
Long-Term Donor Site Morbidity and Flap Perfusion Following Radial versus Ulnar Forearm Free Flap—A Randomized Controlled Prospective Clinical Trial

 ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Monitoring
- I.
- Hyperspectral perfusion monitoring of:
- (a)
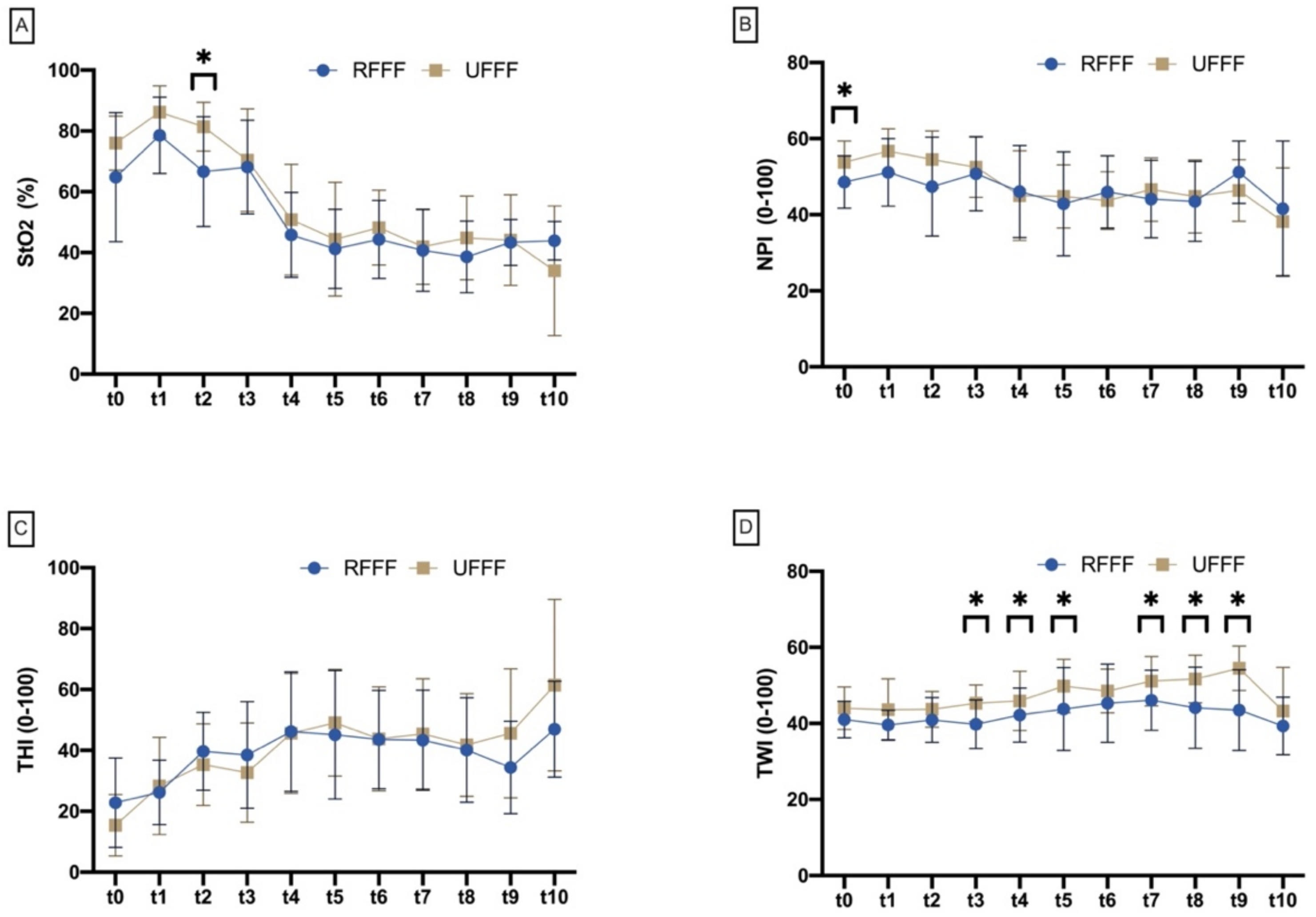
- RFFF and UFFF: The measurement time points of hyperspectral perfusion monitoring were preoperatively/baseline (t0), after flap preparation (t1), after arterial and venous anastomosis (t2), after flap insertion (t3), and at regular intervals until 72 h (t4–t10) after flap insertion. The parameters included were tissue oxygen saturation (StO2), near infrared perfusion index (NPI), tissue hemoglobin index (THI) as a surrogate parameter of microvascular blood flow, as well as tissue water index (TWI). Detailed parameter information was described previously [13].
- (b)
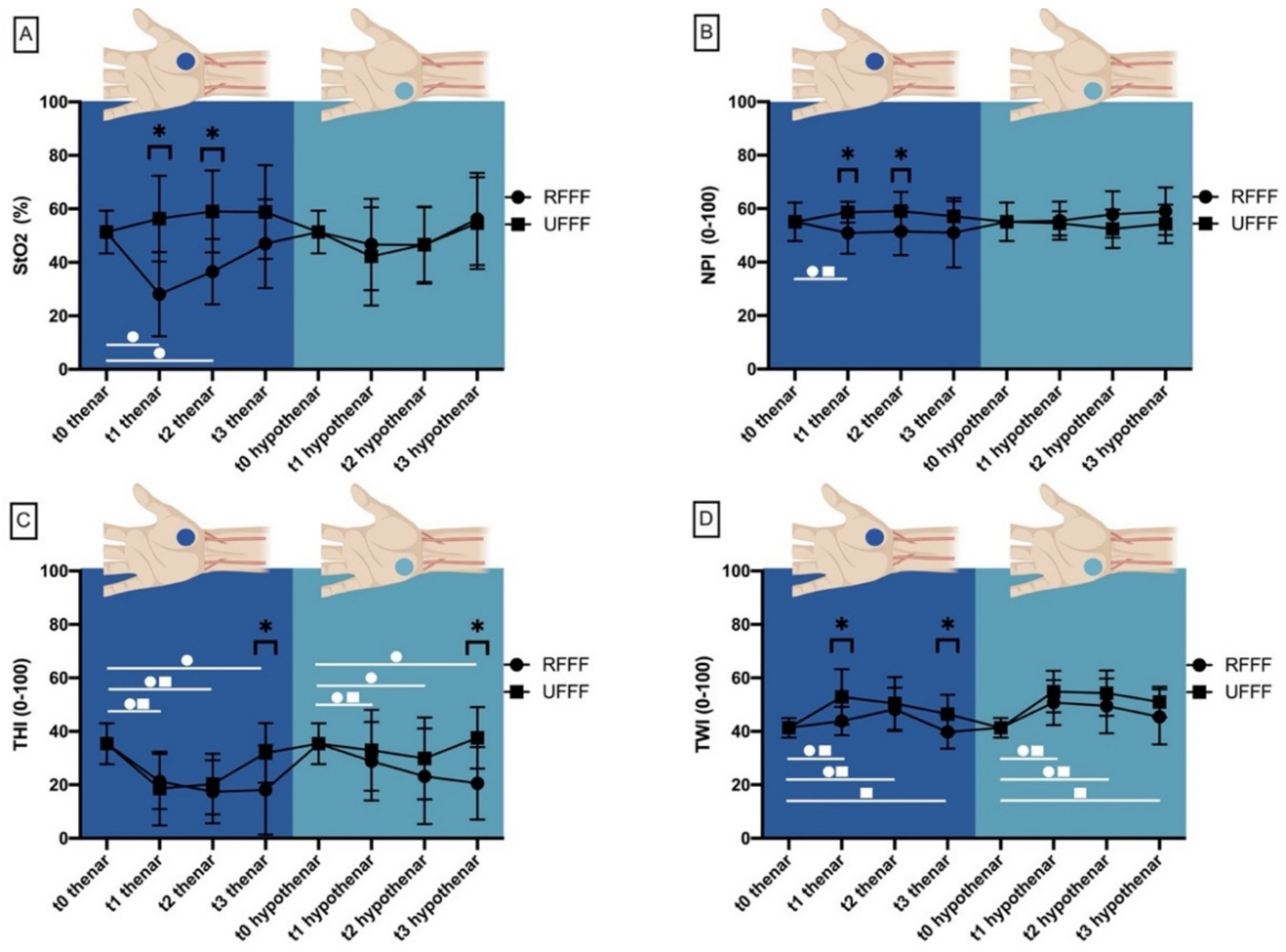
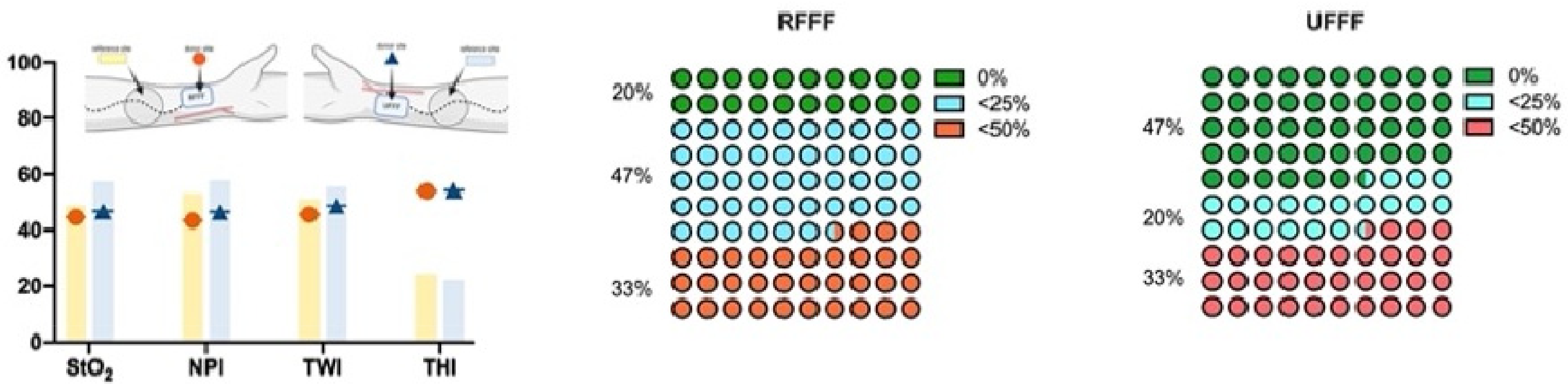
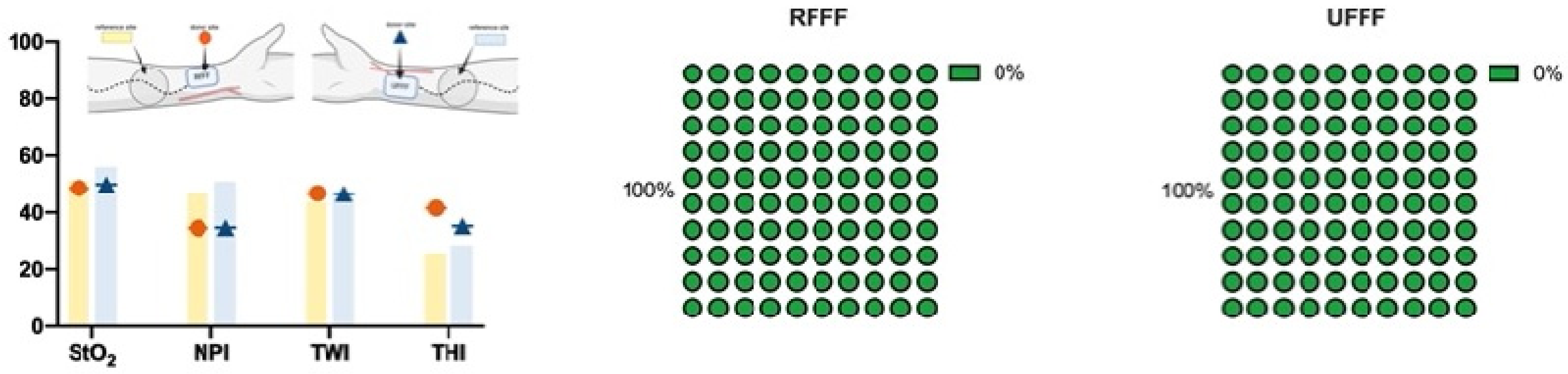
- Thenar and hypothenar eminence: The measurement time points of thenar and hypothenar perfusion monitoring using hyperspectral imaging (HSI) were baseline (prior flap raise) (t0), 10 days after surgery (t1), 4 weeks after surgery (t2), and 6 months after surgery (t3).
- II.
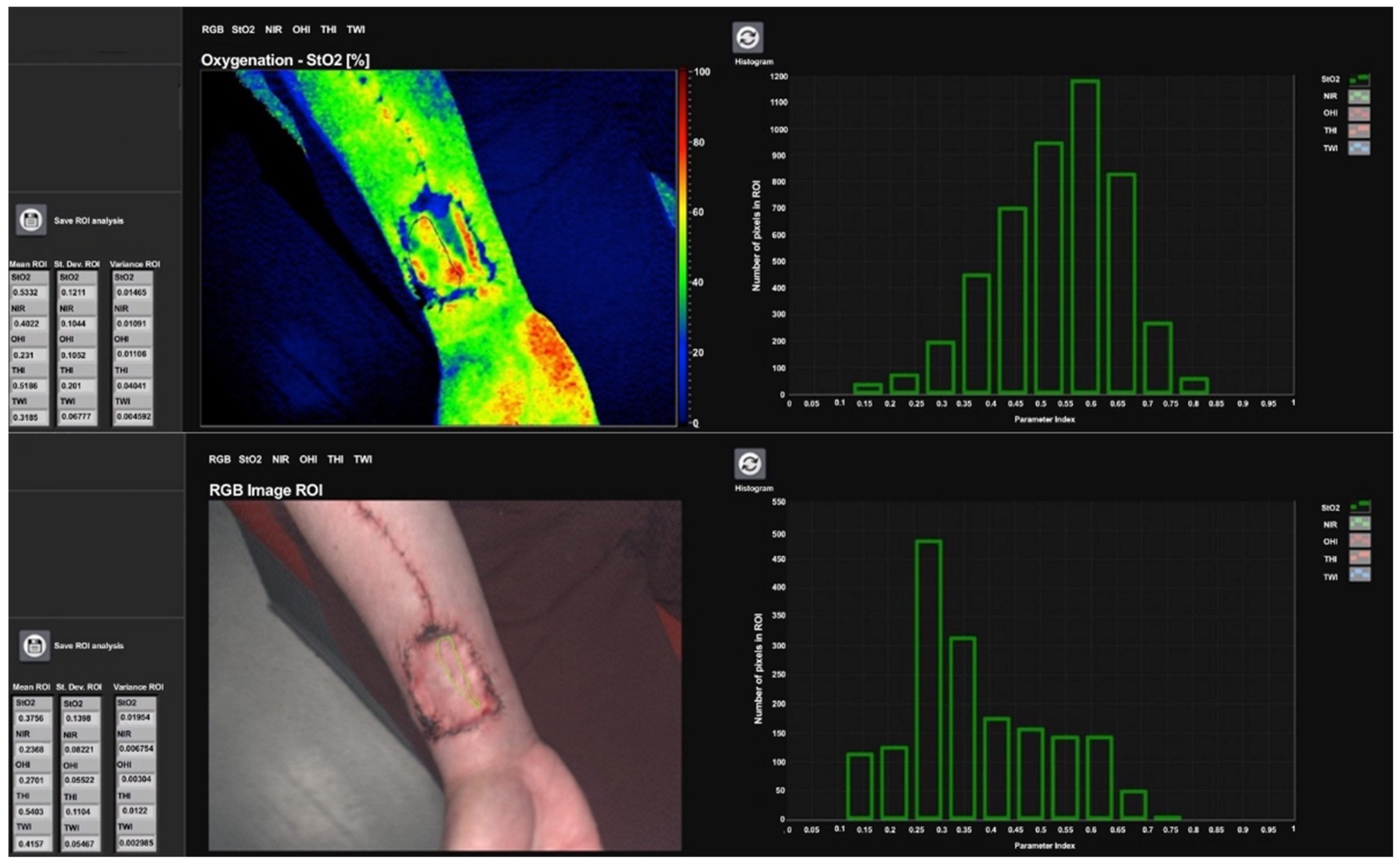
- Quantification of donor site wound healing dynamics via Hyperspectral Imaging
- III.
- Hyperspectral Imaging (HSI)
- IV.
- Clinical Monitoring
2.3. DASH Score
2.4. Scarring, Sensory and Functional Limitations
2.5. Grip Strength and Finger Pinch Strength
2.6. Statistics
3. Results
3.1. Demographics
3.2. Flap Success/Performance
3.2.1. Hyperspectral Flap Perfusion Monitoring
Tissue Oxygenation Saturation (StO2)
Near Infrared Perfusion Index (NPI)
Tissue Hemoglobin Index (THI)
Tissue Water Index (TWI)
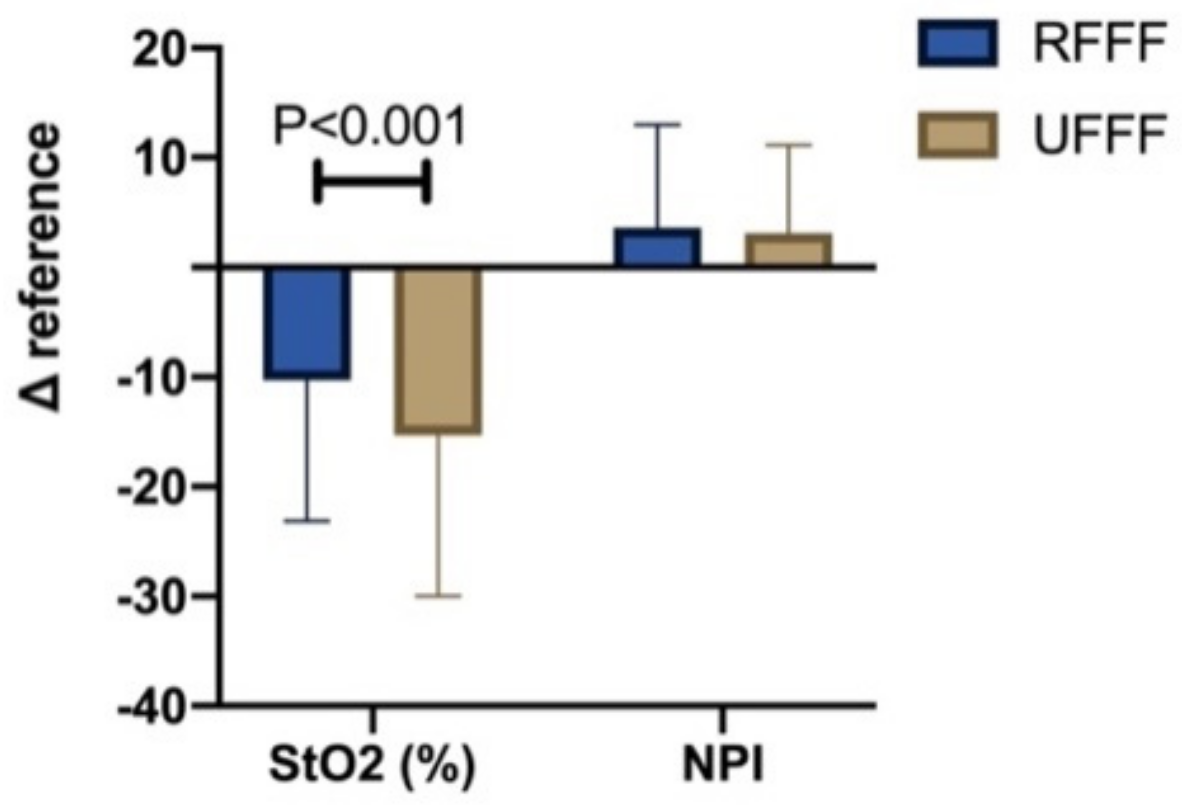
Δ Reference
3.3. Donor Site Morbidity
3.3.1. Thenar and Hypothenar Eminence–HSI Perfusion Monitorin
Tissue Oxygen Saturation (StO2)
Near Infrared Perfusion Index (NPI)
Tissue Hemoglobin Index (THI)
Tissue Water Index (TWI)
3.3.2. Quantification of Wound Healing Dynamics
Baseline (t0)
Ten Days after Surgery (t1)
Four Weeks after Surgery (t2)
Six Months after Surgery (t3)
3.3.3. Quality of Life Analysis
3.3.4. Grip and Finger Pinch Strength
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thiem, D.G.E.; Frick, R.W.; Goetze, E.; Gielisch, M.; Al-Nawas, B.; Kammerer, P.W. Hyperspectral analysis for perioperative perfusion monitoring-a clinical feasibility study on free and pedicled flaps. Clin. Oral Investig. 2020, 25, 933–945. [Google Scholar] [CrossRef] [PubMed]
- Hölzle, F.; Wolff, K.D.; Mohr, C. Reconstructive oral and maxillofacial surgery. Dtsch. Arztebl. Int. 2008, 105, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Lovie, M.J.; Duncan, G.M.; Glasson, D.W. The ulnar artery forearm free flap. Br. J. Plast. Surg. 1984, 37, 486–492. [Google Scholar] [CrossRef]
- Soutar, D.S.; Scheker, L.R.; Tanner, N.S.B.; McGregor, I.A. The radial forearm flap: A versatile method for intra-oral reconstruction. Br. J. Plast. Surg. 1983, 36, 1–8. [Google Scholar] [CrossRef]
- Loeffelbein, D.J.; Al-Benna, S.; Steinstrasser, L.; Satanovskij, R.M.; Rohleder, N.H.; Mucke, T.; Wolff, K.D.; Kesting, M.R. Reduction of donor site morbidity of free radial forearm flaps: What level of evidence is available? Eplasty 2012, 12, e9. [Google Scholar] [PubMed]
- Bertino, G.; Lepenne, Y.; Tinelli, C.; Giordano, L.; Cacciola, S.; Di Santo, D.; Occhini, A.; Benazzo, M.; Bussi, M. Radial vs ulnar forearm flap: A preliminary study of donor site morbidity. Acta Otorhinolaryngol. Ital. 2019, 39, 322–328. [Google Scholar] [CrossRef]
- Heimes, D.; Becker, P.; Thiem, D.G.E.; Kuchen, R.; Kyyak, S.; Kammerer, P.W. Is hyperspectral imaging suitable for assessing collateral circulation prior radial forearm free flap harvesting? Comparison of hyperspectral imaging and conventional allen’s test. J. Pers. Med. 2021, 11, 531. [Google Scholar] [CrossRef] [PubMed]
- Sieg, P.; Bierwolf, S. Ulnar versus radial forearm flap in head and neck reconstruction: An experimental and clinical study. Head Neck 2001, 23, 967–971. [Google Scholar] [CrossRef]
- Sieg, P.; Dericioglu, M.; Hansmann, C.; Jacobsen, H.C.; Trenkle, T.; Hakim, S.G. Long-term functional donor site morbidity after ulnar forearm flap harvest. Head Neck 2012, 34, 1312–1316. [Google Scholar] [CrossRef]
- Hekner, D.D.; Abbink, J.H.; van Es, R.J.; Rosenberg, A.; Koole, R.; Van Cann, E.M. Donor-site morbidity of the radial forearm free flap versus the ulnar forearm free flap. Plast. Reconstr. Surg. 2013, 132, 387–393. [Google Scholar] [CrossRef]
- Halama, D.; Dreilich, R.; Lethaus, B.; Bartella, A.; Pausch, N.C. Donor-site morbidity after harvesting of radial forearm free flaps-comparison of vacuum-assisted closure with conventional wound care: A randomized controlled trial. J. Cranio-Maxillofac Surg. 2019, 47, 1980–1985. [Google Scholar] [CrossRef]
- Shimada, K.; Ojima, Y.; Ida, Y.; Komiya, T.; Matsumura, H. Negative-pressure wound therapy for donor-site closure in radial forearm free flap: A systematic review and meta-analysis. Int. Wound J. 2022, 19, 316–325. [Google Scholar] [CrossRef]
- Thiem, D.G.E.; Romer, P.; Blatt, S.; Al-Nawas, B.; Kammerer, P.W. New approach to the old challenge of free flap monitoring-hyperspectral imaging outperforms clinical assessment by earlier detection of perfusion failure. J. Pers. Med. 2021, 11, 1101. [Google Scholar] [CrossRef]
- Holmer, A.; Marotz, J.; Wahl, P.; Dau, M.; Kammerer, P.W. Hyperspectral imaging in perfusion and wound diagnostics—Methods and algorithms for the determination of tissue parameters. Biomed. Tech. 2018, 63, 547–556. [Google Scholar] [CrossRef]
- Bickler, P.E.; Feiner, J.R.; Rollins, M.D. Factors affecting the performance of 5 cerebral oximeters during hypoxia in healthy volunteers. Anesth. Analg. 2013, 117, 813–823. [Google Scholar] [CrossRef]
- Gummesson, C.; Atroshi, I.; Ekdahl, C. The disabilities of the arm, shoulder and hand (dash) outcome questionnaire: Longitudinal construct validity and measuring self-rated health change after surgery. BMC Musculoskelet. Disord. 2003, 4, 11. [Google Scholar] [CrossRef] [Green Version]
- Franchignoni, F.; Vercelli, S.; Giordano, A.; Sartorio, F.; Bravini, E.; Ferriero, G. Minimal clinically important difference of the disabilities of the arm, shoulder and hand outcome measure (dash) and its shortened version (quickdash). J. Orthop. Sports Phys. Ther. 2014, 44, 30–39. [Google Scholar] [CrossRef] [Green Version]
- Tonks, A.M.; Lawrence, J.; Lovie, M.J. Comparison of ulnar and radial arterial blood-flow at the wrist. J. Hand Surg. Br. 1995, 20, 240–242. [Google Scholar] [CrossRef]
- Keen, J.A. A study of the arterial variations in the limbs, with special reference to symmetry of vascular patterns. Am. J. Anat. 1961, 108, 245–261. [Google Scholar] [CrossRef]
- Coleman, S.S.; Anson, B.J. Arterial patterns in the hand based upon a study of 650 specimens. Surg. Gynecol. Obstet. 1961, 113, 409–424. [Google Scholar] [CrossRef]
- De Vicente, J.C.; Espinosa, C.; Rua-Gonzalvez, L.; Rodriguez-Santamarta, T.; Alonso, M. Hand perfusion following radial or ulnar forearm free flap harvest for oral cavity reconstruction: A prospective study. Int. J. Oral. Maxillofac. Surg. 2020, 49, 1402–1407. [Google Scholar] [CrossRef] [PubMed]
- Patsalis, T.; Hoffmeister, H.E.; Seboldt, H. Arterial dominance of the hand. Handchir. Mikrochir. Plast. Chir. 1997, 29, 247–250. [Google Scholar] [PubMed]
- Harding, K.; Queen, D. Education and improved clinical outcomes. Int. Wound J. 2017, 14, 299. [Google Scholar] [CrossRef] [PubMed]
- Chio, E.G.; Agrawal, A. A randomized, prospective, controlled study of forearm donor site healing when using a vacuum dressing. Otolaryngol. Head Neck Surg. 2010, 142, 174–178. [Google Scholar] [CrossRef]
- Schwarzer, C.; Mucke, T.; Wolff, K.D.; Loeffelbein, D.J.; Rau, A. Donor site morbidity and flap perfusion of subfascial and suprafascial radial forearm flaps: A randomized prospective clinical comparison trial. J. Cranio-Maxillofac. Surg. 2016, 44, 1299–1304. [Google Scholar] [CrossRef]
- Riecke, B.; Kohlmeier, C.; Assaf, A.T.; Wikner, J.; Drabik, A.; Catala-Lehnen, P.; Heiland, M.; Rendenbach, C. Prospective biomechanical evaluation of donor site morbidity after radial forearm free flap. Br. J. Oral. Maxillofac. Surg. 2016, 54, 181–186. [Google Scholar] [CrossRef]
- Yalamanchili, S.; Rotatori, R.M.; Ovalle, F.; Gobble, R. Radial Forearm Flap Donor Site Morbidity: A Systematic Review. J. Aesthet. Reconstr. Surg. 2020, 6, 9. [Google Scholar]
- Molteni, G.; Gazzini, L.; Bisi, N.; Nocini, R.; Ferri, A.; Bellanti, L.; Marchioni, D. Donor site aesthetic and functional outcomes of radial forearm free flap: A comparison between full-thickness and split-thickness skin grafts. Eur. J. Plast. Surg. 2022, 1–8. [Google Scholar] [CrossRef]
- Brown, M.T.; Couch, M.E.; Huchton, D.M. Assessment of donor-site functional morbidity from radial forearm fasciocutaneous free flap harvest. Arch. Otolaryngol. Head Neck Surg. 1999, 125, 1371–1374. [Google Scholar] [CrossRef] [Green Version]
- De Witt, C.A.; de Bree, R.; Verdonck-de Leeuw, I.M.; Quak, J.J.; Leemans, C.R. Donor site morbidity of the fasciocutaneous radial forearm flap: What does the patient really bother? Eur. Arch. Oto-Rhino-Laryngol. 2007, 264, 929–934. [Google Scholar] [CrossRef] [Green Version]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Strongly Disagree | Somewhat Disagree | Neither Agree nor Disagree | Somewhat Agree | Strongly Agree | |
|---|---|---|---|---|---|
| 1. Are you satisfied with the shape of the scar ar your forearm? | 1 | 2 | 3 | 4 | 5 |
| 2. Are you satisfied with the size of the scar at your forearm? | 1 | 2 | 3 | 4 | 5 |
| 3. Are you satisfied with the color of the scar at your forearm? | 1 | 2 | 3 | 4 | 5 |
| 4. Are you satisfied with the thickness of the scar at your forearm? | 1 | 2 | 3 | 4 | 5 |
| 5. Do you feel any sensory disturbances in the area of the donor sites’ palm since surgery? | 1 | 2 | 3 | 4 | 5 |
| 6. If yes, does it limit your everyday life? | 1 | 2 | 3 | 4 | 5 |
| 7. Do you experience any loss of grip strength on the donor site at this time? | 1 | 2 | 3 | 4 | 5 |
| 8. If yes, does it limit your everyday life? | 1 | 2 | 3 | 4 | 5 |
| Total | RFFF | UFFF | |
|---|---|---|---|
| N | 30 | 15 | 15 |
| Age | 66.7 ± 10.4 | 67.6 ± 11.7 | 65.9 ± 9.3 |
| Gender | |||
| Male | 17 (57%) | 8 (53%) | 9 (60%) |
| Female | 13 (43%) | 7 (47%) | 6 (40%) |
| Tumor site | |||
| Tongue | 5 (17%) | 2 (13%) | 3 (20%) |
| Mouth floor | 7 (23%) | 3 (20%) | 4 (27%) |
| Buccal | 8 (27%) | 6 (40%) | 2 (13%) |
| Hard palate | 1 (3%) | 0 | 1 (6%) |
| Soft palate | 1 (3%) | 0 | 1 (6%) |
| Alveolar crest | 8 (27%) | 4 (27%) | 4 (27%) |
| Neck Dissection | |||
| Bilateral | 27 (90%) | 14 (93%) | 13 (87%) |
| Ipsilateral | 2 (7%) | 0 | 2 (13%) |
| Contralateral | 1 (3%) (2nd cancer) | 1 (7%) (2nd cancer) | 0 |
| Adjuvant radiotherapy | |||
| Yes | 20 (67%) | 11 (73%) | 9 (60%) |
| No | 10 (33%) | 4 (27%) | 6 (40%) |
| Recipient vessel (artery) | |||
| Superior thyroid | 22 (73%) | 11 (73%) | 11 (73%) |
| Lingual | 4 (13%) | 2 (13%) | 2 (13%) |
| External carotid | 2 (7%) | 1 (7%) | 1 (7%) |
| Facial | 2 (7%) | 1 (7%) | 1 (7%) |
| Recipient vessel (vein) | |||
| Internal jugular vein | 30 (100%) | 15 (50%) | 15 (50%) |
| Flap size (cm2) | 34.3 ± 12.7 | 37.6 ± 16.4 | 30.90 ± 6.4 |
| Duration of surgery (minutes) | 482 ± 102 | 494 ± 122 | 467 ± 80 |
| Total | RFFF | UFFF | ||||
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Δ DASH 1–2 (%); p-Value | Mean ± SD | Δ DASH 1–2 (%); p-Value | p-Value | |
| DASH 1 4 weeks | 38 ± 22 | 43 ± 19 | −30%; 0.006 * | 33 ± 24 | −3%; 0.865 | 0.191 |
| 0.005 * | ||||||
| DASH 2 6 months | 30 ± 19 | 29 ± 15 | 32 ± 24 | 0.803 | ||
| Likert | ||||||
| Scar | 3 ± 1 | 3 ± 1 | 4 ± 1 | 0.766 | ||
| Sensitivity | 3 ± 1 | 3 ± 1 | 3 ± 1 | 0.120 | ||
| Handicap by < sensitivity | 3 ± 1 | 2 ± 1 | 3 ± 1 | 0.432 | ||
| Grip force | 3 ± 1 | 3 ± 1 | 3 ± 1 | 0.266 | ||
| Handicap by < grip force | 3 ± 1 | 3 ± 1 | 3 ± 1 | 0.413 | ||
| Grip Force | Total | RFFF | UFFF | RFFF vs. UFFF | |||
|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | p-Value | Mean ± SD | p-Value | p-Value | ||
 | Donor presurgical | 27.5 ± 8.9 | 23.9 ± 8.3 | 30.9 ± 8.2 | 0.058 | ||
| Donor 4 weeks | 18.3 ± 8.5 | 17.8 ± 9.9 | 0.019 * | 18.7 ± 7.3 | 0.003 * | 0.830 | |
| Donor 6 months | 25.3 ± 9.1 | 23.9 ± 9.1 | 0.424 | 26.8 ± 9.3 | 0.008 * | 0.562 | |
| Control pre surgical | 29.3 ± 8.6 | 28.1 ± 8.3 | 30.4 ± 9.1 | 0.402 | |||
| Control 4 weeks | 29.9 ± 9.4 | 28.7 ± 10.6 | 0.807 | 31.2 ± 8.5 | 0.279 | 0.650 | |
| Control 6 months | 30.9 ± 7.5 | 29.2 ± 8.2 | 0.594 | 32.6 ± 6.7 | 0.894 | 0.193 | |
| RFFF Surgery |  |  |  |  |  | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre Surgery | 4 we. | 6 mo. | Pre Surgery | 4 we. | 6 mo. | Pre Surgery | 4 we. | 6 mo. | Pre Surgery | 4 we. | 6 mo. | Pre Surgery | 4 we. | 6 mo. | |
| Mean ± SD | 4.1 ± 0.7 | 3.7 ± 0.8 | 4.1 ± 0.8 | 3.7 ± 1.0 | 3.1 ± 1.2 | 3.9 ± 0.8 | 3.8 ± 1.2 | 2.7 ± 1.3 | 3.2 ± 1.0 | 2.7 ± 1.1 | 2.3 ± 1.3 | 2.4 ± 1.0 | 1.9 ± 0.9 | 1.5 ± 0.8 | 1.5 ± 0.6 |
| p-value | 0.18 | 0.012 * | 0.068 | 0.713 | 0.008 * | 0.175 | 0.715 | 0.021 * | 0.015 * | 0.893 | 0.075 | 0.057 | 0.917 | 0.136 | 0.014 * |
| Mean ± SD | 4.5 ± 0.1 | 4.4 ± 0.4 | 4.5 ± 0 | 3.8 ± 0.7 | 4.2 ± 0.5 | 4.2 ± 0.4 | 3.9 ± 0.8 | 3.7 ± 1.0 | 4.1 ± 0.8 | 2.8 ± 1.0 | 2.9 ± 1.1 | 2.9 ± 0.9 | 1.9 ± 0.7 | 1.8 ± 0.8 | 1.8 ± 0.6 |
| RFFF Control |  |  |  |  |  | ||||||||||
| UFFF Surgery | | | | | | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre Surgery | 4 we. | 6 mo. | Pre Surgery | 4 we. | 6 mo. | Pre Surgery | 4 we. | 6 mo. | Pre Surgery | 4 we. | 6 mo. | Pre Surgery | 4 we. | 6 mo. | |
| Mean ±SD | 4.4 ± 0.3 | 3.8 ± 0.9 | 4.4 ± 0.4 | 4.4 ± 0.4 | 2.9 ± 1.1 | 3.9 ± 0.8 | 3.9 ± 0.6 | 2.4 ± 0.9 | 3.7 ± 0.9 | 2.9 ± 0.9 | 1.5 ± 0.6 | 2.9 ± 1.0 | 2.1 ± 1.0 | 1.1 ± 0.7 | 2.0 ± 0.9 |
| p-value | 0.180 | 0.011 * | 0.317 | 0.216 | 0.002 * | 0.043 * | 0.811 | <0.001 * | 0.232 | 0.430 | <0.001 * | 0.050 * | 0.388 | 0.005 * | 0.123 |
| Mean ±SD | 4.3 ± 0.5 | 4.4 ± 0.4 | 4.5 ± 0.2 | 4.2 ± 0.5 | 4.1 ± 0.7 | 4.4 ± 0.4 | 3.9 ± 0.8 | 3.9 ± 1.0 | 4.0 ± 0.8 | 3.0 ± 1.1 | 3.3 ± 1.0 | 3.2 ± 0.9 | 2.2 ± 1.2 | 2.0 ± 1.0 | 2.4 ± 1.0 |
| UFFF Control | | | | | | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thiem, D.G.E.; Siegberg, F.; Römer, P.; Blatt, S.; Pabst, A.; Heimes, D.; Al-Nawas, B.; Kämmerer, P.W. Long-Term Donor Site Morbidity and Flap Perfusion Following Radial versus Ulnar Forearm Free Flap—A Randomized Controlled Prospective Clinical Trial. J. Clin. Med. 2022, 11, 3601. https://doi.org/10.3390/jcm11133601
Thiem DGE, Siegberg F, Römer P, Blatt S, Pabst A, Heimes D, Al-Nawas B, Kämmerer PW. Long-Term Donor Site Morbidity and Flap Perfusion Following Radial versus Ulnar Forearm Free Flap—A Randomized Controlled Prospective Clinical Trial. Journal of Clinical Medicine. 2022; 11(13):3601. https://doi.org/10.3390/jcm11133601
Chicago/Turabian StyleThiem, Daniel G. E., Fabia Siegberg, Paul Römer, Sebastian Blatt, Andreas Pabst, Diana Heimes, Bilal Al-Nawas, and Peer W. Kämmerer. 2022. "Long-Term Donor Site Morbidity and Flap Perfusion Following Radial versus Ulnar Forearm Free Flap—A Randomized Controlled Prospective Clinical Trial" Journal of Clinical Medicine 11, no. 13: 3601. https://doi.org/10.3390/jcm11133601
APA StyleThiem, D. G. E., Siegberg, F., Römer, P., Blatt, S., Pabst, A., Heimes, D., Al-Nawas, B., & Kämmerer, P. W. (2022). Long-Term Donor Site Morbidity and Flap Perfusion Following Radial versus Ulnar Forearm Free Flap—A Randomized Controlled Prospective Clinical Trial. Journal of Clinical Medicine, 11(13), 3601. https://doi.org/10.3390/jcm11133601