
Usefulness of Procalcitonin as a Predictor of Long-Term Prognosis in the Early Postoperative Period after Esophagectomy for Esophageal Cancer

 , and
, and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Blood Assessment for PCT and Determination of the Cutoff Value
2.3. Treatment and Postoperative Complications
2.4. Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Relationship between PCT and Postoperative Infectious Complications at 2 POD, 4 POD, and 7 POD
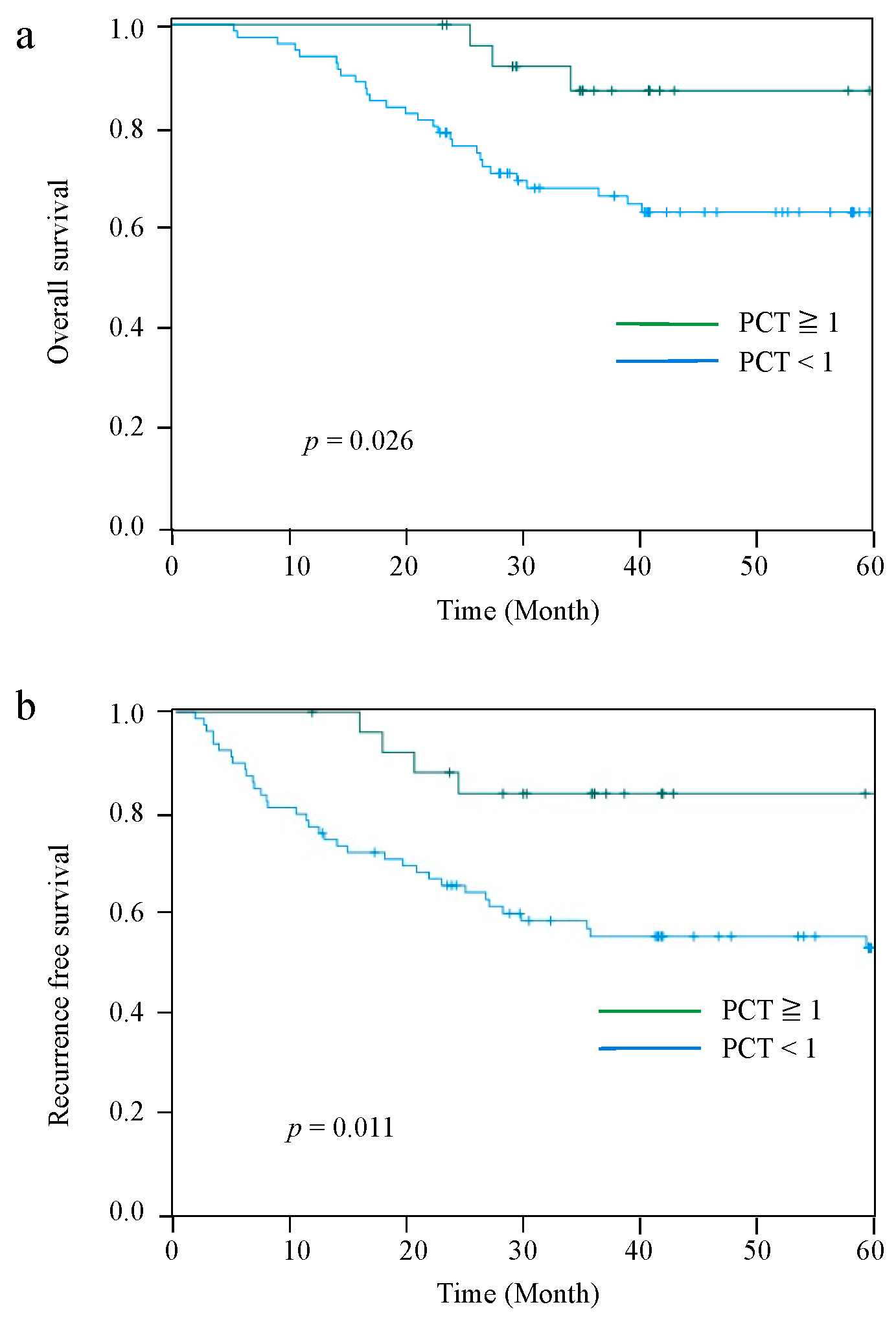
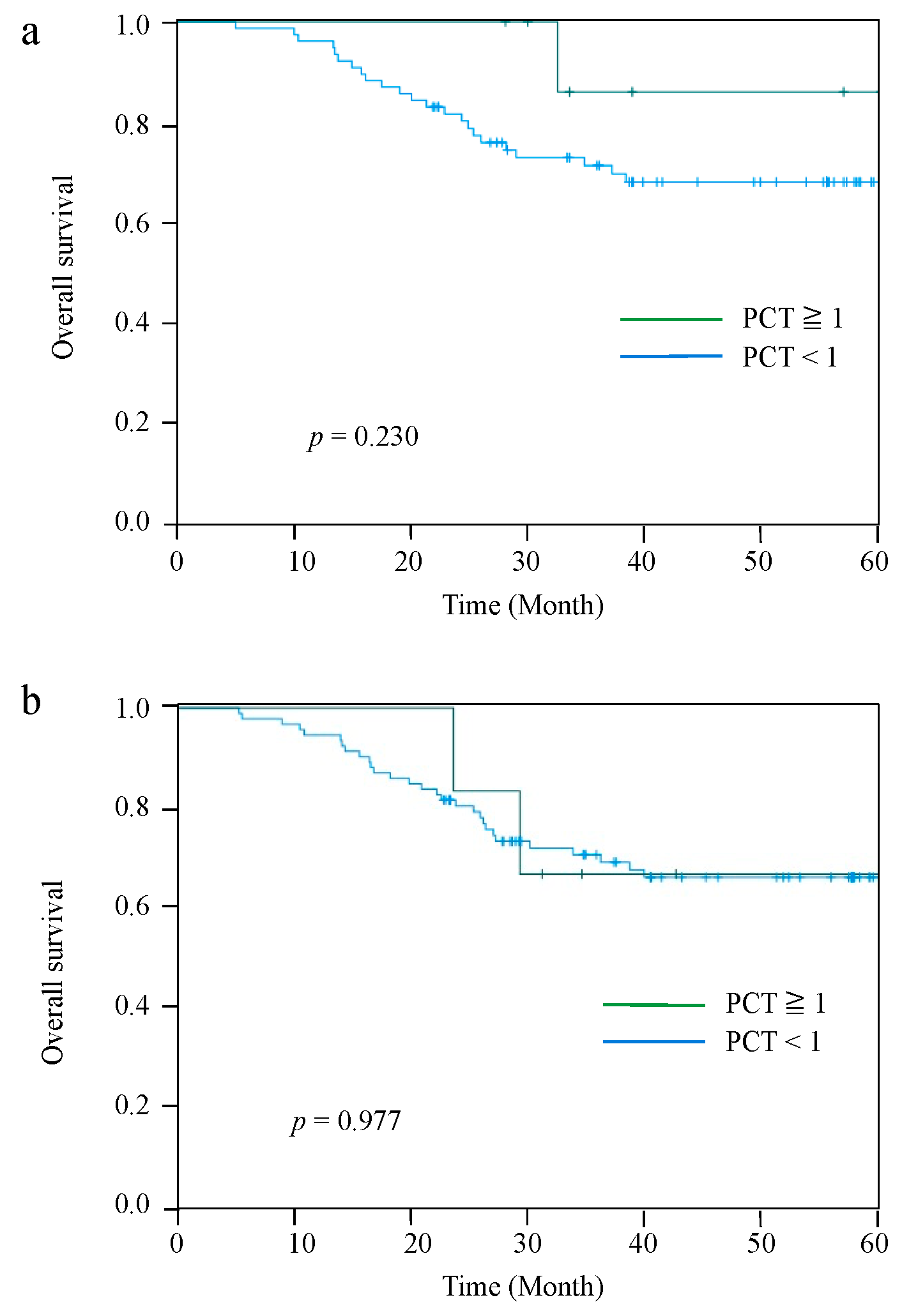
3.3. Patient Survival and Disease Recurrence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kitagawa, Y.; Uno, T.; Oyama, T.; Kato, K.; Kato, H.; Kawakubo, H.; Kawamura, O.; Kusano, M.; Kuwano, H.; Takeuchi, H.; et al. Esophageal cancer practice guidelines 2017 edited by the Japan Esophageal Society: Part 1. Esophagus 2019, 16, 1–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitagawa, Y.; Uno, T.; Oyama, T.; Kato, K.; Kato, H.; Kawakubo, H.; Kawamura, O.; Kusano, M.; Kuwano, H.; Takeuchi, H.; et al. Esophageal cancer practice guidelines 2017 edited by the Japan esophageal society: Part 2. Esophagus 2019, 16, 25–43. [Google Scholar] [CrossRef] [PubMed]
- Booka, E.; Takeuchi, H.; Suda, K.; Fukuda, K.; Nakamura, R.; Wada, N.; Kawakubo, H.; Kitagawa, Y. Meta-analysis of the impact of postoperative complications on survival after oesophagectomy for cancer. BJS Open 2018, 2, 276–284. [Google Scholar] [CrossRef]
- Nylen, E.S.; O’Neill, W.; Jordan, M.H.; Snider, R.H.; Moore, C.F.; Lewis, M.; Silva, O.L.; Becker, K.L. Serum procalcitonin as an index of inhalation injury in burns. Horm. Metab. Res. 1992, 24, 439–443. [Google Scholar] [CrossRef]
- Becker, K.L.; Nylén, E.S.; White, J.C.; Müller, B.; Snider, R.H.J. Clinical review 167: Procalcitonin and the calcitonin gene family of peptides in inflammation, infection, and sepsis: A journey from calcitonin back to its precursors. J. Clin. Endocrinol. Metab. 2004, 89, 1512–1525. [Google Scholar] [CrossRef] [Green Version]
- Linscheid, P.; Seboek, D.; Nylen, E.S.; Langer, I.; Schlatter, M.; Becker, K.L.; Keller, U.; Müller, B. In vitro and in vivo calcitonin I gene expression in parenchymal cells: A novel product of human adipose tissue. Endocrinology 2003, 144, 5578–5584. [Google Scholar] [CrossRef]
- Müller, B.; Peri, G.; Doni, A.; Perruchoud, A.P.; Landmann, R.; Pasqualini, F.; Mantovani, A. High circulating levels of the IL-1 type II decoy receptor in critically ill patients with sepsis: Association of high decoy receptor levels with glucocorticoid administration. J. Leukoc. Biol. 2002, 72, 643–649. [Google Scholar]
- Asti, E.; Bonitta, G.; Melloni, M.; Tornese, S.; Milito, P.; Sironi, A.; Costa, E.; Bonavina, L. Utility of C-reactive protein as predictive biomarker of anastomotic leak after minimally invasive esophagectomy. Langenbecks Arch. Surg./Dtsch. Ges. Fur Chir. 2018, 403, 235–244. [Google Scholar] [CrossRef]
- Bogar, L.; Molnar, Z.; Tarsoly, P.; Kenyeres, P.; Marton, S. Serum procalcitonin level and leukocyte antisedimentation rate as early predictors of respiratory dysfunction after oesophageal tumour resection. Crit. Care 2006, 10, R110. [Google Scholar] [CrossRef] [Green Version]
- Ito, S.; Sato, N.; Kojika, M.; Yaegashi, Y.; Suzuki, Y.; Suzuki, K.; Endo, S. Serum procalcitonin levels are elevated in esophageal cancer patients with postoperative infectious complications. Eur. Surg. Research. Eur. Chir. Forschung. Rech. Chir. Eur. 2005, 37, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Wang, D.; Wei, W.; Ouyang, L.; Lou, N. The predictive value of coefficient of PCT × BG for anastomotic leak in esophageal carcinoma patients with ARDS after esophagectomy. J. Intensive Care Med. 2019, 34, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumors, 8th ed.; Wiley: New York, NY, USA, 2017. [Google Scholar]
- Booka, E.; Kikuchi, H.; Haneda, R.; Soneda, W.; Kawata, S.; Murakami, T.; Matsumoto, T.; Hiramatsu, Y.; Takeuchi, H. Short-term outcomes of robot-assisted minimally invasive esophagectomy compared with thoracoscopic or transthoracic esophagectomy. Anticancer. Res. 2021, 41, 4455–4462. [Google Scholar] [CrossRef] [PubMed]
- Haneda, R.; Hiramatsu, Y.; Kawata, S.; Honke, J.; Soneda, W.; Matsumoto, T.; Morita, Y.; Kikuchi, H.; Kamiya, K.; Takeuchi, H. Survival impact of perioperative changes in prognostic nutritional index levels after esophagectomy. Esophagus 2022, 19, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Christ-Crain, M.; Müller, B. Procalcitonin in bacterial infections—Hype, hope, more or less? Swiss Med. Wkly. 2005, 135, 451–460. [Google Scholar]
- Carsin, H.; Assicot, M.; Feger, F.; Roy, O.; Pennacino, I.; Le Bever, H.; Ainaud, P.; Bohuon, C. Evolution and significance of circulating procalcitonin levels compared with IL-6, TNF alpha and endotoxin levels early after thermal injury. Burns 1997, 23, 218–224. [Google Scholar] [CrossRef]
- von Heimburg, D.; Stieghorst, W.; Khorram-Sefat, R.; Pallua, N. Procalcitonin—A sepsis parameter in severe burn injuries. Burns 1998, 24, 745–750. [Google Scholar] [CrossRef]
- Brunkhorst, F.M.; Heinz, U.; Forycki, Z.F. Kinetics of procalcitonin in iatrogenic sepsis. Intensive Care Med. 1998, 24, 888–889. [Google Scholar] [CrossRef]
- Assicot, M.; Gendrel, D.; Carsin, H.; Raymond, J.; Guilbaud, J.; Bohuon, C. High serum procalcitonin concentrations in patients with sepsis and infection. Lancet 1993, 341, 515–518. [Google Scholar] [CrossRef]
- Matsuda, S.; Takeuchi, H.; Kawakubo, H.; Fukuda, K.; Nakamura, R.; Takahashi, T.; Wada, N.; Saikawa, Y.; Kitagawa, Y. Correlation between intense postoperative inflammatory response and survival of esophageal cancer patients who underwent transthoracic esophagectomy. Ann. Surg. Oncol. 2015, 22, 4453–4460. [Google Scholar] [CrossRef] [PubMed]
- Booka, E.; Kikuchi, H.; Hiramatsu, Y.; Takeuchi, H. The impact of infectious complications after esophagectomy for esophageal cancer on cancer prognosis and treatment strategy. J. Clin. Med. 2021, 10, 4614. [Google Scholar] [CrossRef] [PubMed]
- Kawata, S.; Hiramatsu, Y.; Shirai, Y.; Watanabe, K.; Nagafusa, T.; Matsumoto, T.; Kikuchi, H.; Kamiya, K.; Takeuchi, H. Multidisciplinary team management for prevention of pneumonia and long-term weight loss after esophagectomy: A single-center retrospective study. Esophagus 2020, 17, 270–278. [Google Scholar] [CrossRef] [Green Version]
- Zylstra, J.; Whyte, G.P.; Beckmann, K.; Pate, J.; Santaolalla, A.; Gervais-Andre, L.; Russell, B.; Maisey, N.; Waters, J.; Tham, G.; et al. Exercise prehabilitation during neoadjuvant chemotherapy may enhance tumour regression in oesophageal cancer: Results from a prospective non-randomised trial. Br. J. Sports Med. 2022, 56, 402–409. [Google Scholar] [CrossRef]
- Noma, T.; Makino, T.; Ohshima, K.; Sugimura, K.; Miyata, H.; Honma, K.; Yamashita, K.; Saito, T.; Tanaka, K.; Yamamoto, K.; et al. Immunoscore signatures in surgical specimens and tumor-infiltrating lymphocytes in pretreatment biopsy predict treatment efficacy and survival in esophageal cancer. Ann. Surg. 2021. Epub ahed of print. [Google Scholar] [CrossRef]
- Nylen, E.S.; Whang, K.T.; Snider, R.H.J.; Steinwald, P.M.; White, J.C.; Becker, K.L. Mortality is increased by procalcitonin and decreased by an antiserum reactive to procalcitonin in experimental sepsis. Crit. Care Med. 1998, 26, 1001–1006. [Google Scholar] [CrossRef]
- Kelly, R.J.; Ajani, J.A.; Kuzdzal, J.; Zander, T.; Van Cutsem, E.; Piessen, G.; Mendez, G.; Feliciano, J.; Motoyama, S.; Lièvre, A.; et al. Adjuvant Nivolumab in resected esophageal or gastroesophageal junction cancer. N. Engl. J. Med. 2021, 384, 1191–1203. [Google Scholar] [CrossRef]
- Lazzarin, G.; Di Furia, M.; Romano, L.; Di Sibio, A.; Di Giacomo, C.; Lombardi, L.; Giuliani, A.; Schietroma, M.; Pessia, B.; Carlei, F.; et al. Endoscopic Double-Pigtail Catheter (EDPC) internal drainage as first-line treatment of gastric leak: A case series during laparoscopic sleeve gastrectomy learning curve for morbid obesity. Minim. Invasive Surg. 2020, 2020, 8250904. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| All Cases n = 105 | PCT-High n = 26 | PCT-Low n = 79 | p Value | |
|---|---|---|---|---|
| Age (median, years) † | 67 (42–82) | 66 (48–78) | 67 (42–82) | 0.992 |
| Sex (%) | 0.880 | |||
| Male | 92 (87.6%) | 23 (88.5%) | 69 (87.3%) | |
| Female | 13 (12.4%) | 3 (11.5%) | 10 (12.7%) | |
| Preoperative body weight (median, kg) † | 57.3 (36.0–82.0) | 56.4 (41.6–78.3) | 58.2 (36.0–82.0) | 0.796 |
| Preoperative BMI (median, kg/m2) † | 21.2 (14.2–28.9) | 21.3 (16.2–28.1) | 21.1 (14.2–28.9) | 0.749 |
| Location of tumor (%) | 0.162 | |||
| Ut | 11 (10.5%) | 2 (7.7%) | 9 (11.4%) | |
| Mt | 60 (57.1%) | 19 (73.1%) | 41 (51.9%) | |
| Lt and Ae | 34 (32.4%) | 5 (19.2%) | 29 (36.7%) | |
| Clinical Stage, TNM 8th (%) | 0.140 | |||
| Stage I | 48 (45.7%) | 11 (42.3%) | 37 (46.8%) | |
| Stage II | 26 (24.8%) | 4 (15.4%) | 22 (27.8%) | |
| Stage III | 28 (26.7%) | 11 (42.3%) | 17 (21.5%) | |
| Stage IVA | 3 (2.9%) | 0 (0.0%) | 3 (3.8%) | |
| Preoperative therapy (%) | 0.952 | |||
| None | 56 (53.3%) | 14 (53.8%) | 42 (53.2%) | |
| NAC | 49 (46.7%) | 12 (46.2%) | 37 (46.8%) | |
| Multidisciplinary team support (%) | 50 (47.6%) | 18 (69.2%) | 32 (40.5%) | 0.011 |
| Thoracotomy (%) | 0.776 | |||
| Open | 54 (51.4%) | 14 (53.8%) | 40 (50.6%) | |
| MIE | 51 (48.6%) | 12 (46.2%) | 39 (49.4%) | |
| Laparotomy (%) | 0.602 | |||
| Open | 45 (42.9%) | 10 (38.5%) | 35 (44.3%) | |
| Laparoscopy | 60 (57.1%) | 16 (61.5%) | 44 (55.7%) | |
| LN dissection (%) | 0.128 | |||
| 2-field | 13 (12.4%) | 1 (3.8%) | 12 (15.2%) | |
| 3-field | 92 (87.6%) | 25 (96.2%) | 67 (84.8%) | |
| Reconstruct organ (%) | 0.105 | |||
| Gastric conduit | 99 (94.3%) | 26 (100%) | 73 (92.4%) | |
| Colon conduit | 6 (5.7%) | 0 (0%) | 6 (7.6%) | |
| Jejunostomy (%) | 54 (51.4%) | 10 (38.5%) | 44 (55.7%) | 0.127 |
| Operation time (median, min) † | 600 (318–1008) | 628 (370–1008) | 599 (318–982) | 0.823 |
| Blood loss (median, mL) † | 345 (21–16,340) | 407 (35–1670) | 323 (21–16,340) | 0.577 |
| Complications, C–D grade, ≥2 (%) | ||||
| All infectious complications | 53 (50.5%) | 12 (46.2%) | 41 (51.9%) | 0.611 |
| AL | 16 (15.2%) | 5 (19.2%) | 11 (13.9%) | 0.514 |
| Pneumonia | 31 (29.5%) | 6 (23.1%) | 25 (31.6%) | 0.406 |
| SSI | 15 (14.3%) | 4 (15.4%) | 11 (13.9%) | 0.854 |
| Pathological stage, TNM 8th (%) | 0.659 | |||
| Stage 0 | 3 (2.9%) | 0 (0%) | 3 (3.8%) | |
| Stage IA/IB | 33 (31.4%) | 10 (38.5%) | 23 (29.1%) | |
| Stage IIA/IIB | 21 (20.0%) | 5 (19.2%) | 16 (20.3%) | |
| Stage IIIA/IIIB | 34 (32.4%) | 9 (34.6%) | 25 (31.6%) | |
| Stage IVA/IVB | 14 (13.3%) | 2 (7.7%) | 12 (15.2%) | |
| Adjuvant therapy (%) | 0.127 | |||
| None | 59 (56.2%) | 19 (73.1%) | 40 (50.6%) | |
| Chemotherapy | 45 (42.9%) | 7 (26.9%) | 38 (48.1%) | |
| Radiation | 1 (1.0%) | 0 (0%) | 1 (1.3%) | |
| 2 POD serum procalcitonin level (ng/mL) † | 0.53 (0.05–8.57) | 1.67 (1.00–8.57) | 0.35 (0.05–0.93) | <0.001 |
| Recurrence site * (%) | ||||
| Local recurrence | 6 (5.7%) | 1 (3.8%) | 5 (6.3%) | 0.636 |
| Regional LN | 26 (24.8%) | 2 (7.7%) | 24 (30.4%) | 0.020 |
| Distant organ | 17 (16.2%) | 3 (11.5%) | 14 (17.7%) | 0.458 |
| Death unrelated to esophageal cancer (%) | 3 (2.9%) | 2 (7.7%) | 1 (1.3%) | 0.088 |
| All Cases | Infectious Complication (+) | Infectious Complication (−) | p-Value | |
|---|---|---|---|---|
| 2 POD serum procalcitonin level (ng/mL) | 105 | 53 | 52 | 0.611 |
| ≥1 | 26 (24.8%) | 12 (46.2%) | 14 (53.8%) | |
| <1 | 79 (75.2%) | 41 (51.9%) | 38 (48.1%) | |
| 4 POD serum procalcitonin level (ng/mL) | 84 | 44 | 40 | 0.106 |
| ≥1 | 9 (10.7%) | 7(77.8%) | 2 (22.2%) | |
| <1 | 75 (89.3%) | 37 (49.3%) | 38 (50.7%) | |
| 7 POD serum procalcitonin level (ng/mL) | 98 | 52 | 46 | 0.017 |
| ≥1 | 6 (6.1%) | 6 (100%) | 0 (0%) | |
| <1 | 92 (93.9%) | 46 (50.0%) | 46 (50.0%) |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| HR | p | 95% CI | HR | p | 95% CI | |
| Age (years) | 1.032 | 0.234 | 0.980–1.087 | |||
| Gender (Male vs. Female) | 2.132 | 0.136 | 0.787–5.780 | |||
| Multidisciplinary team support (+ vs. −) | 1.295 | 0.475 | 0.636–2.639 | |||
| Thoracotomy (Open vs. MIE) | 1.12 | 0.754 | 0.552–2.273 | |||
| Laparotomy (Open vs. Laparoscopy) | 1.063 | 0.735 | 0.746–1.514 | |||
| LN dissection (2-field vs. 3-field) | 2.235 | 0.078 | 0.914–5.467 | |||
| All infectious complications (+ vs. −) | 1.299 | 0.478 | 0.631–2.677 | |||
| AL (+ vs. −) | 1.627 | 0.219 | 0.749–3.534 | |||
| Pneumonia (+ vs. −) | 0.959 | 0.917 | 0.442–2.084 | |||
| SSI (+ vs. −) | 1.756 | 0.122 | 0.860–3.584 | |||
| Pathological stage (≥II vs. <II) | 5.263 | <0.001 | 2.257–12.195 | 5.348 | <0.001 | 2.299–12.500 |
| 2 POD serum procalcitonin level (<1 vs. ≥1) | 3.553 | 0.037 | 1.080–11.695 | 3.673 | 0.032 | 1.116–12.092 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Booka, E.; Kikuchi, H.; Haneda, R.; Soneda, W.; Kawata, S.; Murakami, T.; Matsumoto, T.; Hiramatsu, Y.; Takeuchi, H. Usefulness of Procalcitonin as a Predictor of Long-Term Prognosis in the Early Postoperative Period after Esophagectomy for Esophageal Cancer. J. Clin. Med. 2022, 11, 3359. https://doi.org/10.3390/jcm11123359
Booka E, Kikuchi H, Haneda R, Soneda W, Kawata S, Murakami T, Matsumoto T, Hiramatsu Y, Takeuchi H. Usefulness of Procalcitonin as a Predictor of Long-Term Prognosis in the Early Postoperative Period after Esophagectomy for Esophageal Cancer. Journal of Clinical Medicine. 2022; 11(12):3359. https://doi.org/10.3390/jcm11123359
Chicago/Turabian StyleBooka, Eisuke, Hirotoshi Kikuchi, Ryoma Haneda, Wataru Soneda, Sanshiro Kawata, Tomohiro Murakami, Tomohiro Matsumoto, Yoshihiro Hiramatsu, and Hiroya Takeuchi. 2022. "Usefulness of Procalcitonin as a Predictor of Long-Term Prognosis in the Early Postoperative Period after Esophagectomy for Esophageal Cancer" Journal of Clinical Medicine 11, no. 12: 3359. https://doi.org/10.3390/jcm11123359
APA StyleBooka, E., Kikuchi, H., Haneda, R., Soneda, W., Kawata, S., Murakami, T., Matsumoto, T., Hiramatsu, Y., & Takeuchi, H. (2022). Usefulness of Procalcitonin as a Predictor of Long-Term Prognosis in the Early Postoperative Period after Esophagectomy for Esophageal Cancer. Journal of Clinical Medicine, 11(12), 3359. https://doi.org/10.3390/jcm11123359