
Clinical Characteristics and Prognostic Relevance of Different Types of Caregivers for Elderly Patients with Acute Heart Failure—Analysis from the RICA Registry

 , , , , ,
, , , , ,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Design—Type of Study
2.2. Inclusion and Exclusion Criteria
2.3. Variables
2.4. Statistical Analysis
2.5. Ethical Aspects
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fernández-Casso, M.L.; Hernando-Arizaleta, L.; Palomar-Rodriguez, J.A.; Soria-Arcos, F.; Pascual-Figal, D.A. Trends and Characteristics of Hospitalization for Heart Failure in a Population Setting From 2003 to 2013. Rev. Esp. Cardiol. 2017, 70, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Calero-Molina, E.; Hidalgo, E.; Rosenfeld, L.; Verdú-Rotellar, J.M.; Verdú-Soriano, J.; Garay, A.; Alcoberro, L.; Jimenez-Marrero, S.; Garcimartin, P.; Yun, S.; et al. The relationship between self-care, long-term mortality, and heart failure hospitalization: Insights from a real-world cohort study. Eur. J. Cardiovasc. Nurs. 2022, 21, 116. [Google Scholar] [CrossRef] [PubMed]
- Kitko, L.; McIlvennan, C.K.; Bidwell, J.T.; Dionne-Odom, J.N.; Dunlay, S.M.; Lewis, L.M.; Meadows, G.; Sattler, E.L.P.; Schulz, R.; Strömberg, A. American Heart Association Council on Cardiovascular and Stroke Nursing; Council on Quality of Care and Outcomes Research; Council on Clinical Cardiology; and Council on Lifestyle and Cardiometabolic Health. Family Caregiving for Individuals with Heart Failure: A Scientific Statement from the American Heart Association. Circulation 2020, 141, e864–e878. [Google Scholar] [CrossRef] [PubMed]
- Riegel, B.; Moser, D.K.; Anker, S.D.; Appel, L.J.; Dunbar, S.B.; Grady, K.L.; on behalf of the American Heart Association Council on Cardiovascular Nursing; American Heart Association Council on Cardiovascular Nursing; American Heart Association Council on Clinical Cardiology; American Heart Association Council on Nutrition, Physical Activity, and Metabolism; et al. State of the science: Promoting self-care in persons with heart failure: A scientific statement from the American Heart Association. Circulation 2009, 120, 1141–1163. [Google Scholar] [CrossRef] [PubMed]
- Riegel, B.; Moser, D.K.; Buck, H.G.; Dickson, V.V.; Dunbar, S.B.; Lee, C.S.; on behalf of the American Heart Association Council on Cardiovascular and Stroke Nursing; Council on Peripheral Vascular Disease; Council on Quality of Care and Outcomes Research. Self-care for the prevention and management of cardiovascular disease and stroke: A scientific statement for healthcare professionals from the American Heart Association. J. Am. Heart Assoc. 2017, 6, e006997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albert, N.M. A systematic review of transitional-care strategies to reduce rehospitalization in patients with heart failure. Heart Lung 2016, 45, 100–113. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.L. Caregiving in Heart Failure. J. Cardiovasc. Nurs. 2020, 35, 229–230. [Google Scholar] [CrossRef] [PubMed]
- Trullàs, J.C.; Formiga, F.; Montero, M.; Conde, A.; Casado, J.; Carrasco, F.J.; Díez, J.; Ceresuela, L.M.; Grupo RICA. Paradoja de la obesidad en la insuficiencia cardiaca. Resultados del Registro RICA [Paradox of obesity in heart failure: Results from the Spanish RICA Registry]. Med. Clin. 2011, 137, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Rogero-García, J.; García-Sainz, C. Caregiver Leave-Taking in Spain: Rate, Motivations, and Barriers. J. Aging Soc. Policy 2016, 28, 98–112. [Google Scholar] [CrossRef] [PubMed]
- Chivite, D.; Formiga, F.; Corbella, X.; Conde-Martel, A.; Aramburu, Ó.; Carrera, M.; Dávila, M.F.; Pérez-Silvestre, J.; Manzano, L.; Montero-Pérez-Barquero, M.; et al. Basal functional status predicts one-year mortality after a heart failure hospitalization in elderly patients—The RICA prospective study. Int. J. Cardiol. 2018, 254, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Vest, A.R.; Chan, M.; Deswal, A.; Givertz, M.M.; Lekavich, C.; Lennie, T.; Litwin, S.E.; Parsly, L.; Rodgers, J.E.; Rich, M.W.; et al. Nutrition, Obesity, and Cachexia in Patients with Heart Failure: A Consensus Statement from the Heart Failure Society of America Scientific Statements Committee. J. Card. Fail. 2019, 25, 380–400. [Google Scholar] [CrossRef] [PubMed]
- Kamath, D.Y.; Bhuvana, K.B.; Dhiraj, R.S.; Xavier, D.; Varghese, K.; Salazar, L.J.; Granger, C.B.; Pais, P.; Granger, B.B. Patient and caregiver reported facilitators of self-care among patients with chronic heart failure: Report from a formative qualitative study. Wellcome Open Res. 2020, 5, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Méndez-Bailón, M.; Jiménez-García, R.; Hernández-Barrera, V.; Comín-Colet, J.; Esteban-Hernández, J.; de Miguel-Díez, J.; de Miguel-Yanes, J.M.; Muñoz-Rivas, N.; Lorenzo-Villalba, N.; López-de-Andrés, A. Significant and constant increase in hospitalization due to heart failure in Spain over 15 year period. Eur. J. Intern. Med. 2019, 64, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Elkhateeb, O.; Salem, K. Patient and caregiver education levels and readmission and mortality rates of congestive heart failure patients. East Mediterr. Health J. 2018, 24, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Ktaa, S.; Polovina, M.; Rosano, G.; Abdin, A.; Anguita, M.; Lainscak, M.; Lund, L.H.; McDonagh, T.; Metra, M.; Mindham, R.; et al. European Society of Cardiology quality indicators for the care and outcomes of adults with heart failure. Developed by the Working Group for Heart Failure Quality Indicators in collaboration with the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2022, 24, 132–142. [Google Scholar]
- Ghasemi, M.; Arab, M.; Mangolian Shahrbabaki, P. Relationship Between Caregiver Burden and Family Functioning in Family Caregivers of Older Adults with Heart Failure. J. Gerontol. Nurs. 2020, 46, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Iovino, P.; Rebora, P.; Occhino, G.; Zeffiro, V.; Caggianelli, G.; Ausili, D.; Alvaro, R.; Riegel, B.; Vellone, E. Does motivational interviewing reduce health services use and mortality in heart failure patients? A secondary analysis of the MOTIVATE-HF trial. Eur. J. Cardiovasc. Nurs. 2021, 20, zvab060.093. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | All (n= 2147) | Partner Caregiver (n = 703) | Children Caregiver (n = 1097) | Professional Caregiver (n = 199) | No Caregiver (n = 148) | p-Value |
|---|---|---|---|---|---|---|
| Age, median (SD) | 81.06 (8.7) | 77.28 (9.05) | 83.63 (7.02) | 83.53 (8.2) | 76.6 * (10.7) | <0.001 |
| Sex: male, n (%) | 1022 (47.6) | 483 (68.7) * | 375 (34.2) | 76 (38.2) | 88 (59.5) | <0.001 |
| Sex: female, n (%) | 1125 (52.4) | 220 (31.3) | 722 (65.8) * | 123 (61.8) | 60 (40.5) | <0.001 |
| Comorbidities | ||||||
| Hypertension, n (%) | 1889 (88) | 604 (85.9) | 989 (90.2) | 176 (88.4) | 120 (81.1) * | <0.001 |
| T2DM, n (%) | 993 (46.3) | 367 (52.2) | 467 (42.6) | 82 (41.2) * | 77 (52) | <0.001 |
| COPD, n (%) | 448 (20.9) | 182 (25.9) * | 203 (18.5) | 34 (17.1) | 29 (19.6) | 0.001 |
| Atrial fibrillation, n (%) | 1172 (54.6) | 361 (51.4) | 629 (57.3) | 119 (59.8) | 63 (42.6) * | <0.001 |
| Ischemic heart disease, n (%) | 481 (22.4) | 190 (27) | 213 (19) | 167 (16) | 102 (31) * | <0.001 |
| Pfeiffer index, median (SD) | 1.5 (1.9) | 1.08 (1.6) | 1.31 (1.7) | 2.02 (2.3) | 0.5 * (1.09) | <0.001 |
| Barthel index, median (SD) | 81.2 (24.09) | 89.2 (18.02) | 75.3 (25.9) | 73.8 (26.6) | 95.9 * (9.7) | <0.001 |
| Charlson score, median (SD) | 3.05 (2.5) | 3.2 (2.6) | 3.02 (2.4) | 2.9 (2.4) | 2.6 * (3.2) | 0.035 |
| LVEF, median (SD) | 51.8 (15.7) | 50.3 (15.4) | 53.3 (15.7) | 54.5 (15.3) | 44.7 * (15.3) | <0.001 |
| Laboratory, n (%) | ||||||
| Hemoglobin, (g/dL) median (SD) | 12.09 (2.04) | 12.3 (2.09) | 11.9 (1.9) | 11.8 * (1.9) | 12.5 (2.2) | <0.001 |
| Creatinine (ml/min/m3), median (SD) | 1.3 (2.6) | 1.2 (0.5) | 1.4 (3.6) | 1.2 (0.7) | 1.2 (0.5) | 0.692 |
| proBNP (pg/mL), median | 6654.6 | 5697.2 | 7108.06 | 7296.9 | 7555.1 | 0.058 |
| Non-pharmacological treatment | 19(0.88) | |||||
| Fluid restriction, n (%) | 1365 (70.5) | 417 (66.3) | 741 (73.7) | 124 (68.5) | 83 (65.9) | 0.008 |
| Weight monitoring, n (%) | 1555 (80) | 497 (79.1) | 803 (41.3) | 153 (84.1) | 102 (81) | 0.510 |
| Low-sodium diet, n (%) | 1814 (93) | 583 (92.4) | 949 (93.9) | 172 (94.5) | 110 (88) | 0.072 |
| Pharmacological treatment, n (%) | ||||||
| Beta blockers, n (%) | 1522 (70.9) | 516 (73.4) | 753 (68.6) | 127 (63.8) | 126 (85.1) * | <0.001 |
| ACE inhibitors/ARA-2, n (%) | 1266 (59) | 404 (57.5) | 654 (59.6%) | 131 (65.8) * | 77 (52) | 0.054 |
| Sacubitril valsartan, n (%) | 138 (6.4) | 42 (6) | 55 (5) | 6 (3) | 35 (25.4) * | <0.001 |
| Anti-aldosterone agents | 486 (22.6) | 180 (37) * | 233 (21.2) | 38 (19.1) | 35 (23.6) | 0.099 |
| Endpoints n (%) | ||||||
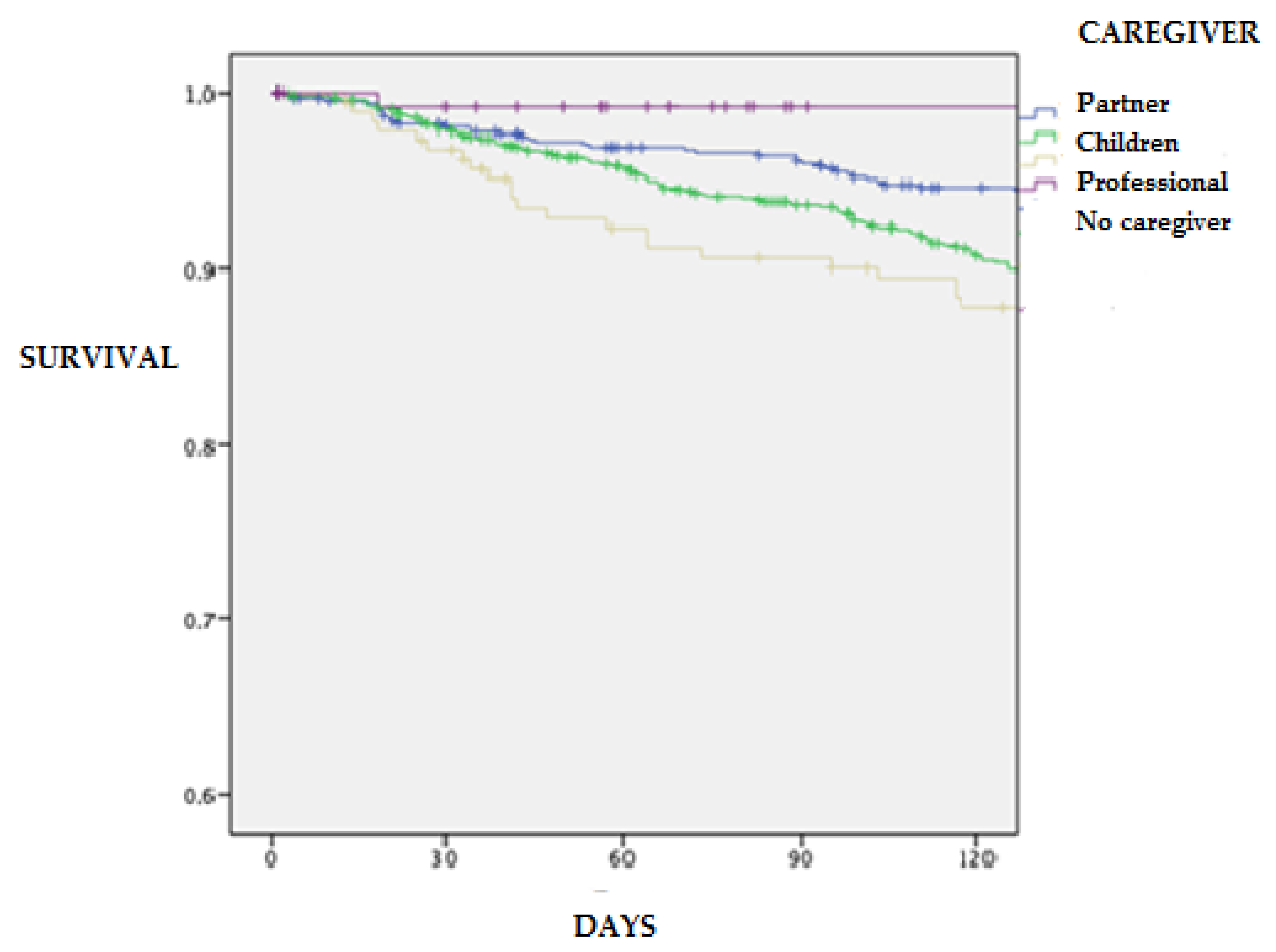
| Mortality at 30 days, n (%) | 546 (27.9) | 155 (29.2) | 299 (35.3) | 67 (35.3) | 25 (22.9) * | 0.011 |
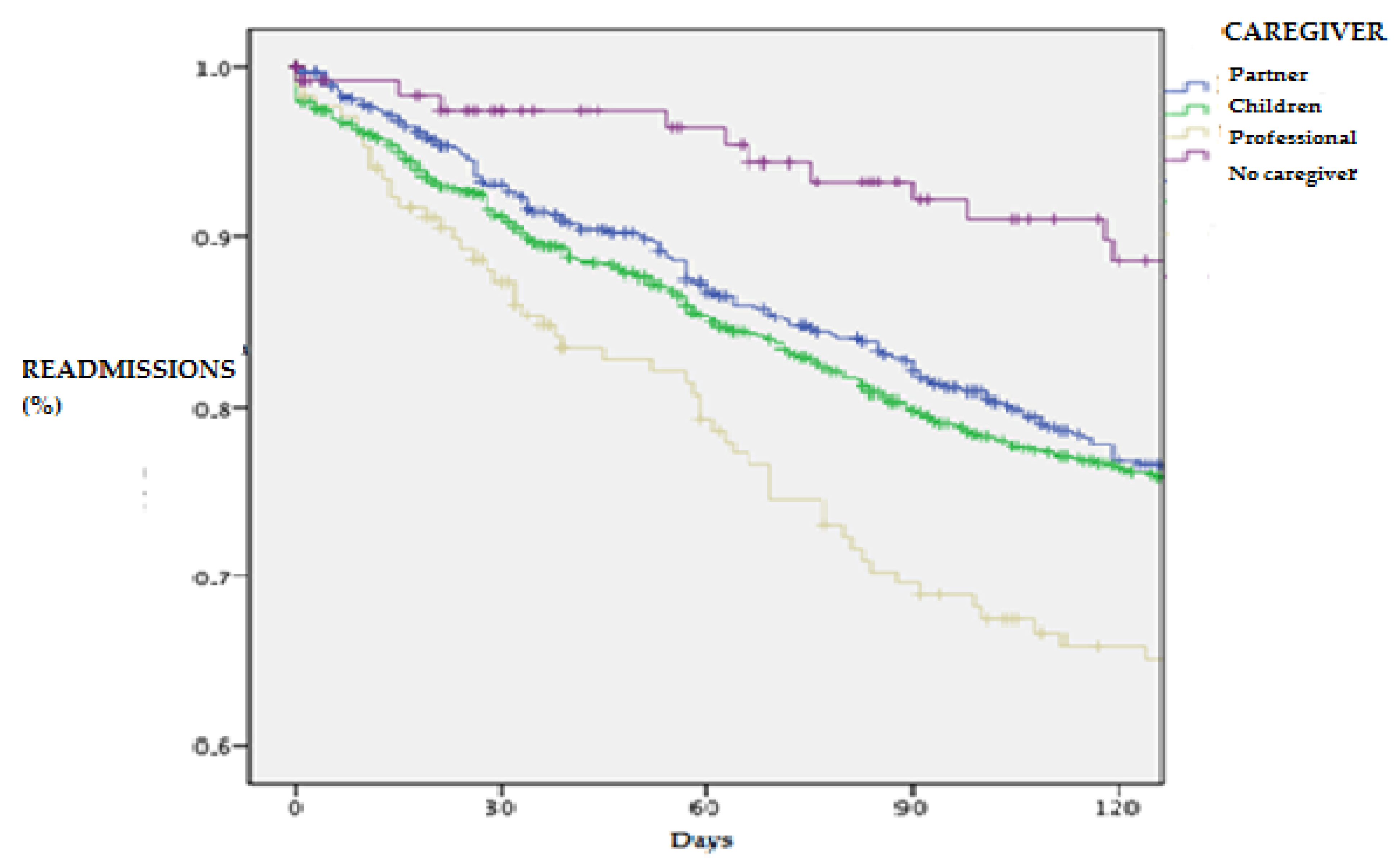
| 30-day readmission, n (%) | 383 (19.7) | 109 (17.3) * | 201 (19.7) | 49 (26.1) | 24 (22.4) | 0.053 |
| Mortality at 120 days, n (%) | 630 (32.1) | 177 (27.8) * | 341 (33.3) | 76 (40) | 336 (33) | 0.010 |
| 120-day readmission, n (%) | 691 (35.5) | 207 (32.8) * | 355 (34.8) | 87 (46.3) | 42 (39.3) | 0.006 |
| One-year readmission, n (%) | 1365 (70.1) | 430 (68.1) | 718 (70.4) | 142 (75.5) | 75 (70.1) | 0.279 |
| One-year mortality, n (%) | 1208 (61.6) | 380 (59.7) | 635 (62) | 121 (63.7) | 72 (66.1) | 0.524 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Méndez-Bailon, M.; Lorenzo-Villalba, N.; Rubio-Garcia, J.; Moreno-García, M.C.; Ropero-Luis, G.; Martínez-Litago, E.; Quirós-López, R.; Carrascosa-García, S.; González-Franco, A.; Andrès, E.; et al. Clinical Characteristics and Prognostic Relevance of Different Types of Caregivers for Elderly Patients with Acute Heart Failure—Analysis from the RICA Registry. J. Clin. Med. 2022, 11, 3516. https://doi.org/10.3390/jcm11123516
Méndez-Bailon M, Lorenzo-Villalba N, Rubio-Garcia J, Moreno-García MC, Ropero-Luis G, Martínez-Litago E, Quirós-López R, Carrascosa-García S, González-Franco A, Andrès E, et al. Clinical Characteristics and Prognostic Relevance of Different Types of Caregivers for Elderly Patients with Acute Heart Failure—Analysis from the RICA Registry. Journal of Clinical Medicine. 2022; 11(12):3516. https://doi.org/10.3390/jcm11123516
Chicago/Turabian StyleMéndez-Bailon, Manuel, Noel Lorenzo-Villalba, Jorge Rubio-Garcia, María Carmen Moreno-García, Guillermo Ropero-Luis, Eduardo Martínez-Litago, Raúl Quirós-López, Sara Carrascosa-García, Alvaro González-Franco, Emmanuel Andrès, and et al. 2022. "Clinical Characteristics and Prognostic Relevance of Different Types of Caregivers for Elderly Patients with Acute Heart Failure—Analysis from the RICA Registry" Journal of Clinical Medicine 11, no. 12: 3516. https://doi.org/10.3390/jcm11123516
APA StyleMéndez-Bailon, M., Lorenzo-Villalba, N., Rubio-Garcia, J., Moreno-García, M. C., Ropero-Luis, G., Martínez-Litago, E., Quirós-López, R., Carrascosa-García, S., González-Franco, A., Andrès, E., Casado-Cerrada, J., & Montero-Pérez-Barquero, M. (2022). Clinical Characteristics and Prognostic Relevance of Different Types of Caregivers for Elderly Patients with Acute Heart Failure—Analysis from the RICA Registry. Journal of Clinical Medicine, 11(12), 3516. https://doi.org/10.3390/jcm11123516