | 100 | - | - | - | |
| Somatic symptom and related | 100 | - | - | - | |
| Feeding and eating | 100 | 5 (10%) | 1 (2%) | 0.102 3,4 | |
| Substance-related and addictive | 100 | 1 (2%) | 1 (2%) | 0.753 3,4 | |
| Lifetime mental disorder | 100 | 39 (78%) | 26 (52%) | 0.006 2,4 | 3.27 |
| Anxiety | 100 | 26 (52%) | 15 (30%) | 0.021 2,4 | 2.53 |
| Bipolar | 100 | - | - | - | |
| Depressive | 100 | 32 (64%) | 15 (30%) | 0.001 2,4 | 4.15 |
| Obsessive-compulsive and related | 100 | 1 (2%) | 3 (6%) | 0.309 3,4 | |
| Trauma- and stressor related | 100 | 4 (8%) | 1 (2%) | 0.181 3,4 | |
| Somatic symptom and related | 100 | 7 (14%) | 1 (2%) | 0.030 3,4 | 7.98 |
| Feeding and eating | 100 | 6 (12%) | 1 (2%) | 0.056 3,4 | |
| Substance-related and addictive | 100 | 1 (2%) | 1 (2%) | 0.753 3,4 | |
| Sexual dysfunction | 100 | 32 (64%) | 10 (20%) | <0.001 2,4 | 7.11 |
| Sexual Desire | 100 | 26 (52%) | 10 (20%) | 0.001 2,4 | 4.33 |
| Sexual Arousal | 100 | 24 (48%) | 7 (14%) | <0.001 2,4 | 5.67 |
| Orgasmic | 100 | 20 (40%) | 6 (12%) | 0.001 2,4 | 4.89 |
| Dyspareunia | 100 | 32 (64%) | 8 (16%) | <0.001 2,4 | 9.33 |
| Vaginismus | 100 | 14 (28%) | 1 (2%) | <0.001 2,4 | 19.06 |
| Rates: childhood maltreatment CM 7 | 92 | 22 (49%) | 15 (32%) | 0.074 2,4 | 2.04 |
| Emotional abuse | 96 | 12 (25%) | 6 (12%) | 0.095 2,4 | |
| Physical abuse | 98 | 5 (10%) | 4 (8%) | 0.500 3,4 | |
| Sexual abuse | 91 | 9 (21%) | 5 (11%) | 0.157 2,4 | |
| Emotional neglect | 96 | 6 (13%) | 8 (16%) | 0.420 2,4 | |
| Physical neglect | 95 | 23 (49%) | 26 (54%) | 0.380 2,4 | |
| Scales: CTQ 8 | 90 | 29.00 (24.00; 35.00) | 28.00 (23.00; 33.00) | 0.437 5,6 | |
| Emotional abuse | 96 | 8.50 (7.00; 12.75) | 9.00 (6.25; 10.00) | 0.472 5,6 | |
| Physical abuse | 98 | 4.00 (4.00; 4.00) | 4.00 (4.00; 4.00) | 0.890 5,6 | |
| Sexual abuse | 91 | 5.00 (5.00; 7.00) | 5.00 (5.00; 5.00) | 0.117 5,6 | |
| Emotional neglect | 96 | 9.00 (7.00; 12.00) | 9.00 (6.00; 12.00) | 0.822 5,6 | |
| Physical neglect | 95 | 9.00 (9.00; 11.00) | 10.00 (9.00; 11.00) | 0.554 5,6 | |
| Trivialization | 95 | 0.00 (0.00; 0.00) | 0.00 (0.00; 0.75) | 0.380 5,6 | |
| Number of CM 7 | 92 | 1.00 (0.00; 2.00) | 1.00 (0.00; 2.00) | 0.547 5,6 | |
| Variable | B (Std.-Error) 1 | p-Value | aOR 1 | 95%-CI 1 |
|---|---|---|---|---|
| Model i) pelvic pain2 | ||||
| Pelvic pain days per month | −0.01 (0.04) | 0.737 | 0.99 | 0.92–1.06 |
| PC_intensity 3 | −0.43 (0.67) | 0.522 | 0.65 | 0.18–2.42 |
| PC_painrelief 4 | 1.41 (0.63) | 0.026 | 4.08 | 1.19–14.04 |
| Constant | −0.49 (0.57) | 0.394 | 0.61 | |
| Model ii) psychosocial5 | ||||
| Childhood maltreatment CM 6 | −0.14 (0.47) | 0.768 | 0.87 | 0.35–2.19 |
| Former mental disorder | 0.84 (0.47) | 0.073 | 2.31 | 0.92–5.78 |
| Any sexual dysfunction | 0.99 (0.46) | 0.031 | 2.69 | 1.09–6.64 |
| Constant | −1.49 (0.47) | 0.001 | 0.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Netzl, J.; Gusy, B.; Voigt, B.; Sehouli, J.; Mechsner, S. Chronic Pelvic Pain in Endometriosis: Cross-Sectional Associations with Mental Disorders, Sexual Dysfunctions and Childhood Maltreatment. J. Clin. Med. 2022, 11, 3714. https://doi.org/10.3390/jcm11133714
Netzl J, Gusy B, Voigt B, Sehouli J, Mechsner S. Chronic Pelvic Pain in Endometriosis: Cross-Sectional Associations with Mental Disorders, Sexual Dysfunctions and Childhood Maltreatment. Journal of Clinical Medicine. 2022; 11(13):3714. https://doi.org/10.3390/jcm11133714
Chicago/Turabian StyleNetzl, Johanna, Burkhard Gusy, Barbara Voigt, Jalid Sehouli, and Sylvia Mechsner. 2022. "Chronic Pelvic Pain in Endometriosis: Cross-Sectional Associations with Mental Disorders, Sexual Dysfunctions and Childhood Maltreatment" Journal of Clinical Medicine 11, no. 13: 3714. https://doi.org/10.3390/jcm11133714
APA StyleNetzl, J., Gusy, B., Voigt, B., Sehouli, J., & Mechsner, S. (2022). Chronic Pelvic Pain in Endometriosis: Cross-Sectional Associations with Mental Disorders, Sexual Dysfunctions and Childhood Maltreatment. Journal of Clinical Medicine, 11(13), 3714. https://doi.org/10.3390/jcm11133714