
Effects of Sacubitril/Valsartan on the Renal Resistance Index

 , , ,
, , , 

Abstract
:1. Introduction
2. Materials and Methods
- -
- Medical examination and ECG. Records were documented, including ischemic heart disease, arterial hypertension, diabetes mellitus, history of ventricular arrhythmic events, NYHA class, arterial pressure, heart rhythm and heart rate at ECG;
- -
- Echocardiographic examinations. Left ventricular end-diastolic volume (LVEDV), end-systolic volume (LVESV), and LVEF were calculated with Simpson’s rule. The peak of the E wave (E), through mitral pulsed Doppler at the level of the mitral leaflets, and early diastolic velocity peak (e’) at the level of the septal and lateral mitral annulus, through tissue Doppler imaging, were measured. The E/e’ ratio was then calculated as the ratio between E and the mean value of septal and lateral e’. The central venous pressure was determined through the assessment of the inferior vena cava diameter and respiratory excursion. The mitral regurgitation (MR) was evaluated and quantified in arbitrary units (a.u. range from 0 to 4). The systolic pulmonary artery pressure (PAP) was estimated by the measurement of the RV–right atrium gradient from the peak velocity of the tricuspid valve regurgitation (TR) with the simplified Bernoulli equation; this value was added to an estimate of the mean right atrium pressure. The RV systolic function was evaluated according to tricuspid annular plane systolic excursion (TAPSE);
- -
- Doppler of interlobular renal arteries. The method to assess the RRI was described previously [12,13]. The renal arterial Doppler was performed after echocardiographic examination by using the same echograph (Vivid 7, GE Vingmed Ultrasound, General Electric or EPIQ CVx system, Philips, Amsterdam, The Netherlands) and the same 4 MHz probe, moving the patient into the sitting position and using a posterior approach to the kidney. The course of the right or left kidney segmental arteries was visualized by color Doppler flow and then, at the middle tract level of the best visualized one, pulsed Doppler was performed. Every effort was made to achieve the best alignment of the ultrasonic beam. An average of 2–3 measurements of the peak systolic velocity and the end-diastolic velocity were used to calculate the RRI according to Peurcelot’s formula, i.e., 100 × [1 − (end-diastolic velocity/peak systolic velocity)].
- -
- Blood sample analyses. Blood samples were collected to evaluate NT-proBNP (immunoassay Dade Behring, Eschborn, Germany) and creatinine (mg/dL). The glomerular filtration rate was calculated with the abbreviated CKD-EPI formula (GFR-EPI, ml/min/1.73 m2) [14].
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mcmurray, J.J.V.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin–Neprilysin Inhibition versus Enalapril in Heart Failure. PARADIGM-HF Investigators and Committees. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, A.S.; Solomon, S.D.; Shah, A.M.; Claggett, B.L.; Fang, J.C.; Izzo, J.; McCague, K.; Abbas, C.A.; Rocha, R.; Mitchell, G.F.; et al. Effect of Sacubitril-Valsartan vs. Enalapril on Aortic Stiffness in Patients with Heart Failure and Reduced Ejection Fraction: A Randomized Clinical Trial. JAMA 2019, 322, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Januzzi, J.L., Jr.; Prescott, M.F.; Butler, J.; Felker, G.M.; Maisel, A.S.; McCague, K.; Camacho, A.; Piña, I.L.; Rocha, R.A.; Shah, A.M.; et al. Association of Change in N-Terminal Pro-B-Type Natriuretic Peptide Following Initiation of Sacubitril-Valsartan Treatment With Cardiac Structure and Function in Patients With Heart Failure With Reduced Ejection Fraction. JAMA 2019, 322, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Buggey, J.; Mentz, R.J.; DeVore, A.D.; Velazquez, E.J. Angiotensin receptor neprilysin inhibition in heart failure: Mech-anistic action and clinical impact. J. Card. Fail. 2015, 21, 741–750. [Google Scholar] [CrossRef] [PubMed]
- Díez, J. Chronic heart failure as a state of reduced effectiveness of the natriuretic peptide system: Implications for therapy. Eur. J. Heart Fail. 2017, 19, 167–176. [Google Scholar] [CrossRef] [Green Version]
- Damman, K.; Gori, M.; Claggett, B.; Jhund, P.; Senni, M.; Lefkowitz, M.P.; Prescott, M.F.; Shi, V.C.; Rouleau, J.L.; Swedberg, K.; et al. Renal Effects and Associated Outcomes During Angiotensin-Neprilysin Inhibition in Heart Failure. JACC Heart Fail. 2018, 6, 489–498. [Google Scholar] [CrossRef]
- Solomon, S.D.; Zile, M.; Pieske, B.; Voors, A.; Shah, A.; Kraigher-Krainer, E.; Shi, V.; Bransford, T.; Takeuchi, M.; Gong, J.; et al. The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: A phase 2 double-blind randomised controlled trial. Lancet 2012, 380, 1387–1395. [Google Scholar] [CrossRef]
- Wang, Y.; Zhou, R.; Lu, C.; Chen, Q.; Xu, T.; Li, D. Effects of the Angiotensin-Receptor Neprilysin Inhibitor on Cardiac Reverse Remodeling: Meta-Analysis. J. Am. Heart Assoc. 2019, 8, e012272. [Google Scholar] [CrossRef] [Green Version]
- Damman, K.; Valente, M.A.; Voors, A.A.; O’Connor, C.M.; Van Veldhuisen, D.J.; Hillege, H.L. Renal impairment, worsening renal function, and outcome in patients with heart failure: An updated meta-analysis. Eur. Heart J. 2014, 35, 455–469. [Google Scholar] [CrossRef] [Green Version]
- Judge, P.; Haynes, R.; Landray, M.J.; Baigent, C. Neprilysin inhibition in chronic kidney disease. Nephrol. Dial. Transplant. 2015, 30, 738–743. [Google Scholar] [CrossRef] [Green Version]
- Iacoviello, M.; Di Serio, F.; Rizzo, C.; Leone, M.; Grande, D.; Guida, P.; Gioia, M.I.; Parisi, G.; Leopizzi, T.; Caldarola, P.; et al. Association between high Gal-3 serum levels and worsening of renal function in chronic heart failure outpatients. Biomark. Med. 2019, 13, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Ciccone, M.M.; Iacoviello, M.; Gesualdo, L.; Puzzovivo, A.; Antoncecchi, V.; Doronzo, A. The renal arterial resistance index: A marker of renal function with an independent and incremental role in predicting heart failure progression. Eur. J. Heart Fail. 2014, 16, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Bigé, N.; Levy, P.; Callard, P.; Faintuch, J.-M.; Chigot, V.; Jousselin, V.; Ronco, P.; Boffa, J.-J. Renal arterial resistive index is associated with severe histological changes and poor renal outcome during chronic kidney disease. BMC Nephrol. 2012, 13, 139. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular fil-tration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Pitzalis, M.V.; Iacoviello, M.; Romito, R.; Massari, F.; Rizzon, B.; Luzzi, G.; Guida, P.; Andriani, A.; Mastropasqua, F.; Rizzon, P. Cardiac resynchronization therapy tailored by echocardiographic evaluation of ventricular asynchrony. J. Am. Coll. Cardiol. 2002, 40, 1615–1622. [Google Scholar] [CrossRef] [Green Version]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; ESC Scientific Document Group; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the Eu-ropean Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2022, 24, 4–131. [Google Scholar]
- Rangaswami, J.; Bhalla, V.; Blair, J.E.A.; Chang, T.I.; Costa, S.; Lentine, K.L.; Lerma, E.V.; Mezue, K.; Molitch, M.; Mullens, W.; et al. American Heart Association Council on the Kidney in Cardiovascular Disease and Council on Clinical Cardiology. Car-diorenal syndrome: Classification, pathophysiology, diagnosis, and treatment strategies: A scientific statement from the American Heart Association. Circulation 2019, 139, e840–e878. [Google Scholar]
- Ushijima, K.; Ando, H.; Arakawa, Y.; Aizawa, K.; Suzuki, C.; Shimada, K.; Tsuruoka, S.; Fujimura, A. Prevention against renal damage in rats with subtotal nephrectomy by sacubitril/valsartan (LCZ696), a dual-acting angiotensin receptor-neprilysin inhibitor. Pharmacol. Res. Perspect. 2017, 5, e00336. [Google Scholar] [CrossRef]
- Iacoviello, M.; Monitillo, F.; Leone, M.; Citarelli, G.; Doronzo, A.; Antoncecchi, V.; Puzzovivo, A.; Rizzo, C.; Lattarulo, M.S.; Massari, F.; et al. The Renal Arterial Resistance Index Predicts Worsening Renal Function in Chronic Heart Failure Patients. Cardiorenal Med. 2016, 7, 42–49. [Google Scholar] [CrossRef] [Green Version]
- Ciccone, M.M.; Iacoviello, M.; Puzzovivo, A.; Scicchitano, P.; Monitillo, F.; De Crescenzo, F.; Caragnano, V.; Sassara, M.; Quistelli, G.; Guida, P.; et al. Clinical correlates of endothelial function in chronic heart failure. Clin. Res. Cardiol. 2011, 100, 515–521. [Google Scholar] [CrossRef]
- Chade, A.R. Renal vascular structure and rarefaction. Compr. Physiol. 2013, 3, 817–831. [Google Scholar]
- Braam, B.; Cupples, W.A.; Joles, J.A.; Gaillard, C. Systemic arterial and venous determinants of renal hemodynamics in congestive heart failure. Heart Fail. Rev. 2012, 17, 161–175. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Number | 66 |
| Age (years) | 56 ± 13 |
| Males, n (%) | 56 (85) |
| Ischemic etiology n, (%) | 24 (36) |
| Diabetes mellitus n, (%) | 13 (20) |
| Arterial Hypertension n, (%) | 31 (47) |
| Atrial Fibrillation n, (%) | 5 (8) |
| NYHA class II, n (%) | 49 (76) |
| III, n (%) | 17 (24) |
| BMI (kg/m2) | 29.4 ± 6.2 |
| SAP (mm Hg) | 120 ± 15 |
| Heart rate (beats/minute) | 67 ± 9 |
| LVEF (%) | 29 ± 6 |
| Creatinine (mg/dL) | 0.99 ± 1.9 |
| GFR-EPI (mL/min/1.73 m2) | 84 ± 22 |
| NT-proBNP (pg/mL) | 1052 ± 1321 |
| Concomitant therapy at the enrollment | |
| ACE-I, n (%) | 45 (68) |
| Enalapril-equivalent dose (mg/die) | 11 ± 6 |
| ACE-I ≥ 50% target dose n (% among treated) | 32 (71) |
| ARB, n (%) | 21 (32) |
| Valsartan-equivalent dose (mg/die) | 138 ± 75 |
| ARB ≥ 50% target dose (% among treated) | 11 (55) |
| Beta-blockers (%) | 65 (98) |
| Bisoprolol-equivalent dose (mg/die) | 7.1 ± 3.2 |
| Beta-blocker ≥ 50% target dose | 50 (76) |
| MRA n, (%) | 58 (88) |
| MRA dose | 45 ± 26 |
| Loop diuretics n, (%) | 52 (79) |
| Furosemide-equivalent dose (mg/die) | 76 ± 102 |
| ICD, n (%) | 61 (95) |
| CRT, n (%) | 22 (34) |
| Sacubitril/Valsartan up-titrated dose | |
| 24/26 mg b.i.d., n (%) | 34 (51) |
| 49/51 mg b.i.d., n (%) | 22 (34) |
| 97/103 mg b.i.d., n (%) | 10 (15) |
| Sacubitril/Valsartan | ||||
|---|---|---|---|---|
| Before | After | |||
| T-1 | T0 | T1 | p | |
| SAP (mmHg) | 122 ± 16 | 120 ± 15 | 116 ± 19 † | 0.037 |
| LVEDV (mL) | 193 ± 50 | 184 ± 57 | 173 ± 56 *† | <0.001 |
| LVESV (mL) | 136 ± 41 | 133 ± 48 | 116 ± 46 *† | <0.001 |
| LVEF (%) | 30 ± 6 | 29 ± 6 † | 34 ± 6 *† | <0.001 |
| MR (a.u.) | 1.8 ± 0.8 | 1.7 ± 0.8 | 1.6 ± 0.6 | 0.154 |
| LAV (mL) | 83 ± 29 | 82 ± 32 | 70 ± 27 *† | <0.001 |
| E/e’ | 10.8 ± 3.4 | 10.9 ± 3.4 | 9.7 ± 3.9 *† | 0.033 |
| TAPSE (mm) | 19.6 ± 3.8 | 19.8 ± 3.3 | 20.4 ± 3.4 | 0.281 |
| TR (a.u.) | 1.6 ± 0.7 | 1.5 ± 0.6 | 1.5 ± 0.6 | 0.541 |
| CVP (mmHg) | 4.9 ± 2.6 | 4.0 ± 2.2 | 4.4 ± 2.5 | 0.132 |
| PAPs (mmHg) | 32 ± 8 | 32 ± 7 | 30 ± 6 * | 0.049 |
| Creatinine (mg/dL) | 0.96 ± 0.24 | 0.99 ± 0.26 | 1.01 ± 0.22 | 0.404 |
| GFR-EPI (mL/min/1.73 m2) | 87 ± 20 | 84 ± 21 | 83 ± 20 | 0.268 |
| NTproBNP (pg/mL) | 857 ± 1105 | 1052 ± 1321 | 614 ± 653 *† | 0.017 |
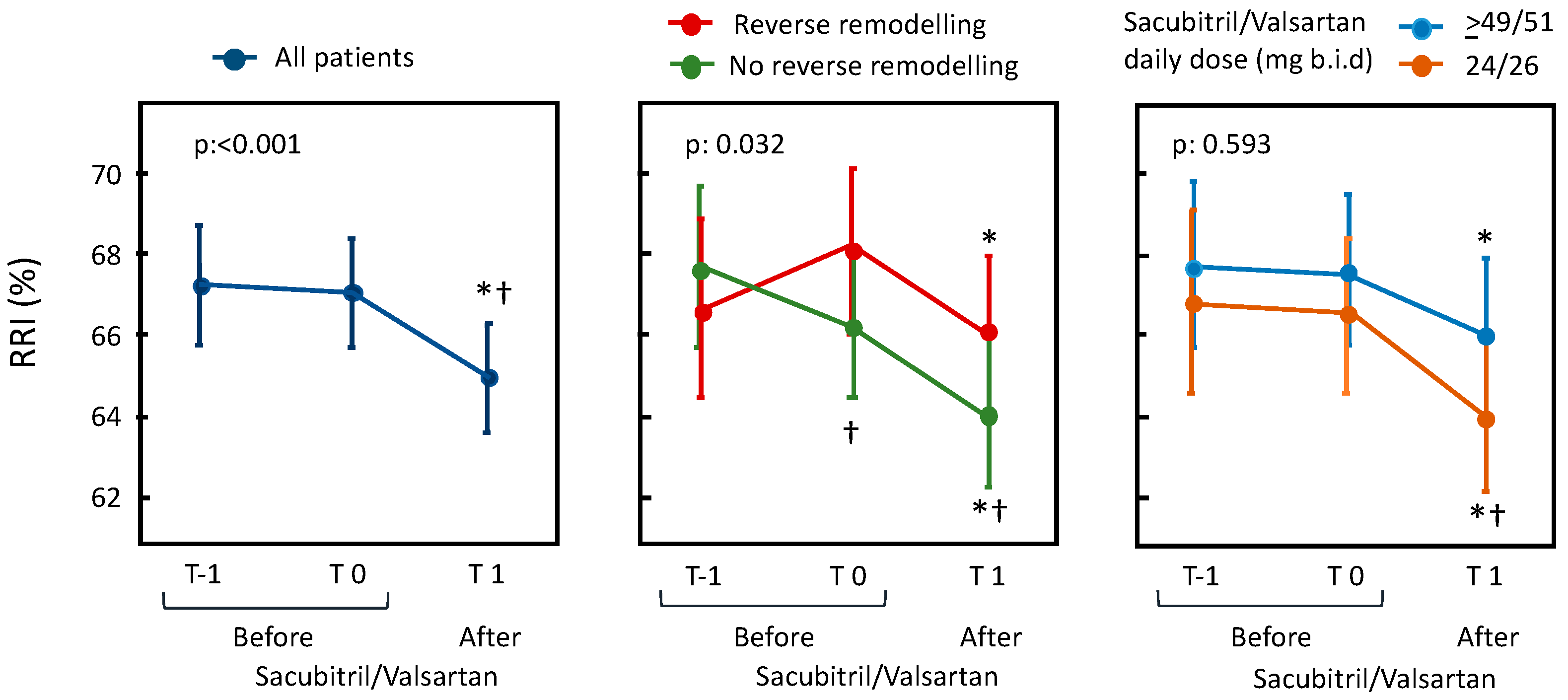
| RRI (%) | 66.9 ± 5.5 | 67.0 ± 5.5 | 64.9 ± 5.5 *† | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gioia, M.I.; Parisi, G.; Grande, D.; Albanese, M.; Alcidi, G.; Correale, M.; Brunetti, N.D.; Ciccone, M.M.; Iacoviello, M. Effects of Sacubitril/Valsartan on the Renal Resistance Index. J. Clin. Med. 2022, 11, 3683. https://doi.org/10.3390/jcm11133683
Gioia MI, Parisi G, Grande D, Albanese M, Alcidi G, Correale M, Brunetti ND, Ciccone MM, Iacoviello M. Effects of Sacubitril/Valsartan on the Renal Resistance Index. Journal of Clinical Medicine. 2022; 11(13):3683. https://doi.org/10.3390/jcm11133683
Chicago/Turabian StyleGioia, Margherita Ilaria, Giuseppe Parisi, Dario Grande, Miriam Albanese, Gianmarco Alcidi, Michele Correale, Natale Daniele Brunetti, Marco Matteo Ciccone, and Massimo Iacoviello. 2022. "Effects of Sacubitril/Valsartan on the Renal Resistance Index" Journal of Clinical Medicine 11, no. 13: 3683. https://doi.org/10.3390/jcm11133683
APA StyleGioia, M. I., Parisi, G., Grande, D., Albanese, M., Alcidi, G., Correale, M., Brunetti, N. D., Ciccone, M. M., & Iacoviello, M. (2022). Effects of Sacubitril/Valsartan on the Renal Resistance Index. Journal of Clinical Medicine, 11(13), 3683. https://doi.org/10.3390/jcm11133683