
Text-Based vs. Graphical Information Formats in Sepsis Prevention and Early Detection: A Randomized Controlled Trial on Informed Choice


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Overview
2.2. Procedure
2.3. Sample Size
2.4. Participant Characteristics
2.5. Participant Flow
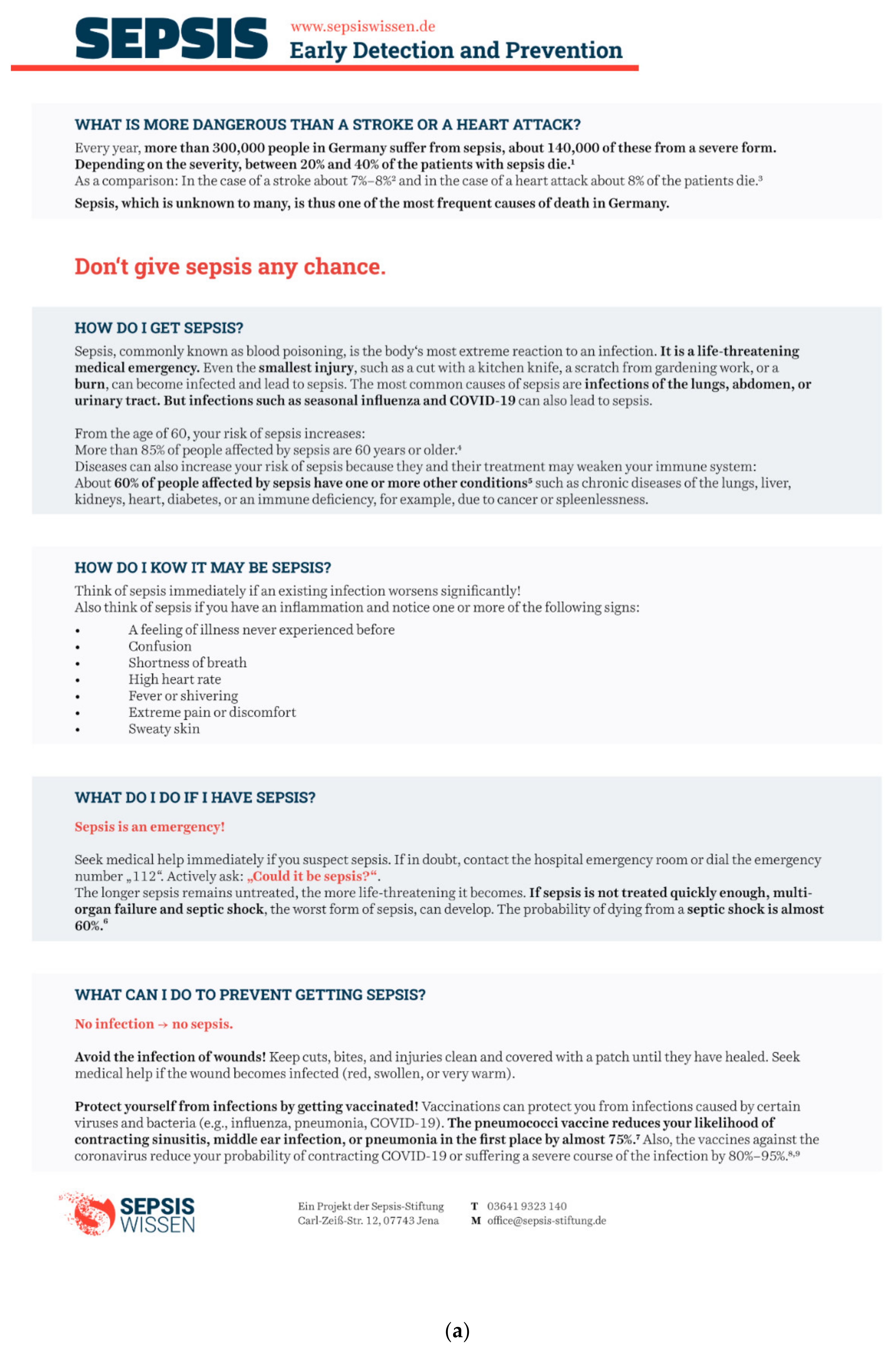
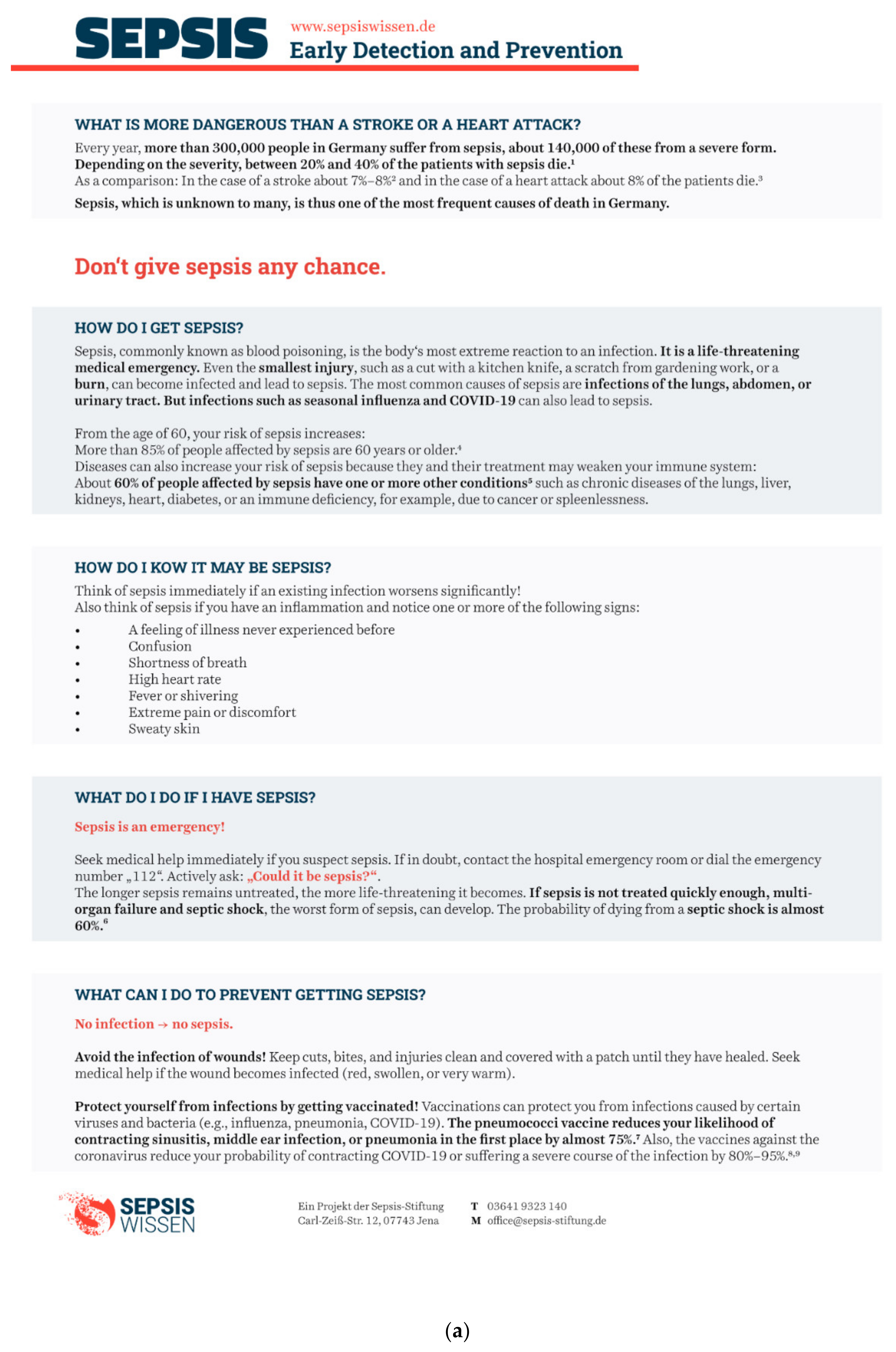
2.6. Materials
Information Formats
2.7. Measures
2.7.1. Informed Choice
2.7.2. Relevance of Information
2.8. Statistical Methods
3. Results
3.1. Sample Characteristics
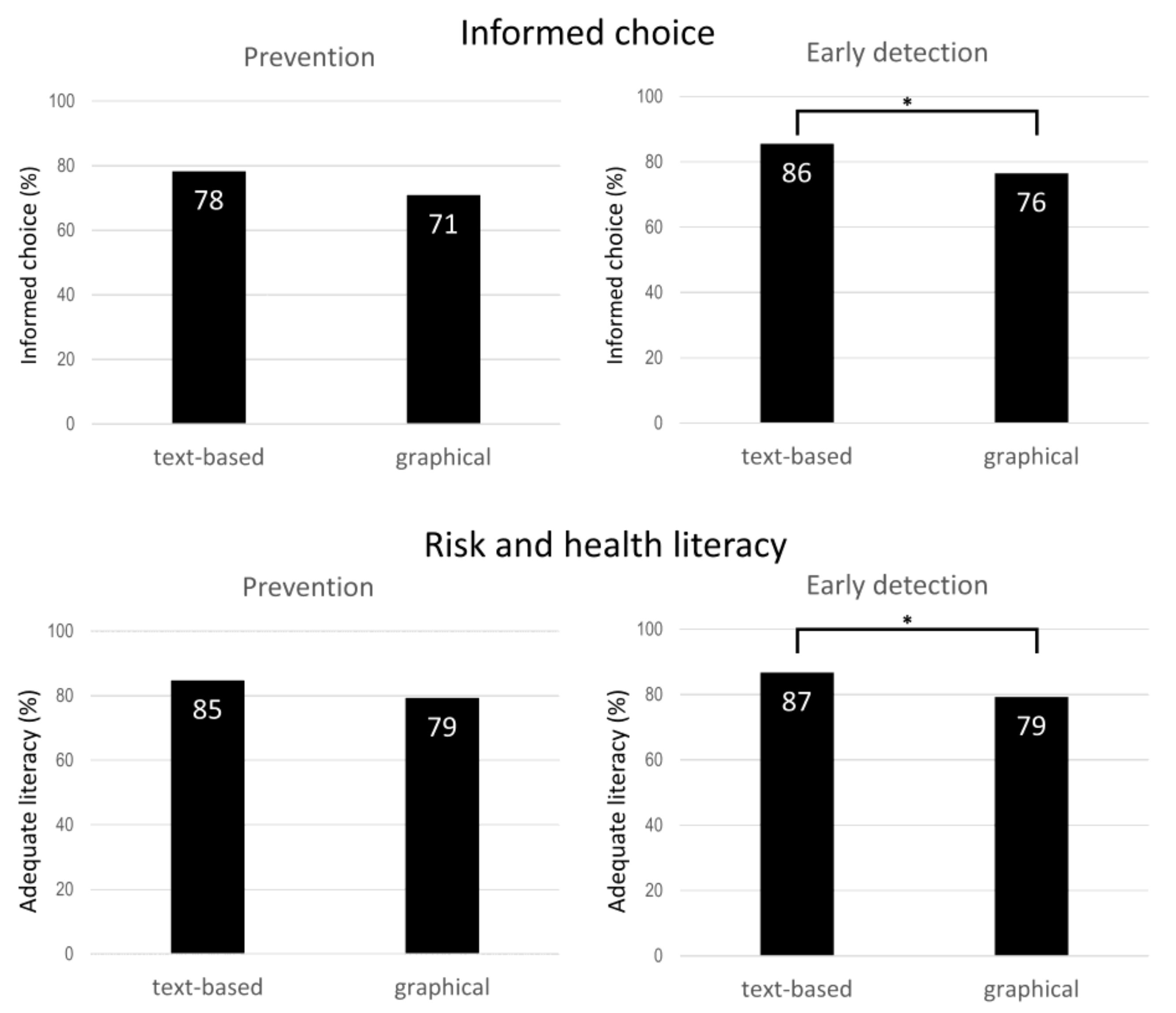
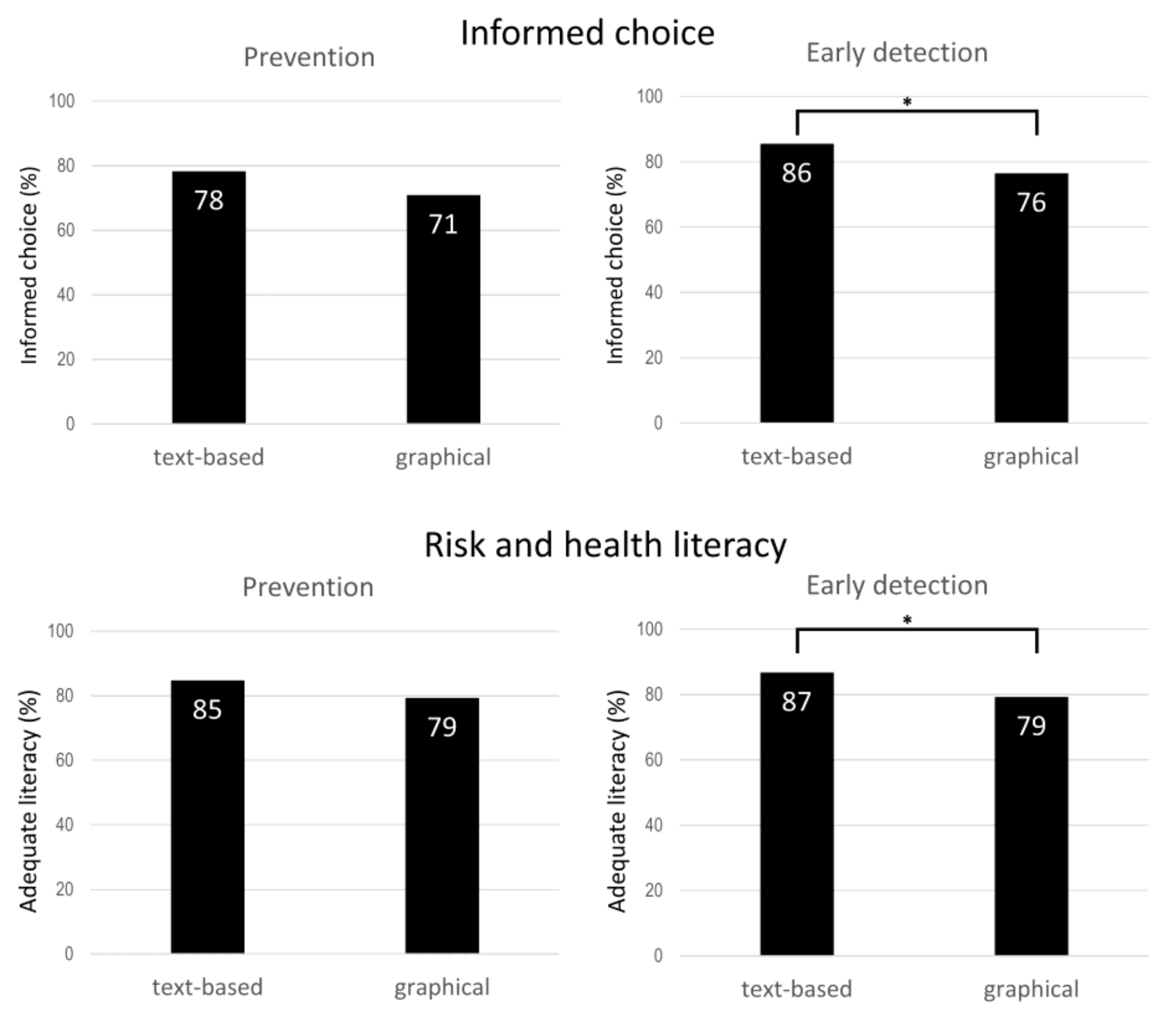
3.2. Informed Choice and Risk and Health Literacy for Text-Based and Graphical Formats
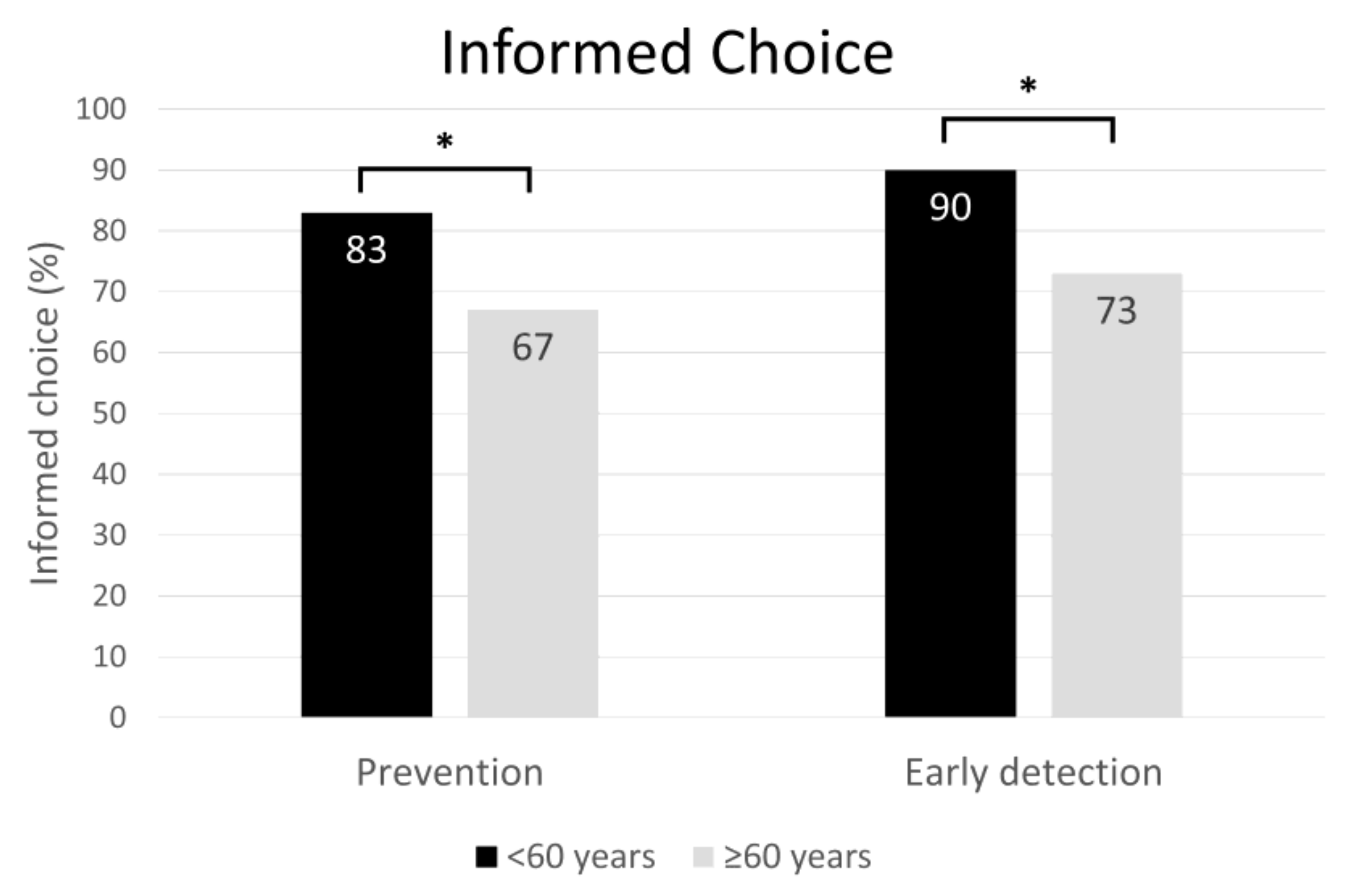
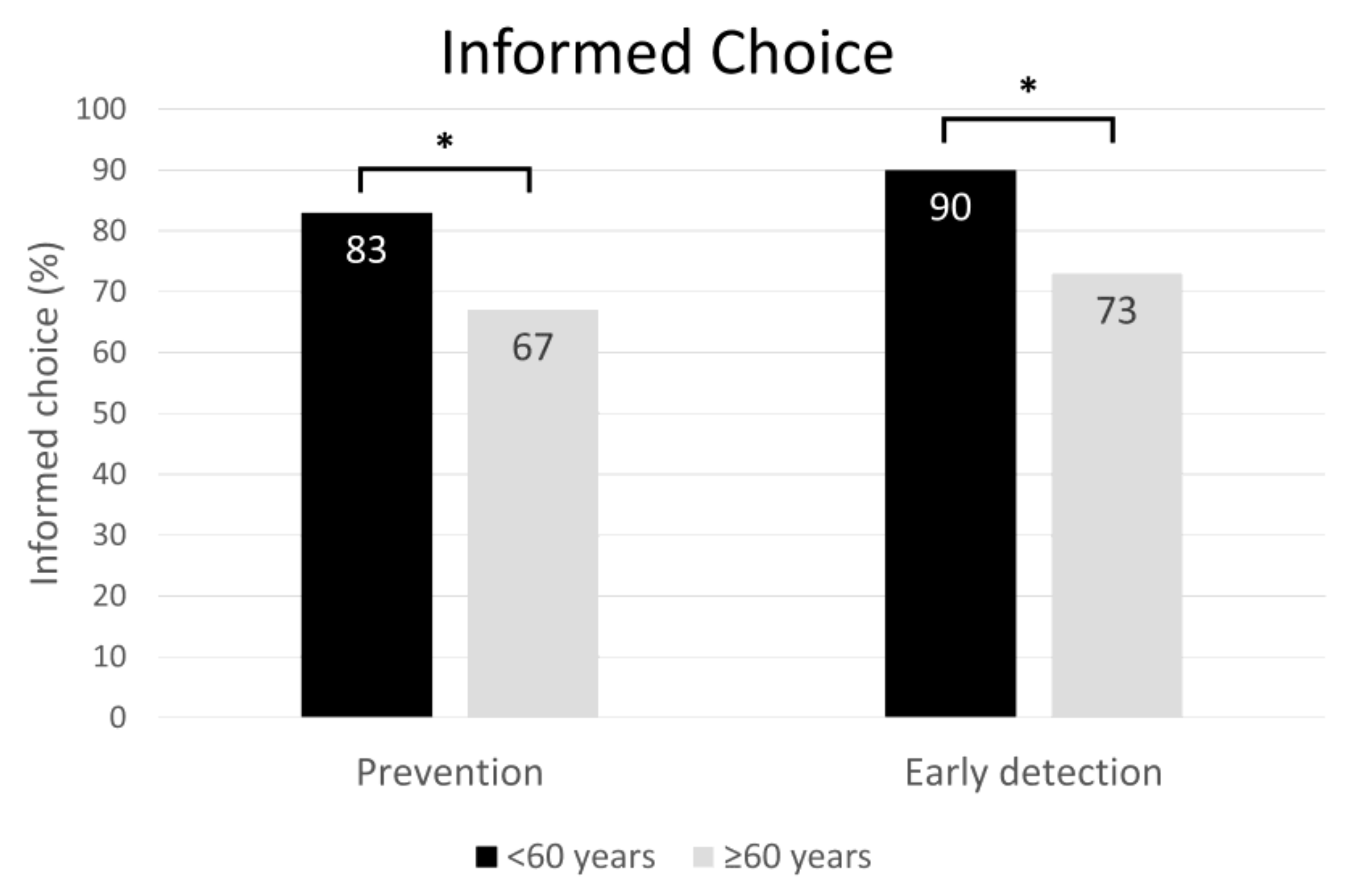
3.3. Differences between Age Groups
3.4. Relevance of Information
3.5. Soft-Launch Data: Pre–Post Differences
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, P.N.; Finfer, P.S.; et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Rose, N.; Matthäus-Krämer, C.; Schwarzkopf, D.; Scherag, A.; Born, S.; Reinhart, K.; Fleischmann-Struzek, C. Association between sepsis incidence and regional socioeconomic deprivation and health care capacity in Germany—An ecological study. BMC Public Health 2021, 21, 1636. [Google Scholar] [CrossRef]
- Iwashyna, T.J.; Cooke, C.; Wunsch, H.; Kahn, J. Population Burden of Long-Term Survivorship After Severe Sepsis in Older Americans. J. Am. Geriatr. Soc. 2012, 60, 1070–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloos, F.; Rüddel, H.; Thomas-Rüddel, D.; Schwarzkopf, D.; Pausch, C.; Harbarth, S.; Schreiber, T.; Gründling, M.; Marshall, J.; Simon, P.; et al. Effect of a multifaceted educational intervention for anti-infectious measures on sepsis mortality: A cluster randomized trial. Intensiv. Care Med. 2017, 43, 1602–1612. [Google Scholar] [CrossRef] [PubMed]
- Evans, I.V.R.; Phillips, G.S.; Alpern, E.R.; Angus, D.C.; Friedrich, M.E.; Kissoon, N.; Lemeshow, S.; Levy, M.M.; Parker, M.M.; Terry, K.M.; et al. Association Between the New York Sepsis Care Mandate and In-Hospital Mortality for Pediatric Sepsis. JAMA 2018, 320, 358–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef]
- Seymour, C.W.; Gesten, F.; Prescott, H.C.; Friedrich, M.E.; Iwashyna, T.J.; Phillips, G.S.; Lemeshow, S.; Osborn, T.; Terry, K.M.; Levy, M.M. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. N. Engl. J. Med. 2017, 376, 2235–2244. [Google Scholar] [CrossRef]
- Liu, V.X.; Fielding-Singh, V.; Greene, J.D.; Baker, J.M.; Iwashyna, T.J.; Bhattacharya, J.; Escobar, G.J. The timing of early antibiotics and hospital mortality in sepsis. Am. J. Respir. Crit. Care Med. 2017, 196, 856–863. [Google Scholar] [CrossRef]
- Marteau, T.M.; Dormandy, E.; Michie, S. A measure of informed choice. Health Expect. 2001, 4, 99–108. [Google Scholar] [CrossRef] [Green Version]
- Mellhammar, L.; Christensson, B.; Linder, A. Public Awareness of sepsis is low in sweden. Open Forum Infect. Dis. 2015, 2, ofv161. [Google Scholar] [CrossRef] [Green Version]
- Park, M.; Kim, K.; Lee, J.H.; Kang, C.; Jo, Y.H.; Kim, D.H.; Kang, K.W.; Lee, S.H.; Park, C.; Kim, J.; et al. Awareness and knowledge of sepsis in the general Korean population: Comparison with the awareness and knowledge of acute myocardial infarction and stroke. Clin. Exp. Emerg Med. 2014, 1, 41–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubulotta, F.M.; Ramsay, G.; Parker, M.M.; Dellinger, R.P.; Levy, M.M.; Poeze, M. An international survey: Public awareness and perception of sepsis. Crit. Care Med. 2009, 37, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Eitze, S.; Fleischmann-Struzek, C.; Betsch, C.; Reinhart, K.; Vaccination60+ Study Group. Determinants of sepsis knowledge: A representative survey of the elderly population in Germany. Crit. Care 2018, 22, 273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Retamero, R.; Galesic, M. Who proficts from visual aids: Overcoming challenges in people’s understanding of risks. Soc. Sci. Med. 2010, 70, 1019–1025. [Google Scholar] [CrossRef] [PubMed]
- Gigerenzer, G.; Gaissmaier, W.; Kurz-Milcke, E.; Schwartz, L.M.; Woloshin, S. Helping doctors and patients make sense of health statistics. Psychol. Sci. Public Interest 2007, 8, 53–96. [Google Scholar] [CrossRef]
- Reyna, V.F.; Nelson, W.L.; Han, P.K.; Dieckmann, N.F. How numeracy influences risk comprehension and medical decision making. Psychol. Bull. 2009, 135, 943–973. [Google Scholar] [CrossRef] [Green Version]
- Wegwarth, O.; Schwartz, L.M.; Woloshin, S.; Gaissmaier, W.; Gigerenzer, G. Do physicians understand cancer screening statistics? A national survey of primary care physicians in the United States. Ann. Intern. Med. 2012, 156, 340–349. [Google Scholar] [CrossRef] [Green Version]
- Wegwarth, O.; Gigerenzer, G. US gynecologists’ estimates and beliefs regarding ovarian cancer screening’s effectiveness 5 years after release of the PLCO evidence. Sci. Rep. 2018, 8, 17181. [Google Scholar] [CrossRef]
- Wegwarth, O.; Widschwendter, M.; Cibula, D.; Sundström, K.; Portuesi, R.; Lein, I.; Rebitschek, F.G. What do European women know about their female cancer risks and cancer screening? A cross-sectional online intervention survey in five European countries. BMJ Open 2018, 8, e023789. [Google Scholar] [CrossRef] [Green Version]
- Hoffrage, U.; Lindsey, S.; Hertwig, R.; Gigerenzer, G. Communicating statistical information. Science 2000, 290, 2261–2262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, L.M.; Woloshin, S.; Welch, H.G. The drug facts box: Providing consumers with simple tabular data on drug benefit and harm. Med. Decis. Mak. 2007, 27, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Wegwarth, O.; Kurzenhauser-Carstens, S.; Gigerenzer, G. Overcoming the knowledge-behavior gap: The effect of evidence-based HPV vaccination leaflets on understanding, intention, and actual vaccination decision. Vaccine 2014, 32, 1388–1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Covey, J. A meta-analysis of the effects of presenting treatment benefits in different formats. Med. Decis. Mak. 2007, 27, 638–654. [Google Scholar] [CrossRef]
- Hoffrage, U.; Gigerenzer, G. Using natural frequencies to improve diagnostic inferences. Acad. Med. 1998, 73, 538–540. [Google Scholar] [CrossRef]
- Naylor, C.D.; Chen, E.; Strauss, B. Measured enthusiasm: Does the method of reporting trial results alter perceptions of therapeutic effectiveness? Ann. Intern. Med. 1992, 117, 916–921. [Google Scholar] [CrossRef]
- Wegwarth, O.; Wagner, G.G.; Gigerenzer, G. Can facts trump unconditional trust? Evidence-based information halves the influence of physicians’ non-evidence-based cancer screening recommendations. PLoS ONE. 2017, 12, e0183024. [Google Scholar] [CrossRef] [Green Version]
- Gigerenzer, G.; Wegwarth, O.; Feufel, M. Misleading communication of risk. BMJ 2010, 341, c4830. [Google Scholar] [CrossRef] [Green Version]
- Gigerenzer, G.; Edwards, A. Simple tools for understanding risks: From innumeracy to insight. BMJ 2003, 327, 741–744. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Retamero, R.; Cokely, E.T. Communicating health risks with visual aids. Curr. Dir. Psychol. Sci. 2013, 22, 392–399. [Google Scholar] [CrossRef]
- Cox, D.S.; Cox, A.D.; Sturm, L.; Zimet, G. Behavioral interventions to increase HPV vaccination acceptability among mothers of young girls. Health Psychol. 2010, 29, 29. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Retamero, R.; Cokely, E.T. Effective communication of risks to young adults: Using message framing and visual aids to increase condom use and STD screening. J. Exp. Psychol Appl. 2011, 17, 270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogt, F.; Marteau, T.M. Perceived effectiveness of stop smoking interventions: Impact of presenting evidence using numbers, visual displays, and different timeframes. Nicotine Tob. Res. 2012, 14, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Gaissmaier, W.; Wegwarth, O.; Skopec, D.; Muller, A.S.; Broschinski, S.; Politi, M.C. Numbers can be worth a thousand pictures: Individual differences in understanding graphical and numerical representations of health-related information. Health Psychol. 2012, 31, 286–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kakkilaya, V.; Groome, L.J.; Platt, D.; Kurepa, D.; Pramanik, A.; Caldito, G.; Conrad, L.; Bocchini, J.A.; Davis, T.C. Use of a visual aid to improve counseling at the threshold of viability. Pediatrics 2011, 128, e1511–e1519. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Retamero, R.; Cokely, E.T. Designing visual aids that promote risk literacy: A systematic review of health research and evidence-based design heuristics. Hum. Factors 2017, 59, 582–627. [Google Scholar] [CrossRef]
- Rodríguez, V.; Andrade, A.D.; García-Retamero, R.; Anam, R.; Rodríguez, R.; Lisigurski, M.; Sharit, J.; Ruiz, J.G. Health literacy, numeracy, and graphical literacy among veterans in primary care and their effect on shared decision making and trust in physicians. J. Health Commun. 2013, 18, 273–289. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Kader, K.; Dew, M.A.; Bhatnagar, M.; Argyropoulos, C.; Karpov, I.; Switzer, G.; Unruh, M.L. Numeracy skills in CKD: Correlates and outcomes. Clin. J. Am. Soc. Nephrol. 2010, 5, 1566–1573. [Google Scholar] [CrossRef] [Green Version]
- Osborn, C.Y.; Cavanaugh, K.; Wallston, K.A.; Rothman, R.L. Self-efficacy links health literacy and numeracy to glycemic control. J. Health Commun. 2010, 15, 146–158. [Google Scholar] [CrossRef]
- Steckelberg, A.; Hulfenhaus, C.; Haastert, B.; Muhlhauser, I. Effect of evidence based risk information on “informed choice” in colorectal cancer screening: Randomised controlled trial. BMJ. 2011, 342, d3193. [Google Scholar] [CrossRef] [Green Version]
- DNEM e.V. Guideline Evidence-Based Health Information. 2016. Available online: https://www.leitlinie-gesundheitsinformation.de/?lang=en (accessed on 24 September 2020).
- Schaeffer, D.; Berens, E.M.; Vogt, D. Health literacy in the German population. Dtsch. Ärzteblatt Int. 2017, 114, 53–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paivio, A.; Rogers, T.B.; Smythe, P.C. Why are pictures easier to recall than words? Psychon. Sci. 1986, 11, 137–138. [Google Scholar] [CrossRef] [Green Version]
- Park, D.C.; Puglisi, J.T.; Sovacool, M. Memory for pictures, words, and spatial location in older adults: Evidence for pictorial superiority. J. Gerontol. 1983, 38, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Shepard, R.N. Recognition memory for words, sentences, andpictures. J. Verbal Learn. Verbal Behav. 1967, 6, 156–163. [Google Scholar] [CrossRef]
- Steckelberg, A.; Meyer, G.; Mühlhauser, I. Correspondence (letter to the editor): Questionnaire should not be used any longer. Dtsch. Ärzteblatt Int. 2017, 114, 330. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Text-Based Format (n = 249) | Graphical Format (n = 251) | |
|---|---|---|
| Age mean (SD) | 55.80 (14.03) | 56.23 (12.92) |
| Female | 123 (49%) | 134 (53%) a |
| Education | ||
| No formal degree | 16 (6%) | 8 (3%) |
| Lower secondary school certificate | 77 (31%) | 79 (32%) |
| Secondary school certificate | 93 (37%) | 104 (41%) |
| A-levels/technical college entrance qualification | 50 (20%) | 35 (14%) |
| University degree | 13 (5%) | 25 (10%) |
| Pre-Existing Condition | Frequency | |
|---|---|---|
| Text-Based Format (n = 174) (%) | Graphical Format (n = 176) (%) | |
| Cancer | ||
| Blood, lymph gland cancer | 22 (13%) | 17 (10%) |
| Breast cancer | 3 (2%) | 7 (4%) |
| Bowel cancer | 9 (5%) | 3 (2%) |
| Urinary bladder, kidney, urinary tract cancer | 5 (3%) | 5 (3%) |
| Lung cancer | 7 (4%) | 6 (3%) |
| Malignant melanoma of the skin | 5 (3%) | 5 (3%) |
| Chronic diseases | ||
| Diabetes mellitus type 1 | 21 (12%) | 15 (9%) |
| Diabetes mellitus type 2 | 27 (16%) | 25 (14%) |
| Chronic heart disease | 22 (13%) | 19 (11%) |
| Chronic lung disease | 20 (11%) | 23 (13%) |
| Chronic renal failure | 19 (11%) | 17 (10%) |
| Chronic liver disease | 16 (9%) | 18 (10%) |
| Chronic neurological diseases | 1 (1%) | 3 (2%) |
| Severe overweight | 6 (3%) | 5 (3%) |
| Autoimmune diseases | ||
| Severe rheumatism | 18 (10%) | 18 (10%) |
| Severe psoriasis | 14 (8%) | 14 (8%) |
| HIV | 24 (14%) | 32 (18%) |
| Other autoimmune diseases or diseases with impaired immune function | 0 | 5 (3%) |
| Therapy that limits immune system function | 109 (63%) | 102 (58%) |
| Informed Choice | Risk and Health Literacy | |||
|---|---|---|---|---|
| Prevention | Early Detection | Prevention | Early Detection | |
| Uninformed/inadequate n (%) | 127 (25%) | 95 (19%) | 90 (18%) | 85 (17%) |
| Informed/adequate n (%) | 373 (75%) | 405 (81%) | 410 (82%) | 415 (83%) |
| Informed Choice | Risk and Health Literacy | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Prevention | Early Detection | Prevention | Early Detection | ||||||||||
| Uninformed | Informed | p | Uninformed | Informed | p | Inadequate | Adequate | p | Inadequate | Adequate | p | ||
| <60 years (n = 235) | text-based (n = 115) | 11 | 104 | 0.005 * | 6 | 109 | 0.027 * | 4 | 111 | 0.108 | 5 | 110 | 0.054 |
| graphical (n = 120) | 28 | 92 | 17 | 103 | 11 | 109 | 14 | 106 | |||||
| ≥60 years (n = 265) | text-based (n = 134) | 43 | 91 | 0.794 | 30 | 104 | 0.097 | 34 | 100 | 0.340 | 28 | 106 | 0.155 |
| graphical (n = 131) | 45 | 86 | 42 | 89 | 41 | 90 | 38 | 93 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Debbeler, L.J.; Pohrt, A.; Fleischmann-Struzek, C.; Schwarzkopf, D.; Born, S.; Reinhart, K.; Wegwarth, O. Text-Based vs. Graphical Information Formats in Sepsis Prevention and Early Detection: A Randomized Controlled Trial on Informed Choice. J. Clin. Med. 2022, 11, 3659. https://doi.org/10.3390/jcm11133659
Debbeler LJ, Pohrt A, Fleischmann-Struzek C, Schwarzkopf D, Born S, Reinhart K, Wegwarth O. Text-Based vs. Graphical Information Formats in Sepsis Prevention and Early Detection: A Randomized Controlled Trial on Informed Choice. Journal of Clinical Medicine. 2022; 11(13):3659. https://doi.org/10.3390/jcm11133659
Chicago/Turabian StyleDebbeler, Luka Johanna, Anne Pohrt, Carolin Fleischmann-Struzek, Daniel Schwarzkopf, Sebastian Born, Konrad Reinhart, and Odette Wegwarth. 2022. "Text-Based vs. Graphical Information Formats in Sepsis Prevention and Early Detection: A Randomized Controlled Trial on Informed Choice" Journal of Clinical Medicine 11, no. 13: 3659. https://doi.org/10.3390/jcm11133659
APA StyleDebbeler, L. J., Pohrt, A., Fleischmann-Struzek, C., Schwarzkopf, D., Born, S., Reinhart, K., & Wegwarth, O. (2022). Text-Based vs. Graphical Information Formats in Sepsis Prevention and Early Detection: A Randomized Controlled Trial on Informed Choice. Journal of Clinical Medicine, 11(13), 3659. https://doi.org/10.3390/jcm11133659