
Effects of Butyrate Supplementation on Inflammation and Kidney Parameters in Type 1 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Procedures
2.2. Endpoints
2.3. Analyses
2.4. Statistical Analysis
3. Results
3.1. Baseline
3.2. Changes in Fecal and Circulating Markers of Inflammation
3.3. Changes in Kidney Parameters, HbA1c and Metabolites
3.4. Changes in Gastrointestinal Symptoms
3.5. Supplementary Analysis
3.6. Safety
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Winther, S.A.; Henriksen, P.; Vogt, J.K.; Hansen, T.H.; Ahonen, L.; Suvitaival, T.; Zobel, E.H.; Frimodt-Møller, M.; Hansen, T.W.; Hansen, T.; et al. Gut microbiota profile and selected plasma metabolites in type 1 diabetes without and with stratification by albuminuria. Diabetologia 2020, 63, 2713–2724. [Google Scholar] [CrossRef] [PubMed]
- Lassenius, M.I.; Fogarty, C.L.; Blaut, M.; Haimila, K.; Riittinen, L.; Paju, A.; Kirveskari, J.; Jaervelae, J.; Ahola, A.J.; Gordin, D.; et al. Intestinal alkaline phosphatase at the crossroad of intestinal health and disease—A putative role in type 1 diabetes. J. Intern. Med. 2017, 281, 586–600. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.; Wang, S.; Nagpal, R.; Miller, B.; Singh, R.; Taraphder, S.; Yadav, H. Probiotics and Prebiotics for the Amelioration of Type 1 Diabetes: Present and Future Perspectives. Microorganisms 2019, 7, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, H.; Sun, L.; Zhang, S.; Zhao, X.; Gang, X.; Wang, G. Evaluating the Causal Role of Gut Microbiota in Type 1 Diabetes and Its Possible Pathogenic Mechanisms. Front. Endocrinol. 2020, 11, 125. [Google Scholar] [CrossRef]
- Harbison, J.E.; Roth-Schulze, A.J.; Giles, L.; Tran, C.D.; Ngui, K.M.; Penno, M.; Thomson, R.L.; Wentworth, J.M.; Colman, P.G.; Craig, M.E.; et al. Gut microbiome dysbiosis and increased intestinal permeability in children with islet autoimmunity and type 1 diabetes: A prospective cohort study. Pediatr. Diabetes 2019, 20, 574–583. [Google Scholar] [CrossRef]
- Vinolo, M.A.; Rodrigues, H.G.; Nachbar, R.T.; Curi, R. Regulation of inflammation by short chain fatty acids. Nutrients 2011, 3, 858–876. [Google Scholar] [CrossRef] [Green Version]
- Vinolo, M.A.R.; Rodrigues, H.G.; Hatanaka, E.; Sato, F.T.; Sampaio, S.C.; Curi, R. Suppressive effect of short-chain fatty acids on production of proinflammatory mediators by neutrophils. J. Nutr. Biochem. 2011, 22, 849–855. [Google Scholar] [CrossRef]
- Tilg, H.; Moschen, A.R. Microbiota and diabetes: An evolving relationship. Gut 2014, 63, 1513–1521. [Google Scholar] [CrossRef]
- Liu, H.; Wang, J.; He, T.; Becker, S.; Zhang, G.; Li, D.; Ma, X. Butyrate: A Double-Edged Sword for Health? Adv Nutr. 2018, 9, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Melo, A.D.B.; Silveira, H.; Bortoluzzi, C.; Lara, L.; Garbossa, C.; Preis, G.; Costa, L.; Rostagno, M. Intestinal alkaline phosphatase and sodium butyrate may be beneficial in attenuating LPS-induced intestinal inflammation. Genet. Mol. Res. 2016, 15, gmr15048875. [Google Scholar] [CrossRef]
- Lallès, J.-P. Intestinal alkaline phosphatase: Multiple biological roles in maintenance of intestinal homeostasis and modulation by diet. Nutr. Rev. 2010, 68, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Lallès, J.-P. Recent advances in intestinal alkaline phosphatase, inflammation, and nutrition. Nutr. Rev. 2019, 77, 710–724. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.S.; Wang, J.; Yannie, P.J.; Ghosh, S. Intestinal Barrier Dysfunction, LPS Translocation, and Disease Development. J. Endocr. Soc. 2020, 4, bvz039. [Google Scholar] [CrossRef] [Green Version]
- Gutzeit, C.; Magri, G.; Cerutti, A. Intestinal IgA production and its role in host-microbe interaction. Immunol. Rev. 2014, 260, 76–85. [Google Scholar] [CrossRef]
- Bilski, J.; Mazur-Bialy, A.; Wojcik, D.; Zahradnik-Bilska, J.; Brzozowski, B.; Magierowski, M.; Mach, T.; Magierowska, K.; Brzozowski, T. The Role of Intestinal Alkaline Phosphatase in Inflammatory Disorders of Gastrointestinal Tract. Mediat. Inflamm. 2017, 2017, 9074601. [Google Scholar] [CrossRef] [PubMed]
- Nighot, M.; Rawat, M.; Al-Sadi, R.; Castillo, E.; Nighot, P.; Ma, T.Y. Lipopolysaccharide-Induced Increase in Intestinal Permeability Is Mediated by TAK-1 Activation of IKK and MLCK/MYLK Gene. Am. J. Pathol. 2019, 189, 797–812. [Google Scholar] [CrossRef] [PubMed]
- Ramezani, A.; Raj, D.S. The gut microbiome, kidney disease, and targeted interventions. J. Am. Soc. Nephrol. 2014, 25, 657–670. [Google Scholar] [CrossRef] [Green Version]
- Lehto, M.; Groop, P.-H. The Gut-Kidney Axis: Putative Interconnections between Gastrointestinal and Renal Disorders. Front. Endocrinol. 2018, 9, 553. [Google Scholar] [CrossRef]
- Gonzalez, A.; Krieg, R.; Massey, H.D.; Carl, D.; Ghosh, S.; Gehr, T.W.B.; Ghosh, S.S. Sodium butyrate ameliorates insulin resistance and renal failure in CKD rats by modulating intestinal permeability and mucin expression. Nephrol. Dial. Transplant. 2018, 34, 783–794. [Google Scholar] [CrossRef]
- Andrade-Oliveira, V.; Amano, M.; Correa-Costa, M.; Castoldi, A.; Felizardo, R.; De Almeida, D.C.; Bassi, J.; Vieira, P.; Hiyane, M.I.; Rodas, A.C.; et al. Gut Bacteria Products Prevent AKI Induced by Ischemia-Reperfusion. J. Am. Soc. Nephrol. 2015, 26, 1877–1888. [Google Scholar] [CrossRef]
- Yang, H.; Zhang, Z.; Peng, R.; Zhang, L.; Liu, H.; Wang, X.; Tian, Y.; Sun, Y. RNA-Seq analysis reveals critical transcriptome changes caused by sodium butyrate in DN mouse models. Biosci. Rep. 2021, 41, bsr20203005. [Google Scholar] [CrossRef] [PubMed]
- Borycka-Kiciak, K.; Banasiewicz, T.; Rydzewska, G. Butyric acid—A well-known molecule revisited. Gastroenterol. Rev. 2017, 2, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Vernero, M.; De Blasio, F.; Ribaldone, D.; Bugianesi, E.; Pellicano, R.; Saracco, G.; Astegiano, M.; Caviglia, G. The Usefulness of Microencapsulated Sodium Butyrate Add-on Therapy in Maintaining Remission in Patients with Ulcerative Colitis: A Prospective Observational Study. J. Clin. Med. 2020, 9, 3941. [Google Scholar] [CrossRef] [PubMed]
- Roshanravan, N.; Mahdavi, R.; Alizadeh, E.; Jafarabadi, M.A.; Hedayati, M.; Ghavami, A.; Alipour, S.; Alamdari, N.M.; Barati, M.; Ostadrahimi, A. Effect of Butyrate and Inulin Supplementation on Glycemic Status, Lipid Profile and Glucagon-Like Peptide 1 Level in Patients with Type 2 Diabetes: A Randomized Double-Blind, Placebo-Controlled Trial. Horm. Metab. Res. 2017, 49, 886–891. [Google Scholar] [CrossRef]
- Ahonen, L.; Jäntti, S.; Suvitaival, T.; Theilade, S.; Risz, C.; Kostiainen, R.; Rossing, P.; Orešič, M.; Hyötyläinen, T. Targeted Clinical Metabolite Profiling Platform for the Stratification of Diabetic Patients. Metabolites 2019, 9, 184. [Google Scholar] [CrossRef] [Green Version]
- Gjymishka, A.; Coman, R.M.; Brusko, T.M.; Glover, S.C. Influence of host immunoregulatory genes, ER stress and gut microbiota on the shared pathogenesis of inflammatory bowel disease and Type 1 diabetes. Immunotherapy 2013, 5, 1357–1366. [Google Scholar] [CrossRef] [Green Version]
- Lind, M.; Svensson, A.-M.; Kosiborod, M.; Gudbjörnsdottir, S.; Pivodic, A.; Wedel, H.; Dahlqvist, S.; Clements, M.; Rosengren, A. glycemic control and excess mortality in type 1 diabetes. N. Engl. J. Med. 2014, 371, 1972–1982. [Google Scholar] [CrossRef]
- Gandhi, S.; Narulak, N.; Marshall, J.K.; Farkouh, M. Are patients with inflammatory bowel disease at increased risk of coronary artery disease? Am. J. Med. 2012, 125, 956–962. [Google Scholar] [CrossRef]
- Penny, H.A.; Leeds, J.S.; Kurien, M.; Averginos, A.; Hopper, A.D.; Hadjivassiliou, M.; Tesfaye, S.; Sanders, D.S. The relationship between inflammatory bowel disease and type 1 diabetes mellitus: A study of relative prevalence in comparison with population controls. J. Gastrointest. Liver Dis. 2015, 24, 125–126. [Google Scholar]
- Wong, J.M.W.; de Souza, R.; Kendall, C.W.C.; Emam, A.; Jenkins, D.J.A. Colonic Health: Fermentation and Short Chain Fatty Acids. J. Clin. Gastroenterol. 2006, 40, 235–243. [Google Scholar] [CrossRef]
- McOrist, A.L.; Miller, R.B.; Bird, A.R.; Keogh, J.; Noakes, M.; Topping, D.L.; Conlon, M.A. Fecal butyrate levels vary widely among individuals but are usually increased by a diet high in resistant starch. J. Nutr. 2011, 141, 883–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Groot, P.F.; Nikolic, T.; Imangaliyev, S.; Bekkering, S.; Duinkerken, G.; Keij, F.M.; Herrema, H.; Winkelmeijer, M.; Kroon, J.; Levin, E.; et al. Oral butyrate does not affect innate immunity and islet autoimmunity in individuals with longstanding type 1 diabetes: A randomised controlled trial. Diabetologia 2020, 63, 597–610. [Google Scholar] [CrossRef] [PubMed]
- Poullis, A.; Foster, R.; Mendall, M.A. Proton pump inhibitors are associated with elevation of faecal calprotectin and may affect specificity. Eur. J. Gastroenterol. Hepatol. 2003, 15, 573–574. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Esteve, E.; Tremaroli, V.; Khan, M.T.; Caesar, R.; Mannerås-Holm, L.; Ståhlman, M.; Olsson, L.M.; Serino, M.; Planas-Fèlix, M.; et al. Metformin alters the gut microbiome of individuals with treatment-naive type 2 diabetes, contributing to the therapeutic effects of the drug. Nat. Med. 2017, 23, 850–858. [Google Scholar] [CrossRef]
- Vieira-Silva, S.; Falony, G.; Belda, E.; Nielsen, T.; Aron-Wisnewsky, J.; Chakaroun, R.; Forslund, S.K.; Assmann, K.; Valles-Colomer, M.; Nguyen, T.T.D.; et al. Statin therapy is associated with lower prevalence of gut microbiota dysbiosis. Nature 2020, 581, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Mosterd, C.; Kanbay, M.; Born, B.V.D.; van Raalte, D.; Rampanelli, E. Intestinal microbiota and diabetic kidney diseases: The Role of microbiota and derived metabolites inmodulation of renal inflammation and disease progression. Best Pract. Res. Clin. Endocrinol. Metab. 2021, 35, 101484. [Google Scholar] [CrossRef]
- Izundegui, D.G.; Nayor, M. Metabolomics of Type 1 and Type 2 Diabetes: Insights into Risk Prediction and Mechanisms. Curr. Diabetes Rep. 2022, 22, 65–76. [Google Scholar] [CrossRef]
- Zaky, A.; Glastras, S.J.; Wong, M.Y.W.; Pollock, C.A.; Saad, S. The Role of the Gut Microbiome in Diabetes and Obesity-Related Kidney Disease. Int. J. Mol. Sci. 2021, 22, 9641. [Google Scholar] [CrossRef]
- Dai, Z.F.; Ma, X.Y.; Yang, R.L.; Wang, H.C.; Xu, D.D.; Yang, J.N.; Guo, X.B.; Meng, S.S.; Xu, R.; Li, Y.X.; et al. Intestinal flora alterations in patients with ulcerative colitis and their association with inflammation. Exp. Ther. Med. 2021, 22, 1322. [Google Scholar] [CrossRef]
- Cronin, P.; Joyce, S.A.; O’Toole, P.W.; O’Connor, E.M. Dietary Fibre Modulates the Gut Microbiota. Nutrients 2021, 13, 1655. [Google Scholar] [CrossRef]
- Rossi, M.; Johnson, D.W.; Morrison, M.; Pascoe, E.M.; Coombes, J.S.; Forbes, J.M.; Szeto, C.-C.; McWhinney, B.C.; Ungerer, J.P.; Campbell, K.L. Synbiotics Easing Renal Failure by Improving Gut Microbiology (SYNERGY): A Randomized Trial. Clin. J. Am. Soc. Nephrol. 2016, 11, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.J.; Guo, J.; Jia, Q.; Huang, Y.S.; Huang, W.-J.; Zhang, W.; Zhang, F.; Liu, W.J.; Wang, Y. The effect of probiotic and synbiotic supplementation on biomarkers of inflammation and oxidative stress in diabetic patients: A systematic review and meta-analysis of randomized controlled trials. Pharmacol. Res. 2019, 142, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Lukas, M.; Drastich, P.; Konecny, M.; Gionchetti, P.; Urban, O.; Cantoni, F.; Bortlik, M.; Duricova, D.; Bulitta, M. Exogenous alkaline phosphatase for the treatment of patients with moderate to severe ulcerative colitis. Inflamm. Bowel Dis. 2010, 16, 1180–1186. [Google Scholar] [CrossRef] [PubMed]
- Estaki, M.; DeCoffe, D.; Gibson, D.L. Interplay between intestinal alkaline phosphatase, diet, gut microbes and immunity. World J. Gastroenterol. 2014, 20, 15650–15656. [Google Scholar] [CrossRef] [PubMed]
- Pickkers, P.; Heemskerk, S.; Schouten, J.; Laterre, P.-F.; Vincent, J.-L.; Beishuizen, A.; Jorens, P.G.; Spapen, H.; Bulitta, M.; Peters, W.H.; et al. Alkaline phosphatase for treatment of sepsis-induced acute kidney injury: A prospective randomized double-blind placebo-controlled trial. Crit. Care 2012, 16, R14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banasiewicz, T.; Domagalska, D.; Borycka-Kiciak, K.; Rydzewska, G. Determination of butyric acid dosage based on clinical and experimental studies—A literature review. Gastroenterol. Rev. 2020, 15, 119–125. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Total | Sodium Butyrate | Placebo | |
|---|---|---|---|
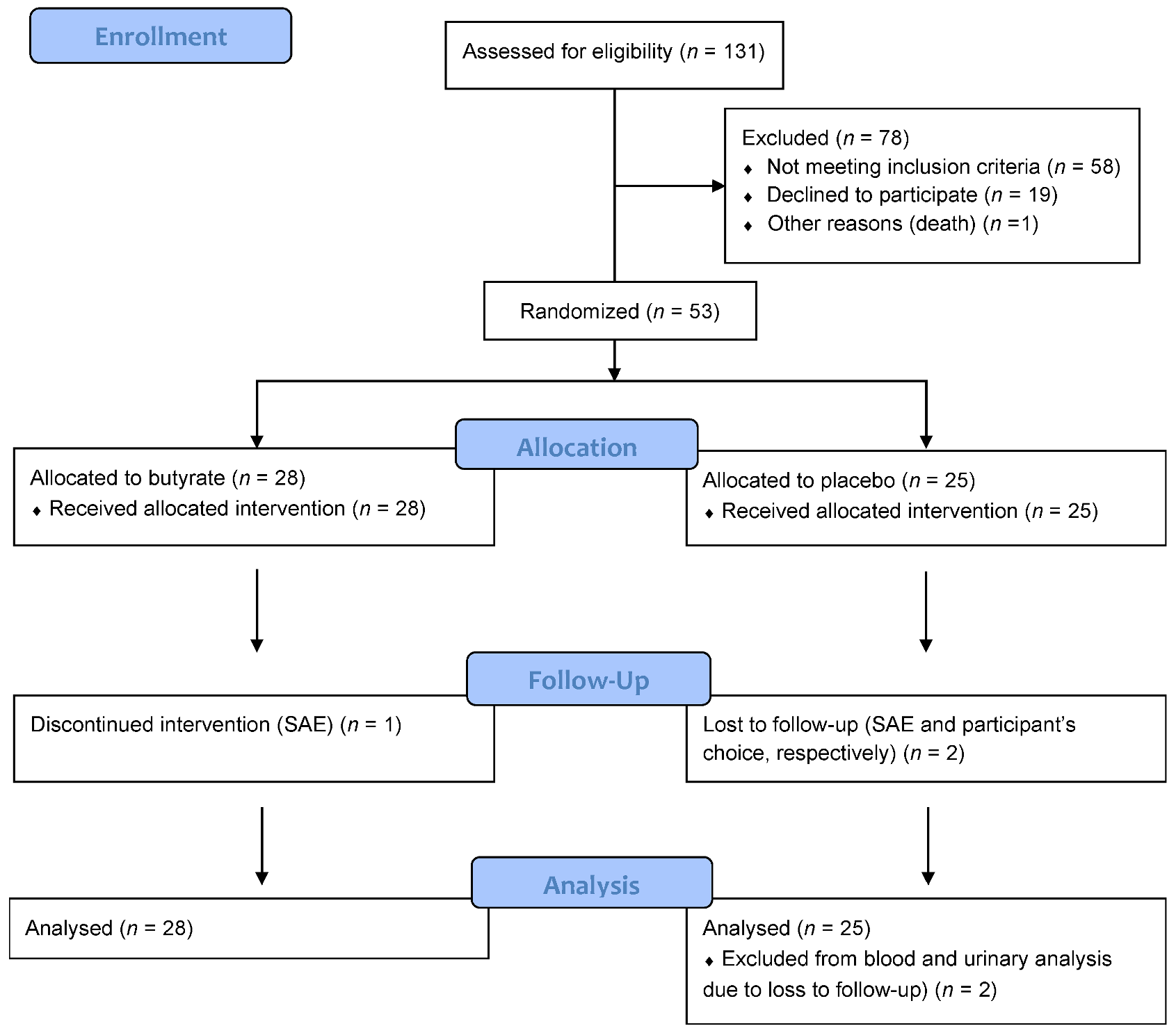
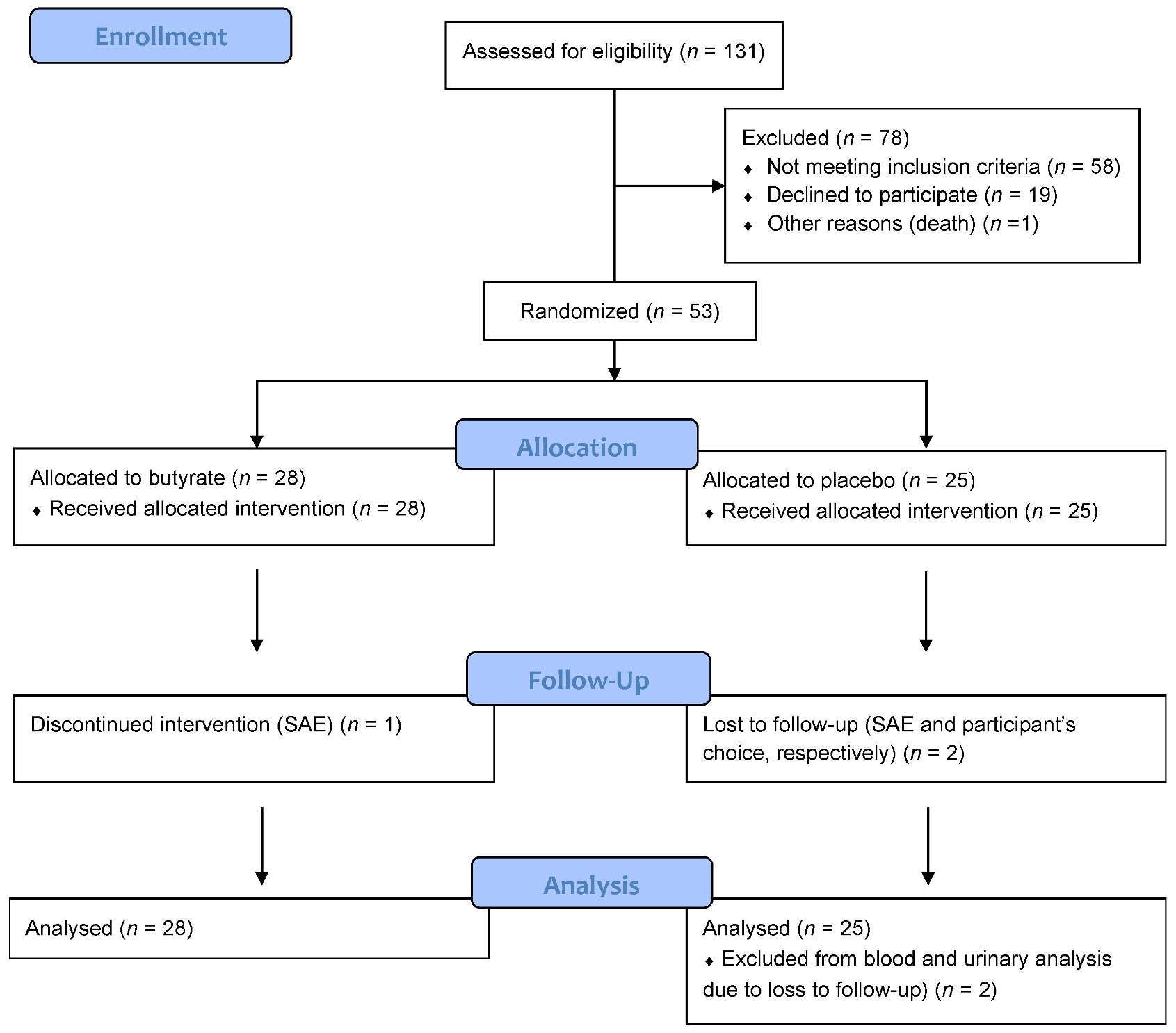
| Number | 53 (100) | 28 (53) | 25 (47) |
| Site (Denmark) | 41 (77) | 22 (79) | 19 (76) |
| Sex (Female) | 23 (43) | 11 (39) | 12 (48) |
| Age, years | 54 ± 13 | 56 ± 11 | 52 ± 15 |
| Diabetes duration, years | 30 ± 15 | 29 ± 17 | 32 ± 14 |
| Current smoking | 7 (13) | 0 | 7 (28) |
| Body Mass Index, kg/m2 | 29 ± 5.8 | 30 ± 6.1 | 29 ± 5.7 |
| Systolic blood pressure, mm Hg | 135 ± 18 | 136 ± 15 | 134 ± 21 |
| Diastolic blood pressure, mm Hg | 78 ± 10 | 80 ± 10 | 77 ± 10 |
| Urinary albumin creatinine ratio, mg/g | 46 [14:121] | 39 [18:121] | 49 [14:121] |
| Normoalbuminuria | 21 (40) | 11 (39) | 10 (40) |
| Microalbuminuria | 24 (45) | 13 (46) | 12 (44) |
| Macroalbuminuria | 8 (15) | 4 (14) | 3 (12) |
| eGFR, mL/min/1.73 m2 | 84 ± 24 | 86 ± 26 | 8.1 ± 1.1 |
| HbA1c, % (mmol/mol) | 8.0 ± 1.0 | 8.0 ± 0.8 | 8.1 ± 1.1 |
| Fecal calprotectin ≥ 50 µg/g | 29 (55) | 14 (48) | 15 (52) |
| RASi treatment | 44 (83) | 23 (82) | 21 (84) |
| Statin treatment | 37 (70) | 21 (75) | 16 (64) |
| Metformin treatment | 10 (19) | 7 (25) | 3 (12) |
| Baseline | After Intervention | Change | ANCOVA p Value | |
|---|---|---|---|---|
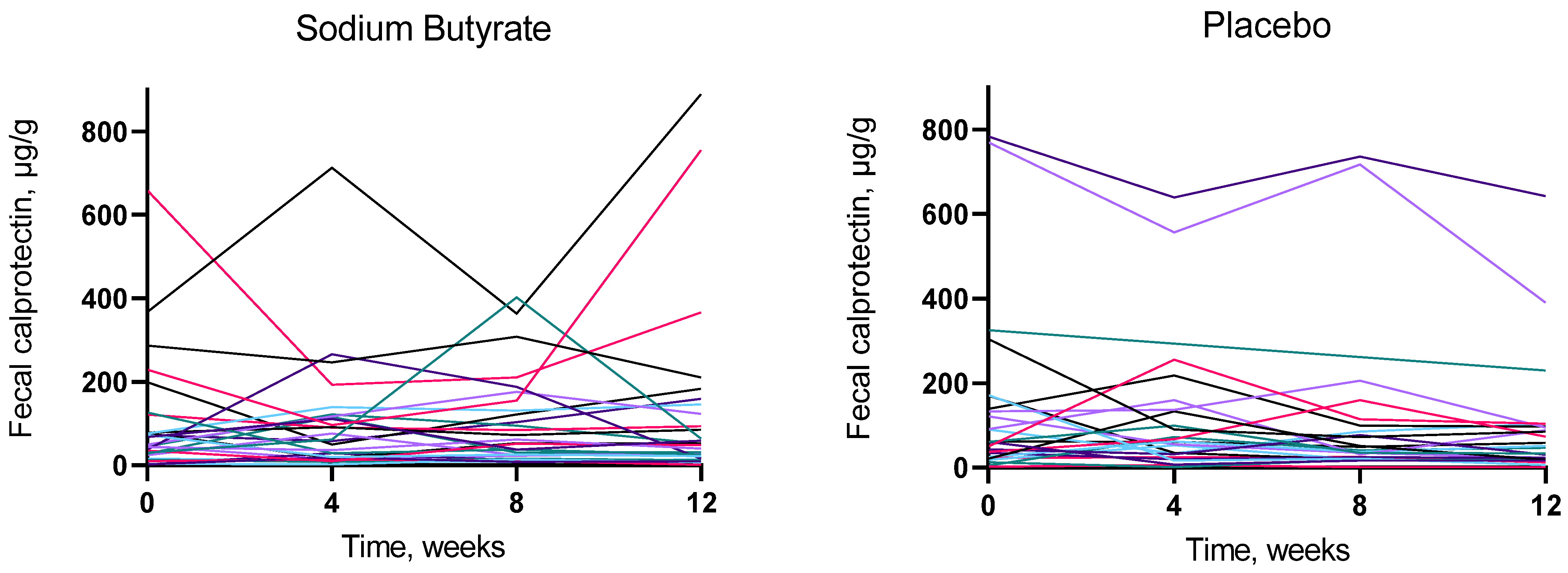
| Fecal calprotectin (µg/g) | ||||
| 48 [26:100] | 50 [19:135] | −1.0 [−20:10] | 0.24 |
| 61 [25:139] | 47 [19:95] | −12 [−95:1] | |
| Fecal IAP activity/Protein (U/g) | ||||
| 92 [49:609] | 83 [39:605] | −3.9 [−25:51] | 0.98 |
| 55 [38:133] | 53 [22:106] | −0.24 [−22:38] | |
| Fecal butyrate (µg/mg) | ||||
| 6.4 [2.8:12] | 6.4 [3.7:12] | 0.7 [−1.5:4.2] | 0.34 |
| 4.3 [2.1:7.6] | 4.4 [2.5:8.8] | 0.052 [−3.5:2.0] | |
| Fecal acetate (µg/mg) | ||||
| 21 ± 8.8 | 21 ± 12 | 0.080 ± 12 | 0.33 |
| 18 ± 9.6 | 17 ± 8.7 | −1.3 ± 10 | |
| Fecal propionate (µg/mg) | ||||
| 8.0 [4.2:12] | 6.8 [3.5:11] | −0.15 [−3.3:1.1] | 0.93 |
| 5.4 [3.6:7.9] | 5.5 [3.7:8.7] | −0.94 [−2.3:1.8] | |
| Fecal valerate (µg/mg) | ||||
| 2.0 ± 1.0 | 2.1 ± 1.6 | 0.13 ± 1.8 | 0.67 |
| 1.7 ± 1.0 | 1.8 ± 1.2 | 0.15 ± 1.3 | |
| Fecal immunoglobulin G/Protein (ng/g) | ||||
| 28 [16:110] | 40 [16:116] | −1.8 [−0.067:0.034] | 0.10 |
| 27 [14:67] | 17 [9.9:36] | −1.9 [−15:18] | |
| Fecal immunoglobulin A/Protein (µg/mg) | ||||
| 1.6 [0.50:7.14] | 2.3 [0.72:4.9] | 0.30 [−1.2:1.31] | 0.69 |
| 2.4 [1.1:7.8] | 1.7 [0.73:9.9] | 0.077 [−2.0:3.7] | |
| Fecal immunoglobulin M/Protein (ng/mg) | ||||
| 0.61 [0.32:2.0] | 1.1 [0.36:2.7] | 0.38 [−0.0011:1.5] | 0.20 |
| 1.0 [0.36:1.9] | 0.72 [0.46:1.8] | 0.18 [−1.4:0.70] | |
| Urinary albumin creatinine ratio (mg/g) | ||||
| 39 [18:121] | 37 [27:82] | 1.5 [−9.5:21] | 0.69 |
| 49 [14:121] | 37 [18:208] | −1.0 [−19:6.0] | |
| Estimated glomerular filtration rate (mL/min/1.73 m2) | ||||
| 86 ± 26 | 84 ± 25 | −2.0 ± 8.3 | 0.30 |
| 82 ± 22 | 83 ± 23 | 0.39 ± 7.1 | |
| Serum high sensitivity CRP (mg/L) | ||||
| 1.7 [0.91:3.1] | 1.7 [0.95:3.0] | −0.06 [−0.65:0.55] | 0.13 |
| 1.9 [1.0:4.0] | 2.0 [1.5:6.0] | −0.18 [−0.84:0.38] | |
| Serum lipopolysaccharide (EU/mL) | ||||
| 0.66 ± 0.18 | 0.66 ± 0.20 | −0.0025 ± 0.20 | 0.093 |
| 0.73 ± 0.11 | 0.80 ± 0.26 | 0.076 ± 0.26 | |
| HbA1c (% (mmol/mol)) | ||||
| 8.0 ± 0.8 | 8.0 ± 0.9 | 0.1 ± 0.4 | 0.32 |
| 8.1 ± 1.1 | 8.3 ± 1.3 | 0.2 ± 0.6 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tougaard, N.H.; Frimodt-Møller, M.; Salmenkari, H.; Stougaard, E.B.; Zawadzki, A.D.; Mattila, I.M.; Hansen, T.W.; Legido-Quigley, C.; Hörkkö, S.; Forsblom, C.; et al. Effects of Butyrate Supplementation on Inflammation and Kidney Parameters in Type 1 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Clin. Med. 2022, 11, 3573. https://doi.org/10.3390/jcm11133573
Tougaard NH, Frimodt-Møller M, Salmenkari H, Stougaard EB, Zawadzki AD, Mattila IM, Hansen TW, Legido-Quigley C, Hörkkö S, Forsblom C, et al. Effects of Butyrate Supplementation on Inflammation and Kidney Parameters in Type 1 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial. Journal of Clinical Medicine. 2022; 11(13):3573. https://doi.org/10.3390/jcm11133573
Chicago/Turabian StyleTougaard, Ninna H., Marie Frimodt-Møller, Hanne Salmenkari, Elisabeth B. Stougaard, Andressa D. Zawadzki, Ismo M. Mattila, Tine W. Hansen, Cristina Legido-Quigley, Sohvi Hörkkö, Carol Forsblom, and et al. 2022. "Effects of Butyrate Supplementation on Inflammation and Kidney Parameters in Type 1 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial" Journal of Clinical Medicine 11, no. 13: 3573. https://doi.org/10.3390/jcm11133573
APA StyleTougaard, N. H., Frimodt-Møller, M., Salmenkari, H., Stougaard, E. B., Zawadzki, A. D., Mattila, I. M., Hansen, T. W., Legido-Quigley, C., Hörkkö, S., Forsblom, C., Groop, P.-H., Lehto, M., & Rossing, P. (2022). Effects of Butyrate Supplementation on Inflammation and Kidney Parameters in Type 1 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial. Journal of Clinical Medicine, 11(13), 3573. https://doi.org/10.3390/jcm11133573