
A Woman’s Place Is in Theatre, but Are Theatres Designed with Women in Mind? A Systematic Review of Ergonomics for Women in Surgery

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
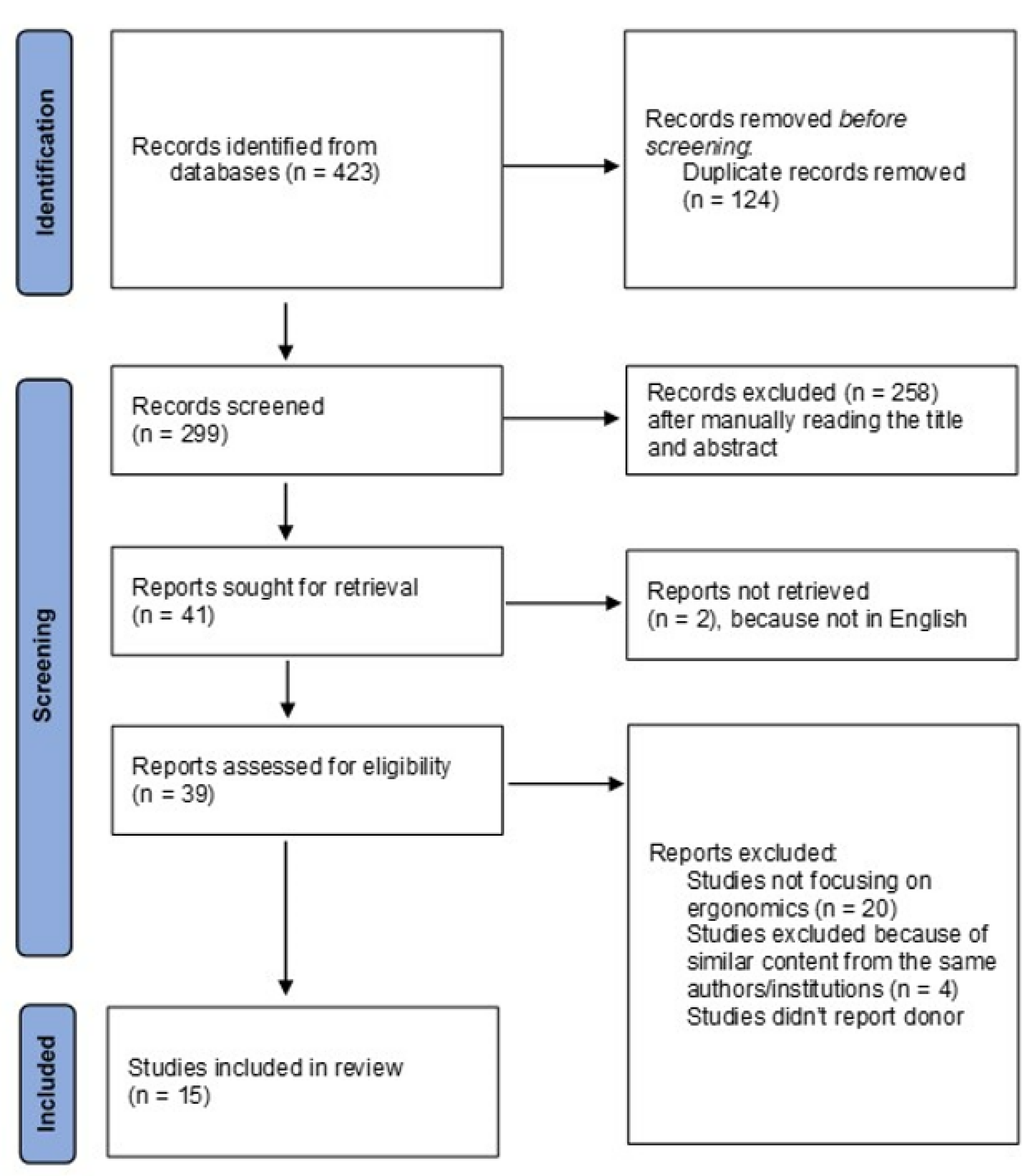
2. Materials and Methods
3. Results
3.1. Work-Related Physical Discomfort
3.2. Compliance of Surgical Devices with Female Requirements
3.3. Impact on Training, Productivity, and Career Longevity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stephens, E.H.; Heisler, C.A.; Temkin, S.M.; Miller, P. The Current Status of Women in Surgery: How to Affect the Future. JAMA Surg. 2020, 155, 876–885. [Google Scholar] [CrossRef] [PubMed]
- Bellini, M.I.; Adair, A.; Fotopoulou, C.; Graham, Y.; Hutson, A.; McNally, S.; Mohan, H.; Vig, S.; Parks, R.; Papalois, V. Changing the norm towards gender equity in surgery: The women in surgery working group of the Association of Surgeons of Great Britain and Ireland’s perspective. J. R. Soc. Med. 2019, 112, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Dossa, F.; Zeltzer, D.; Sutradhar, R.; Simpson, A.N.; Baxter, N.N. Sex Differences in the Pattern of Patient Referrals to Male and Female Surgeons. JAMA Surg. 2022, 157, 95. [Google Scholar] [CrossRef] [PubMed]
- Bellini, M.I.; Graham, Y.; Hayes, C.; Zakeri, R.; Parks, R.; Papalois, V. A woman’s place is in theatre: Women’s perceptions and experiences of working in surgery from the Association of Surgeons of Great Britain and Ireland women in surgery working group. BMJ Open 2019, 9, e024349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenup, R.A.; Pitt, S.C. Women in Academic Surgery: A Double-Edged Scalpel. Acad. Med. 2020, 95, 1483–1484. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Jacob-Brassard, J.; Dossa, F.; Salata, K.; Kishibe, T.; Greco, E.; Baxter, N.N.; Al-Omran, M. Gender differences in faculty rank among academic physicians: A systematic review and meta-analysis. BMJ Open 2021, 11, e050322. [Google Scholar] [CrossRef]
- Murphy, M.; Record, H.; Callander, J.K.; Dohan, D.; Grandis, J.R. Mentoring Relationships and Gender Inequities in Academic Medicine: Findings from a Multi-Institutional Qualitative Study. Acad. Med. 2022, 97, 136–142. [Google Scholar] [CrossRef]
- Sutton, E.; Irvin, M.; Zeigler, C.; Lee, G.; Park, A. The ergonomics of women in surgery. Surg. Endosc. Other Interv. Tech. 2014, 28, 1051–1055. [Google Scholar] [CrossRef]
- Kono, E.; Tada, M.; Kouchi, M.; Endo, Y.; Tomizawa, Y.; Matsuo, T.; Nomura, S. Ergonomic evaluation of a mechanical anastomotic stapler used by Japanese surgeons. Surg. Today 2014, 44, 1040–1047. [Google Scholar] [CrossRef] [Green Version]
- Berguer, R.; Hreljac, A. The relationship between hand size and difficulty using surgical instruments: A survey of 726 laparoscopic surgeons. Surg. Endosc. 2004, 18, 508–512. [Google Scholar] [CrossRef]
- Karwowski, W.; Rizzo, F.; Rodrick, D. Ergonomics. In Encyclopedia of Information Systems; Bidgoli, H., Ed.; Elsevier: New York, NY, USA, 2003; pp. 185–201. [Google Scholar]
- The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 16 December 2019).
- Adams, S.R.; Hacker, M.R.; McKinney, J.L.; Elkadry, E.A.; Rosenblatt, P.L. Musculoskeletal Pain in Gynecologic Surgeons. J. Minim. Invasive Gynecol. 2013, 20, 656–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aitchison, L.P.; Cui, C.K.; Arnold, A.; Nesbitt-Hawes, E.; Abbott, J. The ergonomics of laparoscopic surgery: A quantitative study of the time and motion of laparoscopic surgeons in live surgical environments. Surg. Endosc. Other Interv. Tech. 2016, 30, 5068–5076. [Google Scholar] [CrossRef] [PubMed]
- Armijo, P.R.; Flores, L.; Pokala, B.; Huang, C.K.; Siu, K.C.; Oleynikov, D. Gender equity in ergonomics: Does muscle effort in laparoscopic surgery differ between men and women? Surg. Endosc. Other Interv. Tech. 2022, 36, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Cavanagh, J.; Brake, M.; Kearns, D.; Hong, P. Work environment discomfort and injury: An ergonomic survey study of the American Society of Pediatric Otolaryngology members. Am. J. Otolaryngol. 2012, 33, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Dalsgaard, T.; Jensen, M.D.; Hartwell, D.; Mosgaard, B.J.; Jorgensen, A.; Jensen, B.R. Robotic Surgery Is Less Physically Demanding Than Laparoscopic Surgery Paired Cross Sectional Study. Ann. Surg. 2020, 271, 106–113. [Google Scholar] [CrossRef]
- Gonzalez, A.G.; Salgado, D.R.; García-Moruno, L. Optimisation of a laparoscopic tool handle dimension based on ergonomic analysis. Int. J. Ind. Ergon. 2015, 48, 16–24. [Google Scholar] [CrossRef]
- Harutunian, K.; Gargallo-Albiol, J.; Figueiredo, R.; Escoda, C.G. Ergonomics and musculoskeletal pain among postgraduate students and faculty members of the School of Dentistry of the University of Barcelona (Spain). A cross-sectional study. Med. Oral Patol. Oral Y Cir. Bucal. 2011, 16, e425–e429. [Google Scholar] [CrossRef] [Green Version]
- Hokenstad, E.D.; Hallbeck, M.S.; Lowndes, B.R.; Morrow, M.M.; Weaver, A.L.; McGree, M.; Glaser, G.E.; Occhino, J.A. Ergonomic Robotic Console Configuration in Gynecologic Surgery: An Interventional Study. J. Minim. Invasive Gynecol. 2021, 28, 850–859. [Google Scholar] [CrossRef]
- Jensen, M.J.; Pagedar, N.A.; Sugg, S.L.; Lal, G. Endocrine surgeons have high rates of work-related musculoskeletal (MSK) injury and symptoms. Am. J. Surg. 2021. [Google Scholar] [CrossRef]
- Kono, E.; Tomizawa, Y.; Matsuo, T.; Nomura, S. Rating and issues of mechanical anastomotic staplers in surgical practice: A survey of 241 Japanese gastroenterological surgeons. Surg. Today 2012, 42, 962–972. [Google Scholar] [CrossRef]
- McQuivey, K.S.; Deckey, D.G.; Christopher, Z.K.; Rosenow, C.S.; Mi, L.; Spangehl, M.J.; Bingham, J.S. Surgical Ergonomics and Musculoskeletal Pain in Orthopaedic Surgery Residents: A Multicenter Survey Study. JAAOS Glob. Res. Rev. 2021, 5. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.; Raoof, M.; Fong, Y.; Dellinger, T.; Warner, S. Who is hurting? A prospective study of surgeon ergonomics. Surg. Endosc. 2022, 36, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Bodin, J.; Ha, C.; Chastang, J.-F.; Descatha, A.; Leclerc, A.; Goldberg, M.; Imbernon, E.; Roquelaure, Y. Comparison of risk factors for shoulder pain and rotator cuff syndrome in the working population. Am. J. Ind. Med. 2012, 55, 605–615. [Google Scholar] [CrossRef] [Green Version]
- Dopsaj, M.; Kukić, F.; Đorđević-Nikić, M.; Koropanovski, N.; Radovanović, D.; Miljuš, D.; Subošić, D.; Tomanić, M.; Dopsaj, V. Indicators of Absolute and Relative Changes in Skeletal Muscle Mass during Adulthood and Ageing. Int. J. Environ. Res. Public Health 2020, 17, 5977. [Google Scholar] [CrossRef] [PubMed]
- Surma-Aho, A.; Hölttä-Otto, K.; Nelskylä, K.; Lindfors, N.C. Usability issues in the operating room—Towards contextual design guidelines for medical device design. Appl. Ergon. 2020, 90, 103221. [Google Scholar] [CrossRef] [PubMed]
- Barnard, E.; Sheaffer, K.; Hampton, S.; Measel, M.L.; Farag, A.; Shaw, C. Ergonomics and Work-Related Musculoskeletal Disorders: Characteristics Among Female Interventionists. Cureus 2021, 13, e18226. [Google Scholar] [CrossRef] [PubMed]
- Tokyo Medical University ‘Changed Female Exam Scores’. Available online: https://www.bbc.com/news/world-asia-45043818 (accessed on 30 May 2022).
- Wallis, C.J.D.; Jerath, A.; Coburn, N.; Klaassen, Z.; Luckenbaugh, A.N.; Magee, D.E.; Hird, A.E.; Armstrong, K.; Ravi, B.; Esnaola, N.F.; et al. Association of Surgeon-Patient Sex Concordance with Postoperative Outcomes. JAMA Surg. 2022, 157, 146. [Google Scholar] [CrossRef]
- Tong, A.; Oberbauer, R.; Bellini, M.I.; Budde, K.; Caskey, F.J.; Dobbels, F.; Pengel, L.; Rostaing, L.; Schneeberger, S.; Naesens, M. Patient-Reported Outcomes as Endpoints in Clinical Trials of Kidney Transplantation Interventions. Transpl. Int. 2022, 35, 10134. [Google Scholar] [CrossRef]
- Wallis, C.J.; Ravi, B.; Coburn, N.; Nam, R.K.; Detsky, A.S.; Satkunasivam, R. Comparison of postoperative outcomes among patients treated by male and female surgeons: A population based matched cohort study. BMJ 2017, 359, j4366. [Google Scholar] [CrossRef] [Green Version]
- Rassweiler, J.J.; Klein, J.; Tschada, A.; Gözen, A.S. Laparoscopic retroperitoneal partial nephrectomy using an ergonomic chair -demonstration of technique and matched-pair analysis. Br. J. Urol. 2016, 119, 349–357. [Google Scholar] [CrossRef]
- Sudoł-Szopińska, I.; Bogdan, A.; Szopinski, T.; Panorska, A.K.; Kołodziejczak, M. Prevalence of Chronic Venous Disorders Among Employees Working in Prolonged Sitting and Standing Postures. Int. J. Occup. Saf. Ergon. 2011, 17, 165–173. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Selection | Comparability | Outcome | Total |
|---|---|---|---|---|
| Adams et al. [13] | 2 | 2 | ||
| Aitchison et al. [14] | 3 | 1 | 4 | |
| Armijo et al. [15] | 3 | 1 | 4 | |
| Berguer et al. [10] | 2 | 2 | ||
| Cavanagh et al. [16] | 2 | 2 | ||
| Dalsgaard et al. [17] | 3 | 1 | 4 | |
| Gonzalez et al. [18] | 3 | 1 | 4 | |
| Harutunian et al. [19] | 2 | 2 | ||
| Hokenstad et al. [20] | 3 | 1 | 4 | |
| Jensen et al. [21] | 2 | 2 | ||
| Kono et al. (2012) [22] | 2 | 2 | ||
| Kono et al. (2014) [9] | 3 | 1 | 4 | |
| McQuivey et al. [23] | 2 | 2 | ||
| Stewart et al. [24] | 2 | 2 | ||
| Sutton et al. [8] | 2 | 2 |
| Study | Specialty | Country | Method | Percentage of Female Participants (Female/Total Participants) | Findings |
|---|---|---|---|---|---|
| Adams et al. [13] | Gynaecology | USA | 19-item survey on demographics, surgical practice patterns, physical symptom duration, and effect on work or leisure activities | 49.7% (246/495) | Musculoskeletal symptoms are highly prevalent, and female sex is associated with an approximately twofold risk of reported pain in the lower back region (p = 0.02), in the upper back (p = 0.002), and in the wrist/hand region (p = 0.001) |
| Aitchison et al. [14] | Gynaecology | Australia | Observational: video recordings of 18 surgeons | 83.3% (15/18) | Shorter surgeons maintain significantly greater degrees of neck rotation when looking at the monitor (p < 0.003). Surgeons with shorter arm lengths spend longer time in extreme positions with their non-dominant shoulder at >90° (p = 0.04) and elbow at >120° (p < 0.001) |
| Armijo et al. [15] | General surgery | USA | Observational: evaluation of muscle group activation during surgery via electromyography | 44.4% (8/18) | Increase in muscle activation is observed for female laparoscopic surgeons (p < 0.001). Self-perceived sensory (p = 0.026) and cognitive (p = 0.045) fatigue scores are higher among female surgeons at the end of the surgery. |
| Berguer et al. [10] | General surgery | USA | Online survey on demographic and practice data, musculoskeletal symptoms, and the perceived difficulty in using several types of laparoscopic instruments | 21.9% (159/726) | Hand size is a significant determinant of difficulty using laparoscopic surgical instruments, particularly for sizes 6.5 or smaller (p < 0.001) |
| Cavanagh et al. [16] | Otorhinolaryngology | USA | 28-item online survey on demographics, surgical practice characteristics, physical symptoms, and ergonomics | 15.0% (15/100) | Female surgeons report higher experience of pain/discomfort associated with their surgical practice (p = 0.033) |
| Dalsgaard et al. [17] | Gynaecology | Denmark | Observational (semi-randomised): bipolar surface electromyogram; calculation of gaps per minute plus static and peak muscle activation were calculated during surgeries | 58.3% (7/12) | Neck and static shoulder muscle activities are lower in robotic surgery compared to laparoscopy (p < 0.05) |
| Gonzalez et al. [18] | General surgery | Spain | Observational: Trial to determine the optimal diameter of the handle from an ergonomic point of view | 51.1% (69/135) | The optimal diameter of the instrument’s handle differs according to the hand size, especially for smaller hands (p < 0.05) |
| Harutunian et al. [19] | Dentistry | Spain | 19-item survey on demographics and questions regarding ergonomics of the instrument holder and resulting musculoskeletal disorders | 52.7% (39/74) | Most of the dentists experience musculoskeletal pain, and women show a higher frequency of intense pain (p < 0.05) |
| Hokenstad et al. [20] | Gynaecology | USA | Inertial measurement and survey before and after ergonomic implementation during robotic hysterectomy | 50.0% (3/6) | Improved objective surgeon posture at the console when compared with the surgeons’ self-selected settings: neck (p = 0 .008) and right upper arm (p = 0.02) |
| Jensen et al. [21] | Endocrine surgery | USA | 43-item online survey on demographics, surgical information, prevalence of musculoskeletal symptoms, and pursued therapy/treatment; ergonomic recommendations | 32.9% (72/220) | Women more likely to report pain and stiffness after surgery (p = 0.004). Most common locations are the neck and shoulder |
| Kono et al. (2012) [22] | General surgery | Japan | 9-item online survey on demographics and questions regarding circular and linear staplers | 30.4% (74/243) | Surgeons with small glove sizes express a low satisfaction level regarding the anastomotic staplers (p < 0.0001), suggesting a need to develop instruments whose usability is not affected by different hand sizes and lengths of fingers |
| Kono et al. (2014) [9] | General surgery | Japan | Observational: evaluation of the relationship between grip width and the operation force required to push the lever of the stapler | 53.7% (61/113) | Men have wider optimal grip width than women for both the dominant and non-dominant hands (p < 0.001) |
| McQuivey et al. [23] | Orthopaedics | USA | Online survey on demographics, symptoms by body part, and attitudes/beliefs/behaviours regarding surgical ergonomics | 27.6% (21/76) | No sex-specific differences, but concerns about implications for work satisfaction (p = 0.005), burnout (b = 0.04), and callousness toward others (p < 0.0001) |
| Stewart et al. [24] | General surgery | USA | Survey on demographics, the surgery performed, intraoperative ergonomics, and task load during surgery | 28.2% (24/85) | Short surgeons and male surgeons report more pain after both open and robotic operations (p < 0.001). |
| Sutton et al. [8] | General surgery | USA | 23-item online survey on demographics, physical symptoms, ergonomics, and environment/equipment | 17.2 % (54/314) | Female surgeons experience more treatment for their hands (p = 0.028). Women with a size 5.5–6.5 surgical glove report discomfort in their shoulder area more commonly than men with the same surgical glove size (p = 0.004). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellini, M.I.; Amabile, M.I.; Saullo, P.; Zorzetti, N.; Testini, M.; Caronna, R.; D’Andrea, V. A Woman’s Place Is in Theatre, but Are Theatres Designed with Women in Mind? A Systematic Review of Ergonomics for Women in Surgery. J. Clin. Med. 2022, 11, 3496. https://doi.org/10.3390/jcm11123496
Bellini MI, Amabile MI, Saullo P, Zorzetti N, Testini M, Caronna R, D’Andrea V. A Woman’s Place Is in Theatre, but Are Theatres Designed with Women in Mind? A Systematic Review of Ergonomics for Women in Surgery. Journal of Clinical Medicine. 2022; 11(12):3496. https://doi.org/10.3390/jcm11123496
Chicago/Turabian StyleBellini, Maria Irene, Maria Ida Amabile, Paolina Saullo, Noemi Zorzetti, Mario Testini, Roberto Caronna, and Vito D’Andrea. 2022. "A Woman’s Place Is in Theatre, but Are Theatres Designed with Women in Mind? A Systematic Review of Ergonomics for Women in Surgery" Journal of Clinical Medicine 11, no. 12: 3496. https://doi.org/10.3390/jcm11123496
APA StyleBellini, M. I., Amabile, M. I., Saullo, P., Zorzetti, N., Testini, M., Caronna, R., & D’Andrea, V. (2022). A Woman’s Place Is in Theatre, but Are Theatres Designed with Women in Mind? A Systematic Review of Ergonomics for Women in Surgery. Journal of Clinical Medicine, 11(12), 3496. https://doi.org/10.3390/jcm11123496