
Exercise throughout Pregnancy Prevents Excessive Maternal Weight Gain during the COVID-19 Pandemic: A Randomized Clinical Trial

 ,
,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient and Public Involvement
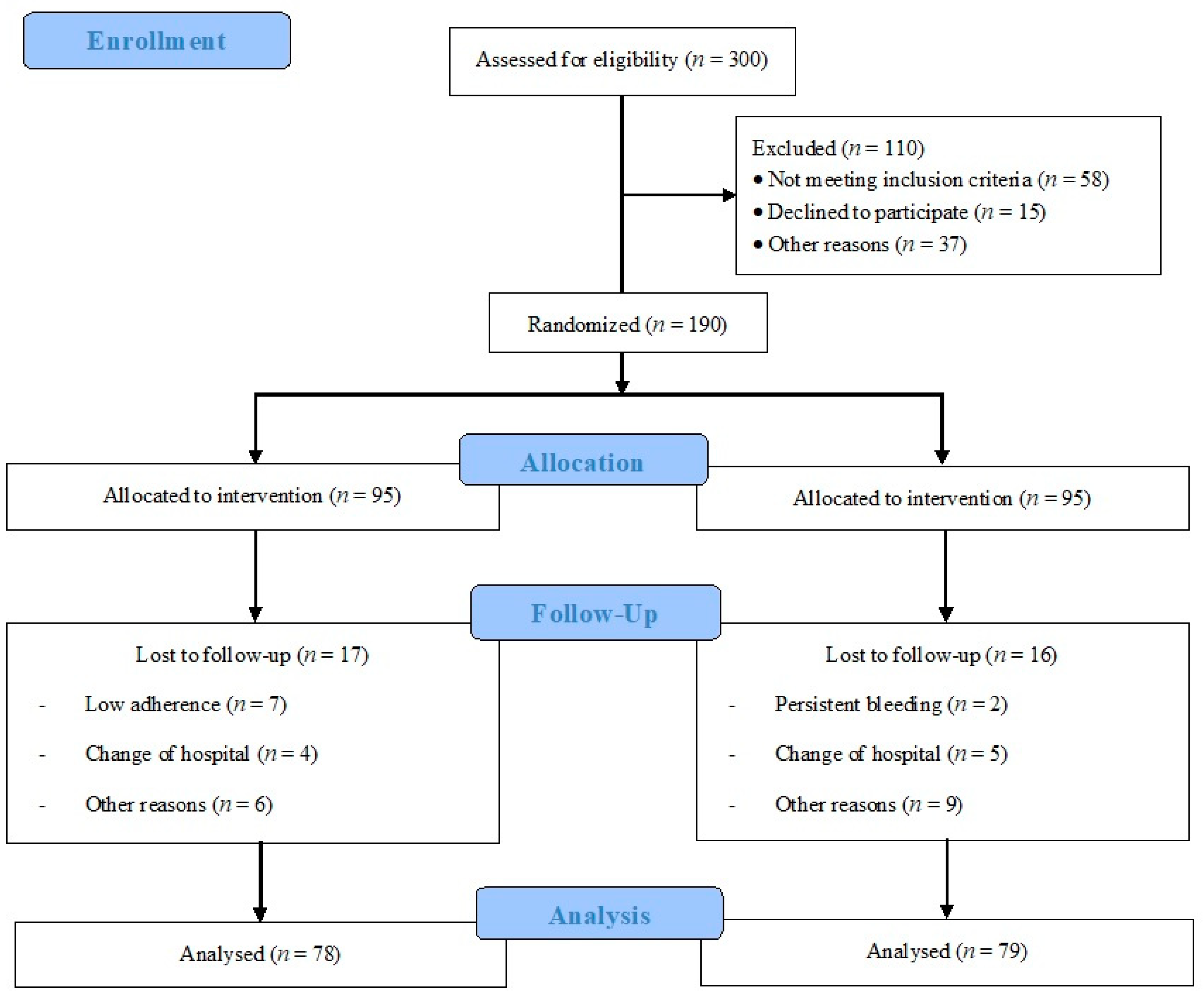
2.3. Participants and Randomization
2.4. Intervention
- Warm-up with general exercises: range of motion varied, but impact activities were not included (avoiding jumps and falls);
- Aerobic exercises: exercises were performed to increase the intensity up to that of moderate activities, 55–65% of heart rate reserve using the Karvonen formula and a range of 12–14 of Borg Rate of Perceived Exertion Scale (somewhat hard);
- Muscle strengthening and general toning exercises of the whole body: Exercises for the lower extremities (calf, quadriceps, hamstrings, adductors, and abductors) and torso (abdominal, pectoral, shoulders, and paravertebral musculature) were included. The muscle groups to train must be distributed into the three weekly sessions. During each session, one or two sets of 10–12 repetitions must be performed from each muscle group using barbells (2–3 kg/exercise) or low-to-medium resistance (elastic) bands (TheraBand’s). Exercises for the most weakened muscle groups (overall regarding lower limbs and thoracolumbar muscles) during pregnancy were also included, as the aim was to avoid muscular decompensation;
- Coordination and balance exercises: simple eye–hand and eye–foot coordination tasks were performed with sports equipment, as well as body axis balance exercises;
- Strengthening the pelvic floor muscles: Kegel exercises were performed;
- Cool-down section of 7–8 min: the aim was to gradually lower the intensity of work with flexibility, stretching, and relaxation exercises;
- Final discussion: The aim of this section was to have the pregnant participants express clearly and openly the sensations and perceptions they experienced during the training session. This part was conducted only during the group virtual session.
- Individual work (two weekly sessions): recorded sessions, with complete visual information and instructions regarding the exercises to be performed. These sessions were designed so that pregnant participants could follow easily and intuitively, with simple access for downloading;
- Group work (one weekly session): classes were supervised online through the video platform (Zoom Video Communications Inc., San José, CA, USA).
- Participants had to send the two sessions weekly by means of videos to one of the researchers as evidence of the exercise session performed;
- Attendance was easily monitored based on the registration tool obtained by the computer application.
2.5. Usual Care (Control) Group
2.6. Outcomes
2.6.1. Primary Outcome
2.6.2. Secondary Outcomes
2.7. Statistical Analysis
2.8. Sample Size Calculation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reichetzeder, C. Overweight and obesity in pregnancy: Their impact on epigenetics. Eur. J. Clin. Nutr. 2021, 75, 1710–1722. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, K.M.; Becker, C.; Healy, H.; Wilcox, S.; Liu, J. Women’s Report of Health Care Provider Advice and Gestational Weight Gain: A Systematic Review. J. Womens Health 2021, 30, 73–89. [Google Scholar] [CrossRef] [PubMed]
- Bautista-Castaño, I.; Henriquez-Sanchez, P.; Alemán-Perez, N.; Garcia-Salvador, J.J.; Gonzalez-Quesada, A.; García-Hernández, J.A.; Serra-Majem, L. Maternal obesity in early pregnancy and risk of adverse outcomes. PLoS ONE 2013, 8, e80410. [Google Scholar] [CrossRef] [Green Version]
- Jago, C.A.; Singh, S.S.; Moretti, F. Coronavirus Disease 2019 (COVID-19) and Pregnancy: Combating Isolation to Improve Outcomes. Obstet. Gynecol. 2020, 136, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Barakat, R.; Perales, M.; Garatachea, N.; Ruiz, J.R.; Lucía, A. Exercise during pregnancy. A narrative review asking: What do we know? Br. J. Sports Med. 2015, 49, 1377–1381. [Google Scholar] [CrossRef] [Green Version]
- Perales, M.; Artal, R.; Lucia, A. Exercise During Pregnancy. JAMA 2017, 317, 1113–1114. [Google Scholar] [CrossRef]
- Wang, J.; Wen, D.; Liu, X.; Liu, Y. Impact of exercise on maternal gestational weight gain: An updated meta-analysis of randomized controlled trials. Medicine 2019, 98, e16199. [Google Scholar] [CrossRef]
- Silva-Jose, C.; Sánchez-Polán, M.; Diaz-Blanco, Á.; Coterón, J.; Barakat, R.; Refoyo, I. Effectiveness of a Virtual Exercise Program During COVID-19 Confinement on Blood Pressure Control in Healthy Pregnant Women. Front. Physiol. 2021, 12, 645136. [Google Scholar] [CrossRef]
- Silva-Jose, C.; Sánchez-Polán, M.; Díaz-Blanco, Á.; Pérez-Medina, T.; Carrero Martínez, V.; Alzola, I.; Barakat, R.; Refoyo, I.; Mottola, M.F. Influence of a Virtual Exercise Program throughout Pregnancy during the COVID-19 Pandemic on Perineal Tears and Episiotomy Rates: A Randomized Clinical Trial. J. Clin. Med. 2021, 10, 5250. [Google Scholar] [CrossRef]
- Mottola, M.F.; Davenport, M.H.; Ruchat, S.M.; Davies, G.A.; Poitras, V.J.; Gray, C.E.; Jaramillo, A.; Barrowman, N.; Adamo, K.B.; Duggan, M.; et al. 2019 Canadian guideline for physical activity throughout pregnancy. Br. J. Sports Med. 2018, 52, 1339–1346. [Google Scholar] [CrossRef] [Green Version]
- American College of Obstetricians and Gynecologists. Physical Activity and Exercise During Pregnancy and the Postpartum Period: ACOG Committee Opinion, Number 804. Obstet. Gynecol. 2020, 135, e178–e188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barakat, R.; Díaz-Blanco, A.; Franco, E.; Rollán-Malmierca, A.; Brik, M.; Vargas, M.; Silva, C.; Sánchez-Polán, M.; Gil, J.; Perales, M.; et al. Guías clínicas para el ejercicio físico durante el embarazo. Prog. Obstet. Ginecol. 2019, 62, 464–471. [Google Scholar] [CrossRef]
- Barakat, R. An exercise program throughout pregnancy: Barakat model. Birth Defects Res. 2021, 113, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Barakat, R.; Pelaez, M.; Cordero, Y.; Perales, M.; Lopez, C.; Coteron, J.; Mottola, M.F. Exercise during pregnancy protects against hypertension and macrosomia: Randomized clinical trial. Am. J. Obstet. Gynecol. 2016, 214, 649.e1–649.e8. [Google Scholar] [CrossRef]
- Rasmussen, K.M.; Yaktine, A.L. Weight Gain during Pregnancy; Institute of Medicine (US), National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines, Eds.; National Institutes of Health: Washington, DC, USA, 2009.
- Ruiz, J.R.; Perales, M.; Pelaez, M.; Lopez, C.; Lucia, A.; Barakat, R. Supervised exercise-based intervention to prevent excessive gestational weight gain: A randomized controlled trial. Mayo Clin. Proc. 2013, 88, 1388–1397. [Google Scholar] [CrossRef]
- Moher, D.; Dulberg, C.S.; Wells, G.A. Statistical power, sample size, and their reporting in randomized controlled trials. JAMA 1994, 272, 122–124. [Google Scholar] [CrossRef]
- Schulz, K.F.; Grimes, D.A. Sample size calculations in randomised trials: Mandatory and mystical. Lancet 2005, 365, 1348–1353. [Google Scholar] [CrossRef]
- Barakat, R.; Refoyo, I.; Coteron, J.; Franco, E. Exercise during pregnancy has a preventative effect on excessive maternal weight gain and gestational diabetes. A randomized controlled trial. Braz. J. Phys. Ther. 2019, 23, 148–155. [Google Scholar] [CrossRef]
- Pelaez, M.; Gonzalez-Cerron, S.; Montejo, R.; Barakat, R. Protective Effect of Exercise in Pregnant Women Including Those Who Exceed Weight Gain Recommendations: A Randomized Controlled Trial. Mayo Clin. Proc. 2019, 94, 1951–1959. [Google Scholar] [CrossRef]
- Haakstad, L.A.; Bø, K. Effect of regular exercise on prevention of excessive weight gain in pregnancy: A randomised controlled trial. Eur. J. Contracept. Reprod. Health Care 2011, 16, 116–125. [Google Scholar] [CrossRef]
- Sánchez-García, J.C.; Aguilar Cordero, M.J.; Menor-Rodríguez, M.J.; Paucar Sánchez, A.M. Influencia del ejercicio físico en la evolución del peso gestacional y posparto. Ensayo clínico aleatorizado [Influence of exercise on weight gain during pregnancy. Randomized clinical trial]. Nutr. Hosp. 2019, 36, 931–938. [Google Scholar] [CrossRef] [PubMed]
- Vargas-Terrones, M.; Nagpal, T.S.; Barakat, R. Impact of exercise during pregnancy on gestational weight gain and birth weight: An overview. Braz. J. Phys. Ther. 2019, 23, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Ruchat, S.M.; Mottola, M.F.; Skow, R.J.; Nagpal, T.S.; Meah, V.L.; James, M.; Riske, L.; Sobierajski, F.; Kathol, A.J.; Marchand, A.A.; et al. Effectiveness of exercise interventions in the prevention of excessive gestational weight gain and postpartum weight retention: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1347–1356. [Google Scholar] [CrossRef] [PubMed]
- Muktabhant, B.; Lawrie, T.A.; Lumbiganon, P.; Laopaiboon, M. Diet or exercise, or both, for preventing excessive weight gain in pregnancy. Cochrane Database Syst. Rev. 2015, 6, CD007145. [Google Scholar] [CrossRef] [PubMed]
- Lamina, S.; Agbanusi, E. Effect of aerobic exercise training on maternal weight gain in pregnancy: A meta-analysis of randomized controlled trials. Ethiop. J. Health Sci. 2013, 23, 59–64. [Google Scholar] [PubMed]

{kind=link}
| Maternal Characteristics | |||
|---|---|---|---|
| Variable | Intervention Group (n = 75) | Control Group (n = 79) | |
| Age (years) | 33.85 ± 4.05 | 33.49 ± 5.37 | |
| Maternal height (m) | 1.63 ± 0.06 | 1.62 ± 0.06 | |
| Maternal weight (kg) | 64.02 ± 16.92 | 66.99 ± 15.42 | |
| BMI (n/%) | 23.47 ± 6.37 | 25.01 ± 4.54 | |
| <18.5 | 5/6.7 | 4/5.1 | |
| 18.5 to 24.9 | 54/72.0 | 43/54.4 | |
| 25 to 29.9 | 11/14.7 | 22/27.8 | |
| >30 | 5/6.7 | 10/12.7 | |
| Parity † (n/%) | |||
| None | 54/72.0 | 45/56.9 | |
| One | 17/22.7 | 26/32.9 | |
| Two or more | 4/5.3 | 8/10.2 | |
| Smoking previous pregnancy | |||
| No | 57/76.0 | 50/63.3 | |
| Yes | 18/24 | 29/36.7 | |
| Occupation (n/%) | |||
| Active job | 35/46.7 | 27/34.2 | |
| Sedentary job | 33/44.0 | 36/45.6 | |
| Homemaker | 7/9.3 | 16/20.2 | |
| Previous miscarriage (n/%) | |||
| None | 56/74.7 | 48/60.8 | |
| One | 16/21.3 | 22/27.8 | |
| Two or more | 3/4.0 | 9/11.4 | |
| IG (n = 68) | CG (n = 72) | p-Value | |||
|---|---|---|---|---|---|
| Pre-Pregnancy BMI | n | n/% | n | n/% | |
| <18.5 | 4 | 0/0 | 3 | 1/33.3 | 0.212 |
| 18.5–24.9 | 49 | 0/0 | 40 | 10/25 | 0.001 |
| 25–29.9 | 11 | 2/18 | 20 | 12/60 | 0.025 |
| >30 | 4 | 2/50 | 9 | 8/88.9 | 0.125 |
| IG (n = 68) | CG (n = 72) | p-Value | |||
|---|---|---|---|---|---|
| Total Weight Gain kg | mean ± SD | mean ± SD | |||
| 9.96 ± 3.27 | 12.48 ± 4.87 | 0.001 | |||
| Pre-pregnancy BMI (kg/m2) | n | mean ± SD | n | mean ± SD | |
| <18.5 | 4 | 11.42 ± 2.12 | 3 | 14.25 ± 7.40 | 0.487 |
| 18.5–24.9 | 49 | 10.27 ± 3.29 | 40 | 12.14 ± 4.75 | 0.032 |
| 25–29.9 | 11 | 9.20 ± 3.11 | 20 | 12.90 ± 5.04 | 0.036 |
| >30.0 | 4 | 8.5 ± 3.33 | 9 | 12.41 ± 4.87 | 0.136 |
| IG (n = 68) | CG (n = 72) | p Value | |||
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||
| Pre-pregnancy weight (kg) | 64.02 ± 16.92 | - | 66.99 ± 15.42 | - | 0.258 |
| Gestational Week 22 + 2 | 65.71 ± 12.78 | 1.69 ± 0.41 | 68.66 ± 13.52 | 1.67 ± 0.79 | 0.178 |
| Week 28 + 4 days | 70.03 ± 12.90 | 4.32 ± 0.52 | 75.33 ± 14.80 | 6.67 ± 1.09 | 0.022 |
| Week 36 + 1 day | 72.52 ± 11.46 | 2.49 ± 1.08 | 78.24 ± 15.11 | 2.91 ± 0.57 | 0.010 |
| Final weight (measured at delivery) | 73.06 ± 11.62 | 0.54 ± 1.02 | 78.81 ± 15.01 | 0.57 ± 1.03 | 0.009 |
| IG (n = 69) | CG (n = 70) | p-Value | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Maternal gestational age | 39.07 ± 1.37 | 38.85 ± 1.45 | 0.363 |
| Birth weight | 3197.85 ± 423.95 | 3187.75 ± 462.37 | 0.896 |
| Birth length | 49.94 ± 2.06 | 49.57 ± 2.15 | 0.329 |
| Apgar 1 | 8.81 ± 0.63 | 8.71 ± 1.01 | 0.527 |
| Apgar 5 | 9.93 ± 0.26 | 9.80 ± 0.58 | 0.104 |
| pH cord blood | 7.24 ± 0.07 | 7.23 ± 0.08 | 0.610 |
| Mode of delivery | n/% | n/% | |
| Non-instrumental | 56/81.2 | 44/62.9 | 0.049 |
| Instrumental | 5/7.2 | 8/11.4 | |
| C-section | 8/11.6 | 10/25.7 | |
| Type of delivery | n/% | n/% | |
| Full term > 37 wk | 64/92.8 | 62/88.6 | 0.257 |
| Preterm < 37 wk | 5/7.2 | 8/11.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva-Jose, C.; Sánchez-Polán, M.; Barakat, R.; Díaz-Blanco, Á.; Carrero Martínez, V.; García Benasach, F.; Alzola, I.; Mottola, M.F.; Refoyo, I. Exercise throughout Pregnancy Prevents Excessive Maternal Weight Gain during the COVID-19 Pandemic: A Randomized Clinical Trial. J. Clin. Med. 2022, 11, 3392. https://doi.org/10.3390/jcm11123392
Silva-Jose C, Sánchez-Polán M, Barakat R, Díaz-Blanco Á, Carrero Martínez V, García Benasach F, Alzola I, Mottola MF, Refoyo I. Exercise throughout Pregnancy Prevents Excessive Maternal Weight Gain during the COVID-19 Pandemic: A Randomized Clinical Trial. Journal of Clinical Medicine. 2022; 11(12):3392. https://doi.org/10.3390/jcm11123392
Chicago/Turabian StyleSilva-Jose, Cristina, Miguel Sánchez-Polán, Rubén Barakat, Ángeles Díaz-Blanco, Vanessa Carrero Martínez, Fátima García Benasach, Irune Alzola, Michelle F. Mottola, and Ignacio Refoyo. 2022. "Exercise throughout Pregnancy Prevents Excessive Maternal Weight Gain during the COVID-19 Pandemic: A Randomized Clinical Trial" Journal of Clinical Medicine 11, no. 12: 3392. https://doi.org/10.3390/jcm11123392
APA StyleSilva-Jose, C., Sánchez-Polán, M., Barakat, R., Díaz-Blanco, Á., Carrero Martínez, V., García Benasach, F., Alzola, I., Mottola, M. F., & Refoyo, I. (2022). Exercise throughout Pregnancy Prevents Excessive Maternal Weight Gain during the COVID-19 Pandemic: A Randomized Clinical Trial. Journal of Clinical Medicine, 11(12), 3392. https://doi.org/10.3390/jcm11123392